Determination of Stent Load Conditions in New Zealand White Rabbit Urethra

 , ,
, ,
Abstract
:1. Introduction
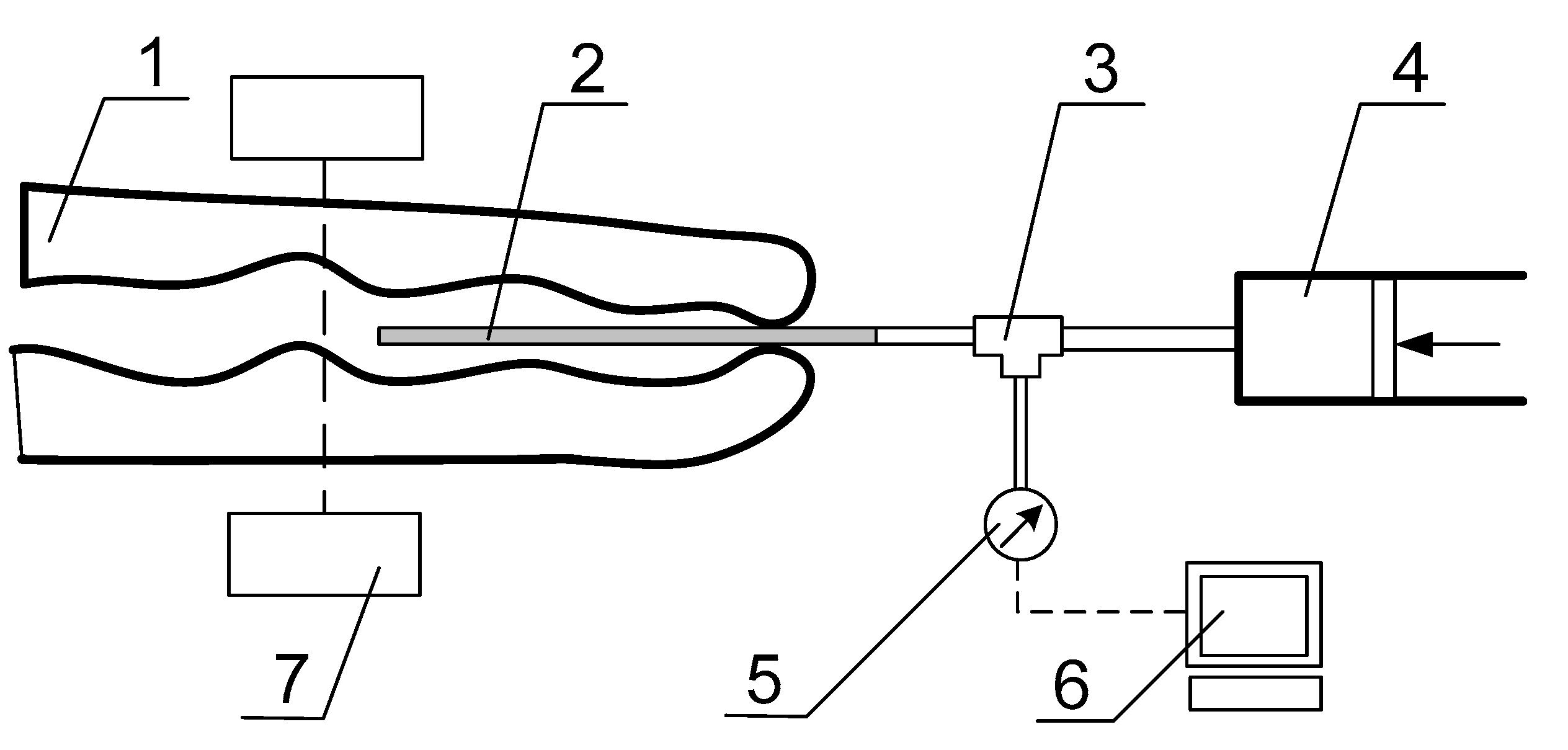
2. Materials and Methods
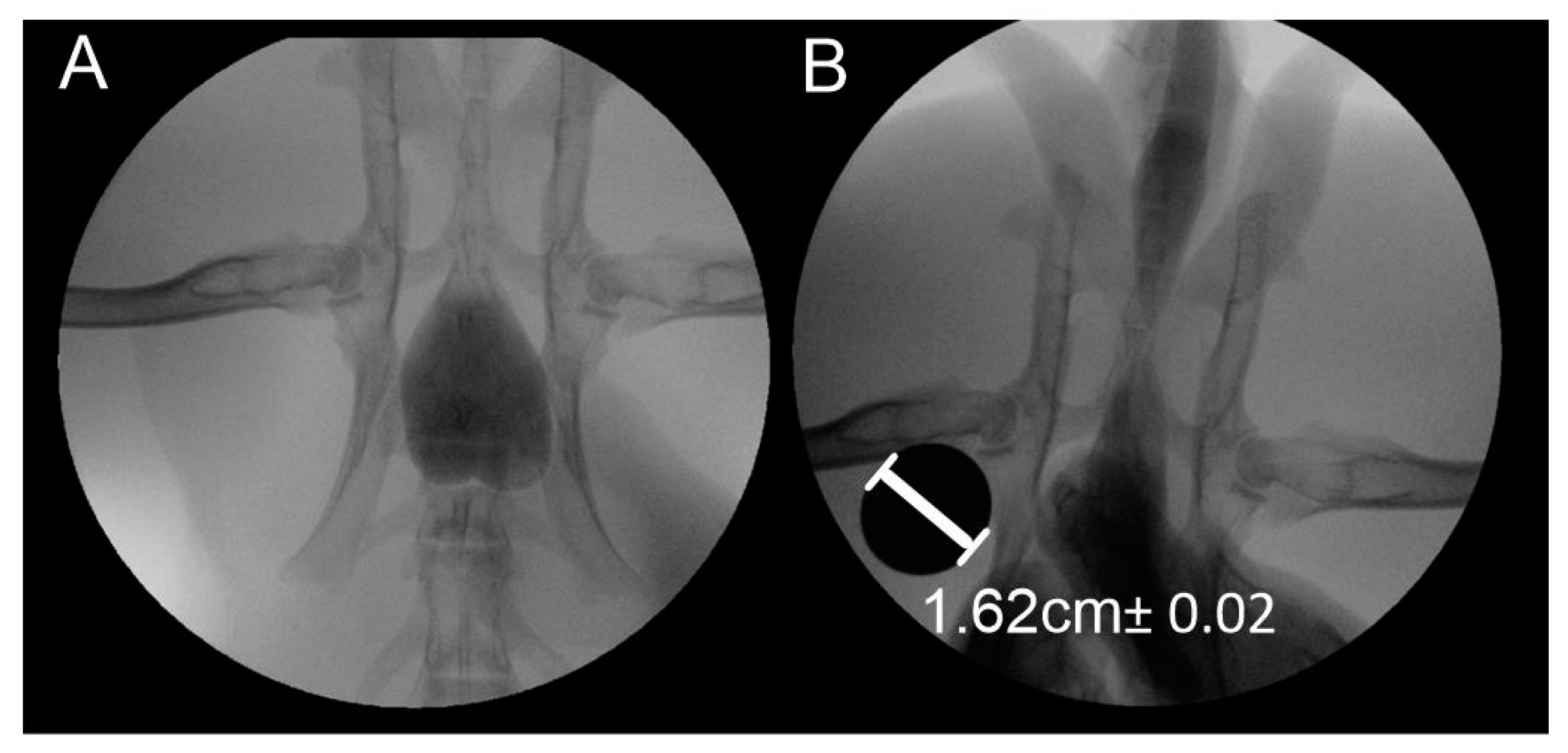
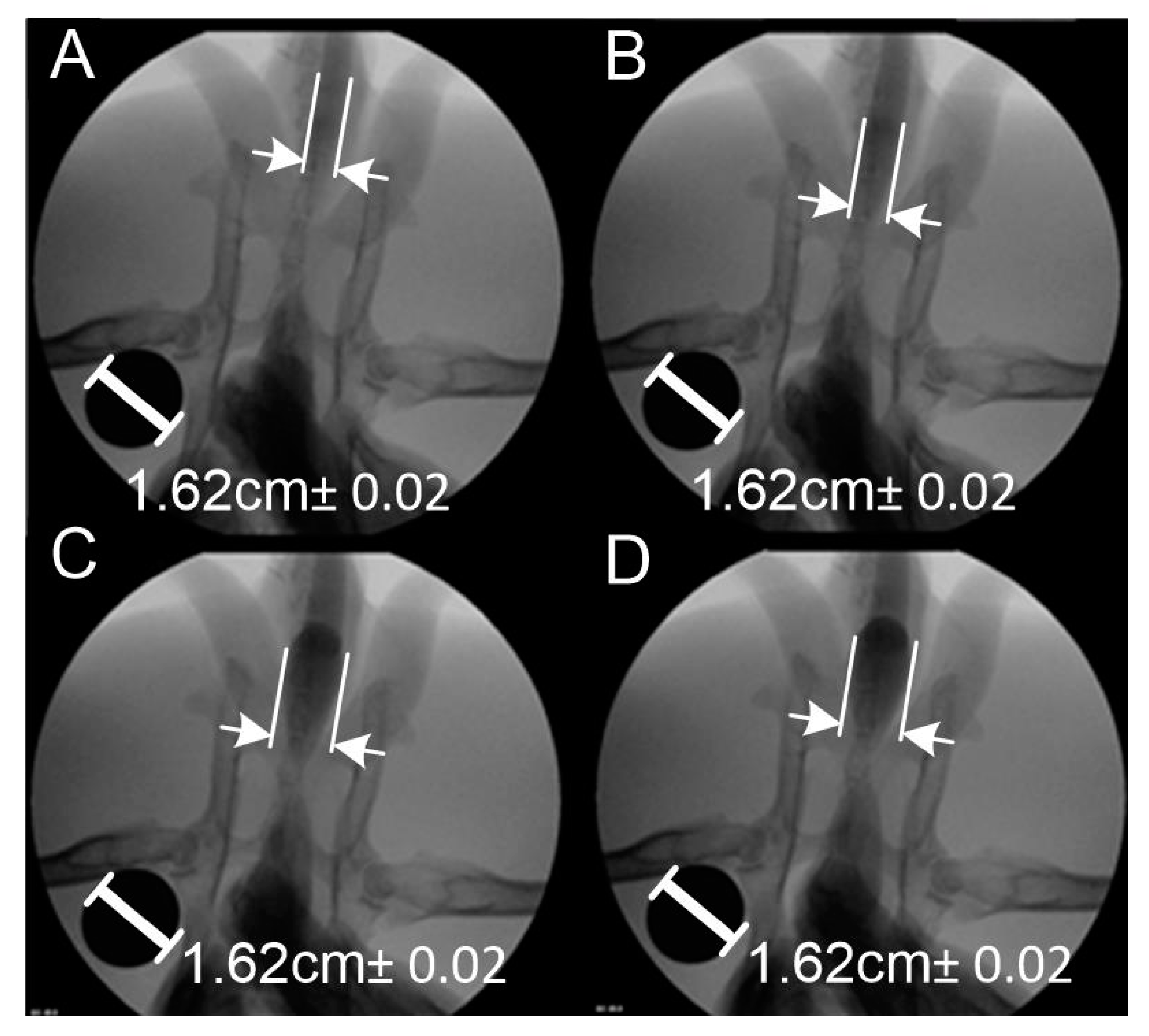
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Santucci, R.; Eisenberg, L. Urethrotomy has a much lower success rate than previously reported. J. Urol. 2010, 183, 1859–1862. [Google Scholar] [CrossRef] [PubMed]
- Jankowski, R.J.; Prantil, R.L.; Fraser, M.O.; Chancellor, M.B.; De Groat, W.C.; Huard, J.; Vorp, D.A. Development of an experimental system for the study of urethral biomechanical function. Am. J. Physiol. Renal Physiol. 2004, 286, 225–322. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, I.; Rogg, B. A simple fluid-mechanical model for the prediction of the stress-strain relation of the male urinary bladder. J. Biomech. 