
Sex-Specific Association of Uric Acid and Kidney Function Decline in Taiwan



1
Department of Leisure Industry and Health Promotion, National Taipei University of Nursing and Health Sciences, Taipei 112, Taiwan
2
Department of Business Management, National Taichung University of Science and Technology, Taichung City 404, Taiwan
3
Graduate Institute of Clinical Medicine, Taipei Medical University, Taipei 110, Taiwan
4
Department of Pediatrics, Tungs’ Taichung Metroharbor Hospital, Taichung 435, Taiwan
*
Author to whom correspondence should be addressed.
J. Pers. Med. 2021, 11(5), 415; https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050415
Submission received: 31 March 2021
/
Revised: 9 May 2021
/
Accepted: 12 May 2021
/
Published: 15 May 2021
(This article belongs to the Special Issue Personalized Medicine in Epidemics)
Abstract
:An elevated serum urate concentration is associated with kidney damage. Men’s uric acid levels are usually higher than women’s. However, postmenopausal women have a higher risk of gout than men, and comorbidities are also higher than in men. This study examined the sex differences in the relationship between hyperuricemia and renal progression in early chronic kidney disease (CKD) and non-CKD, and further examined the incidence of CKD in non-CKD populations among patients over 50 years of age. We analyzed 1856 women and 1852 men participating in the epidemiology and risk factors surveillance of the CKD database. Women showed a significantly higher risk of renal progression and CKD than men within the hyperuricemia group. After adjusting covariates, women, but not men resulted in an hazard ratio (HR) for developing renal progression (HR = 1.12; 95% CI 1.01–1.24 in women and HR = 1.03; 95% CI 0.93–1.13 in men) and CKD (HR = 1.11; 95% CI 1.01–1.22 in women and HR = 0.95; 95% CI 0.85–1.05 in men) for each 1 mg/dL increase in serum urate levels. The association between serum urate levels and renal progression was stronger in women. Given the prevalence and impact of kidney disease, factors that impede optimal renal function management in women and men must be identified to provide tailored treatment recommendations.
1. Introduction
Uric acid is the final product of the breakdown of an exogenous pool of purines and endogenous purine metabolism [1], and most uric acid is excreted via the kidneys [2]. Elevated serum urate concentrations are associated with gout [3], diabetes mellitus [4,5], hypertension [6,7], metabolic syndrome [8] and cardiovascular mortality [9,10]. A meta-analysis of 1,134,073 participants showed a positive dose-response association between uric acid levels and cardiovascular disease mortality risk [11]. Hyperuricemia is common in chronic kidney disease (CKD) patients [12], and several studies have also shown a relationship between serum urate levels and kidney damage [13,14,15,16]. Urate-lowering therapy statistically significantly improved estimated glomerular filtration rate (eGFR) and serum creatinine and serum creatinine [17], and reduced the incidence of kidney failure events [18]. Uric acid crystallizations induce endothelial dysfunction [19,20], systemic inflammation [21], oxidative stress, and renin-angiotensin-aldosterone system activity [22], which may provide a pathogenic mechanism for chronic urate nephropathy.
Previous evidence has suggested that there are sex differences in uric acid levels; men have a higher uric acid level than women [23], and men have a higher prevalence of gout than women [24]. Sex differences decline with increasing age, but men still far exceed women in the prevalence of gout, even in older populations [24]. Age-related factors and hormone are also associated with uric acid levels [25]. Premenopausal women have lower levels of uric acid than men or postmenopausal women because estrogens stimulate kidney clearance, secretion and reabsorption [25,26]. However, there is evidence that postmenopausal women are at higher risk of gout than men [27]. Moreover, women with hyperuricemia had more comorbidities than men with hyperuricemia. Women with high uric acid levels had a higher risk of developing metabolic syndrome [28], diabetes [29,30], hypertension [7], coronary artery disease [31,32], and cardiovascular events [9,23] than men. Sex differences have appeared in the physiological regulation of urate homeostasis. Estrogen may play an important role in the regulation of the expression or activity of urate transporters [33].
In addition, the effects of uric acid on renal function are sex-specific. Both high and low uric acid levels increase the risk of developing chronic kidney disease (CKD) in men, while only high levels are a risk factor in women [34]. A historic cohort study in Japan indicated that uric acid levels greater than 6.0 mg/dL are associated with kidney impairment in men with mild kidney dysfunction [13]. However, a screened study conducted in Japan showed that higher uric acid levels increase the risk of developing ESRD in women but not in men [35].
Sex-specificity exists in renal progression in patients with early CKD [36,37]. In fact, whether the incidence of CKD and renal progression differ between postmenopausal women and men with hyperuricemia is unclear. Early detection of loss of kidney function and early treatment can decrease the risk of complications [38], prevent disease progression and prevent high medical costs in later stages [39]. Therefore, we investigated sex differences in the relationship between hyperuricemia and renal progression in early CKD and non-CKD populations, and further examined the incidence of CKD in non-CKD populations among patients over 50 years of age.
2. Materials and Methods
2.1. Study Population
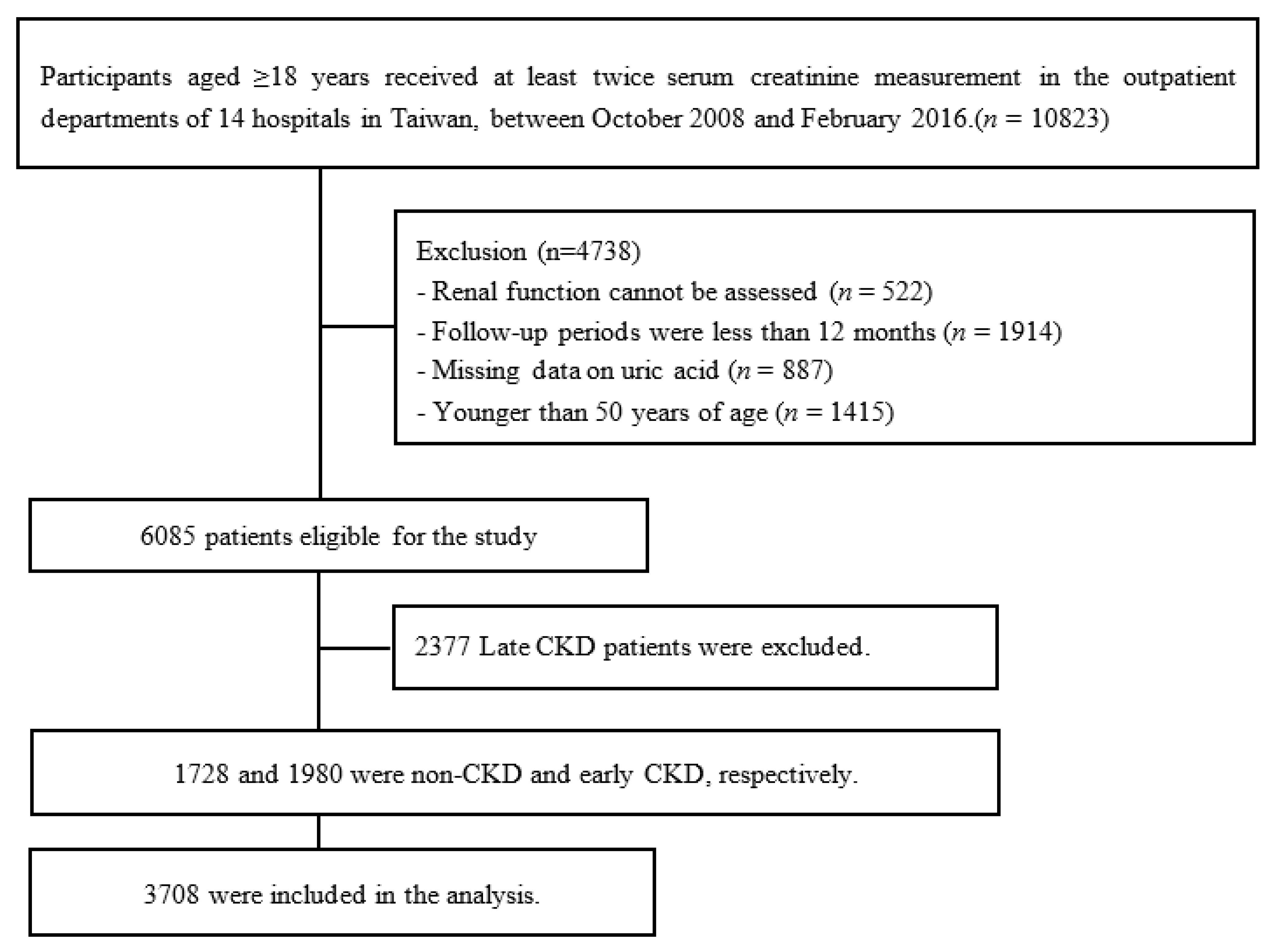
A cohort based on the Epidemiology and Risk Factors Surveillance of CKD database was recruited from 14 medical centers and community in Taiwan, namely Tri-Service General Hospital, Taipei Medical University Hospital, Shuang Ho Hospital, Taipei Chang Gung Memorial Hospital of the C.G.M.F., Cardinal Tien Hospital, E-DA Hospital, National Cheng Kung University Hospital, China Medical University Hospital, Show Chwan Memorial Hospital, Changhua Christian Hospital, Taipei Veterans General Hospital, Kaohsiung Medical University Chung-Ho Memorial Hospital, Kaohsiung Municipal Siaogang Hospital, and Kaohsiung Chang Gung Memorial Hospital from October 2008 to February 2016. A total of 10,823 participants aged ≥18 years who had at least two serum creatinine measurements were recruited in this study. For this study, we excluded patients according to the following criteria: renal function could not be assessed, the follow-up periods were less than 12 months, missing data on uric acid or younger than 50 years of age. In total, 6085 patients were enrolled, with 1728, 1980 and 2377 having non-CKD, early CKD and late CKD, respectively. In the present study, we examined the risk factors for renal progression in subjects with non-CKD and early CKD, as well as the incidence of CKD in subjects with non-CKD (Figure 1).
