Self- and Parent-Reported Psychological Symptoms in Young Cancer Survivors and Control Peers: Results from a Clinical Center

 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
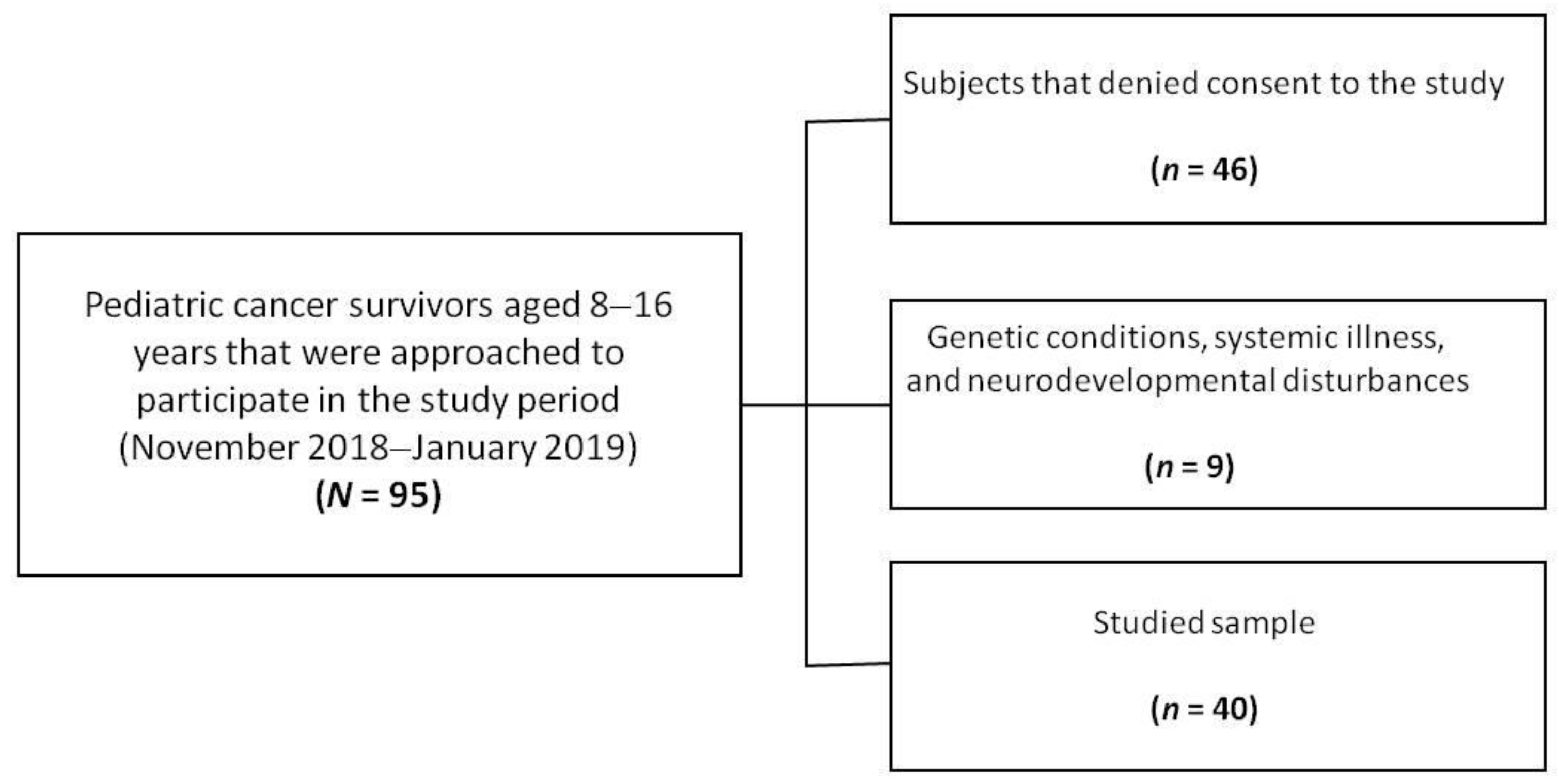
2.1. Participants
2.2. Standardized Assessment
2.3. Anxiety and Depression Symptoms
2.4. Somatic Symptoms
2.5. Behavioral Symptoms
2.6. Functional Disability Measure
2.7. Data Analysis
3. Results
3.1. Emotional Distress Symptoms
3.2. Behavioral Symptoms
3.3. Somatic Symptoms
3.4. Functional Disability
3.5. Symptoms Severity and Co-occurrence
3.6. Multivariate Analysis of the Clinical Parameters and Age-Related Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. SEER Cancer Statistics Review, 1975–2016; National Cancer Institute: Bethesda, MD, USA, 2019.
