
Physiological and Psychological Responses to Three Distinct Exercise Training Regimens Performed in an Outdoor Setting: Acute and Delayed Response

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
2.3. Procedures
2.3.1. Preliminary Assessments
Body Composition
20-m Shuttle Run Test
Familiarization
Exercise Protocols
2.3.2. Physiological and Psychological Assessments in the Three Exercise Protocols
External and Internal Load
HR Recovery (HRR)
Blood Lactate Concentration
Affective Valence, Rating of Perceived Exertion, and Enjoyment
2.3.3. Acute and Delayed Recovery Response
Heart Rate Variability (HRV)
Neuromuscular Function
Hooper Index
Incidental PA
Sleep
2.4. Statistical Analysis
3. Results
3.1. External and Internal Load
3.1.1. HR
3.1.2. HRR and Blood Lactate
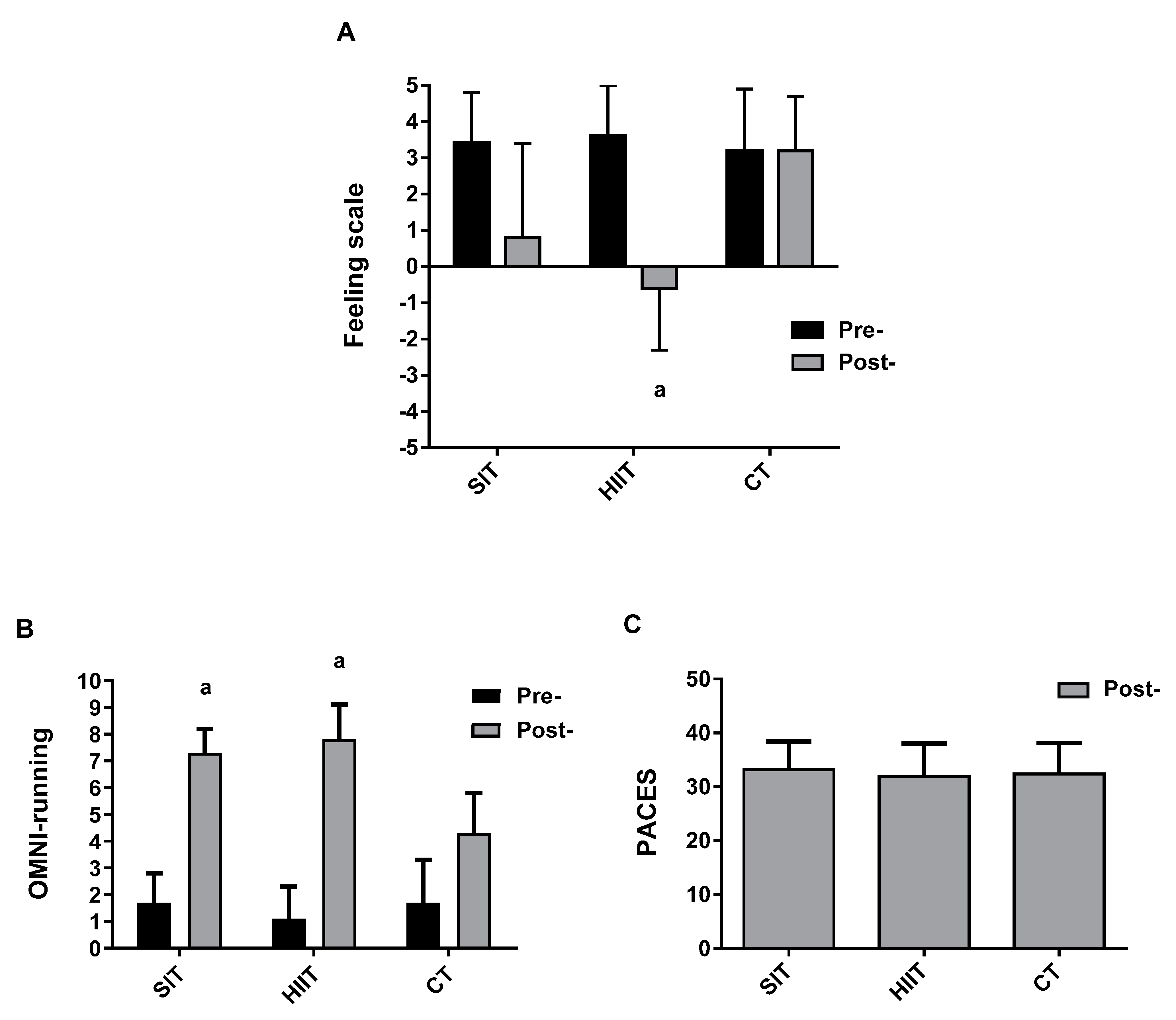
3.1.3. Affective Valence, Perceived Exertion, and Enjoyment
3.2. Acute and Delayed Recovery Response
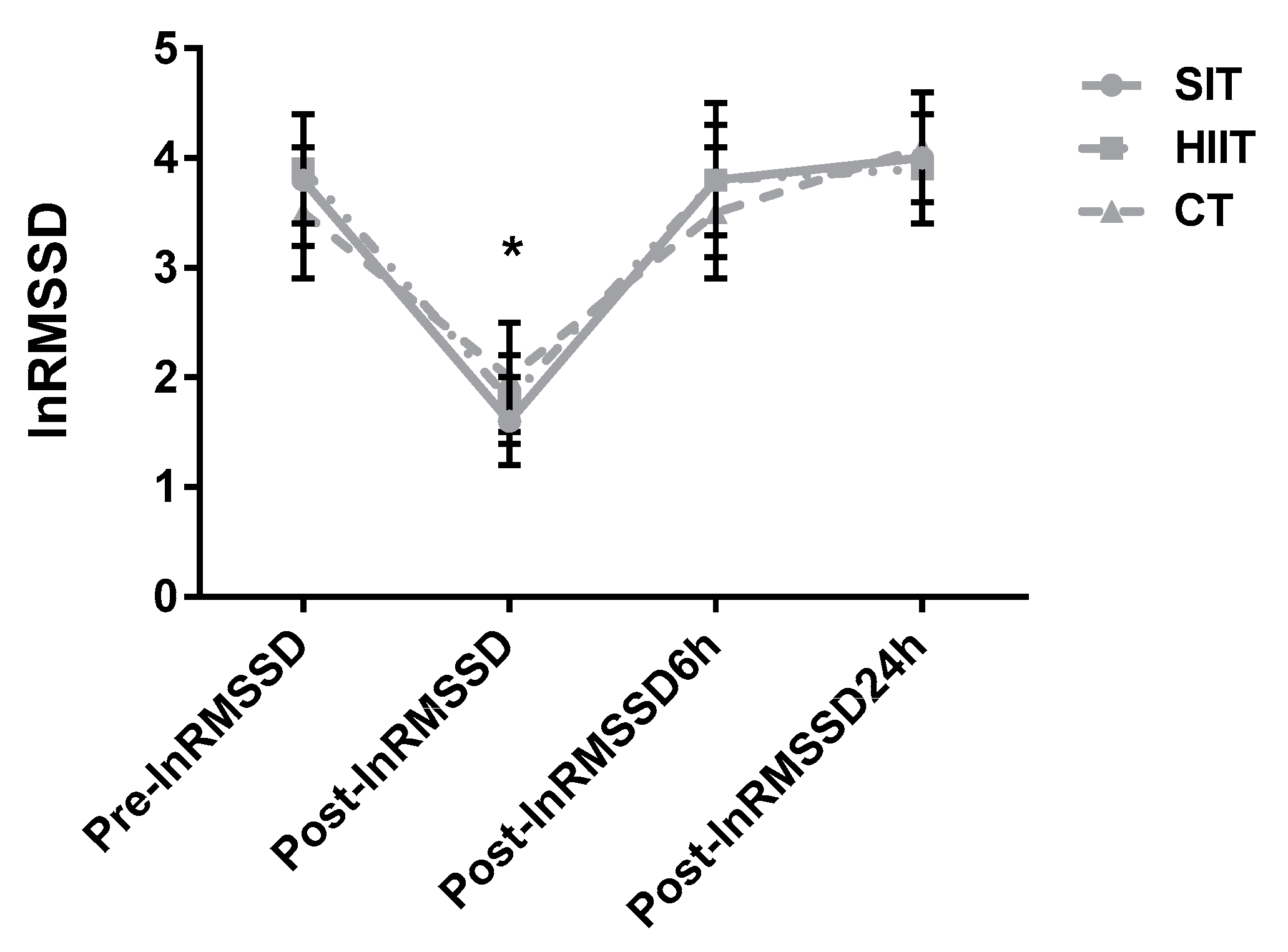
3.2.1. HRV
3.2.2. CMJ and RSI
3.2.3. Hooper Index
3.2.4. Incidental PA and sleep
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Batacan, R.B.; Duncan, M.J.; Dalbo, V.J.; Tucker, P.S.; Fenning, A.S. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br. J. Sports Med. 2017, 51, 494–503. [Google Scholar] [CrossRef]
- Gibala, M.J.; Little, J.P. Physiological basis of brief vigorous exercise to improve health. J. Physiol. 2020, 598, 61–69. [Google Scholar] [CrossRef]
- Foster, C.; Farland, C.V.; Guidotti, F.; Harbin, M.; Roberts, B.; Schuette, J.; Tuuri, A.; Doberstein, S.T.; Porcari, J.P. The effects of high intensity interval training vs steady state training on aerobic and anaerobic capacity. J. Sports Sci. Med. 2015, 14, 747–755. [Google Scholar]
- Townsend, L.K.; Islam, H.; Dunn, E.; Eys, M.; Robertson-Wilson, J.; Hazell, T.J. Modified sprint interval training protocols. Part II. Psychological responses. Appl. Physiol. Nutr. Metab. 2017, 42, 347–353. [Google Scholar] [CrossRef] [Green Version]
- Trost, S.G.; Owen, N.; Bauman, A.E.; Sallis, J.F.; Brown, W. Correlates of adults’ participation in physical activity: Review and update. Med. Sci. Sports Exerc. 2002, 34, 1996–2001. [Google Scholar] [CrossRef]
- Benítez-Flores, S.; Medeiros, A.R.; Voltarelli, F.A.; Iglesias-Soler, E.; Doma, K.; Simões, H.G.; Rosa, T.S.; Boullosa, D.A. Combined effects of very short “all out” efforts during sprint and resistance training on physical and physiological adaptations after 2 weeks of training. Eur. J. Appl. Physiol. 2019, 119, 1337–1351. [Google Scholar] [CrossRef]
