
Prevalence and Risk Factors of Respiratory Syncytial Virus in Children under 5 Years of Age in the WHO European Region: A Systematic Review and Meta-Analysis

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
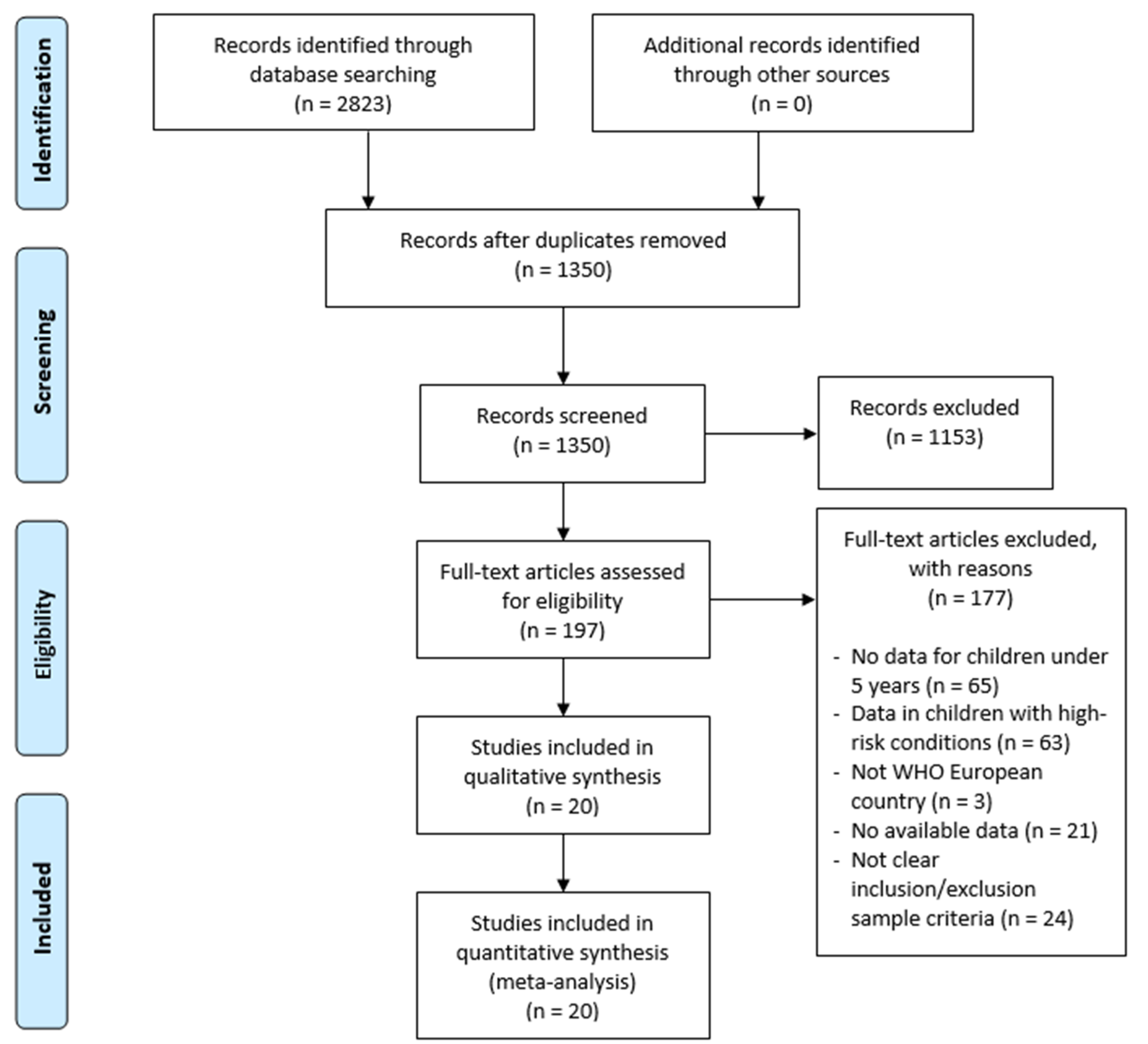
2.2. Study Selection Process
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Quality Evaluation and Risk Bias
2.6. Data Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. Risk Factor (Age)
3.3. Risk Factor (Gender and Weight at Birth)
3.4. Risk Factor (Seasonality)
3.5. Environmental Risk Factors
3.6. Another Risk Factors
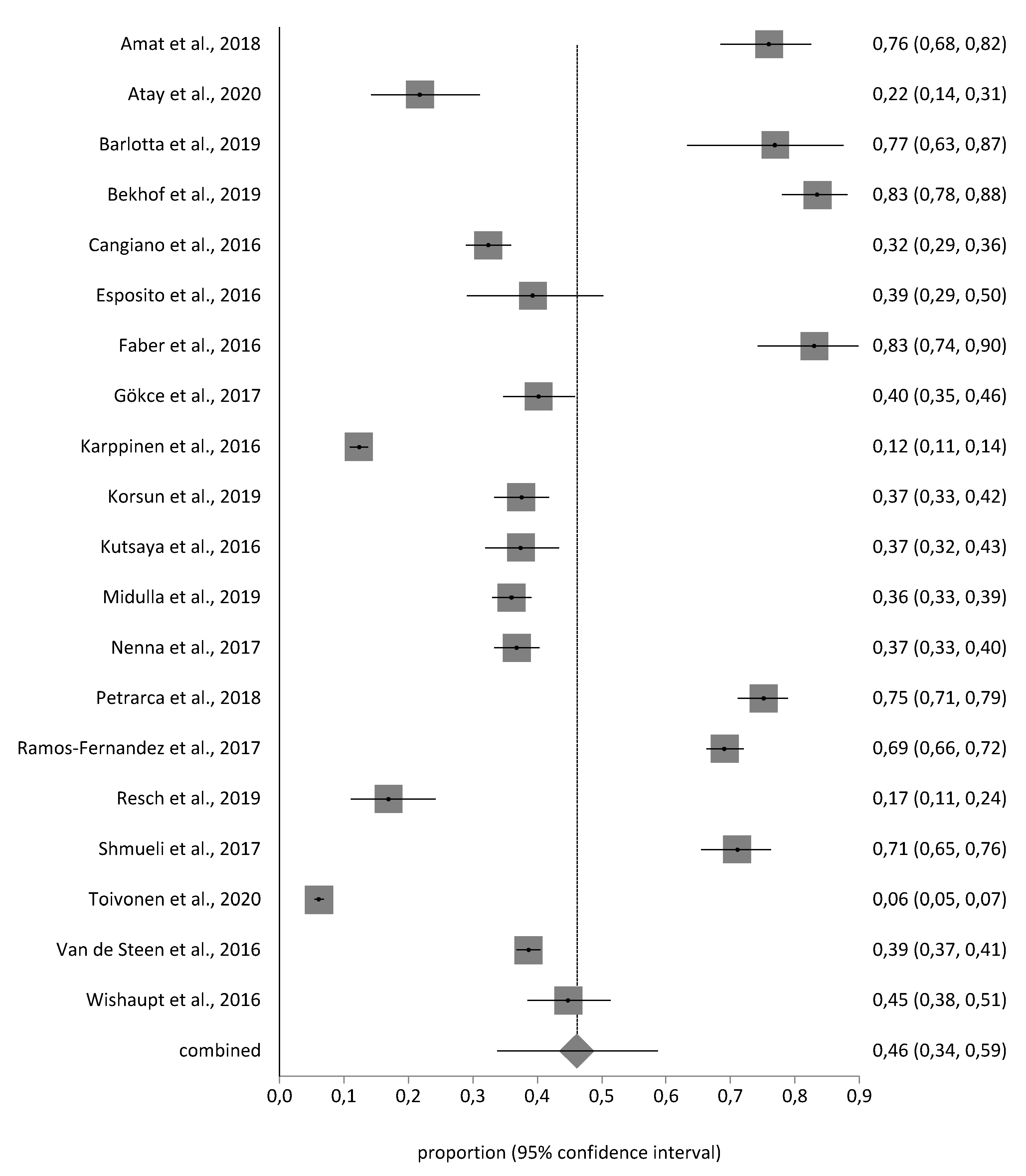
3.7. Meta-Analysis Prevalence Estimation
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pellegrinelli, L.; Galli, C.; Bubba, L.; Cereda, D.; Anselmi, G.; Binda, S.; Gramegna, M.; Pariani, E. Respiratory syncytial virus in influenza-like illness cases: Epidemiology and molecular analyses of four consecutive winter seasons (2014–2015/2017–2018) in Lombardy (Northern Italy). J. Med. Virol. 2020, 92, 2999–3006. [Google Scholar] [CrossRef]
- Simões, E.A.F.; DeVincenzo, J.P.; Boeckh, M.; Bont, L.; Crowe, J.E.; Griffiths, P.; Hayden, F.G.; Hodinka, R.L.; Smyth, R.L.; Spencer, K.; et al. Challenges and opportunities in developing respiratory syncytial virus therapeutics. J. Infect. Dis. 2015, 211, S1–S20. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Strategy to Pilot Global Respiratory Syncytial Virus Surveillance Based on the Global Influenza Surveillance and Response System (GISRS); World Health Organization: Geneva, Switzerland, 2017; Available online: https://apps.who.int/iris/handle/10665/259853 (accessed on 20 December 2020).
