The Impact of Experience, Length of Service, and Workplace Preparedness in Physicians’ Readiness in the Response to Disasters




Abstract
:1. Introduction
2. Material and Method
2.1. Location of The Study
2.2. Study Population
2.3. Questionnaire
2.4. Data Collection
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bazyar, J.; Farrokhi, M.; Salari, A. The principles of triage in emergencies and disasters: A systematic review. Prehospital Disaster Med. 2020, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Orient, J.M. Fukushima and reflections on radiation as a terror weapon. J. Am. Phys. Surg. 2014, 19, 48–55. [Google Scholar]
- American Medical Association. AMA Code of Medical Ethics’ opinion on physician duty to treat. Opinion 9.067–Physician obligation in disaster preparedness and response. Virtual Mentor 2010, 12, 459. [Google Scholar]
- Hansoti, B.; Kellogg, D.S.; Aberle, S.J.; Broccoli, M.C.; Feden, J.; French, A.; Little, C.M.; Moore, B.; Sabato, J.; Sheets, T.; et al. Preparing emergency physicians for acute disaster response: A review of current training opportunities in the US. Prehospital Disaster Med. 2016, 31, 643–647. [Google Scholar] [CrossRef]
- Al-Dahash, H.; Thayaparan, M.; Kulatunga, U. Understanding the terminologies: Disaster, Crisis, and Emergency. In Proceedings of the 32nd Annual ARCOM Conference, ARCOM, Manchester, UK, 5–7 September 2016; pp. 1191–1200. [Google Scholar]
- Burkle, F.M. Triage. In Handbook of Bioterrorism and Disaster Medicine; Springer: Boston, MA, USA, 2006; pp. 11–17. [Google Scholar]
- Lim, G.H.; Lim, B.L.; Vasu, A. Survey of factors affecting health care workers’ perception towards institutional and individual disaster preparedness. Prehospital Disaster Med. 2013, 28, 353–358. [Google Scholar] [CrossRef]
- Badiali, S.; Giugni, A.; Marcis, L. Testing the START triage protocol: Can it improve the ability of nonmedical personnel to better triage patients during disasters and mass casualties incidents? Disaster Med. Public Health Prep. 2017, 11, 305–309. [Google Scholar] [CrossRef]
- Jose, M.M.; Duufrene, C. Educational competencies and technologies for disaster preparedness in undergraduate nursing education: An integrative review. Nurse Educ. Today 2014, 34, 543–551. [Google Scholar] [CrossRef]
- Chavez, S.; Long, B.; Koyfman, A.; Liang, S.Y. Coronavirus disease (COVID-19): A primer for emergency physicians. Am. J. Emerg. Med. 2020. [Google Scholar] [CrossRef]
- Ragazzoni, L.; Linty, M.; Della Corte, F. Worldwide experiences in disaster medicine education. Disaster Med. Public Health Prep. 2020, 1–2. [Google Scholar] [CrossRef]
