Recommendations for Dental Care during COVID-19 Pandemic
by
 , , and
, , and
Katarzyna Gurzawska-Comis
1,†, 
Kathrin Becker
2,3,*,†,
Giulia Brunello
4,†,
Agata Gurzawska
5 and
Frank Schwarz
3 1
Department of Oral Surgery, University of Birmingham, 5 Mill Pool Way, Edgbaston, Birmingham B5 7EG, UK
2
Department of Orthodontics, Universitätsklinikum Düsseldorf, Moorenstr. 5, Building 18.21, 40225 Düsseldorf, Germany
3
Department of Oral Surgery and Implantology, Carolinum, Goethe University, Theodor-Stern-Kai 7/Haus 29, 60596 Frankfurt am Main, Germany
4
Department of Neurosciences, Dentistry Section, University of Padova, Via Giustiniani 2, 35128 Padova, Italy
5
Trilateral Research Ireland, Marine Point, Belview Port, X91 W0XW Waterford, Ireland
*
Author to whom correspondence should be addressed.
†
The authors contributed equally to this work.
J. Clin. Med. 2020, 9(6), 1833; https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061833
Submission received: 20 May 2020
/
Revised: 5 June 2020
/
Accepted: 9 June 2020
/
Published: 12 June 2020
(This article belongs to the Special Issue Biomaterials and Advanced Therapies against Virus: How Could They Help Us for Corona Virus Infection?)
Abstract
:Dental clinics were suspected to be a hotspot for nosocomial transmission of coronavirus disease 19 (COVID-19), yet there has been no clear recommendation about emergency dental care and appropriate personal protective equipment during pandemics. In this paper, we aim to summarize recommendations for (i) patient risk assessment, (ii) patient triage, and (iii) measures to prevent infection of health professionals and nosocomial transmission in dental clinics. The available evidence was collected by performing searches on PubMed, Embase, and Cochrane databases. We reviewed papers on COVID-19, severe acute respiratory syndrome (SARS), Middle East respiratory syndrome (MERS), influenza, and related respiratory viral diseases. Legal and ethical frameworks, as well as international (e.g., World Health Organization (WHO)) and national (e.g., public health institutes, dental associations) guidelines were screened to summarize recommendations related to dental emergency care. To assess the patient risk, a questionnaire was developed to classify patients at unknown, high, and very high risk. Patient triage recommendations were summarized in a flow chart that graded the emergency level of treatments (i.e., urgent, as soon as possible, and postpone). Measures to prevent disease transmission based on current evidence were grouped for dental health professionals, dental clinics, and patients. The present recommendations may support health professionals implement preventative measures during the pandemic.
{kind=link}
{kind=link}
{kind=link}
1. Introduction
A novel coronavirus disease 19 (COVID-19) caused by a β-coronavirus (Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)) was first reported in December 2019 (Wuhan, China). On 11 March 2020, COVID-19 was declared a public health emergency of international concern by the World Health Organization (WHO). As of 5 June 2020, the Johns Hopkins University website reported that there were 6,627,287 confirmed cases worldwide and 391,686 total deaths across 188 different countries. The true number of infected people and deaths, however, is estimated to be even higher [1].
Specific features of the novel coronavirus account for its high transmissibility and pathogenicity. The virus can be directly transmitted through cough, sneeze, and respiratory droplets, as well as by contact-transmission [2,3,4]. Patients are contagious prior to the onset of clinical symptoms [5] and the contagiousness can last up to three weeks after recovery [6,7]. Moreover, patients with very mild or subclinical symptoms were found infective [8]. As incubation periods can exceed 14 days [9] and only a few patients are tested due to limited capabilities, detecting contagious people is challenging. Virus aerosol viability of >3 h and high surface stability of >72 h may further account for a high risk of nosocomial transmission [10].
Recently, the highest infection potential among all health care professionals was reported for dentists, dental assistants, and dental hygienists, as they are in close contact with patients, and exposed to spatter of patient’s secretions, saliva, and aerosol [11]. Hence, dental offices may be a relevant hotspot for virus transmission, putting health professionals at high risk of SARS-CoV-2 infection and patients at risk of nosocomial infection.
Meng et al. were the first to report on personal protection equipment (PPE) that protected dental professionals during the COVID-19 epidemic in Wuhan, China [12]. At that time, all private offices were closed in the Hubei region to prevent nosocomial infection, hospitals were restricted to emergency treatment, and dentists were equipped with PPE. In other countries, such as Poland and Germany, elective treatment is not prohibited and due to a lack of clear recommendations, dentists have to evaluate whether to close their offices, how to communicate with patients, and what type of PPE to buy.
The aim of this work is to summarize recommendations for (i) individual risk assessment, (ii) patient triage, and (iii) measures to prevent health professionals from infection and nosocomial transmission at dental clinics. The study also aimed to synthesize the related legal and ethical frameworks justifying the proposed recommendations.
Present recommendations are provided to serve dentists to implement appropriate measures for minimizing the risks of nosocomial COVID-19 transmission and to prevent infection of dental health professionals.
2. Experimental Section
The present recommendations were prepared after reviewing the available literature and guidelines regarding COVID-19, severe acute respiratory syndrome (SARS), Middle East respiratory syndrome (MERS), pandemic influenza, and related respiratory viral diseases. As public health emergencies also pose ethical, social, and legal dilemmas, available expert statements were also assessed.
2.1. Composition of the Recommendation Development Group
The steering group who developed these recommendations is composed of dental researchers and clinicians with several years of expertise in systematic review and literature searches. In addition, one lawyer was included to address concerns related to dental emergency care from a legal and ethical framework.
2.2. The End-User of the Recommendations
The present recommendations are intended for dental health professionals, hospital managers, and politicians.
2.3. Data Searches
PubMed, Embase, and Cochrane databases were searched using the following terms: “COVID-19”, “coronavirus”, “dental emergencies”, “personal protective equipment”, “SARS”, “MERS”, “dentistry”, “triage”, “medical ethics”, “bioethics”, “right to health”, “dentist code of ethics”, “human rights”, and “pandemics”. A hand search was performed to consider the preventive measures specified in Section 2.4. Due to the topic’s novelty, studies in English, German, Italian, and Polish were screened by the authors. No publication type restrictions were applied. The screening for relevant literature was limited up to 1 June, 2020. Due to the recent onset of COVID-19, expert’ opinions summarized in international guidelines were also considered [13]. Furthermore, legal and ethical frameworks, as well as national (e.g., dental societies, public health institutes) and international guidelines (e.g., WHO, European Centre for Disease Prevention and Control, Infection prevention and control for COVID-19, Council of European Dentists) related to dental emergency care were screened.
2.4. Synthesis of Literature
The available literature was synthesized according to the following topics:
- Virus transmission and pathogenicity.
- Testing.
- Assessment of individual COVID-19 risk.
- Classification of emergency level for dental treatments.
- Measures by health care professionals to limit virus spread, including masks, face shields, coats, gloves, and double shoes.
- Measures to limit nosocomial infection at dental clinics, including disinfection, isolation rooms, ventilation, waiting rooms, dining, and locker rooms.
- Measures applied by patients including overshoes, masks, and mouth rinses.
- Information collected from legal and ethical frameworks relevant to COVID-19 pandemic in dentistry.