- Shi, T.; McAllister, D.A.; O’Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: A systematic review and modelling study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Reeves, R.M.; Wang, X.; Bassat, Q.; Brooks, W.A.; Cohen, C.; Moore, D.P.; Nunes, M.; Rath, B.; Campbell, H.; et al. Global patterns in monthly activity of influenza virus, respiratory syncytial virus, parainfluenza virus, and metapneumovirus: A systematic analysis. Lancet Glob. Health 2019, 7, e1031–e1045. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.; Taylor, R.J.; Lustig, R.L.; Schuck-Paim, C.; Haguinet, F.; Webb, D.J.; Logie, J.; Matias, G.; Fleming, D.M. Modelling estimates of the burden of respiratory syncytial virus infection in children in the UK. BMJ Open 2016, 6, e009337. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Lu, R.; Shen, J.; Xie, Z.; Liu, G.; Tan, W. Comparison of viral and epidemiological profiles of hospitalized children with severe acute respiratory infection in Beijing and Shanghai, China. BMC Infect. Dis. 2019, 19, 729. [Google Scholar] [CrossRef]
- Checchia, P.A.; Paes, B.; Bont, L.; Manzoni, P.; Simões, E.A.F.; Fauroux, B.; Figueras-Aloy, J.; Carbonell-Estrany, X. Defining the Risk and Associated Morbidity and Mortality of Severe Respiratory Syncytial Virus Infection Among Infants with Congenital Heart Disease. Infect. Dis. Ther. 2017, 6, 37–56. [Google Scholar] [CrossRef] [Green Version]
- Paes, B.; Fauroux, B.; Figueras-Aloy, J.; Bont, L.; Checchia, P.A.; Simões, E.A.F.; Manzoni, P.; Carbonell-Estrany, X. Defining the Risk and Associated Morbidity and Mortality of Severe Respiratory Syncytial Virus Infection Among Infants with Chronic Lung Disease. Infect. Dis. Ther. 2016, 5, 453–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Löwensteyn, Y.N.; Phijffer, E.W.E.M.; Simons, J.V.L.; Scheltema, N.M.; Mazur, N.I.; Nair, H.; Bont, L.J. Respiratory syncytial virus-related death in children with down syndrome: The RSV GOLD Study. Pediatr. Infect. Dis. J. 2020, 39, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.J.; Carosone-Link, P.; Yogev, R.; Yi, J.; Simões, E.A.F. Effectiveness of Palivizumab in High-risk Infants and Children: A Propensity Score Weighted Regression Analysis. Pediatr. Infect. Dis. J. 2017, 36, 699–704. [Google Scholar] [CrossRef] [Green Version]
- Mazur, N.I.; Martinón-Torres, F.; Baraldi, E.; Fauroux, B.; Greenough, A.; Heikkinen, T.; Manzoni, P.; Mejias, A.; Nair, H.; Papadopoulos, N.G.; et al. Lower respiratory tract infection caused by respiratory syncytial virus: Current management and new therapeutics. Lancet Respir. Med. 2015, 3, 888–900. [Google Scholar] [CrossRef]
- Higgins, D.; Trujillo, C.; Keech, C. Advances in RSV vaccine research and development—A global agenda. Vaccine 2016, 34, 2870–2875. [Google Scholar] [CrossRef] [PubMed]
- Ventre, K.; Randolph, A. Ribavirin for respiratory syncytial virus infection of the lower respiratory tract in infants and young children. Cochrane Database Syst. Rev. 2010, 5, CD000181. [Google Scholar] [CrossRef]
- Modjarrad, K.; Giersing, B.; Kaslow, D.C.; Smith, P.G.; Moorthy, V.S. WHO consultation on Respiratory Syncytial Virus Vaccine Development Report from a World Health Organization Meeting held on 23–24 March 2015. Vaccine 2016, 34, 190–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reeves, R.M.; Hardelid, P.; Panagiotopoulos, N.; Minaji, M.; Warburton, F.; Pebody, R. Burden of hospital admissions caused by respiratory syncytial virus (RSV) in infants in England: A data linkage modelling study. J. Infect. 2019, 78, 468–475. [Google Scholar] [CrossRef] [Green Version]
- Tam, J.; Papenburg, J.; Fanella, S.; Asner, S.; Barton, M.; Bergeron, C.; Desai, S.; Hui, C.; Foo, C.; Langley, J.M.; et al. Pediatric investigators collaborative network on infections in Canada study of respiratory syncytial virus-associated deaths in pediatric patients in Canada, 2003–2013. Clin. Infect. Dis. 2019, 68, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Cai, W.; Buda, S.; Schuler, E.; Hirve, S.; Zhang, W.; Haas, W. Risk factors for hospitalized respiratory syncytial virus disease and its severe outcomes. Influenza Other Respir. Viruses 2020, 14, 658–670. [Google Scholar] [CrossRef] [Green Version]
- Broberg, E.K.; Waris, M.; Johansen, K.; Snacken, R.; Penttinen, P.; Trebbien, R.; Emborg, H.D.; Krause, T.G.; Fischer, T.K.; Kuznetsova, N.; et al. Seasonality and geographical spread of respiratory syncytial virus epidemics in 15 european countries, 2010 to 2016. Eurosurveillance 2018, 23, 17–00284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalg, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H. The Oxford 2011 Levels of Evidence. Available online: https://www.cebm.net/2016/05/ocebm-levels-of-evidence (accessed on 5 December 2020).