The studied medical centers used the same medical laboratory criteria and protocols, and thus, the serum creatinine values from the different medical centers could be compared and standardized. We measured eGFR changes at the individual level and re-examined patients at the same medical center to control individual variation. After a thorough explanation of the study, all participants provided informed consent before data collection. This study was approved by the Ethics Committees of the Tri-Service General Hospital (TSGHIRB 100-05-197), Taipei Medical University (TMU-JIRB 20124036), Kaohsiung Medical University Chung-Ho Memorial Hospital (KMUHIRB 20120019), National Cheng Kung University Hospital (A-ER-101-117), Changhua Christian Hospital (CCHIRB 120405), Kaohsiung Chang Gung Memorial Hospital (101-1096B), Cardinal Tien Hospital (TMU-JIRB 201204035) and China Medical University Hospital (DMR101-IRB2-273(CR-1)). All the research methods were implemented in accordance with guidelines approved by the Ethics Committees.
2.2. Study Variables and Definitions
The definition of CKD was based on the Kidney Disease Outcomes Quality Initiative guidelines [40]. eGFR was calculated using the chronic nephrology epidemiology collaboration (CKD-EPI) equation [eGFR (mL/min/1.73 m2) = 141 × min (serum creatinine (SCr)/κ, 1)α × max SCr/κ, 1)−1.209 × 0.993age × 1.018 (if women) × 1.159 (if black)], κ = 0.7 (women) and 0.9 (men), α = −0.329 (women) and −0.411(men); min indicates the minimum of SCr/κ or 1, and max indicates the maximum of SCr/κ or 1 [41]. CKD stage 1 was defined as a eGFR value of ≥90 mL/min/1.73 m2 and the presence of kidney damage (i.e., proteinuria dipsticks ≥1+, urine protein-to-creatinine ratio (UPCR) ≥150, or urine albumin-to-creatinine ratio (UACR) ≥ 30); CKD stage 2 was defined as eGFR = 60–89 mL/min/1.73 m2 and the presence of kidney damage (i.e., proteinuria dipsticks ≥1+, urine protein-to-creatinine ratio (UPCR) ≥150, or urine albumin-to-creatinine ratio (UACR) ≥30); CKD stage 3a was defined as eGFR = 45–59 mL/min/1.73 m2; CKD stage 3b was defined as eGFR = 30–44 mL/min/1.73 m2; CKD stage 4 was defined as eGFR = 15–29 mL/min/1.73 m2; and CKD stage 5 was defined as eGFR <15 mL/min/1.73 m2 [42]. CKD stages 1, 2, and 3a referred to patients with early CKD, whereas CKD stages 3b, 4, and 5 referred to patients with late CKD.
According to the baseline eGFR, renal progression was defined as an eGFR that was reduced by more than 25% [43]. Non-CKD patients were followed up from the baseline measurement of renal function to the development of renal progression and CKD, or the end of the study period. Early CKD patients were followed up from the baseline measurement of renal function to the development of renal progression, or the end of the study period. The patients were censored at the end of the follow-up period.
Uric acid status was classified as the absence of hyperuricemia (serum urate concentration values of <7.0 mg/dL for men and <6.0 mg/dL for women) or the presence of hyperuricemia (serum urate concentration values of ≥7.0 mg/dL for men and ≥6.0 mg/dL for women) [44,45].
Sociodemographic characteristics, comorbidities, and health-related behaviors, including age, sex, hypertension, diabetes mellitus, dyslipidemia, CKD, gout, stroke, cigarette smoking, and alcohol consumption, were obtained at baseline using a structured questionnaire. Serum urate levels and physical examination variables, including height, weight, body mass index (BMI), serum creatinine, baseline eGFR, systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting glucose, and total cholesterol, were obtained via medical chart review. Cigarette smoking was divided into never smoking, current smoker (had smoked at least 100 cigarettes in the lifetime and is currently smoking cigarettes) or former smoker (had smoked at least 100 cigarettes in the lifetime but had quit smoking at the time of the interview) [46,47]. Alcohol consumption was divided into current alcohol consumers versus participants who never consumed alcohol.
2.3. Statistical Analysis
To determine the significant differences between women and men, participants were examined using the chi-square test and Student’s t test for categorical and continuous variables, respectively. The incidence density method was used to estimate the uric acid status and sex-specific incidence rates of renal progression and CKD. Multivariate Cox proportional hazards analysis was used to estimate the hazard ratio (HR) and 95% confidence interval (CI) of the risk of renal progression and CKD associated with sex. Covariates included age, CKD, hypertension, diabetes mellitus, dyslipidemia, gout, stroke, BMI, serum creatinine, cigarette smoking, and alcohol consumption.
To induce a similar distribution of covariates between women and men, we used the inverse probability of treatment weighting (IPTW) analysis method, where the weight was the inverse (i.e., reciprocal) of the propensity scores [48]. To assess the balance of baseline covariates between women and men, we applied absolute standardized mean differences. In addition, the value of the absolute standardized mean difference was required to be lower than 10% between the sexes, indicating negligible differences among the covariates. In addition, the value of the absolute standardized mean difference was less than 10% between sexes, indicating negligible differences among the potential confounders [49]. The risks of renal progression and CKD among the groups of women and men were compared using Cox proportional hazards regression with IPTW. In order to compare the results of premenopausal and postmenopausal women, we further analyzed the sex differences in the relationship between hyperuricemia and renal progression and the incidence of CKD among patients before 50 years of age. Analyses were performed using SAS software (SAS Institute), version 9.4.