3. Results
3.1. Virus Transmission and Pathogenicity
The transmission mechanism of SARS-CoV-2 has not yet been fully understood. Initially, the proposed main transmission routes were direct, through cough, sneeze, and respiratory droplets, as well as contact with mucous membranes of eyes, nose, or oral cavity [12,14,15]. Recent studies demonstrated high loads of virus RNA in hospital aerosol [16]. Moreover, particles generated by asymptomatic carriers while speaking are increasingly considered to be a major mode of transmission as the virus remained suspended in air for 10s of minutes or even longer [17,18,19]. Hence, 9 cases out of 10 of SARS-CoV-2 transmission has been estimated to be airborne. This is in-line with recent findings revealing substantial virus load in the oral mucosa and in stimulated saliva from submandibular gland duct [20,21]. Comparable virus loads were reported for children and adults [22], thus suggesting that children may be as infectious as adults.
The median incubation period was reported to be 5.1 days [95% CI: 4.5–5.8 days], however the incubation periods can exceed 14 days [9]. Patients were shown to be contagious prior to the onset of clinical symptoms [23]. Moreover, patients presenting with very mild or subclinical symptoms were found infective [4,6,7] and the contagiousness could persist up to three weeks after recovery [8,24]. The ratio of asymptomatic to symptomatic patients was estimated to be 41–42% [25,26].
3.2. Testing
At present, COVID-19 testing can identify the SARS-CoV-2 virus and two methods are most frequently applied, i.e., nucleoid acid and antibody detection techniques. The first method using real time polymerase chain reaction (RT-PCR) indicates the presence of the virus in the tested sample. The second one detects antibodies produced in response to infection. Another option to identify the COVID-19 is assessment of lung damage via either a computed tomography (CT) scan or low oxygen uptake saturation. Antigen detection [18] and isothermal amplification assays [28,29,30] are considered the fastest methods for detection of COVID-19. However cross-reactivity with other seasonal flu coronaviruses has been reported, which decreases specificity of a positive outcome [31,32,33].
The RT-PCR is currently considered as the “gold standard” and is characterized by rapid detection, high sensitivity, and specificity [34]. The sample for RT-PCR is obtained by a nasopharyngeal swab or sputum, as well as saliva [35]. Within a recent study by Wyllie et al., 2020, saliva and nasopharyngeal swab samples collected from inpatients and co-workers were compared [35]. The results indicated that saliva yielded greater detection sensitivity and consistency throughout the course of infection. Furthermore, the authors suggested that saliva may be more sensitive for detecting asymptomatic or pre-symptomatic infections. Further studies confirmed higher sensitivity of saliva as a diagnostic specimen compared to nasopharyngeal swabs [36,37,38,39].
3.3. Individual Risk Assessment
Clinical manifestations including flu-like symptoms, dry cough, fever, shortness of breath, anosmia, or headache are frequently associated with COVID-19. In addition, patients who recently travelled to COVID-19 high risk countries (WHO) and/or having contact with COVID-19 positive patients during the last 14 days exhibited an elevated risk of infection. Furthermore, asymptomatic patients without travel history/contact with COVID-19 positive patients may be contagious and their risk may be considered unknown [9]. The epidemiological history [40] and clinical manifestation [41] assessment was therefore suggested to identify patients with suspected risk of COVID-19. The Polish Dental Association (PTS) [42] and American Association of Endodontists proposed questionnaires to classify individual patient risk [43]. The risk of severe disease associated with COVID-19 for people in the EU/EEA, Switzerland, and UK is currently considered moderate for the general population and very high for older adults and individuals with chronic underlying conditions [44,45]. As the clinical situation may vary over time, a screening process over the phone has been proposed to be confirmed at the dental office [46,47,48].
3.4. Classification of Emergency Level for Dental Treatments
The various national dental guidelines published by the American Dental Association, the Polish Dental Association, the Società Italiana di Parodontologia e Implantologia, and the Swiss Association of Dentists, recommend avoiding elective treatments during the COVID-19 pandemic [42,45,49,50]. A triage is considered fundamental to prevent nosocomial transmission and infection of health care professionals. Few guidelines further specify the emergency level for dental treatments [45,49,51]. The Scottish recommendation proposed emergency, urgent, and routine care [51]. At this point it has to be emphasized that emergency usually implies life-threatening conditions, which are not-commonly performed by dentists but by oral and maxillofacial surgeons within hospital settings. Most guidelines recommended assessing dental treatment needs using telephone and video review as the primary route.
3.5. Measures by Health Care Professionals to Limit Virus Spread, Including Masks, Face Shields, Coats, Gloves, Double Shoes
3.5.1. Use of Masks
Due to the direct transmission of SARS-COV-2, masks were found to be an effective measure to prevent infection (difference mask versus no mask: 4.65%, p < 2.2 × 10−16) [52].
The efficacy of N95 respirators against surgical masks was examined in a systematic review and meta-analysis [53]. After performing a sensitivity analysis, the authors identified a beneficial effect of N95 respirators on preventing respiratory viral infection compared to surgical masks (relative risk (RR) = 0.61, 95% CI 0.39–0.98, p < 0.05). Furthermore, N95 respirators significantly reduced bacterial colonization in hospitals (RR = 0.58, 95% CI 0.43–0.78, p < 0.05). One in vitro study demonstrated that a tightly sealed surgical mask blocked 94.5% of total virus whereas a tightly sealed respirator blocked 99.8%. In contrast, a poorly fitted respirator blocked only 64.5%. A simulation of how masks are worn by healthcare professionals revealed that 68.5% of total viruses were blocked. These results indicate that a poorly fitted respirator performs no better than a loosely fitting surgical mask [54].
The US National Institute for Occupational Safety and Health (NIOSH) classifies particulate filtering facepiece respirators (FFRs) depending on their capacity to filter oil droplets into nine categories: N, not resistant to oil (N95, N99, N100); R, somewhat resistant to oil (R95, R99, R100); and P, strongly resistant to oil (P95, P99, P100). The numerical identifier corresponds to the minimum filtration efficiency (i.e. 95%, 99%, and 99.97%). The European Standard (EN 149:2001) defines three classes of filtering face pieces (FFP), with minimum filtration efficiencies of 80% (FFP1), 94% (FFP2), and 99% (FFP3). Hence, FFP2 are considered equivalent to N95 and FFP3 to N99 [55].
The WHO recommended in its interim guideline on COVID-19 the use of NIOSH-certified N95, European Union (EU) FFP2, or equivalent masks, when aerosol-generating procedures are performed [56]. In the case of short storage PPE, the cause of N95 respirator was proposed to be reused, with multiple removals between patients [57].
Concerns have been recently raised about use of FFP3 masks with valves, due to the increased risk of COVID-19 transmission for the patient through unfiltered exhaled clinician’s breath. Therefore, it has been suggested to combine the use of surgical masks covering FFP3 with a valve [58]. This should be applied also to FFP2 masks with valves.
3.5.2. Use of Face Shields/Goggles
Face shields and goggles are commonly considered as adjunctive measures combined with either surgical masks or N95/FFP2/FFP3 respirators.
An in vitro study [59] reported, face shields provide about 96% prevention immediately after exposure to influenza-laden cough aerosol. This value decreased to 23% when the aerosol had dispersed throughout the room.
Therefore, goggles may provide increased eye protection [60].
3.5.3. Additional Measures (Gowns, Overshoes, Gloves)
3.6. Measures to Limit Nosocomial Infection at Dental Clinics, including Disinfection, Isolation Rooms, Ventilation, Waiting Rooms, Dining, and Locker Rooms
3.6.1. Disinfectants against Human Coronavirus
SARS-CoV-2 was found to maintain stability on copper surfaces, ceramics and glass up to 4–5 h, on gloves up to 8 h, and on carton plastic and steel from 24 h up to 3 days [10]. Disinfectants containing ethanol (78%–95%), iodopovidone solution (0.23%–7.5%) inactivated high-concentration coronavirus within 30 s to 1 min [5,6,8]. To effectively inactivate SARS-CoV-2 virus with sodium hypochlorite, a minimum concentration of 0.21% (applied for 30 s) was required [63].