- Sanderson, S.; Tatt, I.D.; Higgins, J.P.T. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: A systematic review and annotated bibliography. Int. J. Epidemiol. 2007, 36, 666–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Amat, F.; Plantard, C.; Mulliez, A.; Petit, I.; Rochette, E.; Verdan, M.; Henquell, C.; Labbé, G.; Heraud, M.C.; Evrard, B.; et al. RSV-hRV co-infection is a risk factor for recurrent bronchial obstruction and early sensitization 3 years after bronchiolitis. J. Med. Virol. 2018, 90, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Atay, Ö.; Pekcan, S.; Göktürk, B.; Özdemir, M. Risk factors and clinical determinants in bronchiolitis of infancy. Turk. Thorac. J. 2020, 21, 156–162. [Google Scholar] [PubMed]
- Barlotta, A.; Pirillo, P.; Stocchero, M.; Donato, F.; Giordano, G.; Bont, L.; Zanconato, S.; Carraro, S.; Baraldi, E. Metabolomic profiling of infants with recurrent wheezing after bronchiolitis. J. Infect. Dis. 2019, 219, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Bekhof, J.; Wessels, M.; ten Velde, E.; Hoekstra, M.; Langenhorst, V.; Bruijnesteijn, L.; Brand, P.L.P.; Ruijs, G.J.H.M. Room Sharing in Hospitalized Children with Bronchiolitis and the Occurrence of Hospital-Acquired Infections: A Prospective Cohort Study. Hosp. Pediatr. 2019, 9, 415–422. [Google Scholar] [CrossRef]
- Cangiano, G.; Nenna, R.; Frassanito, A.; Evangelisti, M.; Nicolai, A.; Scagnolari, C.; Pierangeli, A.; Antonelli, G.; Papoff, P.; Petrarca, L.; et al. Bronchiolitis: Analysis of 10 consecutive epidemic seasons. Pediatr. Pulmonol. 2016, 51, 1330–1335. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Scarselli, E.; Lelii, M.; Scala, A.; Vitelli, A.; Capone, S.; Fornili, M.; Biganzoli, E.; Orenti, A.; Nicosia, A.; et al. Antibody response to respiratory syncytial virus infection in children <18 months old. Hum. Vaccines Immunother. 2016, 12, 1700–1706. [Google Scholar]
- Faber, T.E.; Schuurs, T.A.; Veeger, N.J.G.M.; Hennus, M.P.; Bont, L.J. Dynamics of nasopharyngeal pneumococcal carriage during the course of viral bronchiolitis. Pediatr. Pulmonol. 2016, 51, 863–867. [Google Scholar] [CrossRef] [PubMed]
- Gökçe, Ş.; Kurugöl, Z.; Koturoğlu, G.; Çiçek, C.; Aslan, A. Etiology, Seasonality, and Clinical Features of Viral Respiratory Tract Infections in Children Hospitalized With Acute Bronchiolitis: A Single-Center Study. Glob. Pediatr. Health 2017, 4, 2333794X1771437. [Google Scholar] [CrossRef]
- Karppinen, S.; Toivonen, L.; Schuez-Havupalo, L.; Waris, M.; Peltola, V. Interference between respiratory syncytial virus and rhinovirus in respiratory tract infections in children. Clin. Microbiol. Infect. 2016, 22, e1–e208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korsun, N.; Angelova, S.; Trifonova, I.; Georgieva, I.; Voleva, S.; Tzotcheva, I.; Mileva, S.; Ivanov, I.; Tcherveniakova, T.; Perenovska, P. Viral pathogens associated with acute lower respiratory tract infections in children younger than 5 years of age in Bulgaria. Braz. J. Microbiol. 2019, 50, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Kutsaya, A.; Teros-Jaakkola, T.; Kakkola, L.; Toivonen, L.; Peltola, V.; Waris, M.; Julkunen, I. Prospective clinical and serological follow-up in early childhood reveals a high rate of subclinical RSV infection and a relatively high reinfection rate within the first 3 years of life. Epidemiol. Infect. 2016, 144, 1622–1633. [Google Scholar] [CrossRef] [PubMed]
