Unimanual Intensive Therapy with or without Unaffected Hand Containment in Children with Hemiplegia. A Randomized Controlled Pilot Study

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
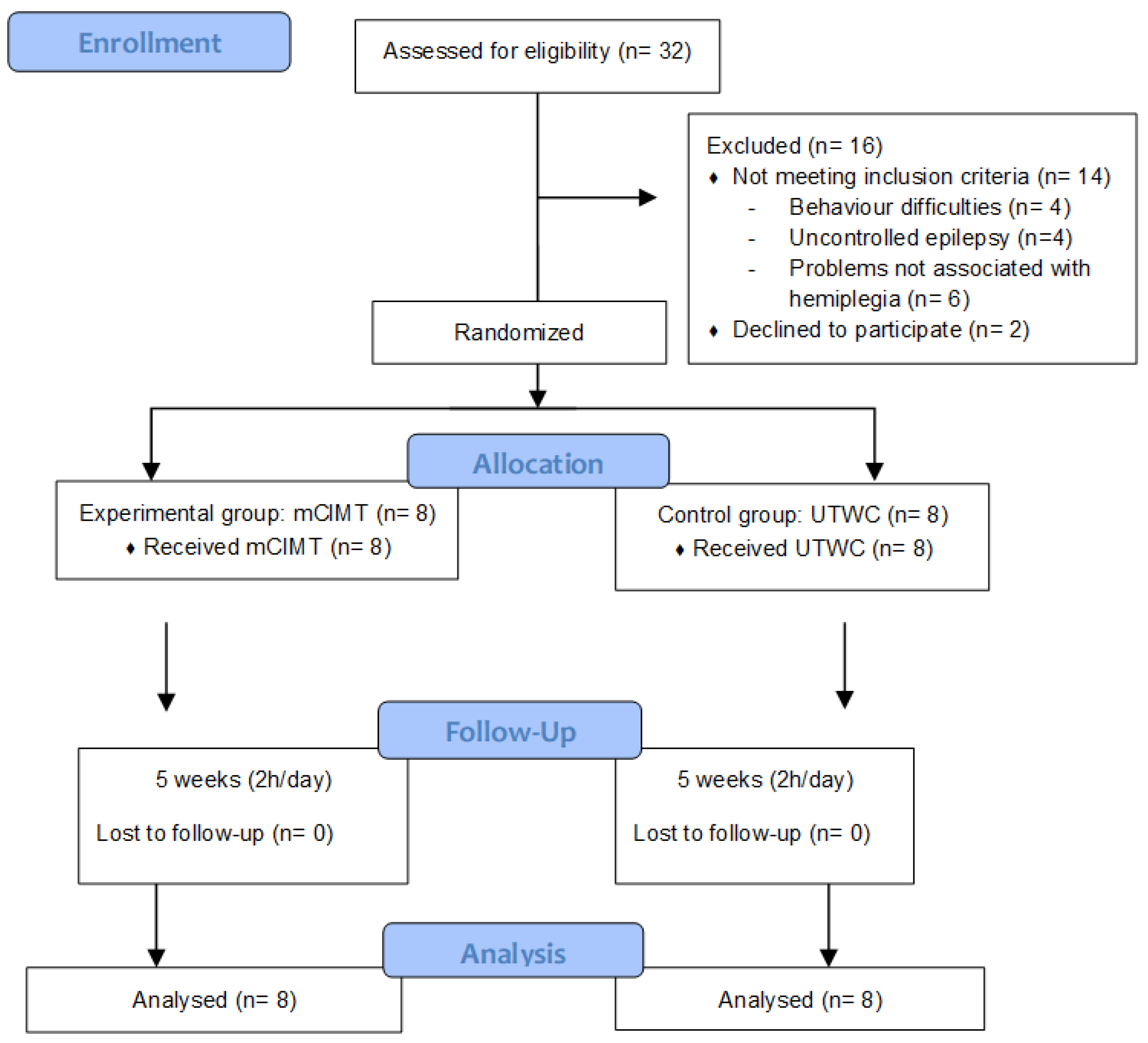
2.1. Study Design
2.2. Participants
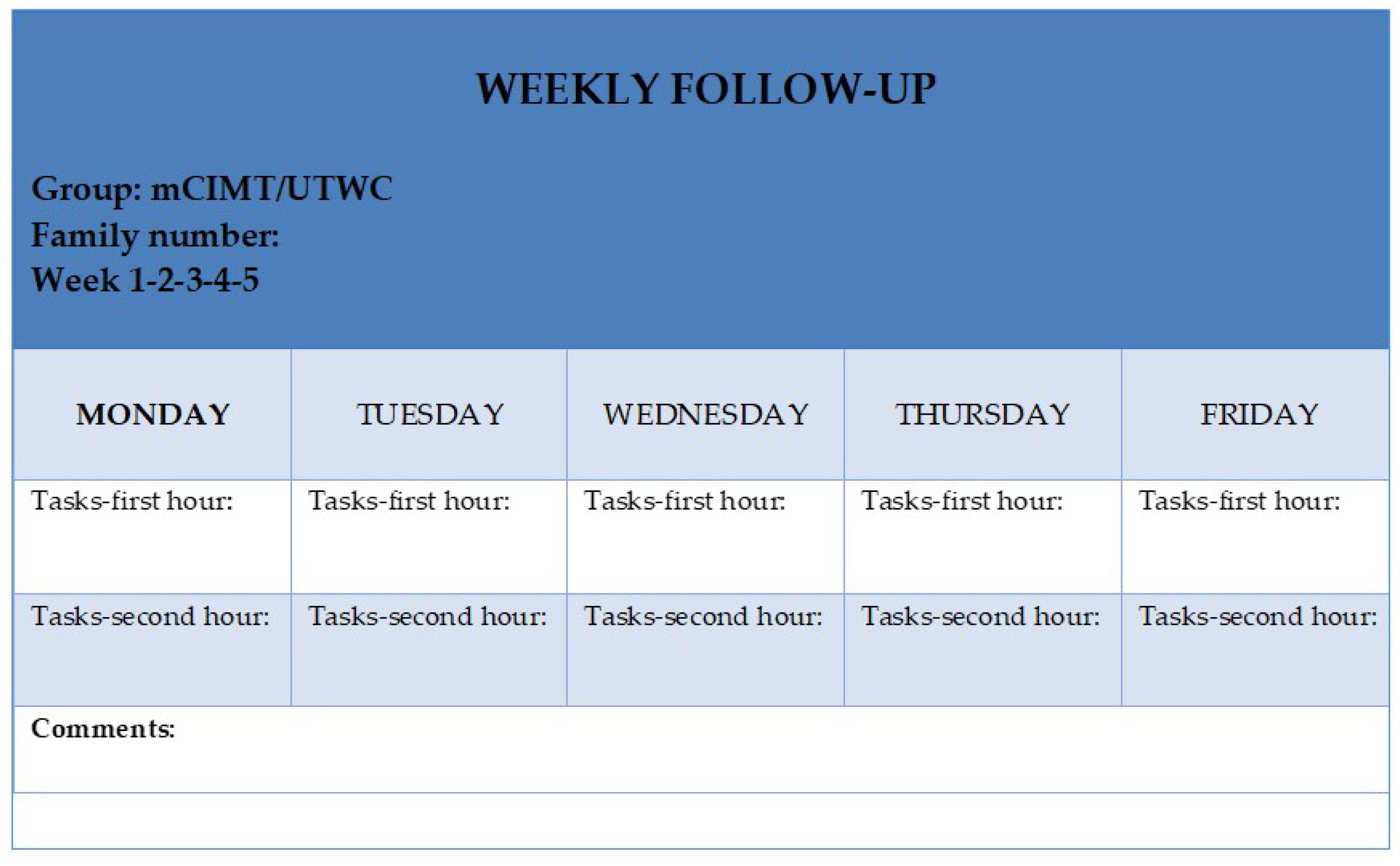
2.3. Procedures and Interventions
2.4. Outcome Measures
2.4.1. Primary Measures
2.4.2. Secondary Measures
2.5. Statistical Analysis
3. Results
3.1. Primary Results
3.2. Secondary Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Intervention Weeks for Both Groups (mCIMT and UTWC) | Designed Tasks for the First Hour (Examples) | Designed Task for the Second Hour (Examples) |
|---|---|---|
| -Week 1- Shoulder Flexion/Shoulder external rotation | 1. Shoe boxes attached on the table. First one, then two and up to three stacked boxes where the parents will place light objects (such as crumpled papers, small boxes or a ball), which the child will first pull and then take. 2. The parents will give the child a small and light ball, which he/she will try to throw higher and higher or towards a target. 3. The parents will throw balloons or bubbles, which the child will try to hit with his/her hand. | 1. The parents will stick plasticine balls on the wall at increasing heights, which the child will try to remove. 2. The parents will put a cardboard or continuous paper stuck on the wall; using finger paint, the child will try to draw a picture or put his/her hand with paint on the paper. 3. The parents will place stickers at different heights on the wall and the child will try to cover them with his/her hand. |
| -Week 2- Elbow extension | 1. The parents will place a rope from one end of a chair to the other and hang different objects (strings, pieces of paper, deflated balloons...). They will ask the child to try and touch these objects from a sitting position on the floor. 2. The parents will place different tools in front of the affected arm on a table, and the child will perform the elbow extension movement to touch them. 3. The parents will place different objects on top and in front of the child, who will try to reach, touch or take them off. | 1. The parents will put pieces of plasticine glued on the table and the child will try to take them off, reproducing the elbow extension movement. 2. The child will glue small empty bottles, with marbles or other elements inside, on the table. Then, he/she will try to knock them down. 3. The child will use the magnet board placed in front of him/her. |