- Schaun, G.Z.; Pinto, S.S.; Silva, M.R.; Dolinski, D.B.; Alberton, C.L. Whole-body high-intensity interval training induce similar cardiorespiratory adaptations compared with traditional high-intensity interval training and moderate-intensity continuous training in healthy men. J. Strength Cond. Res. 2018, 32, 2730–2742. [Google Scholar] [CrossRef]
- Vollaard, N.B.J.; Metcalfe, R.S. Research into the Health Benefits of Sprint Interval Training Should Focus on Protocols with Fewer and Shorter Sprints. Sports Med. 2017, 47, 2443–2451. [Google Scholar] [CrossRef] [Green Version]
- Stamatakis, E.; Johnson, N.A.; Powell, L.; Hamer, M.; Rangul, V.; Holtermann, A. Short and sporadic bouts in the 2018 US physical activity guidelines: Is high-intensity incidental physical activity the new HIIT? Br. J. Sports Med. 2019, 53, 1137–1139. [Google Scholar] [CrossRef] [Green Version]
- Gray, S.R.; Ferguson, C.; Birch, K.; Forrest, L.J.; Gill, J.M. High-intensity interval training: Key data needed to bridge the gap from laboratory to public health policy. Br. J. Sports Med. 2016, 50, 1231–1232. [Google Scholar] [CrossRef]
- Buchheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle: Part I: Cardiopulmonary emphasis. Sports Med. 2013, 43, 313–338. [Google Scholar] [CrossRef]
- Warr-di Piero, D.; Valverde-Esteve, T.; Redondo-Castán, J.C.; Pablos-Abella, C.; Sánchez-Alarcos Díaz-Pintado, J.V. Effects of work-interval duration and sport specificity on blood lactate concentration, heart rate and perceptual responses during high intensity interval training. PLoS ONE 2018, 13, e0200690. [Google Scholar] [CrossRef] [Green Version]
- Cipryan, L.; Tschakert, G.; Hofmann, P. Acute and post-exercise physiological responses to high-intensity interval training in endurance and sprint athletes. J. Sports Sci. Med. 2017, 16, 219–229. [Google Scholar]
- Eigendorf, J.; Maassen, M.; Apitius, D.; Maassen, N. Energy metabolism in continuous, high-Intensity, and sprint interval training protocols with matched mean intensity. J. Strength Cond. Res. 2019. [Google Scholar] [CrossRef]
- Cheung, K.; Hume, P.; Maxwell, L. Delayed onset muscle soreness: Treatment strategies and performance factors. Sports Med. 2003, 33, 145–164. [Google Scholar] [CrossRef] [PubMed]
- Farias-Junior, L.F.; Browne, R.A.V.; Freire, Y.A.; Oliveira-Dantas, F.F.; Lemos, T.; Galvão-Coelho, N.L.; Hardcastle, S.J.; Okano, A.H.; Aoki, M.S.; Costa, E.C. Psychological responses, muscle damage, inflammation, and delayed onset muscle soreness to high-intensity interval and moderate-intensity continuous exercise in overweight men. Physiol. Behav. 2019, 199, 200–209. [Google Scholar] [CrossRef]