2007, 40, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Natali, A.N.; Carniel, E.L.; Frigo, A.; Pavan, P.G.; Todros, S.; Pachera, P.; Fontanella, C.G.; Rubini, A.; Cavicchioli, L.; Avital, Y.; et al. Experimental investigation of the biomechanics of urethral tissues and structures. Exp. Physiol. 2016, 101, 641–656. [Google Scholar] [CrossRef] [PubMed]
- Todros, S.; Pavan, P.G.; Natali, A.N. Biomechanical properties of synthetic surgical meshes for pelvic prolapse repair. J. Mech. Behav. Biomed. Mater. 2016, 55, 271–285. [Google Scholar] [CrossRef]
- Tritschler, S.; Roosen, A.; Füllhase, C.; Stief, C.G.; Rübben, H. Urethral Stricture: Etiology, Investigation and Treatments. Dtsch. Arztebl. Int. 2013, 110, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Ekeke, O.N.; Amusan, O.E. Clinical presentation and treatment of urethral stricture: Experience from a tertiary hospital in Port Harcourt, Nigeria. Afr. J. Urol. 2017, 23, 72–77. [Google Scholar] [CrossRef] [Green Version]
- Barbagli, G.; Montorsi, F.; Guazzoni, G.; Larcher, A.; Fossati, N.; Sansalone, S.; Romano, G.; Buffi, N.; Lazzeri, M. Ventral oral mucosal only graft urethroplasty in non-traumatic bulbar urethral strictures: Surgical technique and multivariable analysis of results in 214 patients. Eur. Urol. 2013, 64, 440–447. [Google Scholar] [CrossRef]
- Cavalcanti, A.G.; Costa, W.S.; Baskin, L.S.; McAninch, J.A.; Sampaio, F.J. A morphometric analysis of bulbar urethral strictures. BJU Int. 2007, 100, 397–402. [Google Scholar] [CrossRef]
- Simsek, A.; Aldamanhori, R.; Chapple, C.R.; MacNeil, S. Overcoming scarring in the urethra: Challenges for tissue engineering. Asian J. Urol. 2018, 5, 69–77. [Google Scholar] [CrossRef]
- Speakman, M.J. Lower Urinary Tract Symptoms Suggestive of Benign Prostatic Hyperplasia (LUTS/BPH): More than Treating Symptoms? Eur. Urol. Suppl. 2008, 7, 680–689. [Google Scholar] [CrossRef]
- Skonieczna, J.; Madej, J.P.; Będziński, R. Accessory genital glands in the New Zealand White rabbit: A morphometrical and histological study. J. Vet. Res. 2019, 63, 