- Bitsko, M.J.; Cohen, D.; Dillon, R.; Harvey, J.; Krull, K.; Klosky, J.L. Psychological Late Effects in Pediatric Cancer Survivors: A Report from the Children’s Oncology Group. Pediatr. Blood Cancer 2016, 63, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Brinkman, T.M.; Recklitis, C.J.; Michel, G.; Grootenhuis, M.A.; Klosky, J.L. Psychological Symptoms, Social Outcomes, Socioeconomic Attainment, and Health Behaviors Among Survivors of Childhood Cancer: Current State of the Literature. J. Clin. Oncol. 2018, 36, 2190–2197. [Google Scholar] [CrossRef] [PubMed]
- Marusak, H.A.; Iadipaolo, A.S.; Harper, F.W.; Elrahal, F.; Taub, J.W.; Goldberg, E.; Rabinak, C.A. Neurodevelopmental consequences of pediatric cancer and its treatment: Applying an early adversity framework to understanding cognitive, behavioral, and emotional outcomes. Neuropsychol. Rev. 2017, 28, 123–175. [Google Scholar] [CrossRef] [PubMed]
- Winter, A.L.; Conklin, H.M.; Tyc, V.L.; Stancel, H.; Hinds, P.S.; Hudson, M.M.; Kahalley, L.S. Executive function late effects in survivors of pediatric brain tumors and acute lymphoblastic leukemia. J. Clin. Exp. Neuropsychol. 2014, 36, 818–830. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.M.; Padgett, L.S.; Leisenring, W.M.; Stratton, K.K.; Bishop, K.; Krull, K.R.; Alfano, C.M.; Gibson, T.M.; De Moor, J.S.; Hartigan, D.B.; et al. Survivors of Childhood Cancer in the United States: Prevalence and Burden of Morbidity. Cancer Epidemiol. Biomark. Prev. 2015, 24, 653–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gianinazzi, M.E.; Rueegg, C.S.; Wengenroth, L.; Bergstraesser, E.; Rischewski, J.; Ammann, R.A.; Kuehni, C.E.; Michel, G.; Swiss Pediatric Oncology Group (SPOG). Adolescent survivors of childhood cancer: Are they vulnerable for psychological distress? Psycho-Oncology 2013, 22, 2051–2058. [Google Scholar] [CrossRef]
- Mertens, A.C.; Marchak, J.G. Mental health status of adolescent cancer survivors. Clin. Oncol. Adolesc. Young Adults 2015, 5, 87–95. [Google Scholar] [CrossRef] [Green Version]
- D’Agostino, N.M.; Edelstein, K.; Zhang, N.; Recklitis, C.J.; Brinkman, T.M.; Srivastava, D.; ScD, W.M.L.; Robison, L.L.; Armstrong, G.T.; Krull, K.R. Comorbid symptoms of emotional distress in adult survivors of childhood cancer. Cancer 2016, 122, 3215–3224. [Google Scholar] [CrossRef]
- Brinkman, T.M.; Li, C.; Vannatta, K.; Marchak, J.G.; Lai, J.-S.; Prasad, P.K.; Kimberg, C.; Vuotto, S.; Di, C.; Srivastava, D.; et al. Behavioral, Social, and Emotional Symptom Comorbidities and Profiles in Adolescent Survivors of Childhood Cancer: A Report From the Childhood Cancer Survivor Study. J. Clin. Oncol. 2016, 34, 3417–3425. [Google Scholar] [CrossRef]
- Liu, W.; Cheung, Y.T.; Brinkman, T.M.; Banerjee, P.; Srivastava, D.; Nolan, V.G.; Zhang, H.; Gurney, J.G.; Pui, C.-H.; Robison, L.L.; et al. Parent-Reported and Self-Perceived Behavioral and Psychiatric Symptoms in Long-Term Survivors of Childhood Acute Lymphoblastic Leukemia. Blood 2016, 128, 3594. [Google Scholar] [CrossRef]