| -Week 3- Forearm supination | 1. The parents will put stickers on the palm of the hand or on the forearm of the affected arm. 2. The parents will place a light object on the palm of the affected hand (for example, a colored pompom) and the child will keep it for a time. 3. The child will comb, play a trumpet or noisemaker, etc. | 1. The child will take things stuck under the table. 2. The child must remove rings towards supination 3. The child will use the affected hand to remove objects stuck on his/her t-shirt (at the level of the abdomen). |
| -Week 4- Wrist extension | 1. The child must roll a ball, bottle. 2. The child must hit a piano or a drum placed vertically. 3. The parents will place an object on the back of the hand and the child will try to raise the back of his/her hand towards the extension while keeping the object from falling. | 1. The child will remove pieces fallen from the wall. 2. The parents will push cardboard boxes or other elements and the child will try to throw them off the table. 3. The child will smash packing paper, balls and/or soft objects with the palm of his/her hand. |
| -Week 5- Grasp | 1. The child will grasp, hold and transfer light and long objects. The child will grasp, hold and transfer heavy, long and rough objects. 2. The child will grasp, hold and transfer rough, light and spherical objects. The child will grasp, hold and transfer rough, heavy and spherical objects. 3. The child will grasp, hold and transfer smooth, light and long objects. The child will grasp, hold and transfer smooth, heavy and long objects. | 1. The child will grasp, hold and transfer smooth, light and spherical objects. The child will grasp, hold and transfer smooth, heavy and spherical objects. 2. The child will grasp, hold and transfer small, light, long and rough objects. The child will grasp, hold and transfer small, heavy, long and rough objects. 3. The child will grasp, hold and transfer small, rough and spherical objects. The child will grasp, hold and transfer small, rough, heavy and spherical objects. |
References
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Dan, B.; Jacobsson, B. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child Neurol. Suppl. 2007, 109, 8–14. [Google Scholar] [PubMed]
- Bax, M.; Goldstein, M.; Rosenbaum, P.; Leviton, A.; Paneth, N.; Dan, B.; Jacobsson, B.; Damiano, D. Executive Committee for the Definition of Cerebral Palsy. Proposed definition and classification of cerebral palsy, April 2005. Dev. Med. Child Neurol. 2005, 47, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.C.; Chen, Y.J.; Chien, C.L.; Kashima, H.; Lin, K.C. Constraint-induced movement therapy as a paradigm of translational research in neurorehabilitation: Reviews and prospects. Am. J. Transl. Res. 2010, 3, 48–60. [Google Scholar]