- Midulla, F.; Nenna, R.; Scagnolari, C.; Petrarca, L.; Frassanito, A.; Viscido, A.; Arima, S.; Antonelli, G.; Pierangeli, A. How Respiratory Syncytial Virus Genotypes Influence the Clinical Course in Infants Hospitalized for Bronchiolitis. J. Infect. Dis. 2019, 219, 526–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nenna, R.; Evangelisti, M.; Frassanito, A.; Scagnolari, C.; Pierangeli, A.; Antonelli, G.; Nicolai, A.; Arima, S.; Moretti, C.; Papoff, P.; et al. Respiratory syncytial virus bronchiolitis, weather conditions and air pollution in an Italian urban area: An observational study. Environ. Res. 2017, 158, 188–193. [Google Scholar] [CrossRef]
- Petrarca, L.; Nenna, R.; Frassanito, A.; Pierangeli, A.; Leonardi, S.; Scagnolari, C.; Antonelli, G.; Papoff, P.; Moretti, C.; Midulla, F. Acute bronchiolitis: Influence of viral co-infection in infants hospitalized over 12 consecutive epidemic seasons. J. Med. Virol. 2018, 90, 631–638. [Google Scholar] [CrossRef]
- Ramos-Fernández, J.M.; Moreno-Pérez, D.; Gutiérrez-Bedmar, M.; Hernández-Yuste, A.; Cordón-Martínez, A.M.; Milano-Manso, G.; Urda-Cardona, A. Predicción de la evolución de la bronquiolitis por virus respiratorio sincitial en lactantes menores de 6 meses. Rev. Esp. Salud Publica 2017, 91, 201701006. [Google Scholar]
- Resch, B.; Wörner, C.; Özdemir, S.; Hubner, M.; Puchas, C.; Urlesberger, B. Respiratory Syncytial Virus Associated Hospitalizations in Infants of 33 to 42 Weeks’ Gestation: Does Gestational Age Matter? Klin. Padiatr. 2019, 231, 206–211. [Google Scholar]
- Shmueli, E.; Berger, T.; Herman, Y.A.; Chodick, G.; Rom, E.; Bilavsky, E.; Ashkenazi-Hoffnung, L.; Ashkenazi, S.; Amir, J.; Prais, D. Real-life comparison of three general paediatric wards showed similar outcomes for children with bronchiolitis despite different treatment regimens. Acta Paediatr. Int. J. Paediatr. 2017, 106, 1507–1511. [Google Scholar] [CrossRef]
- Toivonen, L.; Karppinen, S.; Schuez-Havupalo, L.; Teros-Jaakkola, T.; Mertsola, J.; Waris, M.; Peltola, V. Respiratory syncytial virus infections in children 0–24 months of age in the community. J. Infect. 2020, 80, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Van de Steen, O.; Miri, F.; Gunjaca, M.; Klepac, V.; Gross, B.; Notario, G.; Wegzyn, C.M. The Burden of Severe Respiratory Syncytial Virus Disease Among Children Younger than 1 Year in Central and Eastern Europe. Infect. Dis. Ther. 2016, 5, 125–137. [Google Scholar] [CrossRef] [Green Version]
- Wishaupt, J.; Van Den Berg, E.; Van Wijk, T.; Van Der Ploeg, T.; Versteegh, F.; Hartwig, N. Paediatric apnoeas are not related to a specific respiratory virus, and parental reports predict hospitalisation. Acta Paediatr. Int. J. Paediatr. 2016, 105, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Bardach, A.; Rey-Ares, L.; Cafferata, M.L.; Cormick, G.; Romano, M.; Ruvinsky, S.; Savy, V. Systematic review and meta-analysis of respiratory syncytial virus infection epidemiology in Latin America. Rev. Med. Virol. 2014, 24, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Kenmoe, S.; Bigna, J.J.; Well, E.A.; Simo, F.B.N.; Penlap, V.B.; Vabret, A.; Njouom, R. Prevalence of human respiratory syncytial virus infection in people with acute respiratory tract infections in Africa: A systematic review and meta-analysis. Influenza Other Respi. Viruses 2018, 12, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yuan, L.; Zhang, Y.; Zhang, X.; Zheng, M.; Kyaw, M.H. Burden of respiratory syncytial virus infections in China: Systematic review and meta-analysis. J. Glob. Health 2015, 5, 020417. [Google Scholar] [CrossRef]
- Gaymard, A.; Bouscambert-Duchamp, M.; Pichon, M.; Frobert, E.; Vallee, J.; Lina, B.; Casalegno, J.S.; Morfin, F. Genetic characterization of respiratory syncytial virus highlights a new BA genotype and emergence of the ON1 genotype in Lyon, France, between 2010 and 2014. J. Clin. Virol. 2018, 102, 12–18. [Google Scholar] [CrossRef]