251–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimi, A.; Shojaei, A. An Experimental Study to Measure the Mechanical Properties of the Human Liver. Dig. Dis. 2018, 36, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Nava, A.; Mazza, Q.E.; Kleinermann, F.; Avis, N.J.; McClure, J.; Bajka, J. Evaluation of the mechanical properties of human liver and kidney through aspiration experiments. Technol. Health Care 2004, 12, 269–280. [Google Scholar] [CrossRef]
- Yamashita, Y.; Kubota, M. Ultrasonic Imaging of Elasticity of Soft Tissue Based on Measurement of Internal Displacement and Strain. In Proceedings of the 1995 IEEE Ultrasonics Symposium, Seattle, WA, USA, 7–10 November 1995; pp. 1207–1211. [Google Scholar]
- Samur, E.; Sedef, M.; Basdogan, C.; Avtan, L.; Duzgun, O.A. Robotic indenter for minimally invasive measurement and characterization of soft tissue response. Med. Image Anal. 2007, 11, 361–373. [Google Scholar] [CrossRef]
- Masri, C.; Chagnon, G.; Favier, D.; Sartelet, H.; Girard, E. Experimental characterization and constitutive modeling of the biomechanical behavior of male human urethral tissues validated by histological observations. Biomech. Model. Mechanobiol. 2018, 17, 939–950. [Google Scholar] [CrossRef] [Green Version]
- Bullock, T.L.; Brandes, S.B. Adult anterior urethral strictures: A national practice patterns survey of board certified urologists in the United States. J. Urol. 2007, 177, 685–690. [Google Scholar] [CrossRef]
- Djordjevic, M. Treatment of urethral stricture disease by internal urethrotomy, dilation or stenting. Eur. Urol. Suppl. 2016, 15, 7–12. [Google Scholar] [CrossRef]
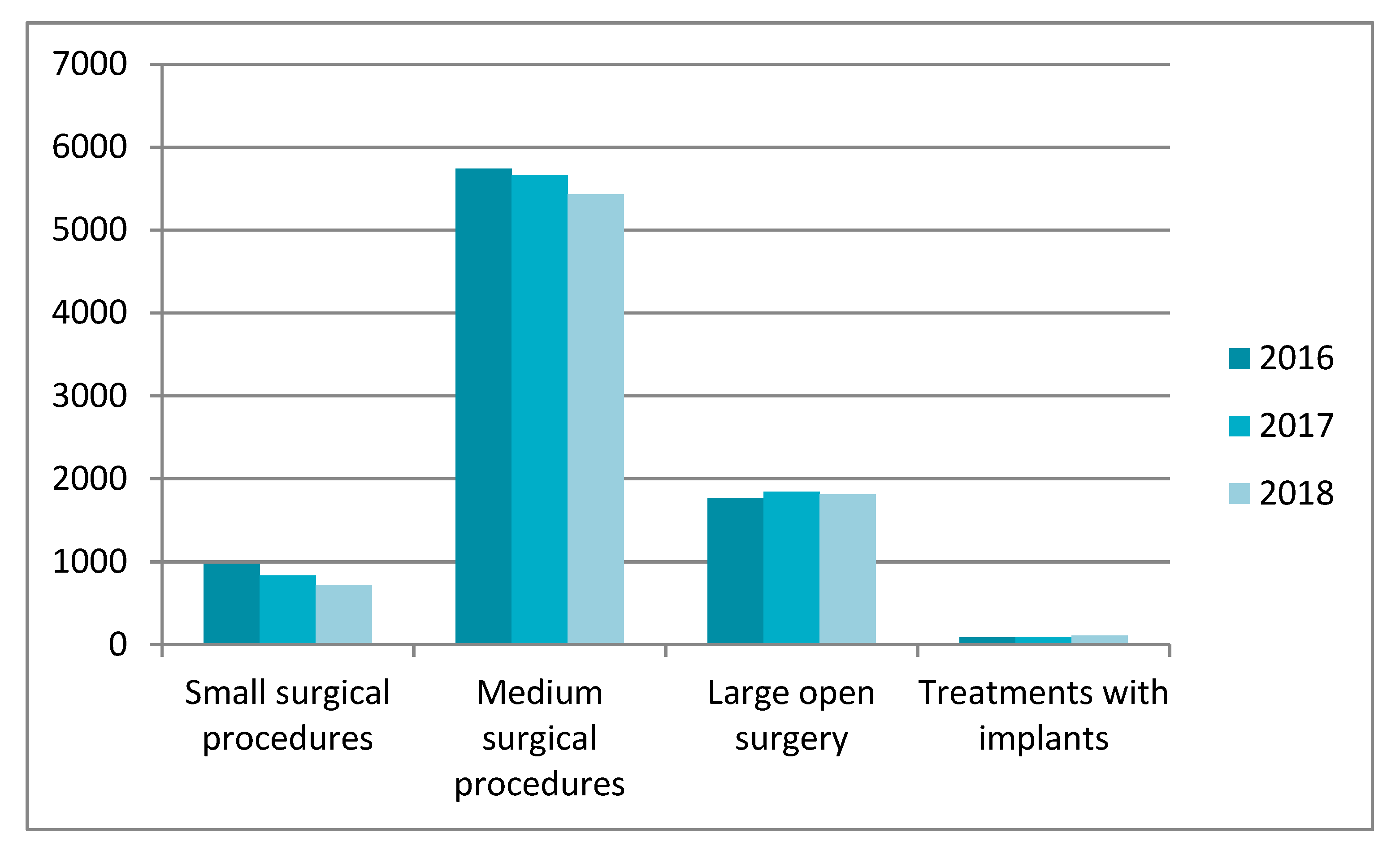
- Polish National Health Fund. Statistics for the Period 2016–2018 for the Code of L—Urinary and Genitourinary Diseases. 3 February 2020. Available online: https://statystyki.nfz.gov.pl/Benefits/1a?S.Section=L+-+Choroby+uk%C5%82adu+moczowo-p%C5%82ciowego&S.Name=&S.Catalog=1a&S.Year=2018&S.SelectedTab=BasicData&search=true (accessed on 10 June 2020).
- Sountoulides, P.; Kaplan, A.; Kaufmann, O.G. Current status of metal stents for managing malignant ureteric obstruction. BJU Int. 2010, 105, 1066–1072. [Google Scholar] [CrossRef]
- Temeltas, G.; Ucer, O.; Yuksel, M.B.; Gumus, B.; Tatli, V.; Muezzinoglu, T. The long-term results of temporary urethral stent placement for the treatment of recurrent bulbar urethral stricture disease. Int. Braz. J. Urol. 2016, 42, 351–355. [Google Scholar] [CrossRef]
- Park, J.-H.; Song, H.-H.; Shin, J.H.; Kim, J.H.; Jun, E.J.; Cho, Y.C.; Kim, S.H.; Park, J. Polydioxanone Biodegradable Stent Placement in a Canine Urethral Model: Analysis of Inflammatory Reaction and Biodegradation. J. Vasc. Interv. Radiol. 2014, 25, 1257–1264. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Chung, K.J.; Choo, S.H.; Han, D.H. Long-term outcomes of two types of metal stent for chronic benign ureteral strictures. BMC Urol. 2019, 19, 19–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurowiak, J.; Kaczmarek-Pawelska, A.; Mackiewicz, A.G.; Bedzinski, R. Analysis of the Degradation Process of Alginate-Based Hydrogels in Artificial Urine for Use as a Bioresorbable Material in the Treatment of Urethral Injuries. Processes 2020, 8, 304. [Google Scholar] [CrossRef] [Green Version]
- Arkusz, K.; Nycz, M.; Paradowska, E. Electrochemical Evaluation of the Compact and Nanotubular Oxide Layer Destruction under Ex Vivo Ti6Al4V ELI Transpedicular Screw Implantation. Materials 2020, 13, 176. [Google Scholar] [CrossRef] [Green Version]
- Nycz, M.; Arkusz, K.; Pijanowska, D. Influence of the Silver Nanoparticles (AgNPs) Formation Conditions onto Titanium Dioxide (TiO2) Nanotubes Based Electrodes on Their Impedimetric Response. Nanomaterials 2019, 9, 1072. [Google Scholar] [CrossRef] [Green Version]
- Klekiel, T.; Mackiewicz, A.; Kaczmarek-Pawelska, A.; Skonieczna, A.; Kurowiak, J.; Piasecki, T.; Noszczyk-Nowak, A.; Bedzinski, R. Novel design of sodium alginate based absorbable stent for the use in urethral stricture disease. J. Mater. Res. Technol. 2020, 9, 9004–9015. [Google Scholar] [CrossRef]
- Versteegden, L.R.M.; de Jonge, P.K.J.D.; IntHout, J.; van Kuppevelt, T.H.; Oosterwijk, E.; Feitz, W.F.J.; de Vries, R.B.M.; Daamen, W.F. Tissue Engineering of the Urethra: A Systematic Review and Meta-Analysis of Preclinical and Clinical Studies. Eur. Urol. 2017, 72, 594–606. [Google Scholar] [CrossRef]
- Wang, F.; Liu, T.; Yang, L.; Zhang, G.; Liu, H.; Yi, D.; Yang, X.; Lin, T.-Y.; Qin, W.; Yuan, J. Urethral Reconstruction with Tissue-Engineered Human Amniotic Scaffold in Rabbit Urethral Injury Models. Med. Sci. Monit. 2014, 20, 2430–2438. [Google Scholar] [CrossRef] [Green Version]
- Glybochko, P.V.; Aljaev, J.G.; Nikolenko, V.N.; Shehter, A.B.; Vinarov, A.Z.; Istranov, L.P. Tissue-Engineered Substitution Urethroplasty Based on Decellularized Vascular Matrix and Autologous Cells of the Buccal Mucosa: The First Experience. Urologiia 2015, 3, 4–10. [Google Scholar]
- Gu, G.L.; Zhu, Y.J.; Xia, S.J.; Zhang, J.; Jiang, J.T.; Hong, Y. Peritoneal cavity as bioreactor to grow autologous tubular urethral grafts in a rabbit model. World J. Urol. 2010, 28, 227–232. [Google Scholar] [CrossRef]
- Huang, J.W.; Xie, M.K.; Zhang, Y.; Wei, G.J.; Li, X.; Li, H.B. Reconstruction of Penile Urethra with the 3-Dimensional Porous Bladder Acellular Matrix in a Rabbit Model. Urology 2014, 84, 1499–1505. [Google Scholar] [CrossRef] [PubMed]
- Lv, X.; Li, Z.; Chen, S.; Xie, M.; Huang, J.; Peng, X. Structural and functional evaluation of oxygenating keratin/silk fibroin scaffold and initial assessment of their potential for urethral tissue engineering. Biomaterials 2016, 84, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Nuininga, J.E.; Koens, M.J.; Tiemessen, D.M.; Oosterwijk, E.; Daamen, W.F.; Geutjes, P.J. Urethral reconstruction of critical defects in rabbits using molecularly defined tubular type I collagen biomatrices: Key issues in growth factor addition. Tissue Eng. Part A 2010, 16, 3319–3328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uthamanthil, R.K.; Hachem, R.Y.; Gagea, M.; Reitzel, R.A.; Borne, A.T.; Tinkey, P.T. Urinary Catheterization of Male Rabbits: A New Technique and a Review of Urogenital Anatomy. J. Am. Assoc. Lab. Anim. Sci. 2013, 52, 180–185. [Google Scholar] [PubMed]
- Shaw, N.M.; Venkatesan, K. Endoscopic Management of Urethral Stricture: Review and Practice Algorithm for Management of Male Urethral Stricture Disease. Curr. Urol. Rep. 2018, 19, 19. [Google Scholar] [CrossRef] [PubMed]
- Cotter, K.J.; Hahn, A.E.; Voelzke, B.B.; Myers, J.B.; Smith, T.G.; Elliott, S.P.; Alsikafi, N.F.; Breyer, B.N.; Vanni, A.J.; Buckley, J.C.; et al. Trends in Urethral Stricture Disease Etiology and Urethroplasty Technique from a Multi-institutional Surgical Outcomes Research Group. Urology 2019, 130, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Natali, A.N.; Carniel, E.L.; Frigo, A.; Fontanella, C.G.; Rubinim, A.; Avital, Y.; De Benedictis, G.M. Experimental investigation of the structural behavior of equine urethra. Comput. Methods Programs Biomed. 2017, 141, 35–41. [Google Scholar] [CrossRef]
- Bagi, P.; Thind, P.; Colstrup, H.; Kristensen, J.K. The dynamic pressure response to rapid dilatation of the resting urethra in healthy women: An in vivo evaluation of visco-elastic properties. Urol. Res. 1993, 21, 339–343. [Google Scholar] [CrossRef]
- Vanderbrink, B.A.; Rastinehad, A.R.; Badlani, G.H. Prostatic stents for the treatment of benign prostatic hyperplasia. Curr. Opin. Urol. 2007, 17, 1–6. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Volume of Fluid [mL] | Diameter of the Urethra [mm] | Pressure Inside Urethra [kPa] |
|---|---|---|
| 20 | 4.19 Na | 1.5 ± 0.015 |
| 40 | 6.41 | 1.5 ± 0.015 |
| 60 | 7.54 | 1.5 ± 0.015 |
| 80 | 10.66 | 1.5 ± 0.015 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mackiewicz, A.G.; Klekiel, T.; Kurowiak, J.; Piasecki, T.; Bedzinski, R. Determination of Stent Load Conditions in New Zealand White Rabbit Urethra. J. Funct. Biomater. 2020, 11, 70. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb11040070
Mackiewicz AG, Klekiel T, Kurowiak J, Piasecki T, Bedzinski R. Determination of Stent Load Conditions in New Zealand White Rabbit Urethra. Journal of Functional Biomaterials. 2020; 11(4):70. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb11040070
Chicago/Turabian StyleMackiewicz, Agnieszka G., Tomasz Klekiel, Jagoda Kurowiak, Tomasz Piasecki, and Romuald Bedzinski. 2020. "Determination of Stent Load Conditions in New Zealand White Rabbit Urethra" Journal of Functional Biomaterials 11, no. 4: 70. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb11040070