- Buchheit, M. Monitoring training status with HR measures: Do all roads lead to Rome? Front. Physiol. 2014, 5, 73. [Google Scholar] [CrossRef] [Green Version]
- Léger, L.; Gadoury, C. Validity of the 20 m shuttle run test with 1 min stages to predict VO2max in adults. Can. J. Sport Sci. 1989, 14, 21–26. [Google Scholar] [PubMed]
- Benitez-Flores, S.; De Sousa, A.F.; Da Cunha Totó, E.C.; Rosa, T.S.; Del Rosso, S.; Foster, C.; Boullosa, D.A. Shorter sprints elicit greater cardiorespiratory and mechanical responses with less fatigue during time-matched sprint interval training (SIT) sessions. J. Electromyogr. Kinesiol. 2018, 50, 137–148. [Google Scholar] [CrossRef]
- Boullosa, D.A.; Barros, E.S.; del Rosso, S.; Nakamura, F.Y.; Leicht, A.S. Reliability of heart rate measures during walking before and after running maximal efforts. Int. J. Sports Med. 2014, 35, 999–1005. [Google Scholar] [CrossRef]
- Hardy, C.J.; Rejeski, W.J. Not what, but how one feels: The measurement of affect during exercise. J. Sport Exerc. Psychol. 1989, 11, 304–317. [Google Scholar] [CrossRef]
- Utter, A.C.; Robertson, R.J.; Green, J.M.; Suminski, R.R.; McAnulty, S.R.; Nieman, D.C. Validation of the Adult OMNI Scale of perceived exertion for walking/running exercise. Med. Sci. Sports Exerc. 2004, 36, 1776–1780. [Google Scholar] [CrossRef]
- Fernández García, E.; Sánchez Bañuelos, F.; Salinero Martín, J.J. Validation and adaptation of the PACES scale of enjoyment of the practice of physical activity for Spanish adolescent girls. Psicothema 2008, 20, 890–895. [Google Scholar] [PubMed]
- Esco, M.R.; Williford, H.N.; Flatt, A.A.; Freeborn, T.J.; Nakamura, F.Y. Ultra-shortened time-domain HRV parameters at rest and following exercise in athletes: An alternative to frequency computation of sympathovagal balance. Eur. J. Appl. Physiol. 2018, 118, 175–184. [Google Scholar] [CrossRef]
- Montalvo, S.; Gonzalez, M.P.; Dietze-Hermosa, M.S.; Eggleston, J.D.; Dorgo, S. Common vertical jump and reactive strength index measuring devices: A validity and reliability analysis. J. Strength Cond. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Markovic, G.; Dizdar, D.; Jukic, I.; Cardinale, M. Reliability and factorial validity of squat and countermovement jump tests. J. Strength Cond. Res. 2004, 18, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Comyns, T.M.; Flanagan, E.P.; Fleming, S.; Fitzgerald, E.; Harper, D.J. Interday reliability and usefulness of a reactive strength index derived from 2 maximal rebound jump tests. Int. J. Sports Physiol. Perform. 2019, 14, 1200–1204. [Google Scholar] [CrossRef]
- Hooper, S.L.; Mackinnon, L.T.; Howard, A.; Gordon, R.D.; Bachmann, A.W. Markers for monitoring overtraining and recovery. Med. Sci. Sports Exerc. 1995, 27, 106–112. [Google Scholar] [CrossRef]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the Computer Science and Applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Cole, R.J.; Kripke, D.F.; Gruen, W.; Mullaney, D.J.; Gillin, J.C. Automatic sleep/wake identification from wrist activity. Sleep 1992, 15, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Andreato, L.V.; Esteves, J.V.; Coimbra, D.R.; Moraes, A.J.P.; de Carvalho, T. The influence of high-intensity interval training on anthropometric variables of adults with overweight or obesity: A systematic review and network meta-analysis. Obes. Rev. 2019, 20, 142–155. [Google Scholar] [CrossRef] [Green Version]
- Tschakert, G.; Hofmann, P. High-intensity intermittent exercise: Methodological and physiological aspects. Int. J. Sports Physiol. Perform. 2013, 8, 600–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almquist, N.W.; Nygaard, H.; Vegge, G.; Hammarström, D.; Ellefsen, S.; Rønnestad, B.R. Systemic and muscular responses to effort-matched short intervals and long intervals in elite cyclists. Scand. J. Med. Sci. Sports 2020, 30, 1140–1150. [Google Scholar] [CrossRef] [Green Version]
- Tschakert, G.; Kroepfl, J.; Mueller, A.; Moser, O.; Groeschl, W.; Hofmann, P. How to regulate the acute physiological response to “aerobic” high-intensity interval exercise. J. Sports Sci. Med. 2015, 14, 29–36. [Google Scholar] [PubMed]
- Glaister, M. Multiple sprint work: Physiological responses, mechanisms of fatigue and the influence of aerobic fitness. Sports Med. 2005, 35, 757–777. [Google Scholar] [CrossRef]
- Olney, N.; Wertz, T.; LaPorta, Z.; Mora, A.; Serbas, J.; Astorino, T.A. Comparison of acute physiological and psychological responses between moderate-intensity continuous exercise and three regimes of high-intensity interval training. J. Strength Cond. Res. 2018, 32, 2130–2138. [Google Scholar] [CrossRef] [PubMed]
- Islam, H.; Townsend, L.K.; Hazell, T.J. Modified sprint interval training protocols. Part I. Physiological responses. Appl. Physiol. Nutr. Metab. 2017, 42, 339–346. [Google Scholar] [CrossRef] [Green Version]
- Kilpatrick, M.; Kraemer, R.; Bartholomew, J.; Acevedo, E.; Jarreau, D. Affective responses to exercise are dependent on intensity rather than total work. Med. Sci. Sports Exerc. 2007, 39, 1417–1422. [Google Scholar] [CrossRef] [Green Version]
- Jung, M.E.; Bourne, J.E.; Little, J.P. Where does HIT fit? An examination of the affective response to high-intensity intervals in comparison to continuous moderate- and continuous vigorous-intensity exercise in the exercise intensity-affect continuum. PLoS ONE 2014, 9, e114541. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, B.R.; Slama, F.A.; Deslandes, A.C.; Furtado, E.S.; Santos, T.M. Continuous and high-intensity interval training: Which promotes higher pleasure? PLoS ONE 2013, 8, e79965. [Google Scholar] [CrossRef] [PubMed]
- Saanijoki, T.; Nummenmaa, L.; Koivumäki, M.; Löyttyniemi, E.; Kalliokoski, K.K.; Hannukainen, J.C. Affective adaptation to repeated SIT and MICT protocols in insulin-resistant subjects. Med. Sci. Sports Exerc. 2018, 50, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Solomon, R.L. The opponent-process theory of acquired motivation: The costs of pleasure and the benefits of pain. Am. Psychol. 1980, 35, 691–712. [Google Scholar] [CrossRef] [PubMed]
- Astorino, T.A.; Vella, C.A. Predictors of change in affect in response to high intensity interval exercise (HIIE) and sprint interval exercise (SIE). Physiol. Behav. 2018, 196, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Soylu, Y.; Arslan, E.; Sogut, M.; Kilit, B.; Clemente, F. Effects of self-paced high-intensity interval training and moderate intensity continuous training on the physical performance and psychophysiological responses in recreationally active young adults. Biol. Sport 2021, 38, 555–562. [Google Scholar] [CrossRef]
- Rabbani, A.; Clemente, F.M.; Kargarfard, M.; Chamari, K. Match fatigue time-course assessment over four days: Usefulness of the hooper index and heart rate variability in professional soccer players. Front. Physiol. 2019, 10, 109. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | |
|---|---|
| Age (yr) | 25.9 ± 5.6 |
| Height (cm) | 173.2 ± 7.6 |
| Weight (kg) | 66.3 ± 7.3 |
| BMI (kg·m−2) | 22.1 ± 1.8 |
| Body fat mass (%) | 19.0 ± 7.6 |
| Body skeletal muscle mass (%) | 38.5 ± 5.8 |
| HRrest (beat·min−1) | 55 ± 5 |
| HRpeak SRT (beat·min−1) | 200 ± 9 |
| VO2max SRT (mL·kg−1·min−1) | 50.9 ± 5.4 |
| Variable | SIT | HIIT | CT |
|---|---|---|---|
| Total exercise duration (min) | 13.75 | 13.75 | 13.75 |
| Exercise duration (min) | 8.75 | 8.75 | 8.75 |
| Number of efforts | 14 | 18 | 1 |
| Work/recovery (s) | 5/35 | 15/15 | None |
| Intensity | all-out | ~90 %HRpeak | ~85 %HRpeak |
| Distance (m) | 428.8 ± 27.4 * | 1318.4 ± 112.9 † | 1784.5 ± 192.6 |
| HRmax (beat·min−1) | 177 ± 10 | 185 ± 10 † | 182 ± 8 |