- Boyd, R.N.; Sakzewski, L.; Ziviani, J.; Abbott, D.F.; Badawy, R.; Gilmore, R.; Provan, K.; Tournier, J.D.; Al Macdonell, R.; Jackson, G.D. INCITE: A randomised trial comparing constraint induced movement therapy and bimanual training in children with congenital hemiplegia. BMC Neurol. 2010, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Ferrel, C.; Bard, C.; Fleury, M. Coordination in childhood: Modifications of visuomotor representations in 6- to 11-year-old children. Exp. Brain Res. 2001, 138, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Hay, L.; Bard, C.; Ferrel, C.; Olivier, I.; Fleury, M. Role of proprioceptive information in movement programming and control in 5 to 11-year old children. Hum. Mov. Sci. 2005, 24, 139–154. [Google Scholar] [CrossRef]
- Thibaut, J.P.; Toussaint, L. Developing motor planning over ages. J. Exp. Child Psychol. 2010, 105, 116–129. [Google Scholar] [CrossRef]
- Casey, B.J.; Galvan, A.; Hare, T.A. Changes in cerebral functional organization during cognitive development. Curr. Opin. Neurobiol. 2005, 15, 239–244. [Google Scholar] [CrossRef]
- Casey, B.J.; Tottenham, N.; Liston, C.; Durston, S. Imaging the developing brain: What have we learned about cognitive development? Trends Cogn. Sci. 2005, 9, 104–110. [Google Scholar] [CrossRef]
- Abd El-Kafy, E.M.; Elshemy, S.A.; Alghamdi, M.S. Effect of constraint-induced therapy on upper limb functions: A randomized control trial. Scand. J. Occup. Ther. 2013, 1–13. [Google Scholar] [CrossRef]
- Mark, V.W.; Taub, E. Constraint-induced movement therapy for chronic stroke hemiparesis and other disabilities. Restor. Neurol. Neurosci. 2004, 22, 317–336. [Google Scholar]
- Morris, D.M.; Taub, E.; Mark, V.W. Constraint-induced movement therapy: Characterizing the intervention protocol. Eur. Medicophys. 2006, 42, 257. [Google Scholar]
- Page, S.J.; Sisto, S.; Johnston, M.V.; Levine, P. Modified constraint-induced therapy after subacute stroke: A preliminary study. Neurorehabil. Neural Repair 2002, 16, 290–295. [Google Scholar]
- Page, S.J.; Levine, P.; Leonard, A.C. Modified constraint-induced therapy in acute stroke: A randomized controlled pilot study. Neurorehabil. Neural Repair 2005, 19, 27–32. [Google Scholar] [PubMed]
- Charles, J.R.; Wolf, S.L.; Schneider, J.A.; Gordon, A.M. Efficacy of a child-friendly form of constraint-induced movement therapy in hemiplegic cerebral palsy: A randomized control trial. Dev. Med. Child Neurol. 2006, 48, 635. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.L.; Kang, L.J.; Hong, W.H.; Chen, F.C.; Chen, H.C.; Wu, C.Y. Effect of therapist-based constraint-induced therapy at home on motor control, motor performance and daily function in children with cerebral palsy: A randomized controlled study. Clin. Rehabil. 2012, 27, 236–245. [Google Scholar]