- Janczukowicz, J. Medical education in Poland. Med. Teach. 2013, 35, 537–543. [Google Scholar] [CrossRef]
- Hoffmann, R.; Muttarak, R. Learn from the past, prepare for the future: Impacts of education and experience on disaster preparedness in the Philippines and Thailand. World Dev. 2017, 96, 32–51. [Google Scholar] [CrossRef] [Green Version]
- Phattharapornjaroen, P.; Glantz, V.; Carlström, E.; Holmqvist, L.D.; Khorram-Manesh, A. Alternative leadership in flexible surge capacity—The perceived impact of tabletop simulation exercises on thai emergency physicians capability to manage a major incident. Sustainability 2020, 12, 6216. [Google Scholar] [CrossRef]
- Tierney, K. Disaster governance: Social, political, and economic dimensions. Annu. Rev. Environ. Resour. 2012, 37, 341–363. [Google Scholar] [CrossRef]
- Adger, W.N.; Brooks, N. Does global Environmental Change Cause Vulnerability to Disaster? In Natural Disaster and Development in a Globalizing World; Routledge: London, UK, 2003; pp. 35–58. [Google Scholar]
- Goniewicz, K.; Osiak, B.; Pawłowski, W.; Czerski, R.; Burkle, F.M.; Lasota, D.; Goniewicz, M. Bioterrorism preparedness and response in Poland: Prevention, surveillance, and mitigation planning. Disaster Med. Public Health Prep. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, K.; Burkle, F.M. Challenges in implementing Sendai framework for disaster risk reduction in Poland. Int. J. Environ. Res. Public Health 2019, 16, 2574. [Google Scholar] [CrossRef] [Green Version]
- Gerber, B.J.; Robinson, S.E. Local government performance and the challenges of regional preparedness for disasters. Public Perform. Manag. Rev. 2009, 32, 345–371. [Google Scholar] [CrossRef]
- Simpson, D.M. Disaster preparedness measures: A test case development and application. Disaster Prev. Manag. Int. J. 2008, 17, 645–661. [Google Scholar] [CrossRef] [Green Version]
- Shuffler, M.L.; Carter, D.R. Teamwork situated in multiteam systems: Key lessons learned and future opportunities. Am. Psychol. 2018, 73, 390. [Google Scholar] [CrossRef]
- Sayed, M.E.; Chami, A.F.; Hitti, E. Developing a hospital disaster preparedness plan for mass casualty incidents: Lessons learned from the downtown Beirut bombing. Disaster Med. Public Health Prep. 2018, 12, 379–385. [Google Scholar] [CrossRef]
- King, M.A.; Dorfman, M.V.; Einav, S.; Niven, A.S.; Kissoon, N.; Grissom, C.K. Evacuation of intensive care units during disaster: Learning from the Hurricane Sandy experience. Disaster Med. Public Health Prep. 2016, 10, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Khorram-Manesh, A.; Berlin, J.; Carlström, E. Two validated ways of improving the ability of decision-making in emergencies: Results from a literature review. Bull. Emerg. Trauma 2016, 4, 186. [Google Scholar] [PubMed]