| HRmean (beat·min−1) | 166 ± 10 * | 175 ± 8 | 173 ± 8 |
| HRmin (beat·min−1) | 146 ± 15 | 148 ± 18 | 134 ± 17 |
| time ≥ 70 %HRpeak (s) | 114 ± 100 | 30 ± 32 | 18 ± 29 |
| time ≥ 80 %HRpeak (s) | 384 ± 99 | 300 ± 141 | 414 ± 143 |
| time ≥ 90 %HRpeak (s) | 30 ± 58 ‡ | 180 ± 141 | 90 ± 156 |
| HRend (beat·min−1) | 168 ± 12 | 182 ± 10† | 174 ± 8 |
| HRΔ30s (beat·min−1) | 14 ± 8 | 15 ± 5 | 18 ± 11 |
| HRΔ60s (beat·min−1) | 27 ± 9 | 30 ± 10 | 36 ± 13 |
| HRΔ90s (beat·min−1) | 36 ± 11 * | 49 ± 7 | 50 ± 11 |
| HRΔ120s (beat·min−1) | 46 ± 13 ‡ | 59 ± 6 | 53 ± 10 |
| SIT | HIIT | CT | SIT | HIIT | CT | |
|---|---|---|---|---|---|---|
| Variable | Before 48 h | After 24 h | ||||
| INCIDENTAL PA | ||||||
| Kcal·day−1 | 717.5 ± 185 | 842.4 ± 300.1 | 849.7 ± 239.2 | 1138 ± 351.5 | 1303.4 ± 418.3 | 1218.9 ± 458.6 |
| %sedentary domain | 74.6 ± 5.5 | 70.6 ± 9.9 | 68.1 ± 7.2 | 69.6 ± 5.7 | 65.8 ± 6.3 | 68.3 ± 6.4 |
| %light domain | 13.6 ± 3 | 15.4 ± 4.7 | 17.3 ± 3.1 | 15 ± 4.9 | 16.2 ± 3 | 15.1 ± 3.7 |
| %MVPA domain | 11.8 ± 3 | 14 ± 5.8 | 14.6 ± 4.9 | 15.5 ± 1.2 | 18 ± 4.5 | 16.6 ± 3.2 |
| SLEEP | ||||||
| Efficiency | 88.1 ± 5.9 | 89.2 ± 4.3 | 90 ± 3.3 | 89.8 ± 5.1 | 91.6 ± 4.4 | 89.6 ± 5.3 |
| TST | 365 ± 76.4 | 373.9 ± 106.2 | 366.4 ± 68.5 | 360.1 ± 90.3 | 317.3 ± 82.2 | 349.2 ± 85.6 |
| WASO | 49.8 ± 26.6 | 43.9 ± 16.5 | 38.6 ± 18.9 | 43 ± 24.3 | 27.8 ± 11.5 | 37.7 ± 17.8 |
| Nºawakenings | 17.6 ± 6.6 | 19.5 ± 6.5 | 16.8 ± 7.8 | 18.8 ± 11.4 | 15.1 ± 6 | 17.7 ± 8.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benítez-Flores, S.; Magallanes, C.A.; Alberton, C.L.; Astorino, T.A. Physiological and Psychological Responses to Three Distinct Exercise Training Regimens Performed in an Outdoor Setting: Acute and Delayed Response. J. Funct. Morphol. Kinesiol. 2021, 6, 44. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk6020044
Benítez-Flores S, Magallanes CA, Alberton CL, Astorino TA. Physiological and Psychological Responses to Three Distinct Exercise Training Regimens Performed in an Outdoor Setting: Acute and Delayed Response. Journal of Functional Morphology and Kinesiology. 2021; 6(2):44. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk6020044
Chicago/Turabian StyleBenítez-Flores, Stefano, Carlos A. Magallanes, Cristine Lima Alberton, and Todd A. Astorino. 2021. "Physiological and Psychological Responses to Three Distinct Exercise Training Regimens Performed in an Outdoor Setting: Acute and Delayed Response" Journal of Functional Morphology and Kinesiology 6, no. 2: 44. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk6020044