- Hasegawa, K.; Linnemann, R.W.; Avadhanula, V.; Mansbach, J.M.; Piedra, P.A.; Gern, J.E.; Camargo, C.A. Detection of respiratory syncytial virus and rhinovirus in healthy infants. BMC Res. Notes 2015, 8, 718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirve, S.; Crawford, N.; Palekar, R.; Zhang, W.; Bancej, C.; Barr, I.; Baumeister, E.; Broor, S.; Burmaa, A.; Campbell, H.; et al. Clinical characteristics, predictors, and performance of case definition—Interim results from the WHO global respiratory syncytial virus surveillance pilot. Influenza Other Respir. Viruses 2019, 14, 647–657. [Google Scholar] [CrossRef] [Green Version]
- Güllü, E.İ.; Akın, Y.; Karaaslan, A.; Vayvada, E.R.; Atabek, A.A.; Narter, F.K. RSV infection in Istanbul: Risk factors and frequency. J. Infect. Dev. Ctries 2017, 11, 691–696. [Google Scholar] [CrossRef] [Green Version]
- Amini, R.; Gilca, R.; Boucher, F.D.; Charest, H.; De Serres, G. Respiratory syncytial virus contributes to more severe respiratory morbidity than influenza in children <2 years during seasonal influenza peaks. Infection 2019, 47, 595–601. [Google Scholar] [CrossRef]
- Cattoir, L.; Vankeerberghen, A.; Boel, A.; Van Vaerenbergh, K.; De Beenhouwer, H. Epidemiology of RSV and hMPV in Belgium: A 10-year follow-up. Acta Clin. Belg. Int. J. Clin. Lab. Med. 2019, 74, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Yassine, H.M.; Sohail, M.U.; Younes, N.; Nasrallah, G.K. Systematic review of the respiratory syncytial virus (RSV) prevalence, genotype distribution, and seasonality in children from the middle east and North Africa (MENA) region. Microorganisms 2020, 8, 713. [Google Scholar] [CrossRef] [PubMed]
- Reeves, R.M.; van Wijhe, M.; Tong, S.; Lehtonen, T.; Stona, L.; Teirlinck, A.C.; Fernandez, L.V.; Li, Y.; Giaquinto, C.; Fischer, T.K.; et al. Respiratory Syncytial Virus-Associated Hospital Admissions in Children Younger Than 5 Years in 7 European Countries Using Routinely Collected Datasets. J. Infect. Dis. 2020, 222, S599–S605. [Google Scholar] [CrossRef]
- Tsou, P.; Vadivelan, A.; Kovvuri, M.; Garg, N.; Thangavelu, M.; Wang, Y.; Raj, S. Association between multiple respiratory viral infections and pediatric intensive care unit admission among infants with bronchiolitis. Arch. Pediatr. 2020, 27, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Oliveira-Santos, M.; Santos, J.A.; Soares, J.; Dias, A.; Quaresma, M. Influence of meteorological conditions on RSV infection in Portugal. Int. J. Biometeorol. 2016, 60, 1807–1817. [Google Scholar] [CrossRef]
- Relić, T.; Ilić, N.; Kostić, G.; Jovanović, D.; Tambur, Z.; Lazarević, I. Respiratory syncytial virus infection and bronchial hyperreactivity in children up to two years of age in correlation with atopy. Vojnosanit. Pregl. 2016, 73, 59–65. [Google Scholar] [CrossRef]
- Jepsen, M.T.; Trebbien, R.; Emborg, H.D.; Krause, T.G.; Schønning, K.; Voldstedlund, M.; Nielsen, J.; Fischer, T.K. Incidence and seasonality of respiratory syncytial virus hospitalisations in young children in Denmark, 2010 to 2015. Eurosurveillance 2018, 23, 17–00163. [Google Scholar] [CrossRef] [Green Version]
- Kramer, R.; Duclos, A.; Lina, B.; Casalegno, J.S. Cost and burden of RSV related hospitalisation from 2012 to 2017 in the first year of life in Lyon, France. Vaccine 2018, 36, 6591–6593. [Google Scholar] [CrossRef]
- Vandini, S.; Bottau, P.; Faldella, G.; Lanari, M. Immunological, viral, environmental, and individual factors modulating lung immune response to respiratory syncytial virus. Biomed Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [Green Version]