- Liu, W.; Cheung, Y.T.; Brinkman, T.M.; Banerjee, P.; Srivastava, D.; Nolan, V.G.; Zhang, H.; Gurney, J.G.; Pui, C.-H.; Robison, L.L.; et al. Behavioral symptoms and psychiatric disorders in child and adolescent long-term survivors of childhood acute lymphoblastic leukemia treated with chemotherapy only. Psycho-Oncology 2018, 27, 1597–1607. [Google Scholar] [CrossRef]
- Erickson, S.J.; Hile, S.; Kubinec, N.; Annett, R.D. Self-reported and parent proxy reported functional impairment among pediatric cancer survivors and controls. Health Qual. Life Outcomes 2020, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, D. Wechsler Intelligence Scale for Children—Third Edition: Canadian (WISC-III); Psychological Corporation: Toronto, ON, Canada, 1991. [Google Scholar]
- March, J.S.; Parker, J.D.; Sullivan, K.; Stallings, P.; Conners, C.K. The Multidimensional Anxiety Scale for Children (MASC): Factor Structure, Reliability, and Validity. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 554–565. [Google Scholar] [CrossRef]
- Kovacs, M. The Children’s Depression, Inventory (CDI). Psychopharmacol. Bull. 1985, 21, 995–998. [Google Scholar]
- Stone, A.L.; Walker, L.S.; Heathcote, L.; Hernandez, J.M.; Basch, M.C.; Wilson, A.C.; Simons, L.E. Somatic Symptoms in Pediatric Patients with Chronic Pain: Proposed Clinical Reference Points for the Children’s Somatic Symptoms Inventory (Formerly the Children’s Somatization Inventory). J. Pain 2019, 20, 932–940. [Google Scholar] [CrossRef]
- Achenbach, T.M. Manual for the CBCL/4-18 and Profile; Department of Psychiatry, University of Vermont: Burlington, VA, USA, 1991. [Google Scholar]
- Kashikar-Zuck, S.; Flowers, S.R.; Claar, R.L.; Guite, J.W.; Logan, D.E.; Lynch-Jordan, A.M.; Palermo, T.M.; Wilson, A.C. Clinical utility and validity of the Functional Disability Inventory among a multicenter sample of youth with chronic pain. Pain 2011, 152, 1600–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attarbaschi, A.; Mann, G.; Zimmermann, M.; Bader, P.; Barisone, E.; Basso, G.; Biondi, A.; Cario, G.; Cazzaniga, G.; Colombini, A.; et al. Randomized post-induction and delayed intensification therapy in high-risk pediatric acute lymphoblastic leukemia: Long-term results of the international AIEOP-BFM ALL 2000 trial. Leukemia 2019, 34, 1694–1700. [Google Scholar] [CrossRef]
- Würthwein, G.; Lanvers-Kaminsky, C.; Gerss, J.; Möricke, A.; Zimmermann, M.; Stary, J.; Smisek, P.; Attarbaschi, A.; Nath, C.; Zucchetti, M.; et al. Therapeutic Drug Monitoring of Asparaginase: Intra-individual Variability and Predictivity in Children with Acute Lymphoblastic Leukemia Treated with PEG-Asparaginase in the AIEOP-BFM Acute Lymphoblastic Leukemia 2009 Study. Ther. Drug Monit. 2020, 42, 435–444. [Google Scholar] [CrossRef]
- Mussolin, L.; Lovisa, F.; Gallingani, I.; Cavallaro, E.; Carraro, E.; Damanti, C.C.; Vinti, L.; Sala, A.; Micalizzi, C.; Santoro, N.; et al. Minimal residual disease analysis in childhood mature B-cell leukaemia/lymphoma treated with AIEOP LNH-97 protocol with/without anti-CD20 administration. Br. J. Haematol. 2020, 189, e108–e111. [Google Scholar] [CrossRef] [Green Version]
