
Lincp21-RNA as Predictive Response Marker for Preoperative Chemoradiotherapy in Rectal Cancer

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. RNA Extraction and lincRNA-p21 Quantification
2.3. Statistical Methods
3. Results
3.1. Patient Characteristics
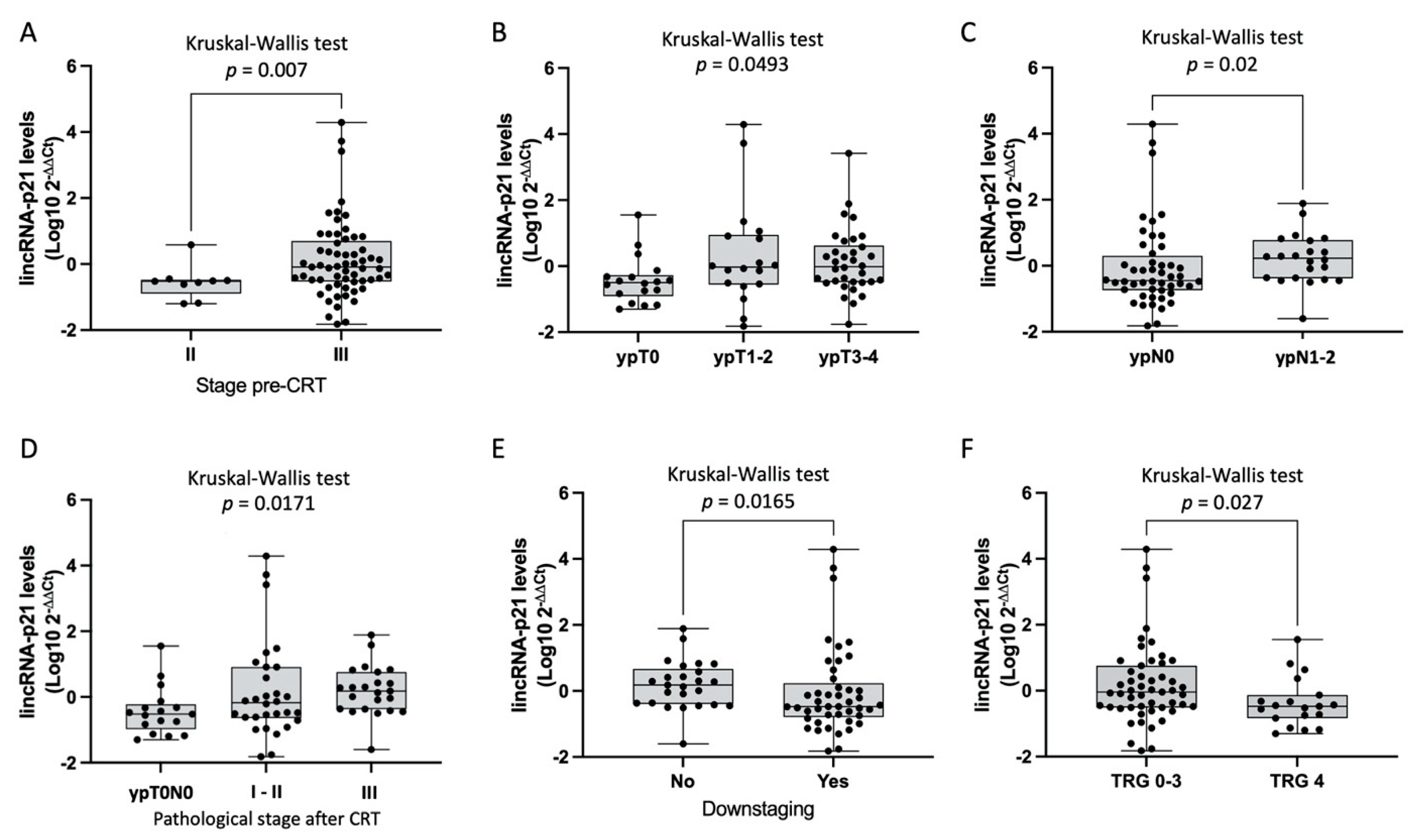
3.2. LincRNA-p21 Expression Levels
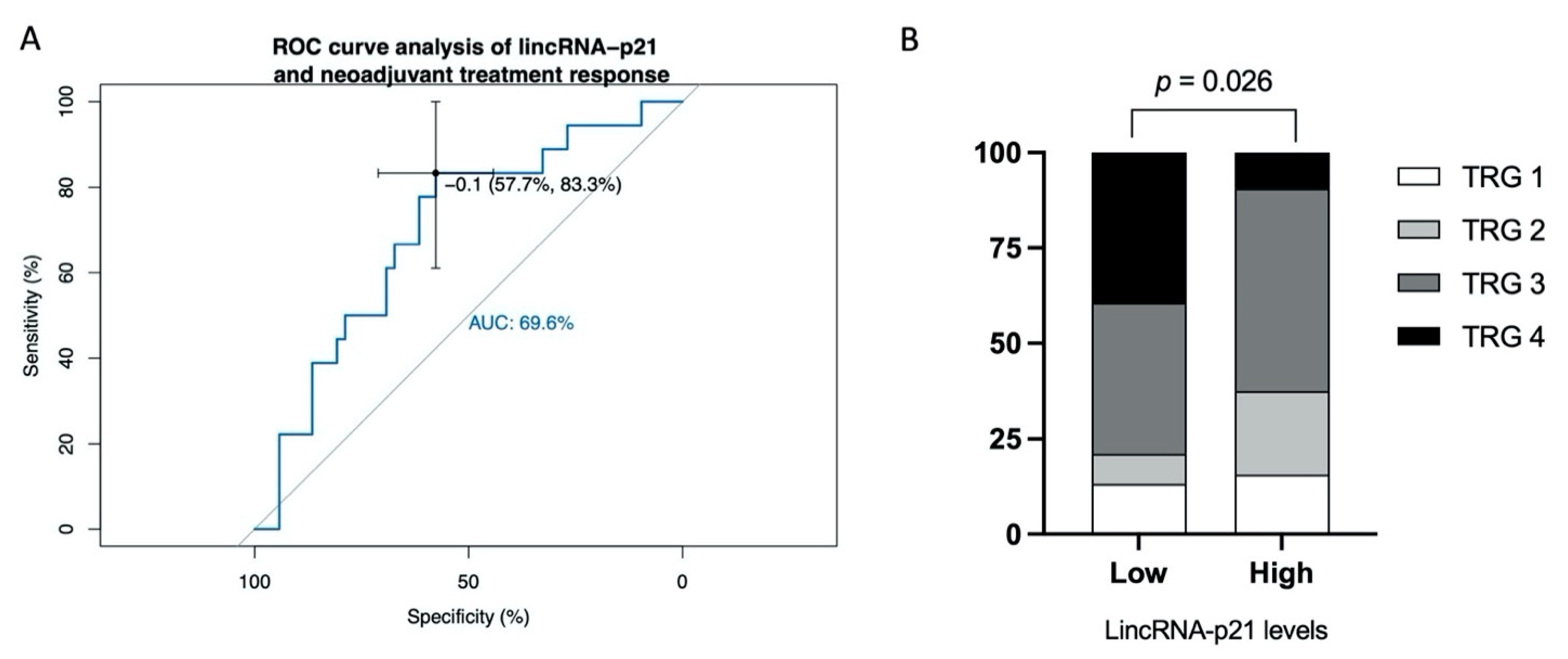
3.3. Predictive Ability of lincRNA-p21 for Response to CRT
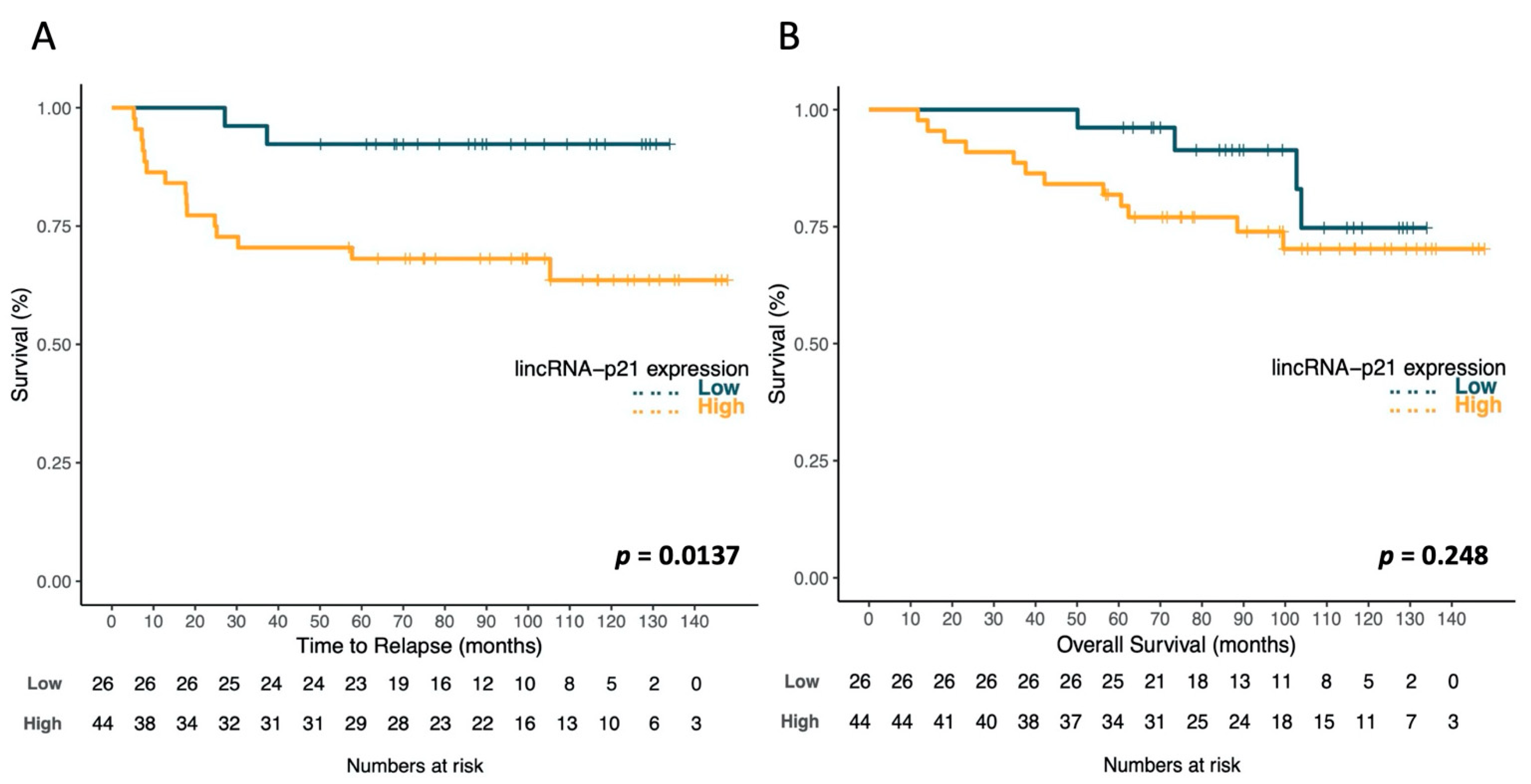
3.4. LincRNA-p21 Expression and Survival
3.5. Multivariate Analysis of TTR and OS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Wei, E.K.; Giovannucci, E.; Wu, K.; Rosner, B.; Fuchs, C.S.; Willett, W.C.; Colditz, G.A. Comparison of risk factors for colon and rectal cancer. Int. J. Cancer 2003, 108, 433–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkegaard, H.; Johnsen, N.F.; Christensen, J.; Frederiksen, K.; Overvad, K.; Tjønneland, A. Association of adherence to lifestyle recommendations and risk of colorectal cancer: A prospective Danish cohort study. BMJ 2010, 341, c5504. [Google Scholar] [CrossRef] [Green Version]