- Nicolai, A.; Frassanito, A.; Nenna, R.; Cangiano, G.; Petrarca, L.; Papoff, P.; Pierangeli, A.; Scagnolari, C.; Moretti, C.; Midulla, F. Risk factors for virus-induced acute respiratory tract infections in children younger than 3 years and recurrent wheezing at 36 months follow-up after discharge. Pediatr. Infect. Dis. J. 2017, 36, 179–183. [Google Scholar] [CrossRef]
- Feldman, A.S.; He, Y.; Moore, M.L.; Hershenson, M.B.; Hartert, T.V. Toward primary prevention of asthma: Reviewing the evidence for early-life respiratory viral infections as modifiable risk factors to prevent childhood asthma. Am. J. Respir. Crit. Care Med. 2015, 191, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Wildenbeest, J.G.; Zuurbier, R.P.; Korsten, K.; van Houten, M.A.; Billard, M.N.; Derksen-Lazet, N.; Snape, M.D.; Drysdale, S.B.; Robinson, H.; Pollard, A.J.; et al. Respiratory Syncytial Virus Consortium in Europe (RESCEU) Birth Cohort Study: Defining the Burden of Infant Respiratory Syncytial Virus Disease in Europe. J. Infect. Dis. 2020, 222, S606–S612. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author, (Year), Country. | Study Design/Period | Age | Diagnostic Laboratory Procedure | Sample Size Positive Cases | Setting | Prevalence | EL/RG |
|---|---|---|---|---|---|---|---|
| Amat et al. [25] 2018 France | Cohort study 2011–2012 | <3 years | Antigen tests/FEIA | N = 154 n = 117 | Outpatients and hospitalized children | 75.9% | 2b/B |
| Atay et al. [26] 2020 Turkey | Cross sectional study 2011–2012 | 2 months–2 years | PCR | N = 101 n = 22 | Inpatient or outpatient clinics | 21.78% | 2c/B |
| Barlotta et al. [27] 2019 Italy | Cohort study 2013–2014 | <1 year | PCR | N = 52 n = 40 | Inpatient ward | 76% | 2b/B |
| Bekhof et al. [28] 2019 Netherlands | Cohort study 2012–2016 | <2 years | PCR | N = 218 n = 182 | Inpatient ward | 83.4% | 2b/B |
| Cangiano et al. [29] 2016 Italy | Cross sectional 2004–2014 | <1 years | PCR | N = 723 n = 234 | Inpatient ward | 32.36% | 2c/B |
| Esposito et al. [30] 2016 Italy | Cohort study 2013 | <18 months | PCR | N = 89 n = 35 | Inpatient ward | 39.3% | 2b/B |
| Faber et al. [31] 2016 Netherlands | Cohort study | <13 months | PCR | N = 100 n = 83 | Inpatient ward | 83% | 2b/B |
| Gökçe et al. [32] 2017 Turkey | Cross sectional study 2013–2016 | <2 years | PCR | N = 316 n = 127 | Inpatient ward | 40.1% | 2b/B |
| Karppinen et al. [33] 2016 Finland | Cohort study 2005–2012 | <2 years | PCR | N = 2275 n = 279 | Inpatient ward | 12.26% | 2b/B |
| Korsun et al. [34] 2019 Bulgaria | Cohort study 2015–2018 | <5 years | PCR | N = 515 n = 193 | Inpatient or outpatient patients | 37.5% | 2b/B |
| Kutsaya et al. [35] 2016 Finland | Cohort study 2009–2013 | <1 years | PCR | N = 291 n = 109 | Inpatient patients | 37.45% | 2b/B |
| Midulla et al. [36] 2019 Italy | Cohort study 2005–2012 | <1 years | PCR | N = 998 n = 359 | Inpatient ward | 35.97% | 2b/B |
| Nenna et al. [37] 2017 Italy | Cohort study 2004–2014 | <1 years | PCR | N = 723 n = 266 | Inpatient ward | 36.79% | 2b/B |
| Petrarca et al. [38] 2018 Italy | Cross sectional 2004–2016 | <1 years | PCR | N = 486 n = 365 | Inpatient ward | 75.1% | 2b/B |
| Ramos-Fernández et al. [39] 2017 Spain | Case-control study2010–2015 | <6 months | Antigen tests | N = 1006 n = 695 | Inpatient ward | 69% | 1b/A |
| Resch et al. [40] 2019 Austria | Cohort study 2005–2015 | 39–42 weeks | PCR | N = 136 n = 23 | Inpatient ward | 16.9% | 2b/B |
| Shmueli et al. [41] 2017 Israel | Cohort study 2012–2013 | <2 years | Antigen tests/FEIA | N = 286 n = 203 | Inpatient ward | 70.9% | 2b/B |
| Toivonen et al. [42] 2020 Finland | Cohort study 2008–2010 | <2 years | Antigen tests/PCR | N = 4728 n = 289 | Inpatient or outpatient clinics | 6% | 2b/B |
