SARS-CoV-2 and Oral Manifestation: An Observational, Human Study

 ,
, 
 ,
,  ,
,  ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design and Sample Selection
2.2. Ethical Consideration
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Questionnaire
| 1. Age | |
| 2. Sex | Male |
| Female | |
| 3. Place of origin | |
| 4. How many teeth do you have in your mouth? | >20 teeth |
| 10–19 teeth | |
| 1–9 teeth | |
| totally edentulous patient | |
| 5. Are you a smoker? | Yes |
| No | |
| 6. When did you last go to the dentist? | performed within 6 months |
| performed within 1 year | |
| more than a year since the last visit | |
| 7. How many times did you brush your teeth in a day before being hospitalized? | times/after meals daily |
| times daily | |
| 1 time daily | |
| Never | |
| 8. Did you use interdental brushes? | Yes |
| No | |
| 9. If yes, how often weekly? | Yes, but it has been treated |
| Yes, but I neglect the problem | |
| No, I wasn’t told | |
| I don’t know | |
| 10. When brushing your teeth, do your gums bleed? | Yes |
| No | |
| 11. Did you clean your tongue before hospitalization? | Yes |
| No | |
| 12. Did the dentist ever tell you that you have gum problems, gum infections or inflammation? | Yes, but it has been treated |
| Yes, but I neglect the problem | |
| No, I wasn’t told | |
| I don’t know | |