- Carr, E.; Chatrath, P.; Palan, P. Audit of doctors’ knowledge of major incident policies. Ann. R. Coll. Surg. Engl. 2006, 88, 313–315. [Google Scholar] [CrossRef] [Green Version]
- Ingrassia, P.L.; Mangini, M.; Azzaretto, M.; Ciaramitaro, I.; Costa, L.; Burkle, F.M.; Della Corte, F.; Djalali, A. Hospital disaster preparedness in Italy: A preliminary study utilizing the World Health Organization hospital emergency response evaluation toolkit. Minerva Anestesiol. 2016, 82, 1259–1266. [Google Scholar] [PubMed]
- Radovic, V.; Vitale, K.; Tchounwou, P.B. Health facilities safety in natural disasters: Experiences and challenges from South East Europe. Int. J. Environ. Res. Public Health 2012, 9, 1677–1686. [Google Scholar] [CrossRef] [Green Version]
- Dückers, M.L.; Witteveen, A.B.; Bisson, J.I.; Olff, M. The association between disaster vulnerability and post-disaster psychosocial service delivery across Europe. Adm. Policy Ment. Health Ment. Health Serv. Res. 2017, 44, 470–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goniewicz, K.; Goniewicz, M. Disaster preparedness and professional competence among healthcare providers: Pilot study results. Sustainability 2020, 12, 493. [Google Scholar] [CrossRef]
- Paganini, M.; Borrelli, F.; Cattani, J.; Ragazzoni, L.; Djalali, A.; Carenzo, L.; Corte, F.D.; Burklejr, F.M.; Ingrassia, P.L. Assessment of disaster preparedness among emergency departments in Italian hospitals: A cautious warning for disaster risk reduction and management capacity. Scand. J. Trauma, Resusc. Emerg. Med. 2016, 24, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nekoie-Moghadam, M.; Kurland, L.; Moosazadeh, M.; Ingrassia, P.L.; Della Corte, F.; Djalali, A. Tools and checklists used for the evaluation of hospital disaster preparedness: A systematic review. Disaster Med. Public Health Prep. 2016, 10, 781–788. [Google Scholar] [CrossRef]
- Shaqsi, A.; Gauld, A.R.; McBride, D. Response time as a sole performance indicator in EMS: Pitfalls and solutions. Open Access Emerg. Med. 2010, 2, 1. [Google Scholar] [CrossRef] [Green Version]
- Rawls, C.G.; Turnquist, M.A. Pre-positioning and dynamic delivery planning for short-term response following a natural disaster. SocioEconomic Plan. Sci. 2012, 46, 46–54. [Google Scholar] [CrossRef]