| Van de Steen et al. [43] 2016 Central and Eastern Europe countries 1 | Cohort study 2009–2011 | <1 years | Antigen tests | N = 2677 n = 1034 | Inpatient ward | 38.62% | 2b/B |
| Wishaupt et al. [44] 2016 Netherlands | Cohort study 2011–2014 | <3 months | PCR | N = 241 n = 108 | Inpatient ward | 40.14% | 2b/B |
| Author, (year) | Risk Factors |
|---|---|
| Atay et al. [26], 2020 | Male gender (OR 1.73, 95% CI 1.0–5.7%, p = 0.302) Crowded household population (OR 1.73, 95% CI 1.0–5.7%, p = 0.046) Heating stoves (OR 0.31, 95% CI 0.1–0.98%, p = 0.025) Urban cities (p < 0.001) Exposure to smoking (p = 0.001) Peak February |
| Cangiano et al. [29], 2016 | Younger (p < 0.001) Peak December–February Maternal smoke during pregnancy (p = 0.036) |
| Esposito et al. [30], 2016 | Age (OR 6.3, 95% CI 1.4–33.9%, p = 0.02) Age ≥ 5 months old (children 5–8 months old and 9–16 months old vs. children 0–4 months old: p = 0.03 and p = 0.003, respectively) Attended day care (p = 0.001) Birth date (OR 2.7, 95% CI 1.1–6.7%, p = 0.03) Male gender (OR 2.3, 95% CI 1.0–5.7%, p = 0.06) |
| Gökçe et al. [32], 2017 | Peak January–March Younger (<6 months) |
| Karppinen et al. [33], 2016 | Male (OR 1.06, 95% CI 0.57–1.99%, p = 0.85) Socioeconomic status (OR 0.78, 95% CI 0.39–1.56%, p = 0.48) |
| Korsun et al. [34], 2019 | Youngest age group: <6 months (50%), followed by 6–11 months (38.5%) Of the RSV-positive children 58.5% were under 2 years of age: 61% were boys and 39% were girls (p = 0.5773) |
| Kutsaya et al. [35], 2016 | RSV seroprevalence increased from 37% at age 1 year to 68% at age 2 years, and to 86% at age 3 years |
| Midulla et al. [36], 2019 | Younger (p < 0.0001) Lower body weight at admission (p = 0.005) Born in winter |
| Nenna et al. [37], 2017 | The number of RSV-positive infants correlated negatively with cold temperature (r = −0.46, p < 0.001), and positively with higher relative humidity (r = 0.36, p < 0.001) Peak December–February |
| Petrarca et al. [38], 2018 | No relation to exposure to smoke, breastfeeding, birth weight and sex |
| Ramos-Fernández et al. [39], 2017 | Male (OR 4.27, 95% CI 1.14–15.93%, p = 0.03) Low birth weight (<3rd percentile) (OR 5.53, 95% CI 0.93–32.97%, p = 0.06) |
| Resch et al. [40], 2019 | No relation to smoking during pregnancy Peak January |
| Toivonen et al. [42], 2020 | Of all RSV infections, 10% occurred before 3 months of age, 16% at 3–5 months of age, 32% at 6–11 months of age, and 42% at 12–24 months of age Peak February–May |
| Van de Steen et al. [43], 2016 | Duration of hospitalization (p < 0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suleiman-Martos, N.; Caballero-Vázquez, A.; Gómez-Urquiza, J.L.; Albendín-García, L.; Romero-Béjar, J.L.; Cañadas-De la Fuente, G.A. Prevalence and Risk Factors of Respiratory Syncytial Virus in Children under 5 Years of Age in the WHO European Region: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 416. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050416
Suleiman-Martos N, Caballero-Vázquez A, Gómez-Urquiza JL, Albendín-García L, Romero-Béjar JL, Cañadas-De la Fuente GA. Prevalence and Risk Factors of Respiratory Syncytial Virus in Children under 5 Years of Age in the WHO European Region: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2021; 11(5):416. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050416
Chicago/Turabian StyleSuleiman-Martos, Nora, Alberto Caballero-Vázquez, Jose Luis Gómez-Urquiza, Luis Albendín-García, Jose Luis Romero-Béjar, and Guillermo A. Cañadas-De la Fuente. 2021. "Prevalence and Risk Factors of Respiratory Syncytial Virus in Children under 5 Years of Age in the WHO European Region: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 11, no. 5: 416. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050416