- Chen, H.C.; Chen, C.L.; Kang, L.J.; Wu, C.Y.; Chen, F.C.; Hong, W.H. Improvement of upper extremity motor control and function after home-based constraint induced therapy in children with unilateral cerebral palsy: Immediate and long-term effects. Arch. Phys. Med. Rehabil. 2014, 95, 1423–1432. [Google Scholar] [CrossRef]
- Choudhary, A.; Gulati, S.; Kabra, M.; Singh, U.P.; Sankhyan, N.; Pandey, R.M.; Kalra, V. Efficacy of modified constraint induced movement therapy in improving upper limb function in children with hemiplegic cerebral palsy: A randomized controlled trial. Brain Dev. 2013, 35, 870–876. [Google Scholar]
- Miltner, W.H.; Bauder, H.; Sommer, M.; Dettmers, C.; Taub, E. Effects of constraint-induced movement therapy on patients with chronic motor deficits after stroke: A replication. Stroke 1999, 30, 586–592. [Google Scholar]
- Brogårdh, C.; Sjölund, B.H. Constraint-induced movement therapy in patients with stroke: A pilot study on effects of small group training and of extended mitt use. Clin. Rehabil. 2006, 20, 218–227. [Google Scholar]
- Eliasson, A.C.; Krumlinde-sundholm, L.; Shaw, K.; Wang, C. Effects of constraint-induced movement therapy in young children with hemiplegic cerebral palsy: An adapted model. Dev. Med. Child Neurol. 2005, 47, 266–275. [Google Scholar] [CrossRef]
- Novak, I.; Honan, I. Effectiveness of paediatric occupational therapy for children with disabilities: A systematic review. Aust. Occup. Ther. J. 2019, 66, 258–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taub, E.; Griffin, A.; Nick, J.; Gammons, K.; Uswatte, G.; Law, C.R. Pediatric CI therapy for stroke-induced hemiparesis in young children. Dev. Neurorehabil. 2007, 10, 3–18. [Google Scholar] [CrossRef]
- Taub, E.; Griffin, A.; Uswatte, G.; Gammons, K.; Nick, J.; Law, C.R. Treatment of congenital hemiparesis with pediatric constraint-induced movement therapy. J. Child Neurol. 2011, 26, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Dromerick, A.W.; Edwards, D.F.; Hahn, M. Does the application of constraint-induced movement therapy during acute rehabilitation reduce arm impairment after ischemic stroke? Stroke 2000, 31, 2984–2988. [Google Scholar] [CrossRef] [Green Version]
- Taub, E.; Uswatte, G.; King, D.K.; Morris, D.; Crago, J.E.; Chatterjee, A. A placebo-controlled trial of constraint-induced movement therapy for upper extremity after stroke. Stroke 2006, 37, 1045–1049. [Google Scholar] [CrossRef] [Green Version]
- Ostendorf, C.G.; Wolf, S.L. Effect of forced use of the upper extremity of a hemiplegic patient on changes in function: A single-case design. Phys. Ther. 1981, 61, 1022–10288. [Google Scholar] [CrossRef]