| 13. Did the dentist extract your teeth because they had high mobility? | Yes |
| No | |
| 14. Are you wearing a fixed prosthesis? | Yes |
| 15. Are you wearing a removable prosthesis? | Yes, total |
| Yes, partial | |
| Yes, both total and partial | |
| No | |
| 16. Has anyone in your family of origin (father, mother, siblings, uncles, …) had gum problems such as periodontitis? | Yes |
| No | |
| I don’t know | |
| 17. Do you suffer from xerostomia (dry mouth)? | Yes |
| No | |
| 18. Which home oral hygiene aids do you use now that you are hospitalized? | toothbrush + toothpaste + floss |
| prosthesis brush + toothpaste + tablets | |
| toothbrush + toothpaste | |
| nothing | |
| 19. How many times do you brush your teeth a day, now that you are hospitalized? | 1230 |
| 20. Do you still clean your tongue now? | Yes |
| No | |
| 21. Do you currently bleed from your gums while cleaning your teeth? | Yes |
| No | |
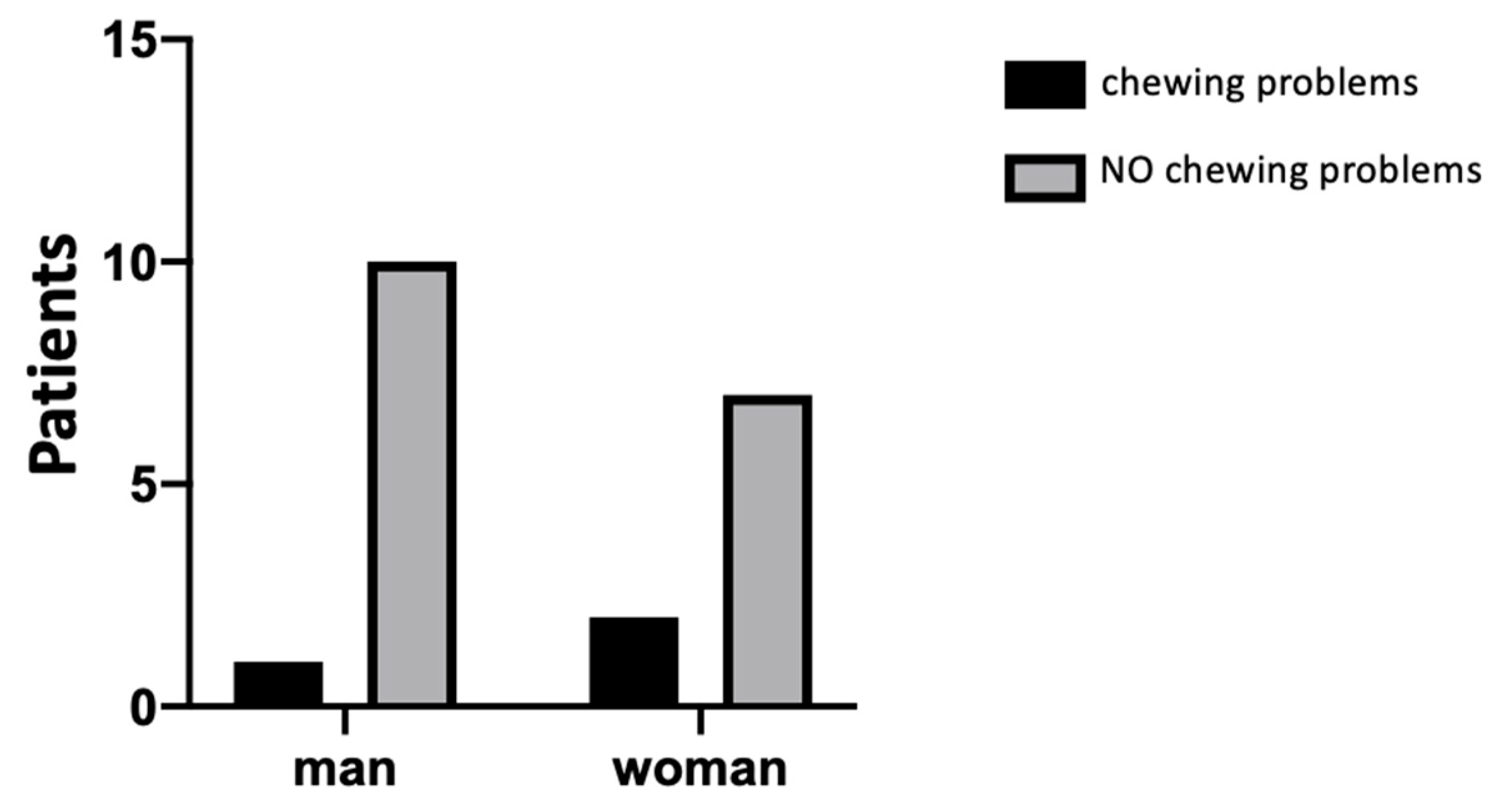
| 22. Did you have any chewing problems during the period of illness (COVID-19)? | Yes |
| No | |
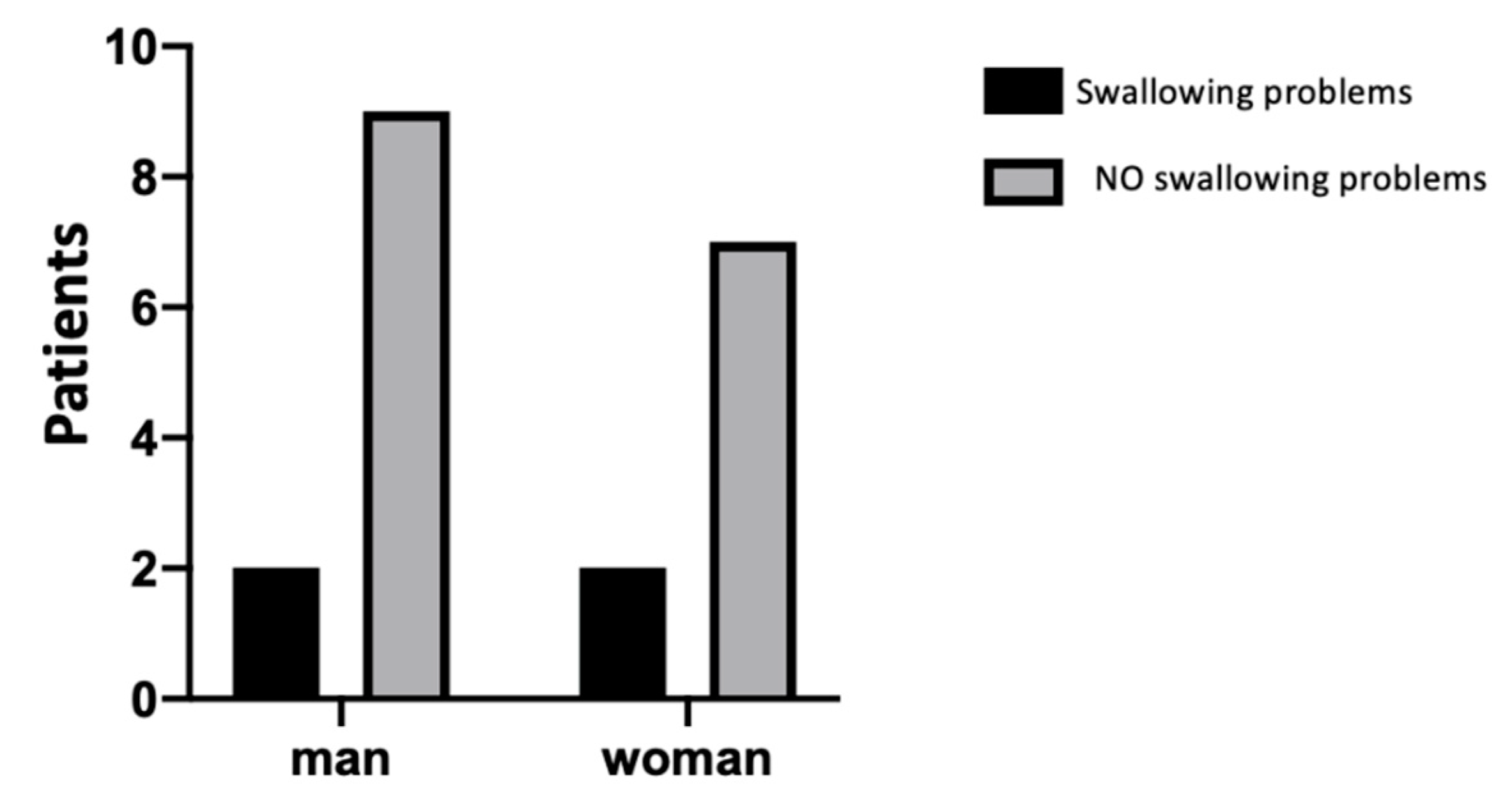
| 23. Did you have any swallowing problems during the period of illness (COVID-19)? | Yes |
| No | |
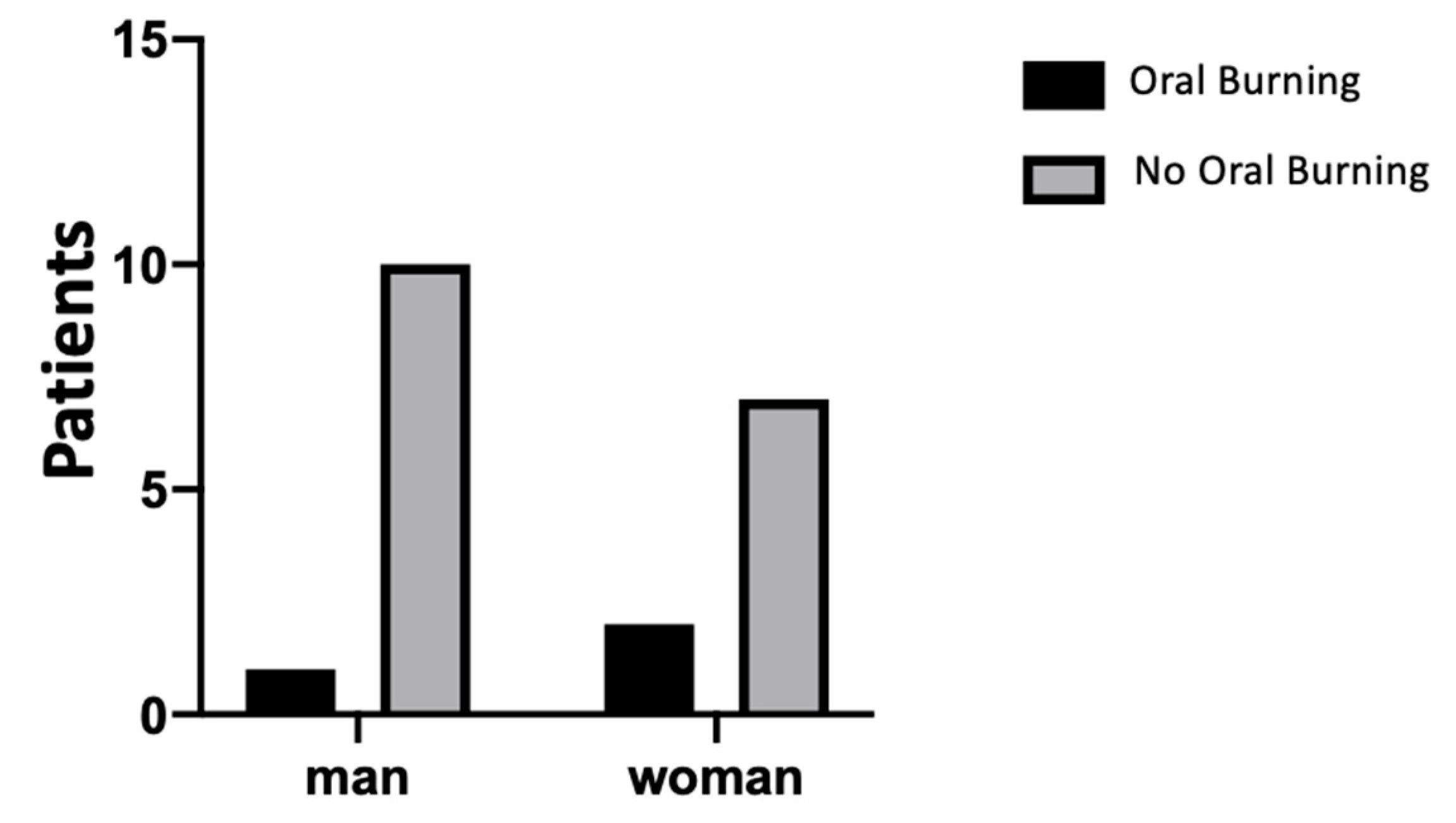
| 24. Did you experience a burning sensation in your mouth during the period of your illness (COVID-19)? | Yes |
| No | |
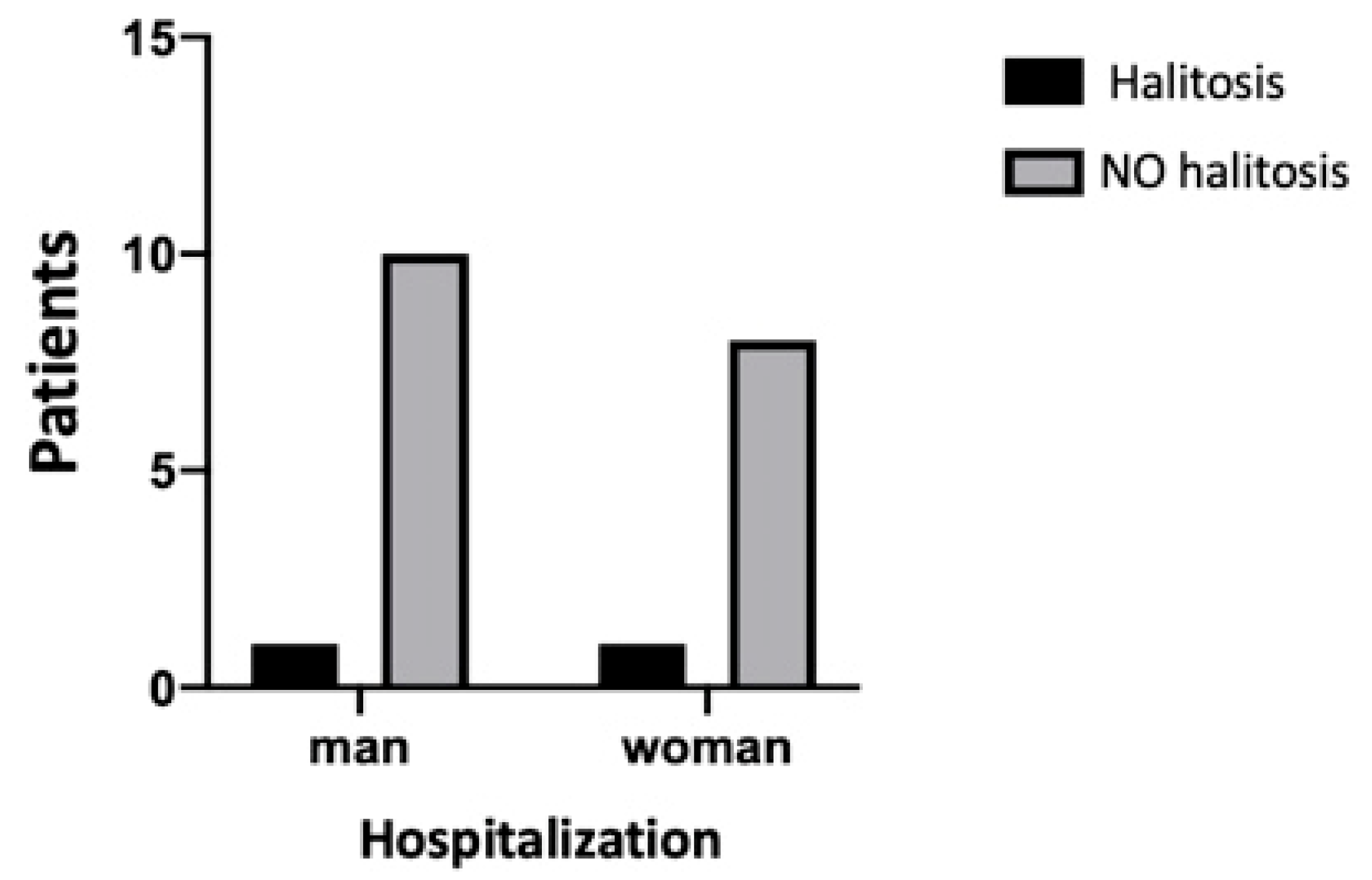
| 25. Did you experience halitosis during the period of your illness (COVID-19)? | Yes |
| No | |
| 26. During the period of your illness (COVID-19) did you have tooth problems/pain? | Yes |
| No | |
| 27. During the period of the disease (COVID-19) did you have any taste alterations? | Yes |
| No | |
| 28. Did you suffer from xerostomia during the period of your illness (COVID-19)? | Yes |
| No | |
| 29. Do you suffer from diabetes? | Yes |
| No | |
| 30. Do you suffer from cardiovascular disease? | Yes |
| No | |
| 31. Do you suffer from senile dementia? | Yes |
| No | |
| 32. Did you experience any other oral problems during hospitalization? | Yes |
| No |
Appendix B. Statistical Results











References
- Andersen, K.G.; Rambaut, A.; Lipkin, W.I.; Holmes, E.C.; Garry, R.F. The proximal origin of SARS-CoV-2. Nat. Med. 2020, 26, 450–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corman, V.M.; Muth, D.; Niemeyer, D.; Drosten, C. Hosts and Sources of Endemic Human Coronaviruses. Adv. Virus Res. 2018, 100, 163–188. [Google Scholar] [PubMed]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Grunewald, M.; Perlman, S. Coronaviruses: An Updated Overview of Their Replication and Pathogenesis. Methods Mol. Biol. Clifton NJ 2020, 2203, 1–29. [Google Scholar]
- Decaro, N.; Lorusso, A. Novel human coronavirus (SARS-CoV-2): A lesson from animal coronaviruses. Vet. Microbiol. 2020, 244, 108693. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Wunderink, R.G. MERS, SARS and other coronaviruses as causes of pneumonia. Respirol. Carlton VIC 2018, 23, 130–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet Lond. Engl. 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet Lond. Engl. 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Epidemiology Working Group for NCIP Epidemic Response, Chinese Center for Disease Control and Prevention. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi Zhonghua Liuxingbingxue Zazhi 2020, 41, 145–151. [Google Scholar]
- To, K.K.-W.; Tsang, O.T.-Y.; Yip, C.C.-Y.; Chan, K.-H.; Wu, T.-C.; Chan, J.M.-C.; Leung, W.-S.; Chik, T.S.-H.; Choi, C.Y.-C.; Kandamby, D.H.; et al. Consistent Detection of 2019 Novel Coronavirus in Saliva. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 841–843. [Google Scholar] [CrossRef] [Green Version]
- ADA Council on Scientific Affairs; ADA Council on Dental Practice. Infection control recommendations for the dental office and the dental laboratory. J. Am. Dent. Assoc. 1996, 127, 672–680. [Google Scholar] [CrossRef] [PubMed]
- Leung, R.L.; Schonfeld, S.E. Gypsum casts as a potential source of microbial cross-contamination. J. Prosthet. Dent. 1983, 49, 210–211. [Google Scholar] [CrossRef]