- Spreafico, F.; Biasoni, D.; Vullo, S.L.; Gandola, L.; D’Angelo, P.; Terenziani, M.; Bianchi, M.; Provenzi, M.; Indolfi, P.; Pession, A.; et al. Results of the Third AIEOP Cooperative Protocol on Wilms Tumor (TW2003) and Related Considerations. J. Urol. 2017, 198, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Purcell, R.V.; Childs, M.; Maibach, R.; Miles, C.; Turner, C.; Zimmermann, A.; Czauderna, P.; Sullivan, M. Potential biomarkers for hepatoblastoma: Results from the SIOPEL-3 study. Eur. J. Cancer 2012, 48, 1853–1859. [Google Scholar] [CrossRef]
- Stam, H.; Grootenhuis, M.A.; Last, B.F. Social and emotional adjustment in young survivors of childhood cancer. Support. Care Cancer 2001, 9, 489–513. [Google Scholar] [CrossRef] [PubMed]
- Daly, A.; Lewis, R.W.; Vangile, K.; Masker, K.W.; Effinger, K.E.; Meacham, L.R.; Mertens, A.C. Survivor clinic attendance among pediatric- and adolescent-aged survivors of childhood cancer. J. Cancer Surviv. 2018, 13, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Schulte, F.; Russell, K.B.; Pelletier, W.; Scott-Lane, L.; Guilcher, G.M.T.; Strother, D.; Dewey, D.M. Screening for psychosocial distress in pediatric cancer patients: An examination of feasibility in a single institution. Pediatr. Hematol. Oncol. 2019, 36, 125–137. [Google Scholar] [CrossRef] [PubMed]
- McGrath, J.J.; Lim, C.C.W.; Plana-Ripoll, O.; Holtz, Y.; Agerbo, E.; Momen, N.C.; Mortensen, P.B.; Pedersen, C.B.; Abdulmalik, J.; Aguilar-Gaxiola, S.; et al. Comorbidity within mental disorders: A comprehensive analysis based on 145 990 survey respondents from 27 countries. Epidemiol. Psychiatr. Sci. 2020, 29, e153. [Google Scholar] [CrossRef]
- Campo, J.V. Annual Research Review: Functional somatic symptoms and associated anxiety and depression-developmental psychopathology in pediatric practice. J. Child Psychol. Psychiatry 2012, 53, 575–592. [Google Scholar] [CrossRef]
- Cerutti, R.; Spensieri, V.; Valastro, C.; Presaghi, F.; Canitano, R.; Guidetti, V. A comprehensive approach to understand somatic symptoms and their impact on emotional and psychosocial functioning in children. PLoS ONE 2017, 12, e0171867. [Google Scholar] [CrossRef]
- Zolog, T.C.; Ballabriga, M.C.J.; Bonillo-Martin, A.; Canals-Sans, J.; Hernández-Martínez, C.; Romero-Acosta, K.; Domenech-llaberia, E. Somatic complaints and symptoms of anxiety and depression in a school-based sample of preadolescents and early adolescents functional impairment and implications for treatment. J. Cogn. Behav. Psychother. 2011, 11, 191–208. [Google Scholar]
- Kassam-Adams, N.; García-España, J.F.; Miller, V.A.; Winston, F. Parent-child agreement regarding children’s acute stress: The role of parent acute stress reactions. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 1485–1493. [Google Scholar] [CrossRef]
- Okado, Y.; Long, A.M.; Phipps, S. Association between Parent and Child Distress and the Moderating Effects of Life Events in Families with and without a History of Pediatric Cancer. J. Pediatr. Psychol. 2014, 39, 1049–1060. [Google Scholar] [CrossRef] [Green Version]
- Marusak, H.A.; Harper, F.W.; Taub, J.W.; A Rabinak, C. Pediatric cancer, posttraumatic stress and fear-related neural circuitry. Int. J. Hematol. Oncol. 2019, 8, IJH17. [Google Scholar] [CrossRef] [PubMed]