3. Results
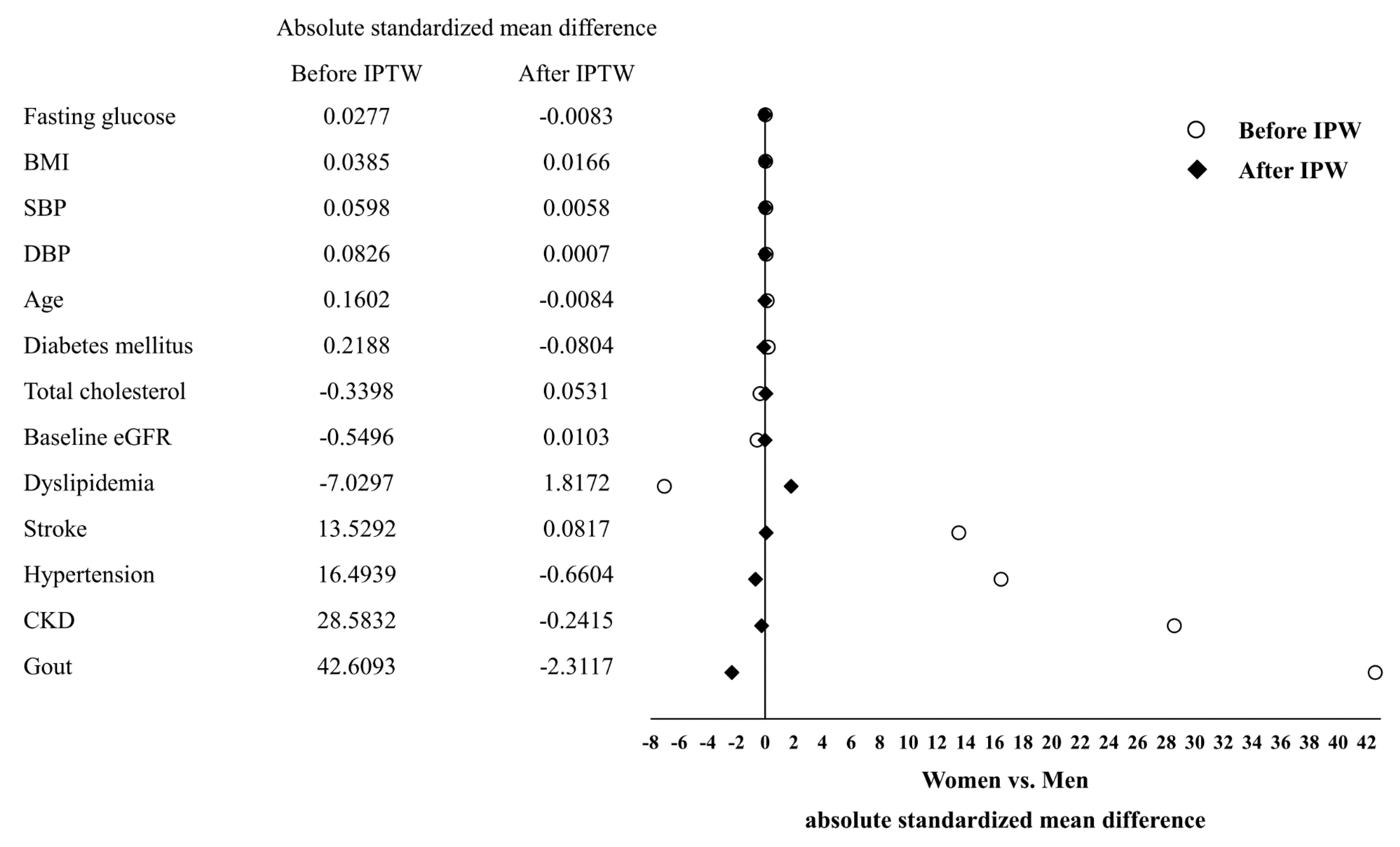
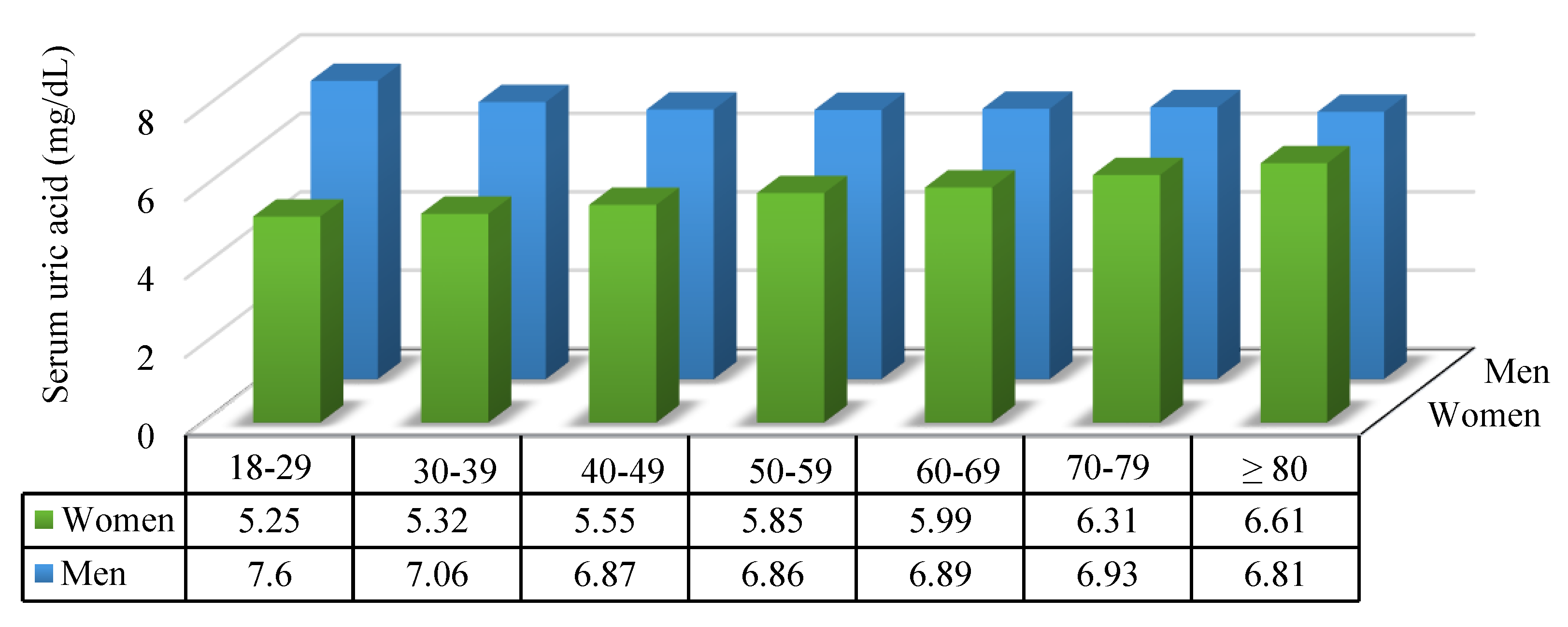
Table 1 shows the demographic and clinical characteristics of the women and men. Of the 3708 participants, 1856 (50.05%) and 1852 (49.95%) were women and men, respectively. Before employing IPTW, the women exhibited significantly lower prevalences of hypertension (1124 (60.56%)), CKD (859 (46.28%)), gout (118 (6.36%)), stroke (87 (4.69%)), current smoking (36 (1.96%)), and alcohol consumption (63 (3.43%)) as well as low levels of serum urate (5.49 (SD 1.36)), serum creatinine (0.73 (SD 0.15)), and DBP (76.02 (SD 10.71)) than men (Table 1). After applying IPTW, the different sexes were well balanced with respect to key characteristics, such as fasting glucose, BMI, SBP, DBP, age, diabetes mellitus, total cholesterol, baseline eGFR, dyslipidemia, stroke, hypertension, CKD, and gout (all absolute standardized mean difference lower than 10%; Figure 2). The mean levels of uric acid in men was higher than that in women in each age group (18–29 group, p < 0.001; 30–39 group, p < 0.001; 40–49 group, p < 0.001; 50–59 group, p < 0.001; 60–69 group, p < 0.001; 70–79 group, p < 0.001; ≥80, p = 0.214), but levels of uric acid were increases with advancing age in women but not in men. Both in women and men, uric acid levels showed statistically significant differences in each age group (women, p < 0.001; men p = 0.004) (Figure 3).
Within the group without hyperuricemia, the incidence rates of renal progression in men and women were 4.86 and 3.79 per 100 patient-years, respectively; the incidence rates of CKD in men and women were 13.31 and 9.54 per 100 patient-years, respectively. Within the hyperuricemia group, the incidence rates for renal progression in men and women were 5.44 and 6.15 per 100 patient-years, respectively; the incidence rates for CKD in men and women were 14.54 and 15.26 per 100 patient-years, respectively (Table 2).