3.6.2. Ventilation
Very few studies have evaluated the association of ventilation on disease transmissibility. A positive effect of (natural) ventilation has been suggested [64], which reduced pathogen transmission [65]. The WHO guideline 2009 on natural ventilation for infection control in healthcare settings recommended an hourly average ventilation rate of 160 l/s/patient for airborne precaution rooms [66].
3.6.3. Isolation Rooms
Isolation rooms are commonly used to exclude patients with highly infectious diseases. Meng, Hua, and Bian [12] suggested negative pressure isolation rooms for dental emergency care for COVID-19+ patients and aerosol-generating procedures. No further evidence was found.
3.6.4. Air Disinfection
3.7. Measures Applied by Patients including Hand Hygiene, Overshoes, Masks, and Mouth Rinse
3.7.1. Hand Hygiene
Handwashing with soap was found to be the most effective for elimination of enveloped viruses (such as SARS-CoV-2), especially when compared with alcohol-based hand rubs [71].
3.7.2. Masks
A tendency towards increased use of masks has been observed in countries affected by the COVID-19 epidemic [72]. Surgical mask worn by infected patients was shown to limit virus transmission [73,74]. Since asymptomatic COVID-19 patients can be highly contagious, use of masks may be an adjunctive measure to limit virus transmission [75].
3.7.3. Other Measures
Additional adjunctive measures including locking personal belongings and wearing disposable overshoes have been recommended [47,48,50], since sources of bioaerosols can arise from human clothes or furniture [76]. Due to the risk of airborne transmission, eliminating the number of patients inside the dental clinic or keeping a distance of at least 1 m in waiting areas has also been advised [55].
3.7.4. Mouth Rinse
Preoperative mouthwash containing oxidative agents, such as 1–1.5% hydrogen peroxide or 0.2% povidione iodine, were reported to be viricide [77,78]. Antiseptic mouth rinses, e.g., Chlorhexidine (0.2%) and Listerine® (with adjunctive alcohol) may also exhibit viricide properties [79,80]. In contrast, Chorhexidine (0.1% and 0.2%) without adjunctive alcohol are suspected not to be effective against viruses [78,81]. Cetylpyridinium chloride (CPC) may possess viricide activity especially against enveloped viruses [82,83]. Flavonoids and β-Cyclodextrin-Citrox compounds were also suggested to be effective [81,84]. However, there is a lack of evidence to what extent adjunctive compounds could elevate the substantivity of the rinses.
3.8. Aspects Collected from Legal and Ethical Frameworks Relevant to COVID-19 Pandemic in Dentistry
The COVID-19 pandemic raises ethical and legal questions including priorities in the allocation of resources and access to medical care. The four principles of medical ethics namely respect for autonomy, beneficence, nonmaleficence, and justice, may support dentists in making decisions when reflecting on moral issues that arise at work during pandemics.
Dentists have a duty to act in the best interests of patients and prioritize their interest (principle of beneficence) while respecting their dignity, autonomy, and choices (principle of autonomy) [87]. COVID-19 threatens particularly vulnerable groups such as the elderly, individuals with underlying systemic diseases (e.g., cardiovascular disease, diabetes, chronic respiratory disease, and hypertension). or individuals living in socially deprived circumstances. During pandemics, personal human dignity remains the highest of all values, it is independent from social standing or of usefulness to others [88]. Hence, treatments should be provided regardless a patient’s age, sex, national or ethnic origin, color, place of residence, social, or economic status (principle of justice). Accordingly, patients should be admitted for the urgent treatment based on strictly medical prognosis. The COVID-19 amplifies the problems to access to medical care and issues related to scarce resources. Therefore, it is ethically justified to re-schedule or cancel elective procedures. Nevertheless, dentists should remain available to manage urgent treatment needs [49,55,89].
Dentists have a duty to provide the most essential and appropriate care and to treat patients according to their needs [87]. Nevertheless, during pandemics the duty to treat or to care may need to be balanced with doctors’ right to life and to protect their own, their family, and dental team’s life and health [90,91].
4. Recommendations
Based on currently available evidence and international guidelines, the following recommendations are proposed.
4.1. Individual Risk Assessment
We recommend that patients who had contact with COVID-19 positive patients or visited any high-risk region according to the WHO in the last 14 days should be classified as very high-risk patients.
We recommend that patients who had contact with COVID-19 positive patients or visited any high-risk region according to the WHO in the last 14 days, but do not show flu-like symptoms should be classified as very high-risk patients.
We recommend that patients who did not have contact with COVID-19+ patients or did not visit any high-risk region according to the WHO in the last 14 days but show flu-like symptoms should be classified as high-risk patients.
All other patients should be classified as having an unknown risk, i.e., being potentially contagious.
A questionnaire to evaluate risk assessment is provided in File S1. The outcomes of the questionnaire are recommended to be translated into the individual risks as follows:
- –
- Very high risk: The patient scores at least 1 YES in epidemiological history AND/OR patient has been tested positive for COVID-19
- –
- High risk: The patient scores at least 0 YES in epidemiological history and at least 1 in clinical manifestation
- –
- Unknown risk: The patient scores 0 YES in epidemiological history and 0 YES in clinical manifestation.
Rationale of the Authors
Due to the high number of asymptomatic patients and the contagiousness prior to and after the onset of clinical symptoms, the authors recommend that every patient has to be considered potentially contagious during the COVID-19 pandemic. However, particular precaution is advisable for patients with a very high likelihood of contagiousness.