- Karlson, C.W.; Sarver, D.E.; Raiker, J.S.; Espil, F.M.; Cox, A.D.; Elkin, T.D.; Annett, R.D. The contribution of neurocognitive functions to academic and psychological outcomes in pediatric cancer: A latent profile analysis. Child Neuropsychol. 2020, 26, 881–899. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Clinical Variable | Survivors Mean (SD) (n = 40) | Controls Mean (SD) (n = 79) | df | t | p * |
|---|---|---|---|---|---|
| Age at study time (years) Cognitive level (WISC III total IQ) | 12.9 (3.1) 99.5 (14.74) | 12.5 (3.3) 96.15(12.46) | 117 79 | 0.895 0.928 | 0.256 0.357 |
| Anxiety symptoms (MASC total T-score) | 48.30 (10.89) | 42.96 (10.22) | 116 | 3.241 | 0.0016 |
| Depression symptoms (CDI total T-score) | 46.48 (9.49) | 49.08 (7.55) | 117 | 0.606 | 0.504 |
| Behavioral symptoms (CBCL total T-score) | 47.08 (9.82) | 43.01 (11.02) | 117 | 2.431 | 0.016 |
| Somatic symptoms (CSSI-24 child total) | 5.56 (7.79) | 7.35 (8.94) | 112 | −0.531 | 0.597 |
| Somatic symptoms (CSSI-24 parent total) | 4.98 (1.91) | 5. 23(2.34) | 117 | 0.156 | 0.876 |
| Functional disability (FDI—child total) | 2.58 (3.85) | 2.62 (4.60) | 112 | 0.396 | 0.693 |
| Functional disability( FDI—parent total) | 0.44 (1.42) | 0.31 (1.23) | 117 | 0.404 | 0.575 |
| Severity Scores | CBCL Total T-Score | Parent CSSI-24 Total | Child CSSI-24 Total | Parent FDI Total | Child FDI Total |
|---|---|---|---|---|---|
| MASC total T-score | 0.489 * (0.536) a | 0.430 ** (0.041) | 0.441 ** (0.561) ** | 0.320 * (0.061) | 0.490 ** (0.289) |
| CDI total T-score | 0.735 ** (0.413) | 0.559 ** (0.061) | 0.554 ** (0.416) ** | 0.683 ** (0.229) | 0.633 ** (0.020) |
| CBCL total T-score | 0.375 * (0.710) ** | 0.493 * (0.173) | 0.430 (0.616) ** | 0.387 * (−0.364) | |
| Parent-CSSI-24 total | 0.350 * (0.199) | 0.387 * (0.951) ** | |||
| Child CSSI-24 total | 0.368 * (0.209) * | 0.79 ** (0.801) ** | |||
| Parent FDI total | 0.440 ** (0.237) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barone, R.; Gulisano, M.; Cannata, E.; Padalino, S.; Saia, F.; Maugeri, N.; Pettinato, F.; Lo Nigro, L.; Casabona, A.; Russo, G.; et al. Self- and Parent-Reported Psychological Symptoms in Young Cancer Survivors and Control Peers: Results from a Clinical Center. J. Clin. Med. 2020, 9, 3444. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113444
Barone R, Gulisano M, Cannata E, Padalino S, Saia F, Maugeri N, Pettinato F, Lo Nigro L, Casabona A, Russo G, et al. Self- and Parent-Reported Psychological Symptoms in Young Cancer Survivors and Control Peers: Results from a Clinical Center. Journal of Clinical Medicine. 2020; 9(11):3444. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113444
Chicago/Turabian StyleBarone, Rita, Mariangela Gulisano, Emanuela Cannata, Sara Padalino, Federica Saia, Nicoletta Maugeri, Fabio Pettinato, Luca Lo Nigro, Antonino Casabona, Giovanna Russo, and et al. 2020. "Self- and Parent-Reported Psychological Symptoms in Young Cancer Survivors and Control Peers: Results from a Clinical Center" Journal of Clinical Medicine 9, no. 11: 3444. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113444