- Wolf, S.L.; Winstein, C.J.; Miller, P.J.; Taub, E.; Uswatte, G.; Morris, D.; Giuliani, C.; Light, K.E.; Larsen, D.N. Effect of constraint-induced movement therapy on upper extremity function 3 to 9 months after stroke: The EXCITE randomized clinical trial. JAMA 2006, 296, 2095–2104. [Google Scholar] [CrossRef]
- Van Der Lee, J.H.; Wagenaar, R.C.; Lankhorst, G.J.; Vogelaar, T.W.; Devillé, W.L.; Bouter, L.M. Forced use of the upper extremity in chronic stroke patients: Results from a single-blind randomized clinical trial. Stroke 1999, 30, 2369–2375. [Google Scholar] [CrossRef]
- Ferre, C.L.; Gordon, A.M. Coaction of individual and environmental factors: A review of intensive therapy paradigms for children with unilateral spastic cerebral palsy. Dev. Med. Child Neurol. 2017, 59, 1139–1145. [Google Scholar] [CrossRef] [Green Version]
- Hadders-Algra, M.; Boxum, A.G.; Hielkema, T.; Hamer, E.G. Effect of early intervention in infants at very high risk of cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2016, 59, 246–258. [Google Scholar]
- Davids, J.R.; Peace, L.C.; Wagner, L.V.; Gidewall, M.A.; Blackhurst, D.W.; Roberson, W.M. Validation of the Shriners Hospital for Children Upper Extremity Evaluation (SHUEE) for children with hemiplegic cerebral palsy. J. Bone Joint Surg. Am. 2006, 88, 326–833. [Google Scholar] [CrossRef]
- De Matteo, C.; Law, M.; Russell, D.; Pollock, N.; Rosenbaum, P.; Walter, S. The reliability and validity of Quality of Upper Extremity Skills Test. Phys. Occup. Ther. Pediatrics 1993, 13, 1–18. [Google Scholar] [CrossRef]
- Hickey, A.; Ziviani, J. A Review of the Quality of Upper Extremities Skills Test (QUEST) for Children with Cerebral Palsy. Phys. Occup. Ther. Pediatrics 1998, 18, 123–135. [Google Scholar] [CrossRef]
- Hoare, B.J.; Wasiak, J.; Imms, C.; Carey, L. Constraint-induced movement therapy in the treatment of the upper limb in children with hemiplegic cerebral palsy. Cochrane Database Syst. Rev. 2007, 2, CD004149. [Google Scholar] [CrossRef]
- Simon-Martinez, C.; Mailleux, L.; Hoskens, J.; Ortibus, E.; Jaspers, E.; Wenderoth, N.; Sgandurra, G.; Cioni, G.; Molenaers, G.; Klingels, K.; et al. Randomized controlled trial combining constraint-induced movement therapy and action-observation training in unilateral cerebral palsy: Clinical effects and influencing factors of treatment response. Ther. Adv. Neurol. Disord. 2020, 13. [Google Scholar] [CrossRef]
- Adler, C.; Berweck, S.; Lidzba, K.; Becher, T.; Staudt, M. Mirror movements in unilateral spastic cerebral palsy: Specific negative impact on bimanual activities of daily living. Eur. J. Paediatric Neurol. 2015, 19, 504–509. [Google Scholar] [CrossRef] [PubMed]
- Steenbergen, B.; Charles, J.; Gordon, A.M. Fingertip force control during bimanual object lifting in hemiplegic cerebral palsy. Exp. Brain Res. 2008, 186, 191–201. [Google Scholar] [CrossRef] [Green Version]