4.2. Patient Triage Recommendation
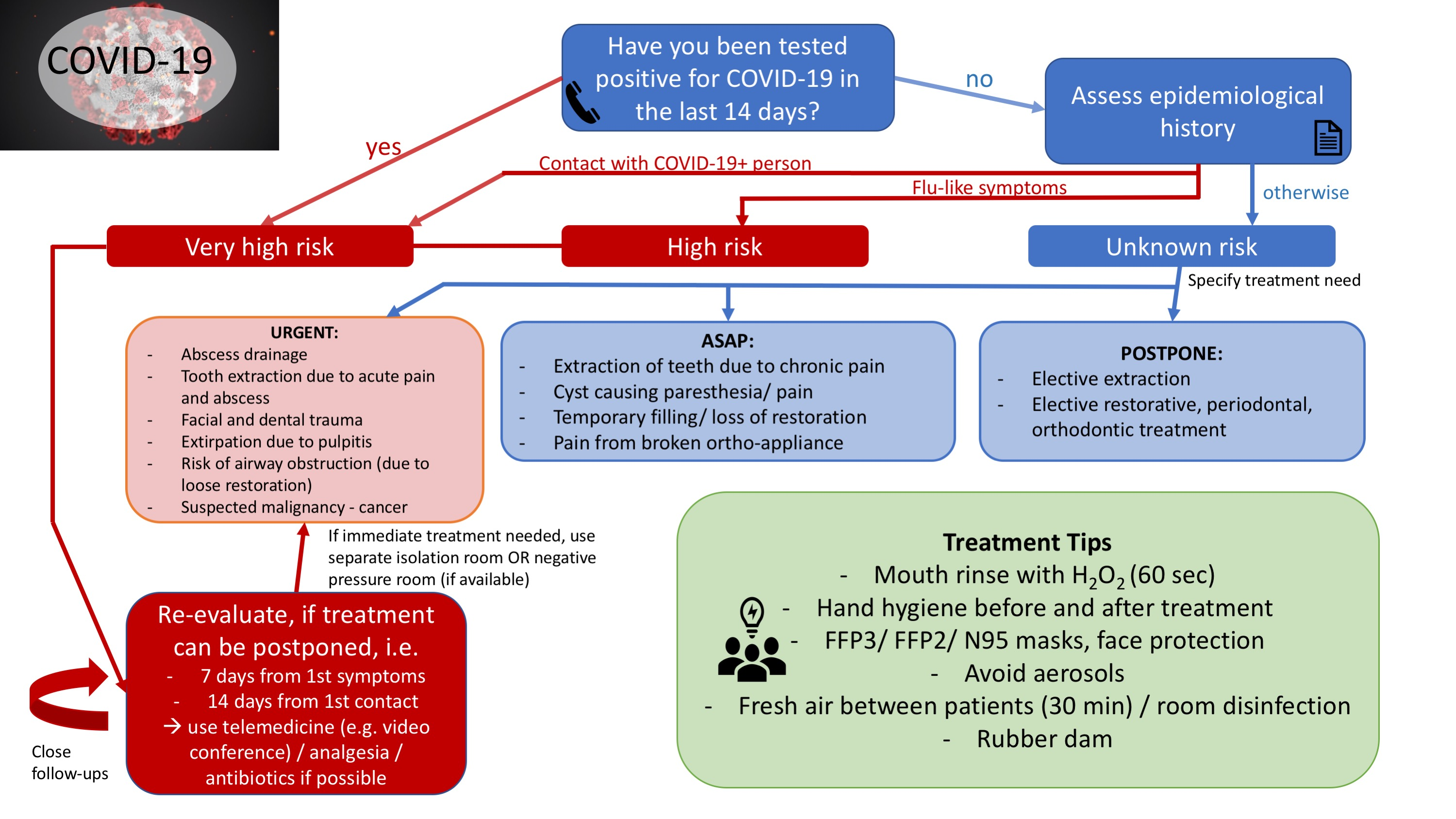
We recommend classifying dental treatment needs as urgent (within the next 24 h), as soon as possible (ASAP) (within the next 7 days) and postpone (no urgency). The recommendations are summarized in Figure 1. For the patient triage, we divided the recommendations into general, as well as COVID-19 risk specific (see Section 4.1).
4.2.1. General Recommendations
Prior to the visit, we recommend assessing individual patient risk and dental treatment needs at the telephone or through a video conference.
To limit the number of potentially contagious people in the clinic, the patient should not report with accompanying people. Exceptions comprise disabled, children, or geriatric and hospitalized patients. Furthermore, aerosol free treatments should be selected (if possible). When radiographs are needed, extraoral radiographs should be preferred. Rubber dam may be used when applicable to limit virus transmission.
4.2.2. Triage Recommendations
Patients exhibiting very high risk should generally not be seen at the clinic unless they have an urgent treatment need (video conference may be used to validate urgent treatment needs). Otherwise, antiseptics or antibiotics in combination with frequent telephone interviews may be used to postpone the treatment until recovery.
Questions to identify urgent treatment needs may include:
- Do you have pain? Yes/No
- If yes, where is the pain and from how long? Yes/No
- Is the pain associated with swelling and limited opening of the mouth? Yes/No
- Have you taken any medication, like paracetamol/ibuprofen/Aspirin? If yes, did you find any relief? Yes/No
- Do you have any underlying medical conditions? If yes, which one.
Rationale of the Authors
Based on legal and ethical frameworks, dental treatments have to be provided to all patients in demand or pain. During the COVID-19 pandemic, social distancing is mandatory to minimize the spread of the virus and there is a risk of nosocomial transmission at dental clinics. Therefore, we recommend avoiding dental treatments unless they cannot be postponed. However, concerns may arise regarding the unnecessary overprescribing of antibiotics from tele-dentistry, thus contributing to the development of antibiotic resistance.
4.3. Measures to Prevent Infection in Dental Settings
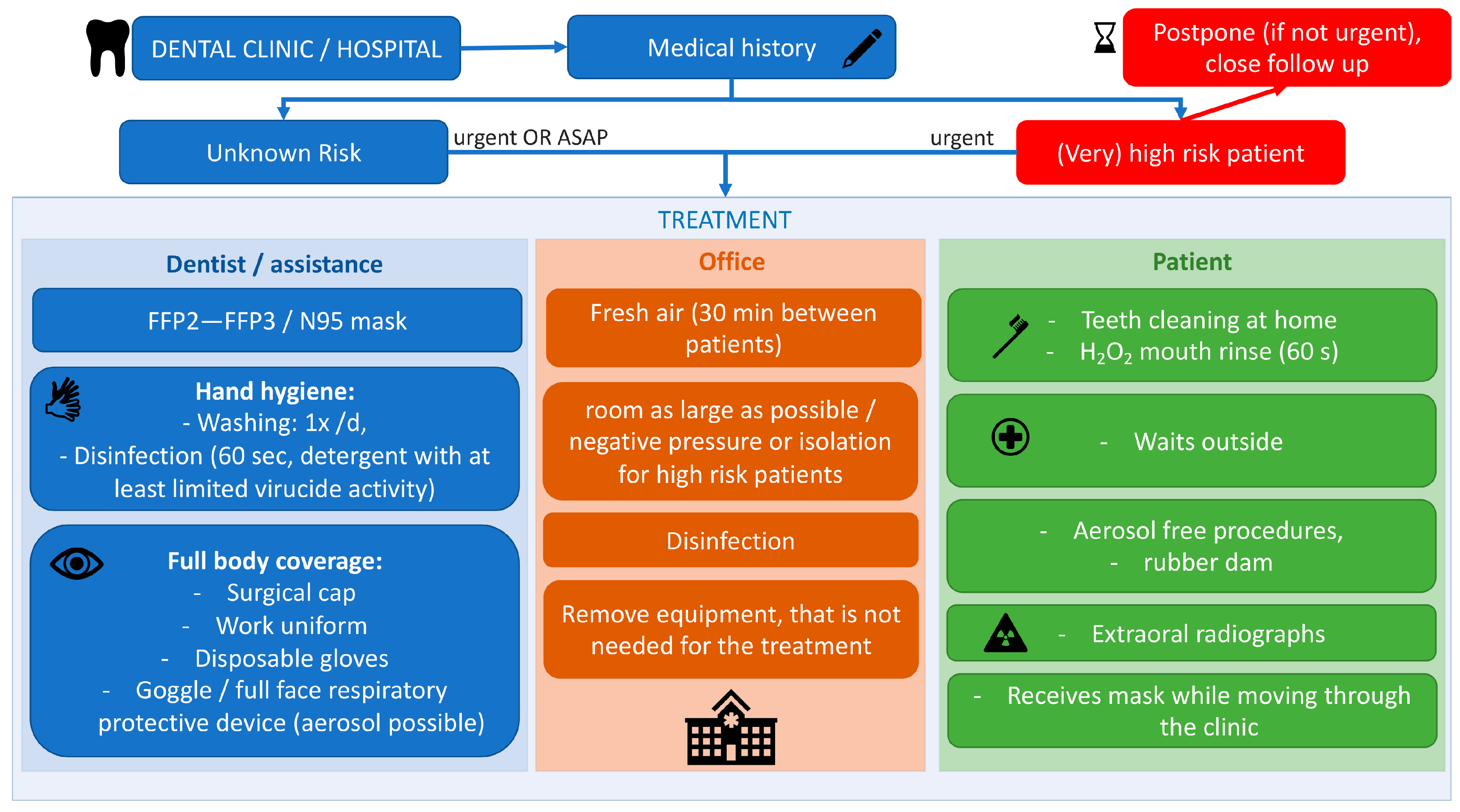
We recommend the following measures to be adopted during COVID-19 pandemic. The measures are summarized in Figure 2.