After using IPTW, women showed a significantly higher risk of renal progression (HR 2.21; 95% CI 1.55–3.14) and CKD (HR 2.69; 95% CI 1.90–3.81) than men within the group without hyperuricemia. Women showed a significantly higher risk of renal progression (HR 2.14; 95% CI 1.35–3.40) and CKD (HR 3.56; 95% CI 2.04–6.25) than men within the hyperuricemia group (Table 3).
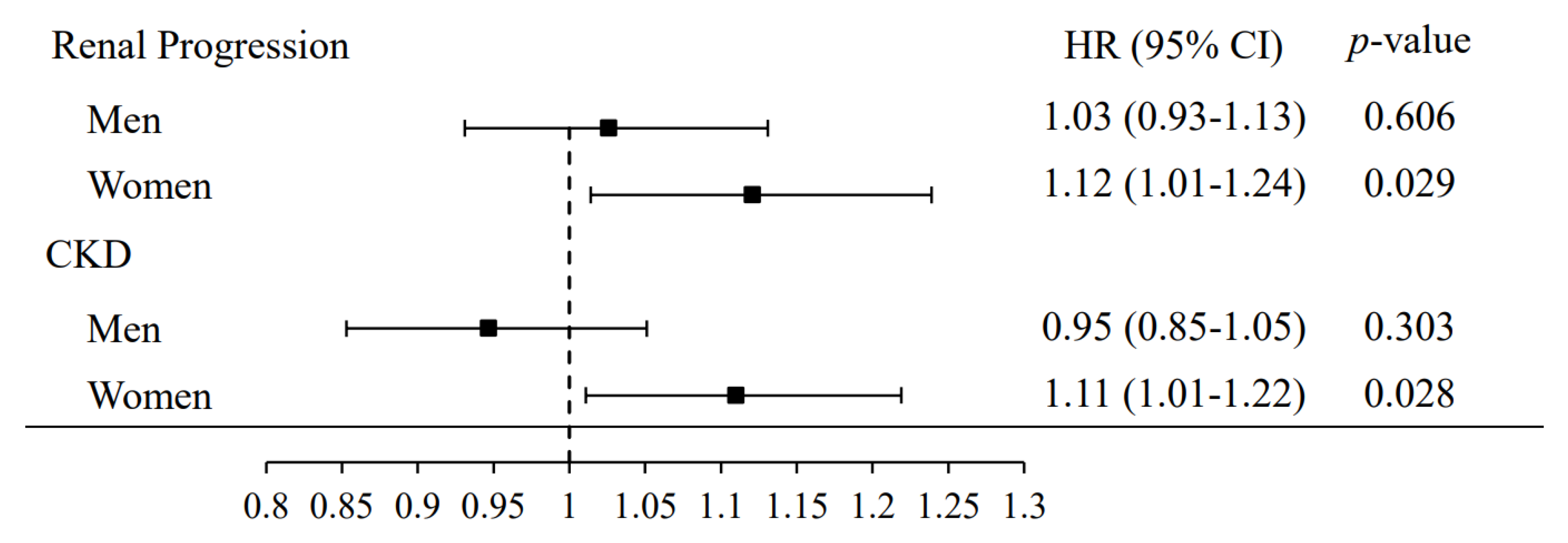
In women, the multivariate adjustment for age, CKD, hypertension, diabetes mellitus, dyslipidemia, gout, stroke, BMI, serum creatinine, cigarette smoking, and alcohol consumption resulted in an HR for developing renal progression of 1.12 (95% CI, 1.01–1.24) and for CKD of 1.11 (95% CI, 1.01–1.22) for each 1 mg/dL increase in serum urate levels. In men, there was no association between serum urate levels and developing renal progression and CKD (Figure 4).
We further analyzed the results of patients before the age of 50. Women did not have a higher risk of renal progression and CKD than men within the group without hyperuricemia (Table S1).
4. Discussion
The multicenter cohort study enrolled subjects with early CKD and without CKD to demonstrate that serum urate levels are an independent predictor of renal progression and incident CKD. We found significant differences between men and women. The effect of sex differences in the role of serum urate levels on the long-term prognosis of patients in terms of renal progression and incident CKD among early CKD and non-CKD has not previously been fully explored in middle-aged and elderly adults. To our knowledge, this is the first study to elucidate sex differences in serum urate levels for the prognosis of patients with kidney damage among middle-aged and elderly adults with early CKD and without CKD.
Serum urate levels are a well-known marker of hypertension, gout, arterial stiffness, cardiac hypertrophy, metabolic syndrome, and cardiovascular damage [3,8,9,50,51,52,53]. Our findings on the effect of serum urate levels on the risk of renal progression among individuals with early CKD are consistent with previous studies. In patients with renal disease, a higher uric acid concentration was a strong independent predictor of kidney failure in earlier stages of CKD [16]. Srivastava et al. described this relationship of uric acid concentration with all-cause mortality as J-shaped in individuals with CKD [16]. High uric acid was found to be a risk factor for CKD and a rapid decline in eGFR in patients with mild kidney dysfunction [13]. We observed that hyperuricemia is an independent risk factor for incident CKD among individuals without CKD. In the general population, uric acid levels promote initial kidney damage and incident kidney disease [14,54,55].
However, a recently meta-analysis of randomized controlled trials demonstrated that urate-lowering therapy was associated with slowing the decline rate of GFR, but there is insufficient evidence to support urate lowering in patients to improve kidney outcomes [12]. Previous Mendelian randomized study found that there is no evidence to support a causal relationship between serum uric acid levels and eGFR levels or incident CKD [56]. The Controlled Trial of Slowing of Kidney Disease Progression from the Inhibition of Xanthine Oxidase (CKD-FIX) demonstrated that allopurinol dose not slow down the progression of CKD in patients with severe CKD and high risk of progression [57]. The Preventing Early Renal Loss in Diabetes (PERL) trial did not show a beneficial effect of reduction of the serum urate level with allopurinol therapy on the kidney outcomes in persons with type 1 diabetes and early-to-moderate diabetic kidney disease [58]. The PERL and CKD-FIX trials do not support the clinical benefits of allopurinol in the treatment of asymptomatic hyperuricemia on kidney outcomes [57,58].
Although, the causal relationship between the effects of uric acid and CKD is still debatable. In a perspectives article argues that hyperuricemia is directly related to the development and progression of CKD, and treatment with urate-lowering therapy may provide clinical benefits [59]. Hyperuricemia has a detrimental effect on kidney function [59].
Hyperuricemia accelerates renal progression by increasing renal renin and cyclooxygenase-2 expression and causing vascular smooth muscle cell proliferation [60]. Oxidative stress plays an important pathophysiological role in renal progression [22]. Furthermore, impaired kidney clearance is responsible for increased uric acid concentrations [16].
There are sex differences in hypertension and cardiovascular events in patients with high serum urate levels, and the rates in female patients are significantly higher than those in males [9,61]. The present study demonstrated that sex differences in the association between uric acid level and renal progression and incident CKD were stronger in women than in men. A previous study in Okinawa, Japan also found a significant association between uric acid and renal failure requiring renal replacement in women, but no significant association was observed in men [35].
It is well known that men have higher uric acid levels than women. Our findings also showed that men had higher levels of uric acid than women in each age group; however, we found that uric acid levels increased with advancing age in women but not in men. Women before the age of 50 did not have a higher risk of renal progression and CKD than men. Uric acid levels increase with age, and after menopause, the levels roughly equal the levels in men in later years [62]. A previous study in Japan showed that women uric acid levels increased until the age of 70 years or older as a result of changes in hormones accompanying menopause [63]. This finding provides a potential explanation for why women have a higher risk of kidney damage than men.
Young women have higher levels of estrogen, which can promote renal uric acid excretion and reduce uric acid levels [26,64]. The Third National Health and Nutrition Examination Survey reported that postmenopausal women receiving hormone replacement therapy may have reduced uric acid levels [25]. Further investigations are encouraged to investigate the mechanism by which hyperuricemic women have a higher risk of reduced renal function than men among elderly populations.