- Forssberg, H.; Eliasson, A.C.; Redon-Zouitenn, C.; Mercuri, E.; Dubowitz, L. Impaired grip-lift synergy in children with unilateral brain lesions. Brain 1999, 122, 1157–1168. [Google Scholar] [CrossRef]
- Krajenbrink, H.; Crichton, A.; Steenbergen, B.; Hoare, B. The development of anticipatory action planning in children with unilateral cerebral palsy. Res. Dev. Disabil. 2019, 85, 163–171. [Google Scholar] [CrossRef] [Green Version]
- Ferre, C.L.; Brandão, M.B.; Hung, Y.C.; Carmel, J.B.; Gordon, A.M. Feasibility of caregiver-directed home-based hand-arm bimanual intensive training: A brief report. Dev. Neurorehabilit. 2014, 18, 69–74. [Google Scholar]



| VARIABLES | Total (n = 16) | mCIMT (n = 8) | UTWC (n = 8) | p-Value |
|---|---|---|---|---|
| AGE, years (SD) | 5.54 (1.55) | 5.63 (1.21) | 5.50 (1.12) | 0.78 |
| SEX | ||||
| Male, n. (%) | 8 (50) | 4 (50) | 4 (50) | 1.00 |
| Female, n. (%) | 8 (50) | 4 (50) | 4 (50) | |
| HEMIPLEGIA | ||||
| Left, n. (%) | 10 (62.50) | 5 (62.50) | 5 (62.50) | - |
| Right, n. (%) | 6 (37.50) | 3 (37.50) | 3 (37.50) | |
| MACS score (I–V) | ||||
| II, n. (%) | 9 (56.25) | 6 (75.00) | 3 (37.50) | - |
| III, n. (%) | 7 (43.75) | 2 (25.00) | 5 (62.50) | |
| SHUEE Evaluation % median. (IQR) | ||||
| Spontaneous Use Analysis | 64.33 (42.22, 95.55) | 70.00 (42.22, 95.55) | 63.72 (44.44, 88.44) | 0.64 |
| Dynamic Positional Analysis | 76.39 (45.83, 88.89) | 77.78 (45.83, 88.89) | 74.39 (48.00, 78.88) | 1.20 |
| Grasp and Release | 64 (50.00, 100.00) | 58.34 (50.00, 100.00) | 64 (50.00, 100.00) | 1.48 |
| QUEST Scale % median. (IQR) | ||||
| Movement Quality Total score | 74.15 (56.24, 85,14) | 74.15 (56.24, 85.14) | 74.15 (60.00, 83.17) | 1.76 |
| Dissociated Movements | 57.82 (49.45, 85.94) | 59.38 (50.00, 82.82) | 57.82 (49.45, 85.94) | 1.92 |
| Grasp | 66.67 (25.96, 88.88) | 62.97 (25.96, 88.88) | 66.67 (25.16, 85.18) | 1.92 |
| Weight Bearing | 77.78 (37.04, 100.00) | 87 (72.00, 98.00) | 94 (76.00, 98.00) | 0.44 |
| Protective Extension | 80.56 (75.00, 100.00) | 80.56 (75.00, 100.00) | 80 (75.00, 90.00) | 1.16 |
| SHUEE Evaluation | Total Sample (n = 16) | m-CIMT (n = 8) | UTWC (n = 8) | p-Value |
|---|---|---|---|---|
| SUA Week 0 Week 5 Percent of improvement | 64.33 (42.22, 95.55) 84.44 (44.44, 97.78) 34.77 (0.00, 110.42) | 70 (42.22, 95.55) 88.87 (84.44, 97.78) 31.65 (2.33, 110.42) | 63.72 (44.44, 88.44) 63.72 (44.44, 88.44) 0.00 (0.00, 0.00) | 0.64 <0.001 <0.001 |
| DPA Week 0 Week 5 Percent of improvement | 76.39 (45.83, 88.89) 79.71 (48.00, 97.22) 2.38 (0.00, 78,36) | 77.78 (45.83, 88.89) 88.20 (65.27, 97.22) 15.17 (4.77, 78.36) | 74.39 (48.00, 78.88) 74.40 (48.00, 78.88) 0.00 (0.00, 0.00) | 1.20 <0.001 <0.001 |