4.3.1. Personal Protective Equipment for Dental Professionals
For patients exhibiting a (very) high COVID-19 risk, we recommend using N95/FFP2 or FFP3 masks with proper fit, face-shields, and regular gloves. Adjunctive use of caps, overshoes, and coats may further increase safety. The same measures are recommended to be used for patients exhibiting an unknown risk, whereas a regular surgical mask may be combined with a face-shield for aerosol-free treatments in scarcity of PPE.
4.3.2. Recommendations Regarding the Dental Clinic
Between consecutive patients, we recommend proper disinfection and sufficient room ventilation (time depends on the size of the room, the number and the size of the windows, the type of treatment). For room disinfection, ethyl-alcohol (78%) is considered to be the most effective. Disinfection should include all flat surfaces, computers, keyboard, mouse, lamps, and doorknobs.
Negative pressure isolation rooms may be considered to treat patients with COVID-19 or very high risk of disease to prevent virus-laden aerosols transmission. However, it has to be noted that isolation rooms are only effective when the airflow direction is well controlled by adequate pressure monitors and negative pressure control devices.
4.3.3. Recommendations to Be Followed by Patients
We recommend patients attending dental clinics must perform hand hygiene using alcohol-based hand rub or soap and water. Patients should store their belongings in a locker outside the clinic and wear overshoes (if available). They should be instructed to refrain from touching their mouth, nose, and eyes with dirty hands, and they should avoid shaking hands. If outdoor waiting is inevitable, patients are recommended to maintain at least a 1 m distance in the waiting areas. Prior to the treatment, we recommend rinsing with a mouth wash to reduce the virus load in saliva prior to beginning dental treatment. Hydrogen peroxide (1–1.5%) or povidione iodine (0.2%) were reported to be most effective.
Rationale of the Authors
Due to the high risk of nosocomial transmission and as every person is potentially contagious, maximum prevention measures are required to prevent direct-contact transmission, but also indirect transmission of the virus.
4.4. Future Perspectives for Elective Dental Care
We recommend that patients, before visiting the dental office, have epidemiological and clinical screening. Ideally, patients and health professionals should also be tested for COVID-19 before dental treatment. Unless COVID-19 test of a patient has been negative, elective treatments should be performed following the infection control measures presented in above recommendations. Briefly, if the treatment includes aerosol generating procedures, the FFP2/FFP3 masks and other PPE should be used. If the treatment does not include aerosol, surgical mask with visor may be used unless there are other risks such as underlying medical conditions.
5. Conclusions
The risk of COVID-19 infection by dental staff and also the risk of nosocomial transmission in dental practices is considered high. The reasons are the short distance to the patient, proximity to saliva, blood, spatter and aerosol exposure. In many countries affected by COVID-19, elective dental treatments were suggested to be postponed. Since every patient can be potentially contagious, increased safety measures were suggested to all patients when treatment is mandatory.
As neither dentists nor the (inter-)national hygiene guidelines appeared to be prepared for the present pandemic and to limit infection and COVID-19 transmission in dental clinics, the present article proposed recommendation on the following topics: (i) individual risk assessment, (ii) patient triage, (iii) measures to prevent infection of health professionals’, and nosocomial transmission at dental clinics.
However, limited evidence was available regarding COVID-19. Therefore, the present recommendations were also based on evidence from similar diseases, such as SARS and MERS.
The described recommendations were suggested for the COVID-19 pandemic only. Before vaccination is available, less strict recommendations may be required to prevent infection and nosocomial transmission in dentistry.
Furthermore, rapid test kits are becoming available and their extensive use prior to dental care provision might help in determining the health status of the patients. As the duration of the pandemic cannot be predicted at the moment and elective treatments cannot be indefinitely postponed, testing may represent a positive turning point in dental patients’ management during pandemic, thus allowing to safely provide elective treatments, also involving aerosol-generating procedures, in COVID-19 negative patients.
Supplementary Materials
The following are available online at https://0-www-mdpi-com.brum.beds.ac.uk/2077-0383/9/6/1833/s1, File S1: Questionnaire for risk assessment.
Author Contributions
Conceptualization, K.G.-C., K.B., G.B., and F.S.; design: K.G.-C., K.B., G.B., and F.S.; literature synthesis and interpretation, K.G.-C., K.B., G.B., and F.S.; literature synthesis on ethical and legal frameworks, A.G.; writing—original draft preparation, K.G.-C., K.B., and G.B.; writing—review and editing, K.G.-C., K.B., G.B., A.G., and F.S. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
In order to avoid potential bias in the development of these recommendations, financial and/or personal conflict of interests were surveyed and disclosed prior to the preparation of the manuscript. No conflicts of interests were declared.
References
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2). Science 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, J.F.; Yuan, S.; Kok, K.H.; To, K.K.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.; Poon, R.W.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.; Zhu, J.; Zhang, Z.; Han, Y.; Huang, L. A familial cluster of infection associated with the 2019 novel coronavirus indicating potential person-to-person transmission during the incubation period. J. Infect. Dis. 2020. [Google Scholar] [CrossRef] [Green Version]
- Woelfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Mueller, M.A.; Niemeyer, D.; Vollmar, P.; Rothe, C.; Hoelscher, M.; et al. Clinical presentation and virological assessment of hospitalized cases of coronavirus disease 2019 in a travel-associated transmission cluster. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [Green Version]
- Hoehl, S.; Rabenau, H.; Berger, A.; Kortenbusch, M.; Cinatl, J.; Bojkova, D.; Behrens, P.; Boddinghaus, B.; Gotsch, U.; Naujoks, F.; et al. Evidence of SARS-CoV-2 Infection in Returning Travelers from Wuhan, China. N. Engl. J. Med. 2020, 382, 1278–1280. [Google Scholar] [CrossRef]