- Sinjari, B.; Rexhepi, I.; Santilli, M.; D’Addazio, G.; Chiacchiaretta, P.; Di Carlo, P.; Caputi, S. The Impact of COVID-19 Related Lockdown on Dental Practice in Central Italy-Outcomes of A Survey. Int. J. Environ. Res. Public. Health 2020, 17, 5780. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Zhang, T.; Zhao, D.; Haapasalo, M.; Shen, Y. Characteristics of Endodontic Emergencies during Coronavirus Disease 2019 Outbreak in Wuhan. J. Endod. 2020, 46, 730–735. [Google Scholar] [CrossRef]
- Wang, D.; Yin, Y.; Hu, C.; Liu, X.; Zhang, X.; Zhou, S.; Jian, M.; Xu, H.; Prowle, J.; Hu, B.; et al. Clinical course and outcome of 107 patients infected with the novel coronavirus, SARS-CoV-2, discharged from two hospitals in Wuhan, China. Crit. Care Lond. Engl. 2020, 24, 188. [Google Scholar] [CrossRef]
- Vinayachandran, D.; Balasubramanian, S. Is gustatory impairment the first report of an oral manifestation in COVID-19? Oral Dis. 2020. [Google Scholar] [CrossRef]
- Freni, F.; Meduri, A.; Gazia, F.; Nicastro, V.; Galletti, C.; Aragona, P.; Galletti, C.; Galletti, B.; Galletti, F. Symptomatology in head and neck district in coronavirus disease (COVID-19): A possible neuroinvasive action of SARS-CoV-2. Am. J. Otolaryngol. 2020, 41, 102612. [Google Scholar] [CrossRef]
- Saniasiaya, J. Xerostomia and COVID-19: Unleashing Pandora’s Box. Ear Nose Throat J. 2020. [Google Scholar] [CrossRef]
- Martín Carreras-Presas, C.; Amaro Sánchez, J.; López-Sánchez, A.F.; Jané-Salas, E.; Somacarrera Pérez, M.L. Oral vesiculobullous lesions associated with SARS-CoV-2 infection. Oral Dis. 2020. [Google Scholar] [CrossRef]
- Chaux-Bodard, A.-G.; Deneuve, S.; Desoutter, A. Oral manifestation of Covid-19 as an inaugural symptom? J. Oral Med. Oral Surg. 2020, 26, 18. [Google Scholar] [CrossRef]
- Soares, C.-D.; Carvalho, R.-A.; Carvalho, K.-A.; Carvalho, M.-G.; Almeida, O.-P. Letter to Editor: Oral lesions in a patient with Covid-19. Med. Oral Patol. Oral Cirugia Bucal 2020, 25, e563–e564. [Google Scholar]
- Badran, Z.; Gaudin, A.; Struillou, X.; Amador, G.; Soueidan, A. Periodontal pockets: A potential reservoir for SARS-CoV-2? Med. Hypotheses 2020, 143, 109907. [Google Scholar] [CrossRef] [PubMed]
- Metagenome of SARS-Cov2 Patients in Shenzhen with Travel to Wuhan Shows a Wide Range of Species—Lautropia, Cutibacterium, Haemophilus Being Most Abundant—and Campylobacter Explaining Diarrhea. Available online: https://www.researchgate.net/publication/340152514_Metagenome_of_SARS-Cov2_patients_in_Shenzhen_with_travel_to_Wuhan_shows_a_wide_range_of_species_-_Lautropia_Cutibacterium_Haemophilus_being_most_abundant_-_and_Campylobacter_explaining_diarrhea (accessed on 15 September 2020).