- Reifels, L.; Pietrantoni, L.; Prati, G.; Kim, Y.; Kilpatrick, D.G.; Dyb, G.; Halpern, J.; Olff, M.; Brewin, C.R.; O’Donnell, M. Lessons learned about psychosocial responses to disaster and mass trauma: An international perspective. Eur. J. Psychotraumatol. 2013, 4, 22897. [Google Scholar] [CrossRef]
- Nilsson, J.; Johansson, E.; Carlsson, M.; Florin, J.; Leksell, J.; Lepp, M.; Lindholm, C.; Nordstrom, G.; Theander, K.; Wilde-Larsson, B.; et al. Disaster nursing: Self-reported competence of nursing students and registered nurses, with focus on their readiness to manage violence, serious events and disasters. Nurse Educ. Pract. 2016, 17, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Djalali, A.; Della Corte, F.; Foletti, M.; Ragazzoni, L.; Gallardo, A.R.; Lupescu, O.; Arculeo, C.; Von Arnim, G.; Friedl, T.; Ashkenazi, M.; et al. Art of disaster preparedness in European Union: A survey on the health systems. PLoS Curr. 2014, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Mortelmans, L.J.; Van Boxstael, S.; De Cauwer, H.G.; Sabbe, M.B. Preparedness of Belgian civil hospitals for chemical, biological, radiation, and nuclear incidents: Are we there yet? Eur. J. Emerg. Med. 2014, 21, 296–300. [Google Scholar] [CrossRef]
- Goniewicz, K.; Misztal-Okońska, P.; Pawłowski, W.; Burkle, F.M.B., Jr.; Czerski, R.; Hertelendy, A.J.; Goniewicz, M. Evacuation from healthcare facilities in Poland: Legal preparedness and preparation. Int. J. Environ. Res. Public Health 2020, 17, 1779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misztal-Okońska, P.; Goniewicz, K.; Hertelendy, A.J.; Khorram-Manesh, A.; Al-Wathinani, A.; Alhazmi, R.A.; Goniewicz, M. How medical studies in Poland prepare future healthcare managers for crises and disasters: Results of a pilot study. Healthcare 2020, 8, 202. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age | n | % |
| Up to 34 | 127 | 23.1% |
| 35–44 years | 147 | 26.8% |
| 45–54 years | 134 | 24.4% |
| 55 years and over | 141 | 25.7% |
| Gender | n | % |
| Women | 251 | 45.7% |
| Men | 298 | 54.3% |
| Length of service | n | % |
| From 0 to 5 years | 81 | 14.8% |
| 6–10 years | 89 | 16.2% |
| 11–15 years | 84 | 15.3% |
| 16–20 years | 100 | 18.2% |
| More than 20 years | 195 | 35.5% |
| Workplace | n | % |
| Public hospital | 438 | 79.8% |
| Research facility | 110 | 20.0% |
| Outpatient Clinic | 1 | 0.2% |
| Risk of Disaster Occurring | Very low | Low | Possible | Probable | Very High | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Type of Incident | n | % | n | % | n | % | n | % | n | % |
| Flooding | 19 | 3.5% | 66 | 12.0% | 136 | 24.8% | 246 | 44.8% | 82 | 14.9% |
| Epidemic | 4 | 0.7% | 31 | 5.6% | 109 | 19.9% | 243 | 44.3% | 162 | 29.5% |
| Terrorist/bioterrorist attack | 99 | 18.0% | 176 | 32.1% | 198 | 36.1% | 76 | 13.8% | 0 | 0.0% |
| Chemical disaster | 67 | 12.2% | 120 | 21.9% | 249 | 45.4% | 113 | 20.6% | 0 | 0.0% |
| Air crash | 82 | 14.9% | 188 | 34.2% | 208 | 37.9% | 71 | 12.9% | 0 | 0.0% |
| Railway crash | 31 | 5.6% | 136 | 24.8% | 274 | 49.9% | 104 | 18.9% | 4 | 0.7% |
| Drought | 5 | 0.9% | 57 | 10.4% | 221 | 40.3% | 212 | 38.6% | 54 | 9.8% |
| Large fire | 17 | 3.1% | 68 | 12.4% | 217 | 39.5% | 236 | 43.0% | 11 | 2.0% |
| Earthquake | 235 | 42.8% | 198 | 36.1% | 93 | 16.9% | 23 | 4.2% | 0 | 0.0% |
| Type of Incident | Place of Incident: Lublin | Other | ||
|---|---|---|---|---|
| n | % | n | % | |
| Flooding | 78 | 33.5% | 155 | 66.5% |
| Epidemic | 361 | 89.1% | 44 | 10.9% |
| Terrorist/bioterrorist attack | 0 | 0.0% | 14 | 100.0% |
| Chemical disaster | 1 | 2.2% | 44 | 97.8% |
| Air crash | 0 | 0.0% | 14 | 100.0% |
| Railway crash | 0 | 0.0% | 38 | 100.0% |
| Drought | 1 | 4.3% | 22 | 95.7% |
| Large fire | 14 | 17.7% | 65 | 82.3% |
| Earthquake | 1 | 3.4% | 28 | 96.6% |
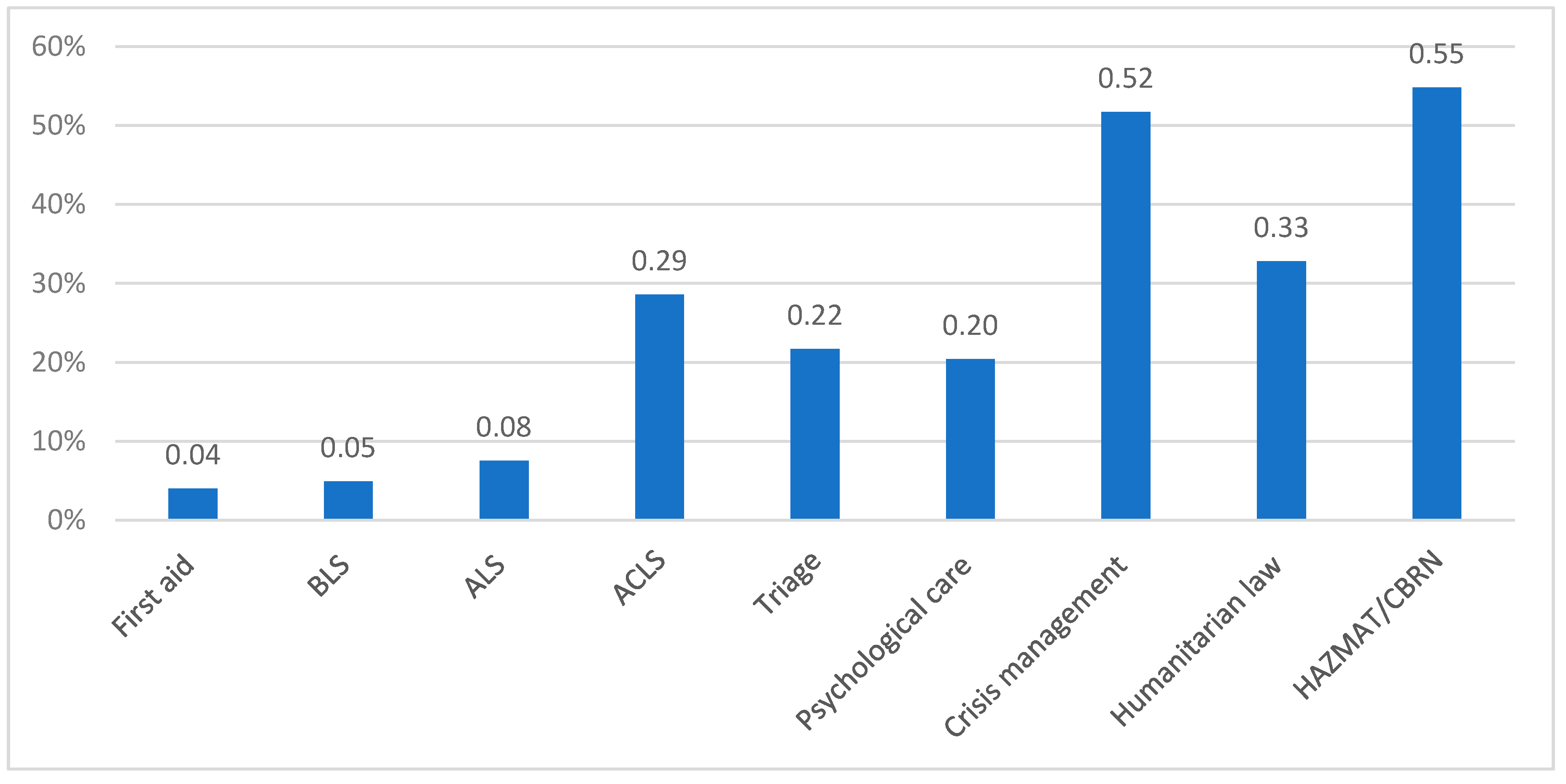
| Type of Training | Yes | No | ||
|---|---|---|---|---|
| n | % | n | % | |
| First aid | 535 | 97.4% | 14 | 2.6% |
| BLS | 508 | 92.5% | 41 | 7.5% |
| ALS | 512 | 93.3% | 37 | 6.7% |
| ACLS | 349 | 63.6% | 200 | 36.4% |
| Triage | 377 | 68.7% | 172 | 31.3% |
| Psychological care | 88 | 16.0% | 461 | 84.0% |
| Crisis management | 84 | 15.3% | 465 | 84.7% |
| Humanitarian law | 91 | 16.6% | 458 | 83.4% |
| HAZMAT/CBRN | 130 | 23.7% | 419 | 76.3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goniewicz, K.; Goniewicz, M.; Burkle, F.M.; Khorram-Manesh, A. The Impact of Experience, Length of Service, and Workplace Preparedness in Physicians’ Readiness in the Response to Disasters. J. Clin. Med. 2020, 9, 3328. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103328
Goniewicz K, Goniewicz M, Burkle FM, Khorram-Manesh A. The Impact of Experience, Length of Service, and Workplace Preparedness in Physicians’ Readiness in the Response to Disasters. Journal of Clinical Medicine. 2020; 9(10):3328. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103328
Chicago/Turabian StyleGoniewicz, Krzysztof, Mariusz Goniewicz, Frederick M. Burkle, and Amir Khorram-Manesh. 2020. "The Impact of Experience, Length of Service, and Workplace Preparedness in Physicians’ Readiness in the Response to Disasters" Journal of Clinical Medicine 9, no. 10: 3328. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103328