- Qian, G.; Yang, N.; Ma, A.H.Y.; Wang, L.; Li, G.; Chen, X.; Chen, X. A COVID-19 Transmission within a family cluster by presymptomatic infectors in China. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The Incubation Period of Coronavirus Disease 2019 (COVID-19) from Publicly Reported Confirmed Cases: Estimation and Application. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Fallahi, H.R.; Keyhan, S.O.; Zandian, D.; Kim, S.G.; Cheshmi, B. Being a front-line dentist during the Covid-19 pandemic: A literature review. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 12. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schunemann, H.J.; Zhang, Y.; Oxman, A.D. Distinguishing opinion from evidence in guidelines. BMJ 2019, 366, l4606. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.W.; Liu, X.F.; Jia, Z.F. 2019-nCoV transmission through the ocular surface must not be ignored. Lancet 2020, 395, e39. [Google Scholar] [CrossRef] [Green Version]
- Xia, J.; Tong, J.; Liu, M.; Shen, Y.; Guo, D. Evaluation of coronavirus in tears and conjunctival secretions of patients with SARS-CoV-2 infection. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Liu., Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdahl, D.; et al. Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals. Nature 2020. [Google Scholar] [CrossRef]
- Stadnytskyi, V.; Bax, C.E.; Bax, A.; Anfinrud, P. The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. Proc. Natl. Acad. Sci. USA 2020. [Google Scholar] [CrossRef]
- Jianyun, L.; Jieni, G.; Kuibiao, L.; Conghui, X.; Wenzhe, S.; Zhisheng, L.; Deqian, Z.; Chao, Y.; Bin, X.; Zhicong, Y. COVID-19 Outbreak Associated with Air Conditioning in Restaurant, Guangzhou, China, 2020. Emerg. Infect. Dis. J. 2020, 26. [Google Scholar] [CrossRef]
- Buonanno, G.; Stabile, L.; Morawska, L. Estimation of airborne viral emission: Quanta emission rate of SARS-CoV-2 for infection risk assessment. Environ. Int. 2020, 141, 105794. [Google Scholar] [CrossRef]
- Chen, L.; Zhao, J.; Peng, J.; Li, X.; Deng, X.; Geng, Z.; Shen, Z.; Guo, F.; Zhang, Q.; Jin, Y.; et al. Detection of 2019-nCoV in Saliva and Characterization of Oral Symptoms in COVID-19 Patients. SSRN 2020, in press. [Google Scholar]
- To, K.K.-W.; Tsang, O.T.-Y.; Yip, C.C.-Y.; Chan, K.-H.; Wu, T.-C.; Chan, J.M.-C.; Leung, W.-S.; Chik, T.S.-H.; Choi, C.Y.-C.; Kandamby, D.H.; et al. Consistent Detection of 2019 Novel Coronavirus in Saliva. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, T.C.; Mühlemann, B.; Veith, T.; Zuchowski, M.; Hofmann, J.; Stein, A.; Edelmann, A.; Corman, V.M.; Drosten, C. An analysis of SARS-CoV-2 viral load by patient age. Ger. Res. Netw. Zoonotic Infect. Dis. Website 2020, in press. [Google Scholar]
- Ganyani, T.; Kremer, C.; Chen, D.; Torneri, A.; Faes, C.; Wallinga, J.; Hens, N. Estimating the generation interval for COVID-19 based on symptom onset data. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Xing, Y.; Mo, P.; Xiao, Y.; Zhao, O.; Zhang, Y.; Wang, F. Post-discharge surveillance and positive virus detection in two medical staff recovered from coronavirus disease 2019 (COVID-19), China, January to February 2020. Eurosurveillance 2020, 25. [Google Scholar] [CrossRef]
- Nishiura, H.; Kobayashi, T.; Miyama, T.; Suzuki, A.; Jung, S.; Hayashi, K.; Kinoshita, R.; Yang, Y.; Yuan, B.; Akhmetzhanov, A.R.; et al. Estimation of the asymptomatic ratio of novel coronavirus infections (COVID-19). medRxiv 2020. [Google Scholar] [CrossRef]
- Mizumoto, K.; Kagaya, K.; Zarebski, A.; Chowell, G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Eurosurveillance 2020, 25, 2000180. [Google Scholar] [CrossRef] [Green Version]
- Wax, R.S.; Christian, M.D. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can. J. Anaesth. 2020, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Carter, L.J.; Garner, L.V.; Smoot, J.W.; Li, Y.; Zhou, Q.; Saveson, C.J.; Sasso, J.M.; Gregg, A.C.; Soares, D.J.; Beskid, T.R.; et al. Assay Techniques and Test Development for COVID-19 Diagnosis. ACS Cent. Sci. 2020, 6, 591–605. [Google Scholar] [CrossRef]
- Tang, Y.W.; Schmitz, J.E.; Persing, D.H.; Stratton, C.W. Laboratory Diagnosis of COVID-19: Current Issues and Challenges. J. Clin. Microbiol. 2020, 58, e00512–e00520. [Google Scholar] [CrossRef] [Green Version]
- Sharma, S.; Kumar, V.; Chawla, A.; Logani, A. Rapid detection of SARS-CoV-2 in saliva: Can an endodontist take the lead in point-of-care COVID-19 testing? Int. Endod. J. 2020. [Google Scholar] [CrossRef]
- Lv, H.; Wu, N.C.; Tak-Yin Tsang, O.; Yuan, M.; Perera, R.A.P.M.; Leung, W.S.; So, R.T.Y.; Chun Chan, J.M.; Yip, G.K.; Hong Chik, T.S.; et al. Cross-reactive antibody response between SARS-CoV-2 and SARS-CoV infections. Cell Rep. 2020. [Google Scholar] [CrossRef] [PubMed]
- Jacofsky, D.; Jacofsky, E.M.; Jacofsky, M. Understanding Antibody Testing for COVID-19. J. Arthroplast. 2020, 27, S0883–S5403. [Google Scholar] [CrossRef] [PubMed]
- Jääskeläinen, A.J.; Kekäläinen, E.; Kallio-Kokko, H.; Mannonen, L.; Kortela, E.; Vapalahti, O.; Kurkela, S.; Lappalainen, M. Evaluation of commercial and automated SARS-CoV-2 IgG and IgA ELISAs using coronavirus disease (COVID-19) patient samples. Eurosurveillance 2020, 25, 2000603. [Google Scholar] [CrossRef]
- Tahamtan, A.; Ardebili, A. Real-time RT-PCR in COVID-19 detection: Issues affecting the results. Expert Rev. Mol. Diagn. 2020, 20, 453–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyllie, A.L.; Fournier, J.; Casanovas-Massana, A.; Campbell, M.; Tokuyama, M.; Vijayakumar, P.; Geng, B.; Muenker, M.C.; Moore, A.J.; Vogels, C.B.F.; et al. Saliva is more sensitive for SARS-CoV-2 detection in COVID-19 patients than nasopharyngeal swabs. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Williams, E.; Bond, K.; Zhang, B.; Putland, M.; Williamson, D.A. Saliva as a non-invasive specimen for detection of SARS-CoV-2. J. Clin. Microbiol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Azzi, L.; Carcano, G.; Gianfagna, F.; Grossi, P.; Gasperina, D.D.; Genoni, A.; Fasano, M.; Sessa, F.; Tettamanti, L.; Carinci, F.; et al. Saliva is a reliable tool to detect SARS-CoV-2. J. Infect. 2020, S0163–S4453. [Google Scholar] [CrossRef]
- Alizargar, J.; Etemadi, S.M.; Aghamohammadi, M.; Hatefi, S. Saliva samples as an alternative for novel coronavirus (COVID-19) diagnosis. J. Formos. Med. Assoc. 2020, S0929–S6646. [Google Scholar] [CrossRef]
- Sapkota, D.; Thapa, S.B.; Hasséus, B.; Jensen, J.L. Saliva testing for COVID-19? Br. Dent. J. 2020, 228, 658–659. [Google Scholar] [CrossRef]
- Bi, Q.; Wu, Y.; Mei, S.; Ye, C.; Zou, X.; Zhang, Z.; Liu, X.; Wei, L.; Truelove, S.A.; Zhang, T.; et al. Epidemiology and Transmission of COVID-19 in Shenzhen China: Analysis of 391 cases and 1,286 of their close contacts. medRxiv 2020. [Google Scholar] [CrossRef]
- Adhikari, S.P.; Meng, S.; Wu, Y.J.; Mao, Y.P.; Ye, R.X.; Wang, Q.Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polish Dental Association (PTS). COVID-19 a Praca Lekarza Dentysty: Wytyczne PTS Uaktualnione. Available online: https://pts.net.pl/covid-19-a-praca-lekarza-dentysty-wytyczne-pts-uaktualnione/ (accessed on 21 March 2020).
- Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Coronavirus Disease 19 (COVID-19): Implications for Clinical Dental Care. J. Endod. 2020, 46, 584–595. [Google Scholar] [CrossRef] [PubMed]
- European Center for Disease Prevention and Control 2020-risk. Available online: https://www.ecdc.europa.eu/en/current-risk-assessment-novel-coronavirus-situation (accessed on 20 May 2020).
- Vereinigung der Kantonszahnärztinnen und Kantonszahnärzte der Schweiz. Positionspapier. Available online: https://www.sso.ch/fileadmin/upload_sso/5_Newsletter/2020/200323_Positionspapier2_D.pdf?fbclid=IwAR1fLdsyDdAGzWz70NOZb6Q_0hzxEgUyBTVi9ohgL3mKLm8H7FajCsm1BiY (accessed on 26 March 2020).
- American Dental Association (ADA). Return to Work Interim Guidance Toolkit. Available online: https://success.ada.org/~/media/CPS/Files/Open%20Files/ADA_Return_to_Work_Toolkit.pdf (accessed on 15 May 2020).
- Italian Recommendations. Indicazioni Operative Per L’attività Odontoiatrica Durante la Fase 2 Della Pandemia COVID-19. Available online: https://fnomceo-my.sharepoint.com/personal/m_molinari_fnomceo_it/_layouts/15/onedrive.aspx?id=%2Fpersonal%2Fm%5Fmolinari%5Ffnomceo%5Fit%2FDocuments%2Fdocumento%20finale%2Epdf&parent=%2Fpersonal%2Fm%5Fmolinari%5Ffnomceo%5Fit%2FDocuments&originalPath=aHR0cHM6Ly9mbm9tY2VvLW15LnNoYXJlcG9pbnQuY29tLzpiOi9nL3BlcnNvbmFsL21fbW9saW5hcmlfZm5vbWNlb19pdC9FZGVMcF9YdXNHaE1naGNVWTRTeG5wWUJMZEhFcWtxTktORXNMaTJsVjUtZHB3P3J0aW1lPVNSaU8xdnI0MTBn (accessed on 15 May 2020).
- European Federation of Periodontology (EFP). EFP Suggestions for the Management of a Dental Clinic during the Covid-19 Pandemic. Available online: https://www.efp.org/publications/EFP-Infographic-COVID19.pdf (accessed on 15 May 2020).
- ADA Interim Guidance for Management of Emergency and Urgent Dental Care. Available online: https://www.ada.org/~/media/CPS/Files/COVID/ADA_Int_Guidance_Mgmt_Emerg-Urg_Dental_COVID19?utm_source=adaorg&utm_medium=VanityURL&utm_content=interimguidance-flowcharts&utm_campaign=covid-19 (accessed on 15 May 2020).
- Italian Society of Periodontology and Implantology (SIdP). COVID-2019 Norme per L’attività Odontoiatrica. Available online: https://www.sidp.it/media-download/taxtbu3.pdf?v=11032020174011 (accessed on 27 March 2020).
- Scottish Dental Clinical Effectiveness Programme. Emergency Dental Care. Available online: http://www.sdcep.org.uk/wp-content/uploads/2013/03/EDC+Guidance.pdf (accessed on 23 March 2020).
- Wang, X.; Pan, Z.; Cheng, Z. Association between 2019-nCoV transmission and N95 respirator use. J. Hosp. Infect. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, Y.; Hu, T.; Liu, L.; Chen, R.; Guo, Q.; Yang, L.; Cheng, Y.; Huang, J.; Du, L. Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta-analysis. J. Evid. Based Med. 2020. [Google Scholar] [CrossRef]
- Noti, J.D.; Lindsley, W.G.; Blachere, F.M.; Cao, G.; Kashon, M.L.; Thewlis, R.E.; McMillen, C.M.; King, W.P.; Szalajda, J.V.; Beezhold, D.H. Detection of Infectious Influenza Virus in Cough Aerosols Generated in a Simulated Patient Examination Room. Clin. Infect. Dis. 2012, 54, 1569–1577. [Google Scholar] [CrossRef]
- Lee, S.A.; Hwang, D.C.; Li, H.Y.; Tsai, C.F.; Chen, C.W.; Chen, J.K. Particle Size-Selective Assessment of Protection of European Standard FFP Respirators and Surgical Masks against Particles-Tested with Human Subjects. J Healthc Eng 2016, 2016, 8572493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Advice on the Use of Masks in the Community, during Home Care and in Healthcare Settings in the Context of the Novel Coronavirus (COVID-19) Outbreak. 6 April 2020. Available online: https://www.who.int/publications-detail/advice-on-the-use-of-masks-in-the-community-during-home-care-and-in-healthcare-settings-in-the-context-of-the-novel-coronavirus-(2019-ncov)-outbreak (accessed on 20 May 2020).
- Center for Disease Control and Prevention (CDC). Recommended Guidance for Extended Use and Limited Reuse of N95 Filtering Facepiece Respirators in Healthcare Settings. Available online: https://www.cdc.gov/niosh/topics/hcwcontrols/recommendedguidanceextuse.html (accessed on 15 May 2020).
- Magennis, P.; Coulthard, P. FFP3 Masks with Valves Should Be Avoided to Reduce Risk to Patients during Close Interactions when a Clinician Is Unknowingly COVID Positive. Available online: https://www.baoms.org.uk/_userfiles/pages/files/professionals/covid_19/baoms_baos_ppe__avoid_using_ffp3_masks_with_valves_for_close_patient_interactions_may_2020_updated.pdf (accessed on 15 May 2020).
- Lindsley, W.G.; Noti, J.D.; Blachere, F.M.; Szalajda, J.V.; Beezhold, D.H. Efficacy of face shields against cough aerosol droplets from a cough simulator. J. Occup. Environ. Hyg. 2014, 11, 509–518. [Google Scholar] [CrossRef]
- Roberge, R.J. Face shields for infection control: A review. J. Occup. Environ. Hyg. 2016, 13, 235–242. [Google Scholar] [CrossRef]
- Verbeek, J.H.; Rajamaki, B.; Ijaz, S.; Sauni, R.; Toomey, E.; Blackwood, B.; Tikka, C.; Ruotsalainen, J.H.; Kilinc Balci, F.S. Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef]
- Institut, R.K. Haändehygiene in Einrichtungen des Gesundheitswesens. Bundesgesundheitsblatt 2016, 59, 1189–1220. [Google Scholar] [CrossRef]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escombe, A.R.; Oeser, C.C.; Gilman, R.H.; Navincopa, M.; Ticona, E.; Pan, W.; Martínez, C.; Chacaltana, J.; Rodríguez, R.; Moore, D.A.J.; et al. Natural Ventilation for the Prevention of Airborne Contagion. PloS Med. 2007, 4, e68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qian, H.; Zheng, X. Ventilation control for airborne transmission of human exhaled bio-aerosols in buildings. J. Thorac. Dis. 2018, 10, S2295–S2304. [Google Scholar] [CrossRef] [PubMed]
- WHO guideline. Natural Ventilation for Infection Control in Health-Care Settings. Available online: https://apps.who.int/iris/bitstream/handle/10665/44167/9789241547857_eng.pdf?sequence=1 (accessed on 20 May 2020).