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, H.; Zhong, L.; Deng, J.; Peng, J.; Dan, H.; Zeng, X.; Li, T.; Chen, Q. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int. J. Oral Sci. 2020, 12, 8. [Google Scholar] [CrossRef]
- Dziedzic, A.; Wojtyczka, R. The impact of coronavirus infectious disease 19 (COVID-19) on oral health. Oral Dis. 2020. [Google Scholar] [CrossRef]
- Amorim Dos Santos, J.; Normando, A.G.C.; Carvalho da Silva, R.L.; De Paula, R.M.; Cembranel, A.C.; Santos-Silva, A.R.; Guerra, E.N.S. Oral mucosal lesions in a COVID-19 patient: New signs or secondary manifestations? Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2020, 97, 326–328. [Google Scholar]
- Pedrosa, M.; Sipert, C.R.; Nogueira, F.N. Salivary Glands, Saliva and Oral Presentations in COVID-19 infection. SciELO 2020. [Google Scholar] [CrossRef]
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y.; et al. Extrapulmonary manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef]
- Lenti, M.V.; Borrelli de Andreis, F.; Pellegrino, I.; Klersy, C.; Merli, S.; Miceli, E.; Aronico, N.; Mengoli, C.; Di Stefano, M.; Cococcia, S.; et al. Impact of COVID-19 on liver function: Results from an internal medicine unit in Northern Italy. Intern. Emerg. Med. 2020. [Google Scholar] [CrossRef]
- Herrera, D.; Serrano, J.; Roldán, S.; Sanz, M. Is the oral cavity relevant in SARS-CoV-2 pandemic? Clin. Oral Investig. 2020, 24, 2925–2930. [Google Scholar] [CrossRef]
- Fu, L.; Wang, B.; Yuan, T.; Chen, X.; Ao, Y.; Fitzpatrick, T.; Li, P.; Zhou, Y.; Lin, Y.-F.; Duan, Q.; et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J. Infect. 2020, 80, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.C.K.; Lexomboon, D.; Sandborgh-Englund, G.; Haasum, Y.; Johnell, K. Medications That Cause Dry Mouth as an Adverse Effect in Older People: A Systematic Review and Metaanalysis. J. Am. Geriatr. Soc. 2018, 66, 76–84. [Google Scholar] [CrossRef] [PubMed]
- López-Pintor, R.M.; Casañas, E.; González-Serrano, J.; Serrano, J.; Ramírez, L.; de Arriba, L.; Hernández, G. Xerostomia, Hyposalivation, and Salivary Flow in Diabetes Patients. J. Diabetes Res. 2016, 2016, 4372852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinjari, B.; Feragalli, B.; Cornelli, U.; Belcaro, G.; Vitacolonna, E.; Santilli, M.; Rexhepi, I.; D’Addazio, G.; Zuccari, F.; Caputi, S. Artificial Saliva in Diabetic Xerostomia (ASDIX): Double Blind Trial of Aldiamed® Versus Placebo. J. Clin. Med. 2020, 9, 2196. [Google Scholar] [CrossRef]
- Xu, J.; Li, Y.; Gan, F.; Du, Y.; Yao, Y. Salivary Glands: Potential Reservoirs for COVID-19 Asymptomatic Infection. J. Dent. Res. 2020, 99, 989. [Google Scholar] [CrossRef] [Green Version]
- Carrillo-Larco, R.M.; Altez-Fernandez, C. Anosmia and dysgeusia in COVID-19: A systematic review. Wellcome Open Res. 2020, 5, 94. [Google Scholar] [CrossRef]
- Lozada-Nur, F.; Chainani-Wu, N.; Fortuna, G.; Sroussi, H. Dysgeusia in COVID-19: Possible Mechanisms and Implications. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; The Northwell COVID-19 Research Consortium; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- World Health Organization. Smoking and COVID-19: Scientific Brief, 30 June 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Shibata, S.; Arima, H.; Asayama, K.; Hoshide, S.; Ichihara, A.; Ishimitsu, T.; Kario, K.; Kishi, T.; Mogi, M.; Nishiyama, A.; et al. Hypertension and related diseases in the era of COVID-19: A report from the Japanese Society of Hypertension Task Force on COVID-19. Hypertens. Res. 2020, 43, 1028–1046. [Google Scholar] [CrossRef]
- Schiffrin, E.L.; Flack, J.M.; Ito, S.; Muntner, P.; Webb, R.C. Hypertension and COVID-19. Am. J. Hypertens. 2020, 33, 373–374. [Google Scholar] [CrossRef]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sinjari, B.; D’Ardes, D.; Santilli, M.; Rexhepi, I.; D’Addazio, G.; Di Carlo, P.; Chiacchiaretta, P.; Caputi, S.; Cipollone, F. SARS-CoV-2 and Oral Manifestation: An Observational, Human Study. J. Clin. Med. 2020, 9, 3218. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103218
Sinjari B, D’Ardes D, Santilli M, Rexhepi I, D’Addazio G, Di Carlo P, Chiacchiaretta P, Caputi S, Cipollone F. SARS-CoV-2 and Oral Manifestation: An Observational, Human Study. Journal of Clinical Medicine. 2020; 9(10):3218. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103218
Chicago/Turabian StyleSinjari, Bruna, Damiano D’Ardes, Manlio Santilli, Imena Rexhepi, Gianmaria D’Addazio, Piero Di Carlo, Piero Chiacchiaretta, Sergio Caputi, and Francesco Cipollone. 2020. "SARS-CoV-2 and Oral Manifestation: An Observational, Human Study" Journal of Clinical Medicine 9, no. 10: 3218. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103218