Our findings indicate that young men aged 18–29 and 30–39 have higher serum urate levels and decrease with age, while the opposite is the case in women. If young people aged 18–40 have normal kidney function and they develop hyperuricemia, the most likely clinical indication is genetic variants in urate transporters, such as SLC2A9 [65], rather than underlying chronic kidney disease. Additionally, there is extensive evidence that variants in ABCG2 cause hyperuricemia in young people [66,67,68]. Thus, predicting whether these patients develop CKD or whether hyperuricemia contributes to CKD progression later in life is impossible due to genetic components and environmental factors as previously described in a study in Taiwan [69]. Therefore, in this study, the sex-specific relationship between hyperuricemia and renal progression was studied, with a focus on patients over 50 years of age.
In addition, we found that younger women with hyperuricemia have a higher risk of kidney deterioration than men with hyperuricemia. A study of a military cohort of young individuals also found that the association between hyperuricemia and raised blood pressure was stronger in women than in men [70]. One possible explanation for the sex difference is that women with hyperuricemia may have higher levels of xanthine oxidase activity and reactive oxygen species productions than men, leading to more severe renal vascular inflammation in women than in men [71,72].
This study has several advantages. First, we had a large cohort that recruited patients from multiple centers throughout Taiwan. Second, we provided sex-specific data showing a difference in the relationship between hyperuricemia and renal progression. Third, this study used well-trained interviewers to collect data on demographic characteristics and health-related behaviors face to face. Finally, in order to reduce the effects of confounding in observational study, we used the IPTW analysis method to induce similar covariate distribution between women and men.
However, our study has some limitations. First, this research may have potential selection bias because our patients were voluntarily recruited. Second, certain test results may be underestimated due to the use of structured questionnaires to collect clinical disease data. Third, this study does not contain information on potential factors, including menopausal age and hormone replacement therapy. Fourth, this study uses structured questionnaires to collect alcohol consumption data, but does not include daily alcohol consumption. Therefore, it is difficult to accurately analyze the possible relationship between alcohol consumption with hyperuricemia and renal decline. Therefore, these factors should be considered in future research.
5. Conclusions
Given the prevalence and impact of kidney disease, factors that impede optimal renal function management in women and men must be identified to provide tailored treatment recommendations. Elevated serum urate levels are a strong risk factor for developing kidney disease. Therefore, our results suggest that individuals, especially postmenopausal women, with higher uric acid levels are at increased risk of developing renal progression and incident CKD.
Supplementary Materials
The following are available online at https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/jpm11050415/s1, Table S1: Risk of renal progression and CKD by hyperuricemia in younger women and men (Less than 50 years old).
Author Contributions
Conceptualization, P.-Y.C.; methodology, P.-Y.C.; software, P.-Y.C.; validation, Y.-W.C. and Y.-F.L.; formal analysis, P.-Y.C.; investigation, P.-Y.C. and Y.-F.L.; writing—original draft preparation, P.-Y.C. and Y.-W.C.; writing—review and editing, P.-Y.C.; supervision, Y.-F.L. and H.-C.F.; funding acquisition, Y.-F.L. and H.-C.F. All authors have read and agree to the published version of the manuscript.
Funding
This study was funded by a grant from the Health Promotion Administration, Ministry of Health and Welfare, Taiwan, Republic of China (DOH101-HP-1103, DOH102-HP-1103, MOHW103-HPA-H-114-134101, MOHW104-HPA-H-114-134101); National Taipei University of Nursing and Health Sciences (109ntunhs-NT-02).
Institutional Review Board Statement
This study was approved by the Ethics Committees of Tri-Service General Hospital (TSGHIRB 100-05-197), Taipei Medical University (TMU-JIRB 20124036), Kaohsiung Medical University Chung-Ho Memorial Hospital (KMUHIRB 20120019), National Cheng Kung University Hospital (A-ER-101-117), Changhua Christian Hospital (CCHIRB 120405), Kaohsiung Chang Gung Memorial Hospital (101-1096B), Cardinal Tien Hospital (TMU-JIRB 201204035) and China Medical University Hospital (DMR101-IRB2-273(CR-1)). All research methods were implemented in accordance with guidelines approved by the Ethics Committees.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are not publicly available due to subject’s privacy.
Conflicts of Interest
The authors declare that there is no duality of interest associated with this manuscript.
References
- Maiuolo, J.; Oppedisano, F.; Gratteri, S.; Muscoli, C.; Mollace, V. Regulation of uric acid metabolism and excretion. Int. J. Cardiol. 2016, 213, 8–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipkowitz, M.S. Regulation of uric acid excretion by the kidney. Curr. Rheumatol. Rep. 2012, 14, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Shiozawa, A.; Szabo, S.M.; Bolzani, A.; Cheung, A.; Choi, H.K. Serum Uric Acid and the Risk of Incident and Recurrent Gout: A Systematic Review. J. Rheumatol. 2017, 44, 388–396. [Google Scholar] [CrossRef]
- Dehghan, A.; van Hoek, M.; Sijbrands, E.J.G.; Hofman, A.; Witteman, J.C.M. High Serum Uric Acid as a Novel Risk Factor for Type 2 Diabetes. Diabetes Care 2008, 31, 361–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juraschek, S.P.; McAdams-Demarco, M.; Miller, E.R.; Gelber, A.C.; Maynard, J.W.; Pankow, J.S.; Young, H.; Coresh, J.; Selvin, E. Temporal relationship between uric acid concentration and risk of diabetes in a community-based study population. Am. J. Epidemiol. 2014, 179, 684–691. [Google Scholar] [CrossRef]
- Sundstrom, J.; Sullivan, L.; D’Agostino, R.B.; Levy, D.; Kannel, W.B.; Vasan, R.S. Relations of serum uric acid to longitudinal blood pressure tracking and hypertension incidence. Hypertension 2005, 45, 28–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwabara, M.; Hisatome, I.; Niwa, K.; Hara, S.; Roncal-Jimenez, C.A.; Bjornstad, P.; Nakagawa, T.; Andres-Hernando, A.; Sato, Y.; Jensen, T.; et al. Uric Acid Is a Strong Risk Marker for Developing Hypertension from Prehypertension: A 5-Year Japanese Cohort Study. Hypertension 2018, 71, 78–86. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Al-Attas, O.S.; Wani, K.; Sabico, S.; Alokail, M.S. Serum Uric Acid to Creatinine Ratio and Risk of Metabolic Syndrome in Saudi Type 2 Diabetic Patients. Sci. Rep. 2017, 7, 12104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, J.; Alderman, M.H. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971–1992. National Health and Nutrition Examination Survey. JAMA 2000, 283, 2404–2410. [Google Scholar] [CrossRef] [Green Version]
- Feig, D.I.; Kang, D.H.; Johnson, R.J. Uric acid and cardiovascular risk. N. Engl. J. Med. 2008, 359, 1811–1821. [Google Scholar] [CrossRef]