- Guinney, J.; Dienstmann, R.; Wang, X.; De Reyniès, A.; Schlicker, A.; Soneson, C.; Marisa, L.; Roepman, P.; Nyamundanda, G.; Angelino, P.; et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 2015, 21, 1350–1356. [Google Scholar] [CrossRef]
- Bosset, J.-F.; Calais, G.; Mineur, L.; Maingon, P.; Stojanovic-Rundic, S.; Bensadoun, R.-J.; Bardet, E.; Beny, A.; Ollier, J.-C.; Bolla, M.; et al. Fluorouracil-based adjuvant chemotherapy after preoperative chemoradiotherapy in rectal cancer: Long-term results of the EORTC 22921 randomised study. Lancet Oncol. 2014, 15, 184–190. [Google Scholar] [CrossRef]
- Sainato, A.; Nunzia, V.C.L.; Valentini, V.; De Paoli, A.; Maurizi, E.R.; Lupattelli, M.; Aristei, C.; Vidali, C.; Conti, M.; Galardi, A.; et al. No benefit of adjuvant Fluorouracil Leucovorin chemotherapy after neoadjuvant chemoradiotherapy in locally advanced cancer of the rectum (LARC): Long term results of a randomized trial (I-CNR-RT). Radiother. Oncol. 2014, 113, 223–229. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef]
- Rödel, C.; Martus, P.; Papadoupolos, T.; Füzesi, L.; Klimpfinger, M.; Fietkau, R.; Liersch, T.; Hohenberger, W.; Raab, R.; Sauer, R.; et al. Prognostic Significance of Tumor Regression After Preoperative Chemoradiotherapy for Rectal Cancer. J. Clin. Oncol. 2005, 23, 8688–8696. [Google Scholar] [CrossRef] [PubMed]
- Sell, N.M.; Qwaider, Y.Z.; Goldstone, R.N.; Cauley, C.E.; Cusack, J.C.; Ricciardi, R.; Bordeianou, L.G.; Berger, D.L.; Kunitake, H. Ten-year survival after pathologic complete response in rectal adenocarcinoma. J. Surg. Oncol. 2021, 123, 293–298. [Google Scholar] [CrossRef]
- Kasi, A.; Abbasi, S.; Handa, S.; Al-Rajabi, R.; Saeed, A.; Baranda, J.; Sun, W. Total Neoadjuvant Therapy vs Standard Therapy in Locally Advanced Rectal Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2030097. [Google Scholar] [CrossRef]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [Green Version]
- Deng, S.; Calin, G.A.; