
Effect of Resin Infiltration on Enamel: A Systematic Review and Meta-Analysis

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Focused Question and Eligibility Criteria
- “Do infiltrative resin in sound enamel and WSLs improve the surface roughness, microhardness and shear bond strength?” and
- “What is the penetration depth capacity of the infiltrative resin in WSLs?”
- Teeth with sound enamel, and teeth with WSLs or teeth classified with ICDAS 1 or 2 (Population, P); Resin infiltration (Intervention, I); Initial condition or no treatment (Comparison, C); Disappearance or improvement of the surface roughness, microhardness, and shear bond strength (Outcome, O).
- Teeth with WSLs or teeth classified with ICDAS 1 or 2 (Population, P); Resin infiltration (Intervention, I); Not applicable (Comparison, C); Penetration depth (Outcome, O).
2.3. Search Strategy
2.4. Study Process
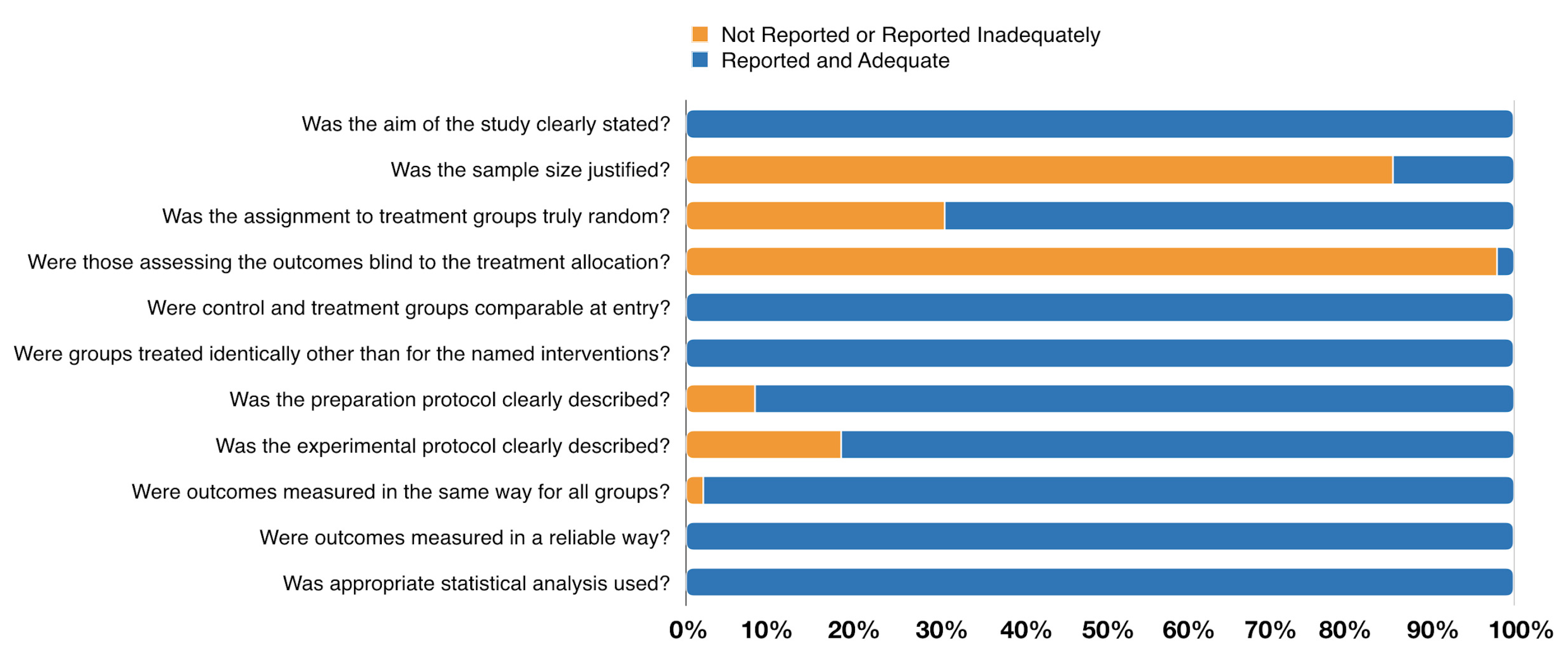
2.5. Methodological Quality Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Characteristics of the Studies

{kind=link}
{kind=link}
| Study | Funding | n | Specimen Origin | Exclusion CRITERIA | WSLs Preparation (pH for hours) | Outcome Reported |
|---|---|---|---|---|---|---|
| Pancu et al. 2011 (Romania) [42] | NR | 10 | Human (bicusps or molars) | NR | pH: 4.4 for 120 h | Microhardness (Vicker hardness- special device for microhardness testing with a squared diamond head) |
| Meyer-Lueckel et al. 2011 (Germany) [59] | DFG: PA 1508/1-1. HML and SP and royalties from DMG, Hamburg | 20 | Human (molars and premolars) | Active non-cavitated proximal WSL (ICDAS code 2) | Without demineralization | Penetration Depth (Confocal laser scanning microscopy (CLSM) |
| Paris et al. 2011 B (Germany) [62] | Institute for Immunology, UK-SH, Christian-Albrechts Universitat zu Kiel for providing the CLSM. The Charité—Universitatmedizin Berlin holds US and European patents | 19 | Human (molars and premolars) | Active non-cavitated proximal lesions scored as ICDAS 2 | Without demineralization | Penetration Depth (confocal laser scanning microscope) |
| Paris et al. 2011 A (Germeny) [64] | DFG: PA 1508/1-2, as part partially by DMG. | 16 | Human (molars) | Cavitated lesions | Without demineralization | Penetration Depth (Confocal laser scanning microscopy CLSM) |
| Taher et al. 2012 (Saudi Arabia) [47] | No | 10 | Human (premolars) | Cracks, restorations, or developmental lesions | Without demineralization | Roughness; Microhardness (microscope with 200 magnification and application of applying a load of 300 g; profilometer) |
| Torres et al. 2012 (Brazil) [48] | NR | 15 | Bovine (incisors) | Damaged or not intact enamel | pH: 5 for 16 h | Microhardness (microhardness tester fitted with a 50-g load) |
| Attin et al. 2012 (Switzerland) [32] | Dentaurum, 3M ESPE, and DMG | 12 | Bovine (incisors) | NR | pH: NR for 504 h | Shear Bond Strength (universal testing machine) |
| Veli et al. 2014 (Turkey) [72] | No | 20 | Human (premolars) | Caries, hypoplastic areas, restorations, and surface abnormalities | pH: 4.8 for 504 h | Shear Bond Strength (universal testing machine) |
| Ekizer et al. 2012 (Turkey) [70] | No | 20 | Human (premolars) | Hypoplastic spots, cracks, or gross irregularities | pH: 4.3 for 6 h | Shear Bond Strength (universal testing machine) |
| Paris et al. 2013 (Germany) [43] | DFG: PA1508/1-2. HML and SP and royalties from DMG, Hamburg. | 12 | Bovine (incisors) | NR | pH: 4.95 for 1200 h | Microhardness (Vickers hardness with a force (F) of 0.981 N for 10 s) |
| Paris et al. 2013 (Germany) [61] | DFG: PA 1508/1-1 | 15 | Human (molars and premolars) | Cavitated caries | Without demineralization | Penetration Depth (confocal laser scanning) |
| Mohammed et al. 2014 (Iraq) [76] | NR | 56 | Human (premolars) | NR | pH: 4.5 for 120 h | Roughness (profilometer) |
| Paris et al. 2014 (Germany) [63] | DFG: PA 1508/1-3 | 9 | Human (molars and premolars) | ICDAS codes 0, 1, 2 | Without demineralization | Penetration Depth (dual fluorescence confocal microscopy) |
| Lausch et al. 2014 (Germany) [57] | The Charité Universitätsmedizin Berlin and DMG | 17 | Human (molars and premolars) | Without active or cavitated WSL | Without demineralization | Penetration Depth (confocal laser scanning) |
| Gelani et al. 2014 (USA) [56] | No | 42 | Bovine (incisors) | WSP, cracks, or any other defect | pH:5 for 24 h | Penetration Depth (Confocal Laser Scanning Microscopy and Transverse Microradiography) |
| Dilber et al. 2014 (Turkey) [69] | NR | 15 | Human (mandibular lateral teeth) | Hypoplastic areas, cracks, or gross irregularities in enamel | ph:4.3 for 6 h | Shear Bond Strength (Universal testing machine) |
| Montasser et al. 2015 (Egypt) [41] | No | 10 | Human (NR) | NR | pH: 4.4 for 504 h | Microhardness (Vickers diamond indenter load of 200 g) |
| Arslan et al. 2015 (Turkey) [31] | NR | 15 | Human (central incisors) | NR | pH: 4.5 for 6 h | Roughness; Microhardness (profilometer; Vickers hardness tester with 2 N load) |
| Min et al. 2015 (South Korea) [60] | Basic Science Research Program through the National Research Foundation of Korea (2013R1A1A2062505) | 20 | Bovine (permanent anterior teeth) | NR | pH:4.8 for 960 h | Penetration Depth (Optical coherence tomography Confocal laser scanning microscopy)) |
| Vianna et al. 2015 (Brazil) [73] | No | 15 | Bovine (incisors) | NR | pH:5 for 56 h | Shear Bond Strength (universal testing machine) |
| Gurdogan et al. 2016 (Turkey) [38] | No | 20 | Bovine (incisors) | NR | pH: 4 for 2 h | Microhardness (Vickers Hardness tester with 100 gr force) |
| Abdel-Hakim et al. 2016 (Egypt) [28] | NR | 6 | Human (molars) | Caries, hypocalcifications, or restorations | pH: 4.4 for 480 h | Microhardness (Vickers michrohardness testing with 200 gm load) |
| El-zankalouny et al. 2016 (Egypt) [46] | No | 7 | Human (premolars) | Cracks, caries, or restorations | pH: 4.4 for 96 h | Microhardness; Penetration Depth (Vickers tester with f 50 g; stereomicroscope) |
| Abdellatif et al. 2016 (Egypt) [29] | NR | 11 | Human (anterior teeth) | NR | pH: 4.8 for 720 h | Microhardness (Vicker’s microhardness test with load of 200 g) |
| Baka et al. 2016 (Turkey) [52] | NR | 20 | Human (premolars) | Hypoplastic areas, cracks, restorations, or gross irregularities | pH: 4.8 for 504 h | Roughness; Shear Bond Strengths (profilometer; a universal testing machine) |
| Neto et al. 2016 (Brazil) [30] | CAPES, Funcap, and CNPq (Brazilian agencies). Project PON 254/Ric | 10 | Human (molars) | NR | pH: 4.9 for 16 h | Microhardness (Knoop microhardness) |
| Horuztepe et al. 2017 (Turkey) [39] | No | 45 | Bovine (incisors) | Cracks or other surface defects | pH: 4.95 for 672 h | Microhardness (microindentation hardness tester with a 50-g load) |
| Mandava et al. 2017 (India) [40] | No | 20 | Human (maxillary central incisors) | Presence of cracks and defects | pH: 4.4 for 96 h | Microhardness; Penetration Depth (Vicker’s microhardness tester with a 300 g load; confocal laser fluorescence microscope) |
| Aziznezhad et al. 2017 (Iran) [34] | Babol University grant | 10 | Human (premolars) | Not intact and time of extraction more than 3 months | pH: 4.5 for 6 h | Microhardness (Vickers device with 500 g load) |
| Prajapati et al. 2017 (India) [44] | No | 10 | Human (premolars) | Teeth with hypoplasia or incipient carious lesions/WSL | pH:4.4 for 504 h | Microhardness (Vickers microhardness tester with 100 g load) |
| Sava-Rosianu et al. 2017 (Romania) [65] | Project for young researchers—Programme II-C3-TC-2015 | 60 | Human (premolar) | NR | NR | Penetration Depth (Confocal Laser Scanning Microscopy) |
| Attia et al. 2018 (Egypt) [77] | NR | 20 | Bovine (NR) | Cracks or defects in the surface | pH:5 for 24 h | Microhardness (micro-indentation hardness tester (with a 50-g load) |
| Nabil et al. 2018 (Egypt) [27] | NR | 15 | Human (anterior teeth) | Cracks and any developmental defects | pH: NR for 1 h | Roughness; Microhardness (profilometer; Vickers Tester with load of 200 g) |
| Enan et al. 2018 (Egypt) [37] | NR | 10 | Human (bicuspid) | Cracks and defects | pH: 4.95 for 160 h | Roughness; Microhardness (profilometer; universal testing machine) |
| Khalid et al. 2018 (Indonesia) [54] | University of Indonesia | 10 | Human (premolars) | Enamel surface that was attached orthodontic appliance; WSL, defects on the buccal side of enamel; restorations | Without demineralization | Roughness (profilometer) |
| Yazkan et al. 2018 (Turkey) [49] | Suleyman Demirel University Scientific Research Projects Foundation (2969-D-11) | 16 | Bovine (incisors) | Caries, fracture, or other defects | pH: 5 for 240 h | Roughness; Microhardness (profilometer; Vickers indenter, with load of 200 g) |
| Askar et al. 2018 (Germany) [55] | Deutsche Forschungsgemeinschaft (DFG; PA 1508/1-3), and DMG | 15 | Human (NR) | Active proximal lesions with ICDAS-2, 3 and 5 | Without demineralization | Penetration Depth (confocal microscopy) |
| Aswani et al. 2019 (India) [51] | No | 10 | Human (anterior teeth) | NR | pH:4.4 for 144 h | Roughness (profilometer) |
| Enan et al. 2019 (Egypt) [53] | No | 30 | Human (premolars) | NR | pH:4.95 for 160 h | Roughness (profilometer) |
| Arora et al. 2019 (India) [50] | No | 30 | Bovine (premolars) | Caries | pH: 4.5 for 96 h | Roughness; Penetration Depth (optical profilometer) |
| Theodory et al. 2019 (USA) [66] | Student Government for Graduate and Professional Students at the University of Iowa | 15 | Human (molars) | NR | pH: 4.3 for 2160 h | Penetration Depth (Confocal Laser Scanning Microscopy) |
| López et al. 2019 (Brazil) [59] | NR | 8 | Human (NR) | Cavity lesions, white stains, cracks, or structural alterations and restorations | pH: 5 for 0.5 h | Penetration Depth (Confocal Laser Scanning Microscopy) |
| Gulec et al. 2019 (Turkey) [71] | NR | 20 | Human (premolars) | Caries, attrition, fracture, restoration, congenital or surface anomalies, or surface | pH: 4.5 for 22 h | Shear Bond Strength (universal testing machine) |
| Borges et al. 2019 (Brazil) [68] | FAPESP(2010/16878-7, 2010/17757-9) | 30 | Bovine (incisors) | NR | pH:5 for 16 h | Shear Bond Strength (Scanning electron microscopy (SEM)) |
| Ayad et al. 2020 (Egypt) [33] | NR | 7 | Bovine (anteriors) | NR | pH: 4.4 for 96 h | Microhardness (Vickers indenter, with a static load of 200 g) |
| Behrouzi P et al. 2020 (Iran) [35] | No | 15 | Human (maxillary central incisors) | Cracks, caries, or mineralization defects | pH: 4.5 for 96 h | Microhardness (Vickers hardness tester with 50 kg load) |
| El Meligy, 2020 (Saudi Arabia) [36] | No | 27 | Human (premolars) | ICDAS 1 and 2 | pH: 4.5 for 399 h | Microhardness (transversal Vickers hardness with a force of 0.891 N) |
| Wang et al. 2020 (Brazil) [67] | FAPESP, 2012/13160-3, #2012/18579-2 and 2013/23310-5) CAPES—Brasil | 13 | Bovine (incisors) | NR | pH: 4.7 for 168 h | Penetration Depth (confocal laser scanning microscopy) |
3.3. Methodological Quality of the Included Studies
3.4. Clinical Measures
3.4.1. Enamel Surface Roughness
3.4.2. Enamel Microhardness
3.4.3. Shear Bond Strength
3.4.4. Penetration Depth in Caries Lesions
4. Discussion
4.1. Summary of the Main Results
4.2. Quality of the Evidence and Potential Biases in the Review Process
4.3. Agreements and Disagreements with Other Reviews or Studies and Clinical Relevance
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dorri, M.; Martinez-Zapata, M.J.; Walsh, T.; Marinho, V.C.; Sheiham deceased, A.; Zaror, C. Atraumatic Restorative Treatment versus Conventional Restorative Treatment for Managing Dental Caries. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [Green Version]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global Burden of Untreated Caries: A Systematic Review and Metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Bishara, S.E.; Ostby, A.W. White Spot Lesions: Formation, Prevention, and Treatment. Semin. Orthod. 2008, 14, 174–182. [Google Scholar] [CrossRef]
- Heymann, G.C.; Grauer, D. A Contemporary Review of White Spot Lesions in Orthodontics: White Spot Lesions in Orthodontics. J. Esthet. Restor. Dent. 2013, 25, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Julien, K.C.; Buschang, P.H.; Campbell, P.M. Prevalence of White Spot Lesion Formation during Orthodontic Treatment. Angle Orthod. 2013, 83, 641–647. [Google Scholar] [CrossRef]
- Sangamesh, B.; Kallury, A. Iatrogenic Effects of Orthodontic Treatment—Review on White Spot Lesions. Int. J. Sci. Eng. Res. 2011, 2, 2–16. [Google Scholar]
- Black, G.V. Operative Dentistry: The Pathology of the Hard Tissues of the Teeth, 1st ed.; Medico-Dnetal Publishing: Chicago, IL, USA, 1908. [Google Scholar]
- Gorelick, L.; Geiger, A.M.; Gwinnett, A.J. Incidence of White Spot Formation after Bonding and Banding. Am. J. Orthod. 1982, 81, 93–98. [Google Scholar] [CrossRef]
- Tufekci, E.; Dixon, J.S.; Gunsolley, J.C.; Lindauer, S.J. Prevalence of White Spot Lesions during Orthodontic Treatment with Fixed Appliances. Angle Orthod. 2011, 81, 206–210. [Google Scholar] [CrossRef] [Green Version]
- Prevalence of White-Spot Lesions before and during Orthodontic Treatment with Fixed Appliances | European Journal of Orthodontics | Oxford Academic. Available online: https://0-academic-oup-com.brum.beds.ac.uk/ejo/article/35/5/664/495801 (accessed on 12 June 2021).
- Sundararaj, D.; Venkatachalapathy, S.; Tandon, A.; Pereira, A. Critical Evaluation of Incidence and Prevalence of White Spot Lesions during Fixed Orthodontic Appliance Treatment: A Meta-Analysis. J. Int. Soc. Prev. Community Dent. 2015, 5, 433–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urquhart, O.; Tampi, M.P.; Pilcher, L.; Slayton, R.L.; Araujo, M.W.B.; Fontana, M.; Guzmán-Armstrong, S.; Nascimento, M.M.; Nový, B.B.; Tinanoff, N.; et al. Nonrestorative Treatments for Caries: Systematic Review and Network Meta-Analysis. J. Dent. Res. 2019, 98, 14–26. [Google Scholar] [CrossRef]
- Giudice, G.L.; Lipari, F.; Lizio, A.; Cervino, G.; Cicciù, M. Tooth Fragment Reattachment Technique on a Pluri Traumatized Tooth. J. Conserv. Dent. JCD 2012, 15, 80–83. [Google Scholar] [CrossRef] [Green Version]
- Jobim Jardim, J.; Henz, S.; Barbachan, E.; Silva, B. Restorative Treatment Decisions in Posterior Teeth: A Systematic Review. Oral Health Prev. Dent. 2017, 15, 107–115. [Google Scholar] [CrossRef]
- Abdullah, Z.; John, J. Minimally Invasive Treatment of White Spot Lesions—A Systematic Review. Oral Health Prev. Dent. 2016, 14, 197–205. [Google Scholar] [CrossRef]
- Bhat, S.; Hegde, S.; Bhat, V.; Ramya, K.; Jodalli, P. Assessment of Maternal Risk Factors and Its Relationship with Early Childhood Caries among Preschool Children in Mangaluru City. J. Indian Soc. Pedod. Prev. Dent. 2017, 35, 193. [Google Scholar] [CrossRef]
- Domöjean, S.; Ducamp, R.; Löger, S.; Holmgren, C. Resin Infiltration of Non-Cavitated Caries Lesions: A Systematic Review. Med. Princ. Pract. 2015, 24, 216–221. [Google Scholar] [CrossRef]
- Meyer-Lueckel, H.; Paris, S.; Kielbassa, A.M. Surface Layer Erosion of Natural Caries Lesions with Phosphoric and Hydrochloric Acid Gels in Preparation for Resin Infiltration. Caries Res. 2007, 41, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Dorri, M.; Dunne, S.M.; Walsh, T.; Schwendicke, F. Micro-Invasive Interventions for Managing Proximal Dental Decay in Primary and Permanent Teeth. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Zakizade, M.; Davoudi, A.; Akhavan, A.; Shirban, F. Effect of Resin Infiltration Technique on Improving Surface Hardness of Enamel Lesions: A Systematic Review and Meta-Analysis. J. Evid. Based Dent. Pract. 2020, 20, 101405. [Google Scholar] [CrossRef] [PubMed]
- Borges, A.B.; Caneppele, T.M.F.; Masterson, D.; Maia, L.C. Is Resin Infiltration an Effective Esthetic Treatment for Enamel Development Defects and White Spot Lesions? A Systematic Review. J. Dent. 2017, 56, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aminoshariae, A.; Kulild, J. Master Apical File Size—Smaller or Larger: A Systematic Review of Microbial Reduction. Int. Endod. J. 2015, 48, 1007–1022. [Google Scholar] [CrossRef]
- Dos Reis-Prado, A.H.; Abreu, L.G.; Tavares, W.L.F.; da Cunha Peixoto, I.F.; Viana, A.C.D.; de Oliveira, E.M.C.; Bastos, J.V.; Ribeiro-Sobrinho, A.P.; Benetti, F. Comparison between Immediate and Delayed Post Space Preparations: A Systematic Review and Meta-Analysis. Clin. Oral Investig. 2021, 25, 417–440. [Google Scholar] [CrossRef] [PubMed]
- Ethem Yaylali, I.; Kececi, A.D.; Ureyen Kaya, B. Ultrasonically Activated Irrigation to Remove Calcium Hydroxide from Apical Third of Human Root Canal System: A Systematic Review of In Vitro Studies. J. Endod. 2015, 41, 1589–1599. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the Mean and Variance from the Median, Range, and the Size of a Sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- AL Again, N.A.; Atta, M.S.; Alhady, A.A.A. The Effect of Caries Infiltration Technique (Icons) on Surface Roughness and Microhardness of Enamel White Spot Lesions. Al-Azhar J. Dent. Sci. 2018, 21, 79–86. [Google Scholar] [CrossRef]
- Abdel-Hakim, S.; Metwalli, N.; El-Askary, F.; Wassel, M. Microhardness, sem and color change analysis of artificial enamel lesions in primary teeth treated with resin infiltration, cpp-acp or fluoride gel: An in vitro study. Egypt. Dent. J. 2016, 62, 3735–3744. [Google Scholar]
- Abdellatif, A.; Shalan, H.; Elsebaai, A. Effects of Resin Application on White Spot Lesions (Laboratory Study). J. Clin. Pediatr. Dent. 2016, 46, 120–126. [Google Scholar]
- Andrade Neto, D.M.; Carvalho, E.V.; Rodrigues, E.A.; Feitosa, V.P.; Sauro, S.; Mele, G.; Carbone, L.; Mazzetto, S.E.; Rodrigues, L.K.; Fechine, P.B.A. Novel Hydroxyapatite Nanorods Improve Anti-Caries Efficacy of Enamel Infiltrants. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2016, 32, 784–793. [Google Scholar] [CrossRef] [PubMed]
- Arslan, S.; Zorba, Y.O.; Atalay, M.A.; Özcan, S.; Demirbuga, S.; Pala, K.; Percin, D.; Ozer, F. Effect of Resin Infiltration on Enamel Surface Properties and Streptococcus Mutans Adhesion to Artificial Enamel Lesions. Dent. Mater. J. 2015, 34, 25–30. [Google Scholar] [CrossRef] [Green Version]
- Attin, R.; Stawarczyk, B.; Keçik, D.; Knösel, M.; Wiechmann, D.; Attin, T. Shear Bond Strength of Brackets to Demineralize Enamel after Different Pretreatment Methods. Angle Orthod. 2012, 82, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Ayad, A.; Mustafa, D.; Nour, K. Effect of Remineralizing Agents and Resin Infiltration on Resistance to Demineralization of Artificial Enamel Lesions. Egypt. Dent. J. 2020, 66, 2763–2771. [Google Scholar] [CrossRef]
- Aziznezhad, M.; Alaghemand, H.; Shahande, Z.; Pasdar, N.; Bijani, A.; Eslami, A.; Dastan, Z. Comparison of the Effect of Resin Infiltrant, Fluoride Varnish, and Nano-Hydroxy Apatite Paste on Surface Hardness and Streptococcus Mutans Adhesion to Artificial Enamel Lesions. Electron. Physician 2017, 9, 3934–3942. [Google Scholar] [CrossRef] [Green Version]
- Behrouzi, P.; Heshmat, H.; Hoorizad Ganjkar, M.; Tabatabaei, S.F.; Kharazifard, M.J. Effect of Two Methods of Remineralization and Resin Infiltration on Surface Hardness of Artificially Induced Enamel Lesions. J. Dent. Shiraz Iran 2020, 21, 12–17. [Google Scholar] [CrossRef]
- El Meligy, O.A.E.S.; Alamoudi, N.M.; Eldin Ibrahim, S.T.; Felemban, O.M.; Al-Tuwirqi, A.A. Effect of Resin Infiltration Application on Early Proximal Caries Lesions in Vitro. J. Dent. Sci. 2021, 16, 296–303. [Google Scholar] [CrossRef]
- Enan, E.T.; Tawfik, M.A.; Ali, A.I.; Anan, A.T. Surface properties of resin-infiltrated incipient enamel lesions after aging under thermal stresses. Egypt. Dent. J. 2018, 64, 2833–2840. [Google Scholar] [CrossRef] [Green Version]
- Gurdogan, E.B.; Ozdemir-Ozenen, D.; Sandalli, N. Evaluation of Surface Roughness Characteristics Using Atomic Force Microscopy and Inspection of Microhardness Following Resin Infiltration with Icon®. J. Esthet. Restor. Dent. Off. Publ. Am. Acad. Esthet. Dent. Al 2017, 29, 201–208. [Google Scholar] [CrossRef]
- Horuztepe, S.A.; Baseren, M. Effect of Resin Infiltration on the Color and Microhardness of Bleached White-Spot Lesions in Bovine Enamel (an in vitro Study). J. Esthet. Restor. Dent. Off. Publ. Am. Acad. Esthet. Dent. Al 2017, 29, 378–385. [Google Scholar] [CrossRef]
- Mandava, J.; Reddy, Y.S.; Kantheti, S.; Chalasani, U.; Ravi, R.C.; Borugadda, R.; Konagala, R.K. Microhardness and Penetration of Artificial White Spot Lesions Treated with Resin or Colloidal Silica Infiltration. J. Clin. Diagn. Res. JCDR 2017, 11, ZC142–ZC146. [Google Scholar] [CrossRef]
- Montasser, M.A.; El-Wassefy, N.A.; Taha, M. In Vitro Study of the Potential Protection of Sound Enamel against Demineralization. Prog. Orthod. 2015, 16, 12. [Google Scholar] [CrossRef] [Green Version]
- Pancu, G.; Andrian, S.; Iovan, G.; Ghiorghe, A.; Topoliceanu, C.; Moldovanu, A.; Georgescu, A.; Pancu, I.; Stoleriu, S. Study regarding the assessment of enamel microhardness in incipient carious lesions treated by icon method. Rom. J. Oral Rehabil. 2011, 3, 94–100. [Google Scholar]
- Paris, S. Micro-Hardness and Mineral Loss of Enamel Lesions after Infiltration with Various Resins: Influence of Infiltrant Composition and Application Frequency in Vitro—ScienceDirect. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/abs/pii/S0300571213000869 (accessed on 10 March 2021).
- Prajapati, D.; Nayak, R.; Pai, D.; Upadhya, N.; Bhaskar, V.K.; Kamath, P. Effect of Resin Infiltration on Artificial Caries: An in Vitro Evaluation of Resin Penetration and Microhardness. Int. J. Clin. Pediatr. Dent. 2017, 10, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Qasim, A. Assessement of White Spot Treated with (ICON) and Flouride Gel (An In Vitro Study). Int. J. Enhanc. Res. Sci. Technol. Eng. 2014, 3, 1–6. [Google Scholar]
- El-zankalouny Shimaa, M.; Abd El Fattah Wegdan, M.; El-Shabrawy Sonia, M. Penetration depth and enamel microhardness of resin infiltrant and traditional techniques for treatment of artificial enamel lesions. Alex. Dent. J. 2016, 41, 20–25. [Google Scholar] [CrossRef]
- Taher, N.M.; Alkhamis, H.A.; Dowaidi, S.M. The Influence of Resin Infiltration System on Enamel Microhardness and Surface Roughness: An in Vitro Study. Saudi Dent. J. 2012, 24, 79–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, C.R.G.; Rosa, P.C.F.; Ferreira, N.S.; Borges, A.B. Effect of Caries Infiltration Technique and Fluoride Therapy on Microhardness of Enamel Carious Lesions. Oper. Dent. 2012, 37, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Yazkan, B.; Ermis, R.B. Effect of Resin Infiltration and Microabrasion on the Microhardness, Surface Roughness and Morphology of Incipient Carious Lesions. Acta Odontol. Scand. 2018, 76, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Arora, T.C.; Arora, D.; Tripathi, A.M.; Yadav, G.; Saha, S.; Dhinsa, K. An In-Vitro Evaluation of Resin Infiltration System and Conventional Pit and Fissure Sealant on Enamel Properties in White Spot Lesions. J. Indian Soc. Pedod. Prev. Dent. 2019, 37, 133–139. [Google Scholar] [CrossRef]
- Aswani, R.; Chandrappa, V.; Uloopi, K.; Chandrasekhar, R.; RojaRamya, K.S. Resin Infiltration of Artificial Enamel Lesions: Evaluation of Penetration Depth, Surface Roughness and Color Stability. Int. J. Clin. Pediatr. Dent. 2019, 12, 520–523. [Google Scholar] [CrossRef]
- Baka, Z.M.; Akin, M.; Ileri, Z.; Basciftci, F.A. Effects of Remineralization Procedures on Shear Bond Strengths of Brackets Bonded to Demineralized Enamel Surfaces with Self-Etch Systems. Angle Orthod. 2016, 86, 661–667. [Google Scholar] [CrossRef]
- Enan, E.T.; Aref, N.S.; Hammad, S.M. Resistance of Resin-Infiltrated Enamel to Surface Changes in Response to Acidic Challenge. J. Esthet. Restor. Dent. Off. Publ. Am. Acad. Esthet. Dent. Al 2019, 31, 353–358. [Google Scholar] [CrossRef]
- Khalid, I.; Anggani, H.S.; Ismah, N. Differences in Enamel Surface Roughness Changes after Debonding Using Resin Infiltration System and Nano-Filled Resin Coating. J. Int. Dent. Med. Res. 2019, 12, 95–100. [Google Scholar]
- Askar, H.; Schwendicke, F.; Lausch, J.; Meyer-Lueckel, H.; Paris, S. Modified Resin Infiltration of Non-, Micro- and Cavitated Proximal Caries Lesions in Vitro. J. Dent. 2018, 74, 56–60. [Google Scholar] [CrossRef]
- Gelani, R.; Zandona, A.F.; Lippert, F.; Kamocka, M.M.; Eckert, G. In Vitro Progression of Artificial White Spot Lesions Sealed with an Infiltrant Resin. Oper. Dent. 2014, 39, 481–488. [Google Scholar] [CrossRef]
- Lausch, J.; Paris, S.; Selje, T.; Dörfer, C.E.; Meyer-Lueckel, H. Resin Infiltration of Fissure Caries with Various Techniques of Pretreatment in Vitro. Caries Res. 2015, 49, 50–55. [Google Scholar] [CrossRef] [PubMed]
- López López, E.A.; Dominguez, J.A.; Gomes, G.M.; Mora, C.A.P.; Bittencourt, B.F.; Gomes, J.C.; Gomes, O.M.M. Effect of Conditioning Protocols and Ultrasonic Application of an Infiltrant Resin in White Spot Lesions. Braz. Dent. J. 2019, 30, 58–65. [Google Scholar] [CrossRef] [Green Version]
- Meyer-Lueckel, H.; Chatzidakis, A.; Naumann, M.; Dörfer, C.E.; Paris, S. Influence of Application Time on Penetration of an Infiltrant into Natural Enamel Caries. J. Dent. 2011, 39, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Min, J.H.; Inaba, D.; Kwon, H.K.; Chung, J.H.; Kim, B.I. Evaluation of Penetration Effect of Resin Infiltrant Using Optical Coherence Tomography. J. Dent. 2015, 43, 720–725. [Google Scholar] [CrossRef]
- Paris, S.; Soviero, V.M.; Schuch, M.; Meyer-Lueckel, H. Pretreatment of Natural Caries Lesions Affects Penetration Depth of Infiltrants in Vitro. Clin. Oral Investig. 2013, 17, 2085–2089. [Google Scholar] [CrossRef]
- Paris, S.; Bitter, K.; Naumann, M.; Dörfer, C.E.; Meyer-Lueckel, H. Resin Infiltration of Proximal Caries Lesions Differing in ICDAS Codes. Eur. J. Oral Sci. 2011, 119, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Paris, S.; Lausch, J.; Selje, T.; Dörfer, C.E.; Meyer-Lueckel, H. Comparison of Sealant and Infiltrant Penetration into Pit and Fissure Caries Lesions in Vitro. J. Dent. 2014, 42, 432–438. [Google Scholar] [CrossRef]
- Paris, S.; Soviero, V.M.; Seddig, S.; Meyer-Lueckel, H. Penetration Depths of an Infiltrant into Proximal Caries Lesions in Primary Molars after Different Application Times in Vitro. Int. J. Paediatr. Dent. 2011, 22, 349–355. [Google Scholar] [CrossRef]
- Sava-rosianu, R.; Podariu, A.; Negrutiu, M.; Szuhanek, C.; Sinescu, C. Low Viscosity Resin Penetration Degree in Incipient Caries Lesions. Rev. Chim. 2017, 68, 2588–2592. [Google Scholar] [CrossRef]
- Theodory, T.G.; Kolker, J.L.; Vargas, M.A.; Maia, R.R.; Dawson, D.V. Masking and Penetration Ability of Various Sealants and ICON in Artificial Initial Caries Lesions In Vitro. J. Adhes. Dent. 2019, 21, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; de Almendra Freitas, M.C.C.; Prakki, A.; Mosquim, V.; González, A.H.M.; Rios, D.; Honório, H.M. Experimental Self-Etching Resin Infiltrants on the Treatment of Simulated Carious White Spot Lesions. J. Mech. Behav. Biomed. Mater. 2021, 113, 104146. [Google Scholar] [CrossRef] [PubMed]
- Borges, A.B.; Abu Hasna, A.; Matuda, A.G.N.; Lopes, S.R.; Mafetano, A.P.V.P.; Arantes, A.; Duarte, A.F.; Barcellos, D.C.; Torres, C.R.G.; Pucci, C.R. Adhesive Systems Effect over Bond Strength of Resin-Infiltrated and de/Remineralized Enamel. F1000Research 2019, 8, 1743. [Google Scholar] [CrossRef]
- Dilber, E.; Akın, M.; Yavuz, T.; Erdem, A. Effects of Different Demineralization-Inhibiting Methods on the Shear Bond Strength of Glass-Ceramics. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2015, 24, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Ekizer, A.; Zorba, Y.O.; Uysal, T.; Ayrikcila, S. Effects of Demineralizaton-Inhibition Procedures on the Bond Strength of Brackets Bonded to Demineralized Enamel Surface. Korean J. Orthod. 2012, 42, 17–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gulec, A. Assessment of the Resin Infiltration and CPP-ACP Applications before Orthodontic Brackets Bonding—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/31434834/ (accessed on 11 March 2021).
- Velİ, I.; Akin, M.; Baka, Z.M.; Uysal, T. Effects of Different Pre-Treatment Methods on the Shear Bond Strength of Orthodontic Brackets to Demineralized Enamel. Acta Odontol. Scand. 2016, 74, 7–13. [Google Scholar] [CrossRef]
- Vianna, J.S.; Marquezan, M.; Lau, T.C.L.; Sant’Anna, E.F. Bonding Brackets on White Spot Lesions Pretreated by Means of Two Methods. Dent. Press J. Orthod. 2016, 21, 39–44. [Google Scholar] [CrossRef] [Green Version]
- Paris, S.; Schwendicke, F.; Keltsch, J.; Dörfer, C.; Meyer-Lueckel, H. Masking of White Spot Lesions by Resin Infiltration in Vitro. J. Dent. 2013, 41, e28–e34. [Google Scholar] [CrossRef] [PubMed]
- Paris, S.; Meyer-Lueckel, H. Resin Infiltration after Enamel Etching. In Tooth Whitening; Perdigão, J., Ed.; Springer International Publishing: Cham, Switzerland, 2016; pp. 211–222. ISBN 978-3-319-38847-2. [Google Scholar]
- Mohamed, A.M.; Wong, K.H.; Lee, W.J.; Marizan Nor, M.; Mohd Hussaini, H.; Rosli, T.I. In Vitro Study of White Spot Lesion: Maxilla and Mandibular Teeth. Saudi Dent. J. 2018, 30, 142–150. [Google Scholar] [CrossRef]
- Attia, R.M. Effect of PH Challenge on the Micro-Hardness of Artificially Induced de-Mineralized Enamel Treated with Resin Infiltrant and Fluoride Varnish. Egypt. Dent. J. 2018, 64, 2841–2850. [Google Scholar] [CrossRef]
- Wong, A.; Subar, P.E.; Young, D.A. Dental Caries. Adv. Pediatr. 2017, 64, 307–330. [Google Scholar] [CrossRef] [PubMed]
- Abou Neel, E.A.; Aljabo, A.; Strange, A.; Ibrahim, S.; Coathup, M.; Young, A.M.; Bozec, L.; Mudera, V. Demineralization–Remineralization Dynamics in Teeth and Bone. Int. J. Nanomed. 2016, 11, 4743–4763. [Google Scholar] [CrossRef] [PubMed]
- Ten Cate, J.M.; Featherstone, J.D.B. Mechanistic Aspects of the Interactions Between Fluoride and Dental Enamel. Crit. Rev. Oral Biol. Med. 1991, 2, 283–296. [Google Scholar] [CrossRef]
- Neres, É.; Moda, M.; Chiba, E.; Briso, A.; Pessan, J.; Fagundes, T. Microhardness and Roughness of Infiltrated White Spot Lesions Submitted to Different Challenges. Oper. Dent. 2017, 42, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, S.T. Analysis of Dental Shear Bond Strength Tests, Shear or Tensile? Int. J. Adhes. Adhes. 1996, 16, 147–154. [Google Scholar] [CrossRef]
- Nakabayashi, N.; Nakamura, M.; Yasuda, N. Hybrid Layer as a Dentin-Bonding Mechanism. J. Esthet. Dent. 1991, 3, 133–138. [Google Scholar] [CrossRef]
- Perdigão, J. Resin Infiltration of Enamel White Spot Lesions: An Ultramorphological Analysis. J. Esthet. Restor. Dent. Off. Publ. Am. Acad. Esthet. Dent. Al 2020, 32, 317–324. [Google Scholar] [CrossRef]
- Yassen, G.H.; Platt, J.A.; Hara, A.T. Bovine Teeth as Substitute for Human Teeth in Dental Research: A Review of Literature. J. Oral Sci. 2011, 53, 273–282. [Google Scholar] [CrossRef] [Green Version]
- Arends, J.; Jongebloed, W.L. Crystallites Dimensions of Enamel. J. Biol. Buccale 1978, 6, 161–171. [Google Scholar]
- Mellberg, J.R. Hard-Tissue Substrates for Evaluation of Cariogenic and Anti-Cariogenic Activity in Situ. J. Dent. Res. 1992, 71, 913–919. [Google Scholar] [CrossRef] [PubMed]
- Feagin, F.; Koulourides, T.; Pigman, W. The Characterization of Enamel Surface Demineralization, Remineralization, and Associated Hardness Changes in Human and Bovine Material. Arch. Oral Biol. 1969, 14, 1407–1417. [Google Scholar] [CrossRef]
- Hara, A.T.; Queiroz, C.S.; Paes Leme, A.F.; Serra, M.C.; Cury, J.A. Caries Progression and Inhibition in Human and Bovine Root Dentine in Situ. Caries Res. 2003, 37, 339–344. [Google Scholar] [CrossRef]
- Rüttermann, S.; Braun, A.; Janda, R. Shear Bond Strength and Fracture Analysis of Human vs. Bovine Teeth. PLoS ONE 2013, 8, e59181. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Variable | n Studies | ROM | 95% CI | p-Value | I2 (%) | Egger Test |
|---|---|---|---|---|---|---|
| Surface roughness | ||||||
| Sound Enamel | 5 | 0.65 | 0.49; 0.85 | 0.0021 | 98.2 | - |
| WSL | 8 | 0.46 | 0.29; 0.74 | 0.0012 | 98.5 | - |
| Enamel microhardness | ||||||
| Sound Enamel | 14 | 0.76 | 0.73; 0.8 | <0.0001 | 99.1 | 0.8893 |
| WSL | 23 | 1.68 | 1.51;1.86 | <0.0001 | 99.8 | 0.1352 |
| Shear Bond strength | ||||||
| Sound Enamel | 6 | 0.75 | 0.60; 0.95 | <0.0001 | 96.9 | - |
| WSL | 8 | 1.89 | 1.28; 2.79 | <0.0001 | 99.8 | - |
| Penetration depth | ||||||
| Sound Enamel | 15 | 65.39 | 56.11; 74.66 | 0.01 | 100.0 | 0.4712 |
| Specimen Origin | n | B | 95% CI | I2 (%) | p-Value |
|---|---|---|---|---|---|
| Surface Roughness of Sound Enamel | |||||
| Human | 4 | 0.65 | 0.49; 0.85 | 98.8 | - |
| Bovine | 0 | - | - | - | |
| Surface Roughness of WSL | |||||
| Human | 8 | 0.46 | 0.29; 0.74 | 98.5 | - |
| Bovine | 0 | - | - | - | |
| Enamel Microhardness of Sound Enamel | |||||
| Human | 8 | 0.58 | 0.46; 0.72 | 99.0 | 0.0188 |
| Bovine | 6 | 0.80 | 0.69; 0.92 | 99.3 | |
| Enamel Microhardness of WSL | |||||
| Human | 15 | 1.59 | 1.29; 1.96 | 99.5 | 0.1375 |
| Bovine | 8 | 1.96 | 1.64; 2.34 | 99.4 | |
| Shear Bond Strength of Sound Enamel | |||||
| Human | 4 | 0.75 | 0.57; 0.99 | 97.2 | 0.9958 |
| Bovine | 2 | 0.75 | 0.41; 1.37 | 97.7 | |
| Shear Bond Strength of WSL | |||||
| Human | 5 | 1.74 | 1.14: 2.65 | 98.7 | 0.6221 |
| Bovine | 3 | 2.20 | 0.93: 5.29 | 98.8 | |
| Penetration Depth | |||||
| Human | 20 | 63.65 | 52.21; 75.09 | 99.3 | 0.5589 |
| Bovine | 6 | 71.22 | 48.57; 93.87 | 99.8 | |
| ICDAS | 16 | 62.37 | 46.12; 78.61 | 99.2 | 0.4500 |
| WSLs | 10 | 70.29 | 57.68;82.90 | 99.7 | |
| Application of infiltrate for less than 1 min | 4 | 49.17 | 33.36; 64.97 | 94.1 | 0.0270 |
| Application of infiltrate for 3 min | 18 | 65.36 | 55.77; 74.96 | 99.4 | |
| Application of infiltrate for 5 min | 4 | 81.45 | 63.88; 99.01 | 96.5 | |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Charateristics | B | 95% CI | p-Value | B | 95% CI | p-Value |
| Surface roughness of WSLs | ||||||
| pH | −0.51 | −2.96; 1.93 | 0.6806 | −1.37 | −2.32; −0.42 | 0.00451 |
| Demineralization time (hours) | 0.00 | −0.00; 0.01 | 1.8929 | 0.01 | 0.00; 0.01 | <0.0001 |
| Enamel microhardness of WSLs | ||||||
| pH | 0.42 | −3.42; 0.67 | 0.0641 | 0.42 | −0.03; 0.00 | 0.0647 |
| Demineralization time (hours) | 0.00 | −0.01; 0.00 | 0.6230 | 0.00 | −0.01; 0.00 | 0.8729 |
| Shear Bond Strength of WSLs | ||||||
| pH | −0.59 | −6.98; 7.62 | 0.9781 | −0.60 | −2.02; 0.82 | 0.4098 |
| Demineralization time (hours) | 0.00 | 0.00; 0.01 | 0.0015 | 0.00 | 0.00; 0.01 | 0.0120 |
| Penetration depth of WSLs | ||||||
| pH | −6.24 | −54.77; 42.29 | 0.8010 | −33.63 | −0.88; 290.10 | 0.0432 |
| Demineralization time (hours) | 0.00 | −0.02; 0.02 | 0.9969 | 0.00 | −0.01; 0.01 | 0.8542 |
| Time of application of resin infiltrate (minutes) | 7.68 | 1.17; 14.18 | 0.0207 | 24.12 | 13.16; 35.07 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soveral, M.; Machado, V.; Botelho, J.; Mendes, J.J.; Manso, C. Effect of Resin Infiltration on Enamel: A Systematic Review and Meta-Analysis. J. Funct. Biomater. 2021, 12, 48. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb12030048
Soveral M, Machado V, Botelho J, Mendes JJ, Manso C. Effect of Resin Infiltration on Enamel: A Systematic Review and Meta-Analysis. Journal of Functional Biomaterials. 2021; 12(3):48. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb12030048
Chicago/Turabian StyleSoveral, Madalena, Vanessa Machado, João Botelho, José João Mendes, and Cristina Manso. 2021. "Effect of Resin Infiltration on Enamel: A Systematic Review and Meta-Analysis" Journal of Functional Biomaterials 12, no. 3: 48. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb12030048