- Rahimi-Sakak, F.; Maroofi, M.; Rahmani, J.; Bellissimo, N.; Hekmatdoost, A. Serum uric acid and risk of cardiovascular mortality: A systematic review and dose-response meta-analysis of cohort studies of over a million participants. BMC Cardiovasc. Disord. 2019, 19, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Wang, Z.; Zhou, J.; Chen, Z.; Li, Y.; Li, S.; Zhao, H.; Badve, S.V.; Lv, J. Effect of Urate-Lowering Therapy on Cardiovascular and Kidney Outcomes: A Systematic Review and Meta-Analysis. Clin. J. Am. Soc. Nephrol. 2020, 15, 1576–1586. [Google Scholar] [CrossRef] [PubMed]
- Toyama, T.; Furuichi, K.; Shimizu, M.; Hara, A.; Iwata, Y.; Sakai, N.; Perkovic, V.; Kobayashi, M.; Mano, T.; Kaneko, S.; et al. Relationship between Serum Uric Acid Levels and Chronic Kidney Disease in a Japanese Cohort with Normal or Mildly Reduced Kidney Function. PLoS ONE 2015, 10, e0137449. [Google Scholar] [CrossRef] [PubMed]
- Obermayr, R.P.; Temml, C.; Gutjahr, G.; Knechtelsdorfer, M.; Oberbauer, R.; Klauser-Braun, R. Elevated uric acid increases the risk for kidney disease. J. Am. Soc. Nephrol. 2008, 19, 2407–2413. [Google Scholar] [CrossRef] [Green Version]
- Ahola, A.J.; Sandholm, N.; Forsblom, C.; Harjutsalo, V.; Dahlström, E.; Groop, P.-H.; FinnDiane Study Group. The serum uric acid concentration is not causally linked to diabetic nephropathy in type 1 diabetes. Kidney Int. 2017, 91, 1178–1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srivastava, A.; Kaze, A.D.; McMullan, C.J.; Isakova, T.; Waikar, S.S. Uric Acid and the Risks of Kidney Failure and Death in Individuals With CKD. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2018, 71, 362–370. [Google Scholar] [CrossRef]
- Kanji, T.; Gandhi, M.; Clase, C.M.; Yang, R. Urate lowering therapy to improve renal outcomes in patients with chronic kidney disease: Systematic review and meta-analysis. BMC Nephrol. 2015, 16, 58. [Google Scholar] [CrossRef] [Green Version]
- Su, X.; Xu, B.; Yan, B.; Qiao, X.; Wang, L. Effects of uric acid-lowering therapy in patients with chronic kidney disease: A meta-analysis. PLoS ONE 2017, 12, e0187550. [Google Scholar] [CrossRef] [Green Version]
- Khosla, U.M.; Zharikov, S.; Finch, J.L.; Nakagawa, T.; Roncal, C.; Mu, W.; Krotova, K.; Block, E.R.; Prabhakar, S.; Johnson, R.J. Hyperuricemia induces endothelial dysfunction. Kidney Int. 2005, 67, 1739–1742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, W.; Duan, X.-M.; Liu, Y.; Yu, J.; Tang, Y.-L.; Liu, Z.-L.; Jiang, S.; Zhang, C.-P.; Liu, J.-Y.; Xu, J.-X. Uric Acid Induces Endothelial Dysfunction by Activating the HMGB1/RAGE Signaling Pathway. BioMed Res. Int. 2017, 2017, 4391920. [Google Scholar] [CrossRef]
- Zhou, Y.; Fang, L.; Jiang, L.; Wen, P.; Cao, H.; He, W.; Dai, C.; Yang, J. Uric acid induces renal inflammation via activating tubular NF-kappaB signaling pathway. PLoS ONE 2012, 7, e39738. [Google Scholar]
- Yu, M.A.; Sanchez-Lozada, L.G.; Johnson, R.J.; Kang, D.H. Oxidative stress with an activation of the renin-angiotensin system in human vascular endothelial cells as a novel mechanism of uric acid-induced endothelial dysfunction. J. Hypertens. 2010, 28, 1234–1242. [Google Scholar] [CrossRef]
- Barbieri, L.; Verdoia, M.; Schaffer, A.; Marino, P.; Suryapranata, H.; De Luca, G. Impact of sex on uric acid levels and its relationship with the extent of coronary artery disease: A single-centre study. Atherosclerosis 2015, 241, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A. Racial and gender disparities among patients with gout. Curr. Rheumatol. Rep. 2013, 15, 307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hak, A.E.; Choi, H.K. Menopause, postmenopausal hormone use and serum uric acid levels in US women--the Third National Health and Nutrition Examination Survey. Arthritis Res. Ther. 2008, 10, R116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yahyaoui, R.; Esteva, I.; Haro-Mora, J.J.; Almaraz, M.C.; Morcillo, S.; Rojo-Martinez, G.; Martinez, J.; Gomez-Zumaquero, J.M.; Gonzalez, I.; Hernando, V.; et al. Effect of long-term administration of cross-sex hormone therapy on serum and urinary uric acid in transsexual persons. J. Clin. Endocrinol. Metab. 2008, 93, 2230–2233. [Google Scholar] [CrossRef] [Green Version]
- Puig, J.G.; Michan, A.D.; Jimenez, M.L.; Perez de Ayala, C.; Mateos, F.A.; Capitan, C.F.; de Miguel, E.; Gijon, J.B. Female gout. Clinical spectrum and uric acid metabolism. Arch. Intern. Med. 1991, 151, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Yadav, D.; Lee, E.S.; Kim, H.M.; Choi, E.; Lee, E.Y.; Lim, J.S.; Ahn, S.V.; Koh, S.B.; Chung, C.H. Prospective study of serum uric acid levels and incident metabolic syndrome in a Korean rural cohort. Atherosclerosis 2015, 241, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Kivity, S.; Kopel, E.; Steinlauf, S.; Segev, S.; Sidi, Y.; Olchovsky, D. The association between serum uric acid and diabetes mellitus is stronger in women. J. Women Health 2013, 22, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Niwa, K.; Hisatome, I.; Nakagawa, T.; Roncal-Jimenez, C.A.; Andres-Hernando, A.; Bjornstad, P.; Jensen, T.; Sato, Y.; Milagres, T.; et al. Asymptomatic Hyperuricemia Without Comorbidities Predicts Cardiometabolic Diseases: Five-Year Japanese Cohort Study. Hypertension 2017, 69, 1036–1044. [Google Scholar] [CrossRef] [PubMed]
- Wingrove, C.S.; Walton, C.; Stevenson, J.C. The effect of menopause on serum uric acid levels in non-obese healthy women. Metabolism Clin. Exp. 1998, 47, 435–438. [Google Scholar] [CrossRef]
- Lan, M.; Liu, B.; He, Q. Evaluation of the association between hyperuricemia and coronary artery disease: A STROBE-compliant article. Medicine 2018, 97, e12926. [Google Scholar] [CrossRef] [PubMed]
- Halperin Kuhns, V.L.; Woodward, O.M. Sex Differences in Urate Handling. Int. J. Mol. Sci. 2020, 21, 4269. [Google Scholar] [CrossRef] [PubMed]
- Mun, K.H.; Yu, G.I.; Choi, B.Y.; Kim, M.K.; Shin, M.H.; Shin, D.H. Effect of Uric Acid on the Development of Chronic Kidney Disease: The Korean Multi-Rural Communities Cohort Study. J. Prev. Med. Public Health Yebang Uihakhoe Chi 2018, 51, 248–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iseki, K.; Ikemiya, Y.; Inoue, T.; Iseki, C.; Kinjo, K.; Takishita, S. Significance of hyperuricemia as a risk factor for developing ESRD in a screened cohort. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2004, 44, 642–650. [Google Scholar] [CrossRef]
- Chang, P.Y.; Chien, L.N.; Lin, Y.F.; Wu, M.S.; Chiu, W.T.; Chiou, H.Y. Risk factors of gender for renal progression in patients with early chronic kidney disease. Medicine 2016, 95, e4203. [Google Scholar] [CrossRef]
- Okada, K.; Yanai, M.; Takeuchi, K.; Matsuyama, K.; Nitta, K.; Hayashi, K.; Takahashi, S. Sex differences in the prevalence, progression, and improvement of chronic kidney disease. Kidney Blood Press. Res. 2014, 39, 279–288. [Google Scholar] [CrossRef]
- Fink, H.A.; Ishani, A.; Taylor, B.C.; Greer, N.L.; MacDonald, R.; Rossini, D.; Sadiq, S.; Lankireddy, S.; Kane, R.L.; Wilt, T.J. AHRQ Comparative Effectiveness Reviews Chronic Kidney Disease Stages 1-3: Screening, Monitoring, and Treatment. In Chronic Kidney Disease Stages 1–3: Screening, Monitoring, and Treatment; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2012. [Google Scholar]
- Honeycutt, A.A.; Segel, J.E.; Zhuo, X.; Hoerger, T.J.; Imai, K.; Williams, D. Medical costs of CKD in the Medicare population. J. Am. Soc. Nephrol. 2013, 24, 1478–1483. [Google Scholar] [CrossRef]
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2002, 39 (Suppl. 1), S1–S266. [Google Scholar]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J. Chronic kidney disease. Lancet 2012, 379, 165–180. [Google Scholar] [CrossRef]