| GR Week 0 Week 5 Percent of improvement | 64 (50.00, 100.00) 83.33 (50.00, 100.00) 0.00 (0.00, 100.00) | 58.34 (50.00,100.00) 91.67 (66.67, 100.00) 41.67 (0.00, 100.00) | 64 (50.00,100.00) 64.40 (50.00, 100.00) 0.00 (0.00, 0.00) | 1.48 0.08 0.008 |
| QUEST Scale | Total Sample (n = 16) | m-CIMT (n = 8) | UTWC (n = 8) | p Value |
|---|---|---|---|---|
| MQ Week 0 Week 5 Percent of improvement | 74.15 (56.24, 85,14) 83.17 (60.00, 96.66) 9.09 (0.00, 50.39) | 74.15 (56.24, 85.14) 94.06 (96.66, 83.11) 24.21 (13.44, 50.39) | 74.15 (60.00, 83.17) 75.92 (60.00, 83.17) 1.34 (0.00, 4.75) | 1.76 <0.001 0.002 |
| DM Week 0 Week 5 Percent of improvement | 57.82 (49.45, 85.94) 83.60 (53.12, 100.00) 8.60 (0.00, 81.24) | 59.38 (50.00, 82.82) 89.84 (78.12, 100.00) 38.68 (9.42, 81.24) | 57.82 (49.45, 85.94) 59.53 (53.12, 85.94) 1.40 (0.00, 7.77) | 1.92 <0.001 0.002 |
| G Week 0 Week 5 Percent of improvement | 66.67 (25.96, 88.88) 77.78 (37.04, 100.00) 18.15 (0.00, 156.78) | 62.97 (88.88, 25.96) 96.30 (66.66, 100.00) 38.92 (8.35, 156.78) | 66.67 (25.16, 85.18) 72.22 (37.04, 88.88) 4.67 (0.00, 42.68) | 1.92 <0.001 0.01 |
| WB Week 0 Week 5 Percent of improvement | 77.78 (37.04, 100.00) 96.00 (76.00, 100.00) 1.02 (0.00, 36.11) | 87.00 (72.00, 98.00) 99.00 (96.00, 100.00) 12.68 (2.04, 36.11) | 94.00 (76.00, 98.00) 94.00 (76.00, 98.00) 0.00 (0.00, 0.00) | 0.44 <0.001 <0.001 |
| PE Week 0 Week 5 Percent of improvement | 80.56 (75.00, 100.00) 90.83 (75.00, 100.00) 0.00 (0.00, 25.92) | 80.56 (75.00, 100.00) 94.44 (91.66, 100.00) 17.25 (0.00, 25.92) | 80.00 (75.00, 90.00) 80,62 (75.41, 90.00) 0.00 (0.00, 0.00) | 1.16 <0.001 0.002 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palomo-Carrión, R.; Pinero-Pinto, E.; Ando-LaFuente, S.; Ferri-Morales, A.; Bravo-Esteban, E.; Romay-Barrero, H. Unimanual Intensive Therapy with or without Unaffected Hand Containment in Children with Hemiplegia. A Randomized Controlled Pilot Study. J. Clin. Med. 2020, 9, 2992. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092992
Palomo-Carrión R, Pinero-Pinto E, Ando-LaFuente S, Ferri-Morales A, Bravo-Esteban E, Romay-Barrero H. Unimanual Intensive Therapy with or without Unaffected Hand Containment in Children with Hemiplegia. A Randomized Controlled Pilot Study. Journal of Clinical Medicine. 2020; 9(9):2992. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092992
Chicago/Turabian StylePalomo-Carrión, Rocío, Elena Pinero-Pinto, Sara Ando-LaFuente, Asunción Ferri-Morales, Elisabeth Bravo-Esteban, and Helena Romay-Barrero. 2020. "Unimanual Intensive Therapy with or without Unaffected Hand Containment in Children with Hemiplegia. A Randomized Controlled Pilot Study" Journal of Clinical Medicine 9, no. 9: 2992. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092992