- Memarzadeh, F.; Olmsted, R.N.; Bartley, J.M. Applications of ultraviolet germicidal irradiation disinfection in health care facilities: Effective adjunct, but not stand-alone technology. Am. J. Infect. Control. 2010, 38, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Walker, C.M.; Ko, G. Effect of ultraviolet germicidal irradiation on viral aerosols. Environ. Sci. Technol. 2007, 41, 5460–5465. [Google Scholar] [CrossRef] [PubMed]
- Duan, S.M.; Zhao, X.S.; Wen, R.F.; Huang, J.J.; Pi, G.H.; Zhang, S.X.; Han, J.; Bi, S.L.; Ruan, L.; Dong, X.P. Stability of SARS coronavirus in human specimens and environment and its sensitivity to heating and UV irradiation. Biomed. Environ. Sci. 2003, 16, 246–255. [Google Scholar]
- Darnell, M.E.; Subbarao, K.; Feinstone, S.M.; Taylor, D.R. Inactivation of the coronavirus that induces severe acute respiratory syndrome, SARS-CoV. J. Virol. Methods 2004, 121, 85–91. [Google Scholar] [CrossRef]
- Tuladhar, E.; Hazeleger, W.C.; Koopmans, M.; Zwietering, M.H.; Duizer, E.; Beumer, R.R. Reducing viral contamination from finger pads: Handwashing is more effective than alcohol-based hand disinfectants. J. Hosp. Infect. 2015, 90, 226–234. [Google Scholar] [CrossRef]
- Feng, S.; Shen, C.; Xia, N.; Song, W.; Fan, M.; Cowling, B.J. Rational use of face masks in the COVID-19 pandemic. Lancet Respir. Med. 2020. [Google Scholar] [CrossRef]
- Leung, N.H.L.; Chu, D.K.W.; Shiu, E.Y.C.; Chan, K.-H.; McDevitt, J.J.; Hau, B.J.P.; Yen, H.-L.; Li, Y.; Ip, D.K.M.; Peiris, J.S.M.; et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.H.; Yuen, K.-Y. COVID-19 epidemic: Disentangling the re-emerging controversy about medical facemasks from an epidemiological perspective. Int. J. Epidemiol. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ECDC. Using Face masks in the Community; European Centre for Disease Prevention and Control: Solna Municipality, Sweden, 2020. [Google Scholar]
- Prussin, A.J., 2nd; Marr, L.C. Sources of airborne microorganisms in the built environment. Microbiome 2015, 3, 78. [Google Scholar] [CrossRef] [Green Version]
- Eggers, M.; Koburger-Janssen, T.; Eickmann, M.; Zorn, J. In Vitro Bactericidal and Virucidal Efficacy of Povidone-Iodine Gargle/Mouthwash against Respiratory and Oral Tract Pathogens. Infect. Dis. Ther. 2018, 7, 249–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral. Sci. 2020, 12, 9. [Google Scholar] [CrossRef]
- Meiller, T.F.; Silva, A.; Ferreira, S.M.; Jabra-Rizk, M.A.; Kelley, J.I.; DePaola, L.G. Efficacy of Listerine Antiseptic in reducing viral contamination of saliva. J. Clin. Periodontol. 2005, 32, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, D.; Schiff, G.; Echler, G.; Prince, A.; Feller, M.; Briner, W. In vitro virucidal effectiveness of a 0.12%-chlorhexidine gluconate mouthrinse. J. Dent. Res. 1990, 69, 874–876. [Google Scholar] [CrossRef] [PubMed]
- Carrouel, F.; Conte, M.P.; Fisher, J.; Gonçalves, L.S.; Dussart., C.; Llodra, J.C.; Bourgeois., D. COVID-19: A Recommendation to Examine the Effect of Mouthrinses with β-Cyclodextrin Combined with Citrox in Preventing Infection and Progression. J. Clin. Med. 2020, 9, 1126. [Google Scholar] [CrossRef] [Green Version]
- Popkin, D.L.; Zilka, S.; Dimaano, M.; Fujioka, H.; Rackley, C.; Salata, R.; Griffith, A.; Mukherjee, P.K.; Ghannoum, M.A.; Esper, F. Cetylpyridinium Chloride (CPC) Exhibits Potent, Rapid Activity Against Influenza Viruses in vitro and in vivo. Pathog. Immun. 2017, 2, 252–269. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, P.K.; Esper, F.; Buchheit, K.; Arters, K.; Adkins, I.; Ghannoum, M.A.; Salata, R.A. Randomized, double-blind, placebo-controlled clinical trial to assess the safety and effectiveness of a novel dual-action oral topical formulation against upper respiratory infections. BMC Infect. Dis. 2017, 17, 74. [Google Scholar] [CrossRef] [Green Version]
- Jones, S.T.; Cagno, V.; Janeček, M.; Ortiz, D.; Gasilova, N.; Piret, J.; Gasbarri, M.; Constant, D.A.; Han, Y.; Vuković, L.; et al. Modified cyclodextrins as broad-spectrum antivirals. Sci. Adv. 2020, 6, eaax9318. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Wei, Q.; Alvarez, X.; Wang, H.; Du, Y.; Zhu, H.; Jiang, H.; Zhou, J.; Lam, P.; Zhang, L.; et al. Epithelial cells lining salivary gland ducts are early target cells of severe acute respiratory syndrome coronavirus infection in theupper respiratory tracts of rhesus macaques. J. Virol. 2011, 85, 4025–4030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, R.; Cui, B.; Duan, X.; Zhang, P.; Zhou, X.; Yuan, Q. Saliva: Potential diagnostic value and transmission of 2019-nCoV. Int. J. Oral Sci. 2020, 12, 11. [Google Scholar] [CrossRef] [PubMed]
- CED. Code of Ethics for Dentists in the European Union. Available online: https://europeanmovement.eu/wp-content/uploads/2017/05/CED-Code-of-Ethics.pdf (accessed on 23 March 2020).
- Alperovitch, A.; Dreifuss-Netter, F.D.R.; Dickele, A.M.; Gaudray, P.; Coz, P.L.; Rouvillois, P.; Roux, M.; Waquet, P. Ethical Issues Raised by a Possible Influenza Pandemic. Available online: https://www.ccne-ethique.fr/sites/default/files/publications/avis_106_anglais.pdf (accessed on 3 April 2020).
- Centers for Disease Control and Prevention (CDC). How Coronavirus Spreads. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prepare/transmission.html (accessed on 28 March 2020).
- Sokol, D. Virulent epidemics and scope of healthcare workers’ duty of care. Emerg. Infect. Dis. 2006, 12, 1238–1241. [Google Scholar] [CrossRef] [PubMed]
- Sokol, D. Ethics and epidemics. Am. J. Bioeth. 2008, 8, 28–29. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Patient triage recommendations (diagram). COVID-19, coronavirus disease 19; ASAP, as soon as possible.
Figure 1.
Patient triage recommendations (diagram). COVID-19, coronavirus disease 19; ASAP, as soon as possible.

Figure 2.
Measures to prevent health professional infection and nosocomial transmission at dental clinics (diagram). FFP, Filtering Face Piece.
Figure 2.
Measures to prevent health professional infection and nosocomial transmission at dental clinics (diagram). FFP, Filtering Face Piece.

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Gurzawska-Comis, K.; Becker, K.; Brunello, G.; Gurzawska, A.; Schwarz, F. Recommendations for Dental Care during COVID-19 Pandemic. J. Clin. Med. 2020, 9, 1833. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061833
AMA Style
Gurzawska-Comis K, Becker K, Brunello G, Gurzawska A, Schwarz F. Recommendations for Dental Care during COVID-19 Pandemic. Journal of Clinical Medicine. 2020; 9(6):1833. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061833
Chicago/Turabian StyleGurzawska-Comis, Katarzyna, Kathrin Becker, Giulia Brunello, Agata Gurzawska, and Frank Schwarz. 2020. "Recommendations for Dental Care during COVID-19 Pandemic" Journal of Clinical Medicine 9, no. 6: 1833. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061833
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.