- Levin, A. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGOKCW; KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Chang, H.Y.; Tung, C.W.; Lee, P.H.; Lei, C.C.; Hsu, Y.C.; Chang, H.H.; Yang, H.F.; Lu, L.C.; Jong, M.C.; Chen, C.Y.; et al. Hyperuricemia as an independent risk factor of chronic kidney disease in middle-aged and elderly population. Am. J. Med. Sci. 2010, 339, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.; Perveen, R.; Rahman, S.; Mahmood, S.; Rahman, S.; Islam, S.; Haque, T.; Sumon, A.H.; Kathak, R.R.; Molla, N.H.; et al. Prevalence of hyperuricemia and the relationship between serum uric acid and obesity: A study on Bangladeshi adults. PLoS ONE 2018, 13, e0206850. [Google Scholar] [CrossRef] [Green Version]
- Vupputuri, S.; Sandler, D.P. Lifestyle risk factors and chronic kidney disease. Ann. Epidemiol. 2003, 13, 712–720. [Google Scholar] [CrossRef]
- Henley, S.J.; Asman, K.; Momin, B.; Gallaway, M.S.; Culp, M.B.; Ragan, K.R.; Richards, T.B.; Babb, S. Smoking cessation behaviors among older, U.S. adults. Prev. Med. Rep. 2019, 16, 100978. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef]
- Austin, P.C. The use of propensity score methods with survival or time-to-event outcomes: Reporting measures of effect similar to those used in randomized experiments. Stat. Med. 2014, 33, 1242–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viazzi, F.; Parodi, D.; Leoncini, G.; Parodi, A.; Falqui, V.; Ratto, E.; Vettoretti, S.; Bezante, G.P.; Del Sette, M.; Deferrari, G.; et al. Serum uric acid and target organ damage in primary hypertension. Hypertension 2005, 45, 991–996. [Google Scholar] [CrossRef] [Green Version]
- Canepa, M.; Viazzi, F.; Strait, J.B.; Ameri, P.; Pontremoli, R.; Brunelli, C.; Studenski, S.; Ferrucci, L.; Lakatta, E.G.; AlGhatrif, M. Longitudinal Association Between Serum Uric Acid and Arterial Stiffness: Results From the Baltimore Longitudinal Study of Aging. Hypertension 2017, 69, 228–235. [Google Scholar] [CrossRef] [Green Version]
- Yoshitomi, R.; Fukui, A.; Nakayama, M.; Ura, Y.; Ikeda, H.; Oniki, H.; Tsuchihashi, T.; Tsuruya, K.; Kitazono, T. Sex differences in the association between serum uric acid levels and cardiac hypertrophy in patients with chronic kidney disease. Hypertens. Res. Off. J. Jpn. Soc. Hypertens. 2014, 37, 246–252. [Google Scholar] [CrossRef]
- Dalbeth, N.; Merriman, T.R.; Stamp, L.K. Gout. Lancet 2016, 388, 2039–2052. [Google Scholar] [CrossRef]
- Heinig, M.; Johnson, R.J. Role of uric acid in hypertension, renal disease, and metabolic syndrome. Clevel. Clin. J. Med. 2006, 73, 1059–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiner, D.E.; Tighiouart, H.; Elsayed, E.F.; Griffith, J.L.; Salem, D.N.; Levey, A.S. Uric acid and incident kidney disease in the community. J. Am. Soc. Nephrol. 2008, 19, 1204–1211. [Google Scholar] [CrossRef] [Green Version]
- Jordan, D.M.; Choi, H.K.; Verbanck, M.; Topless, R.; Won, H.H.; Nadkarni, G.; Merriman, T.R.; Do, R. No causal effects of serum urate levels on the risk of chronic kidney disease: A Mendelian randomization study. PLoS Med. 2019, 16, e1002725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badve, S.V.; Pascoe, E.M.; Tiku, A.; Boudville, N.; Brown, F.G.; Cass, A.; Clarke, P.; Dalbeth, N.; Day, R.O.; de Zoysa, J.R.; et al. Effects of Allopurinol on the Progression of Chronic Kidney Disease. N. Engl. J. Med. 2020, 382, 2504–2513. [Google Scholar] [CrossRef] [PubMed]
- Doria, A.; Galecki, A.T.; Spino, C.; Pop-Busui, R.; Cherney, D.Z.; Lingvay, I.; Parsa, A.; Rossing, P.; Sigal, R.J.; Afkarian, M.; et al. Serum Urate Lowering with Allopurinol and Kidney Function in Type 1 Diabetes. N. Engl. J. Med. 2020, 382, 2493–2503. [Google Scholar] [CrossRef]
- Sato, Y.; Feig, D.I.; Stack, A.G.; Kang, D.H.; Lanaspa, M.A.; Ejaz, A.A.; Sánchez-Lozada, L.G.; Kuwabara, M.; Borghi, C.; Johnson, R.J. The case for uric acid-lowering treatment in patients with hyperuricaemia and CKD. Nat. Rev. Nephrol. 2019, 15, 767–775. [Google Scholar] [CrossRef]
- Johnson, R.J.; Segal, M.S.; Srinivas, T.; Ejaz, A.; Mu, W.; Roncal, C.; Sanchez-Lozada, L.G.; Gersch, M.; Rodriguez-Iturbe, B.; Kang, D.H.; et al. Essential hypertension, progressive renal disease, and uric acid: A pathogenetic link? J. Am. Soc. Nephrol. 2005, 16, 1909–1919. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Sun, K.; Yang, Y.; Zhang, H.; Hu, F.B.; Hui, R. Plasma uric acid and hypertension in a Chinese community: Prospective study and metaanalysis. Clin. Chem. 2009, 55, 2026–2034. [Google Scholar] [CrossRef] [Green Version]
- Gaffo, A.L.; Saag, K.G. Serum urate, menopause, and postmenopausal hormone use: From eminence to evidence-based medicine. Arthritis Res. Ther. 2008, 10, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akizuki, S. Serum uric acid levels among thirty-four thousand people in Japan. Ann. Rheum. Dis. 1982, 41, 272–274. [Google Scholar] [CrossRef] [Green Version]
- Mumford, S.L.; Dasharathy, S.S.; Pollack, A.Z.; Perkins, N.J.; Mattison, D.R.; Cole, S.R.; Wactawski-Wende, J.; Schisterman, E.F. Serum uric acid in relation to endogenous reproductive hormones during the menstrual cycle: Findings from the BioCycle study. Hum. Reprod. 2013, 28, 1853–1862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollis-Moffatt, J.E.; Xu, X.; Dalbeth, N.; Merriman, M.E.; Topless, R.; Waddell, C.; Gow, P.J.; Harrison, A.A.; Highton, J.; Jones, P.B.; et al. Role of the urate transporter SLC2A9 gene in susceptibility to gout in New Zealand Māori, Pacific Island, and Caucasian case-control sample sets. Arthritis Rheum. 2009, 60, 3485–3492. [Google Scholar] [CrossRef]
- Ichida, K.; Matsuo, H.; Takada, T.; Nakayama, A.; Murakami, K.; Shimizu, T.; Yamanashi, Y.; Kasuga, H.; Nakashima, H.; Nakamura, T.; et al. Decreased extra-renal urate excretion is a common cause of hyperuricemia. Nat. Commun. 2012, 3, 764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuo, H.; Nakayama, A.; Sakiyama, M.; Chiba, T.; Shimizu, S.; Kawamura, Y.; Nakashima, H.; Nakamura, T.; Takada, Y.; Oikawa, Y.; et al. ABCG2 dysfunction causes hyperuricemia due to both renal urate underexcretion and renal urate overload. Sci. Rep. 2014, 4, 3755. [Google Scholar] [CrossRef] [PubMed]
- Tin, A.; Marten, J.; Halperin Kuhns, V.L.; Li, Y.; Wuttke, M.; Kirsten, H.; Sieber, K.B.; Qiu, C.; Gorski, M.; Yu, Z.; et al. Target genes, variants, tissues and transcriptional pathways influencing human serum urate levels. Nat. Genet. 2019, 51, 1459–1474. [Google Scholar] [PubMed] [Green Version]
- Chang, H.Y.; Pan, W.H.; Yeh, W.T.; Tsai, K.S. Hyperuricemia and gout in Taiwan: Results from the Nutritional and Health Survey in Taiwan (1993–1996). J. Rheumatol. 2001, 28, 1640–1646. [Google Scholar]
- Lin, Y.K.; Lin, Y.P.; Lee, J.T.; Lin, C.S.; Wu, T.J.; Tsai, K.Z.; Su, F.Y.; Kwon, Y.; Hoshide, S.; Lin, G.M. Sex-specific association of hyperuricemia with cardiometabolic abnormalities in a military cohort: The CHIEF study. Medicine 2020, 99, e19535. [Google Scholar] [CrossRef]
- Kang, D.H.; Park, S.K.; Lee, I.K.; Johnson, R.J. Uric acid-induced C-reactive protein expression: Implication on cell proliferation and nitric oxide production of human vascular cells. J. Am. Soc. Nephrol. 2005, 16, 3553–3562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bove, M.; Cicero, A.F.; Veronesi, M.; Borghi, C. An evidence-based review on urate-lowering treatments: Implications for optimal treatment of chronic hyperuricemia. Vasc. Health Risk Manag. 2017, 13, 23–28. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Flowchart of participants analyzed in this study.

Figure 2.
Women and men by characteristics before and after propensity weighting.

Figure 3.
Bar chart of uric acid concentrations in each age group.

Figure 4.
Risk of renal progression and CKD per 1 mg/dL increase in serum uric acid by sex. Adjusted for age, CKD, hypertension, diabetes mellitus, dyslipidemia, gout, stroke, BMI, serum creatinine, cigarette smoking, and alcohol consumption.
Figure 4.
Risk of renal progression and CKD per 1 mg/dL increase in serum uric acid by sex. Adjusted for age, CKD, hypertension, diabetes mellitus, dyslipidemia, gout, stroke, BMI, serum creatinine, cigarette smoking, and alcohol consumption.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
The baseline characteristics subjects by sex.
| Characteristic | Women | Men | p-Value |
|---|---|---|---|
| (n = 1856) | (n = 1852) | ||
| Serum uric acid (mg/dL) | 5.49 ± 1.36 | 6.36 ± 1.39 | <0.001 *** |
| Uric Acid status, % | 0.369 | ||
| Without hyperuricemia | 1235 (66.54) | 1259 (67.98) | |
| With hyperuricemia a | 621 (33.46) | 593 (32.02) | |
| Follow-up duration (month) | 33.17 (15.30) | 34.18 (15.42) | 0.046 * |
| Age (years) | 63.77 ± 8.57 | 65.21 ± 9.41 | <0.001 *** |
| Comorbidities, % | |||
| Hypertension | 1124 (60.56) | 1270 (68.57) | <0.001 *** |
| Diabetes mellitus | 766 (41.27) | 768 (41.47) | 0.930 |
| Dyslipidemia | 672 (36.21) | 610 (32.94) | 0.040 * |
| Early-CKD | 859 (46.28) | 1121 (60.53) | <0.001 *** |
| Gout | 118 (6.36) | 382 (20.63) | <0.001 *** |
| Stroke | 87 (4.69) | 148 (7.99) | <0.001 *** |
| Physical examination | |||
| Height (cm) | 154.92 ± 5.66 | 165.89 ± 6.29 | <0.001 *** |
| Weight (kg) | 60.69 ± 10.65 | 70.03 ± 11.04 | <0.001 *** |
| BMI (kg/m2) | 25.27 ± 4.20 | 25.41 ± 3.50 | 0.276 |
| Serum creatinine (mg/dl) | 0.73 ± 0.15 | 1.02 ± 0.19 | <0.001 *** |
| Baseline eGFR (mL/min per 1.73 m2) | 73.63 ± 12.07 | 67.05 ± 11.87 | <0.001 *** |
| SBP (mmHg) | 130.17 ± 18.16 | 131.21 ± 16.34 | 0.092 |
| DBP (mmHg) | 76.02 ± 10.71 | 76.92 ± 11.07 | 0.020 ** |
| Fasting glucose (mg/dl) | 113.91 ± 37.25 | 114.91 ± 34.56 | 0.410 |
| Total cholesterol (mg/dL) | 192.45 ± 39.20 | 179.27 ± 38.37 | <0.001 *** |
| Health-related behaviors, % | |||
| Cigarette smoking | <0.001 *** | ||
| Never smoker | 1801 (97.88) | 1153 (62.94) | |
| Current smoker | 36 (1.96) | 451 (24.62) | |
| Former smoker | 3 (0.16) | 228 (12.62) | |
| Alcohol consumption | 63 (3.43) | 353 (19.34) | <0.001 *** |
Abbreviations: CKD, chronic kidney disease; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure. a Female ≥ 6.0 mg/dL; Male ≥ 7.0 mg/dL. * p < 0.05, ** p < 0.01, *** p < 0.001.
Table 2.
Incidence rate for risk of renal progression (25% decline in GFR) and CKD by uric acid in women and men.
Table 2.
Incidence rate for risk of renal progression (25% decline in GFR) and CKD by uric acid in women and men.
| Gender | Renal Progression (n = 3708) | CKD (n = 1728) | ||||
|---|---|---|---|---|---|---|
| Events, n(%) | Person-Years | IR (95% CI) a | Events, n(%) | Person-Years | IR (95% CI) a | |
| Without Hyperuricemia | 305 | 373 | ||||
| Men | 176 (57.70) | 3619.9 | 4.86 (4.17–5.64) | 189 (50.67) | 1420.5 | 13.31 (11.48–15.34) |
| Women | 129 (42.30) | 3405.6 | 3.79 (3.16–4.50) | 184 (49.33) | 1927.9 | 9.54 (8.22–11.03) |
| With Hyperuricemia b | 196 | 164 | ||||
| Men | 90 (45.92) | 1655.5 | 5.44 (4.37–6.68) | 69 (42.07) | 474.4 | 14.54 (11.32–18.41) |
| Women | 106 (54.08) | 1724.9 | 6.15 (5.03–7.43) | 95 (57.93) | 622.6 | 15.26 (12.35–18.65) |
Abbreviation: CKD, chronic kidney disease; CI, confidence interval; IR, incidence rate. a IR/100 person-years. b Female ≥ 6.0 mg/dL; Male ≥ 7.0 mg/dL.
Table 3.
Risk of renal progression and CKD by hyperuricemia in women and men.
| Gender | Renal Progression, HR (95% CI) | CKD, HR (95% CI) | ||||||
|---|---|---|---|---|---|---|---|---|
| Before Propensity Weighting | After Propensity Weighting | Before Propensity Weighting | After Propensity Weighting | |||||
| Crude | Adjusted a | Crude | Adjusted a | Crude | Adjusted b | Crude | Adjusted b | |
| Without Hyperuricemia | ||||||||
| Men | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Women | 0.81 (0.65–1.02) | 1.93 (1.35–2.77) e | 1.42 (1.10–1.82) d | 2.21 (1.55–3.14) e | 0.71 (0.58–0.87) e | 2.35 (1.63–3.40) e | 1.01 (0.81–1.26) | 2.69 (1.90–3.81) e |
| With Hyperuricemia | ||||||||
| Men | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Women | 1.14 (0.86–1.51) | 2.14 (1.30–3.52) d | 1.28 (0.95–1.73) | 2.14 (1.35–3.40) d | 1.10 (0.80–1.50) | 4.05 (2.17–7.56) e | 1.42 (1.00–2.00) c | 3.56 (2.04–6.25) e |
Abbreviation: CKD, chronic kidney disease; HR, hazard ratio; CI, confidence interval. a Adjusted for age, CKD, hypertension, diabetes mellitus, dyslipidemia, gout, stroke, BMI, serum creatinine, cigarette smoking, and alcohol consumption. b Adjusted for age, hypertension, diabetes mellitus, dyslipidemia, gout, stroke, BMI, serum creatinine, cigarette smoking, and alcohol consumption. c p < 0.05; d p < 0.01; e p < 0.001.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chang, P.-Y.; Chang, Y.-W.; Lin, Y.-F.; Fan, H.-C. Sex-Specific Association of Uric Acid and Kidney Function Decline in Taiwan. J. Pers. Med. 2021, 11, 415. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050415
AMA Style
Chang P-Y, Chang Y-W, Lin Y-F, Fan H-C. Sex-Specific Association of Uric Acid and Kidney Function Decline in Taiwan. Journal of Personalized Medicine. 2021; 11(5):415. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050415
Chicago/Turabian StyleChang, Po-Ya, Yu-Wei Chang, Yuh-Feng Lin, and Hueng-Chuen Fan. 2021. "Sex-Specific Association of Uric Acid and Kidney Function Decline in Taiwan" Journal of Personalized Medicine 11, no. 5: 415. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050415
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.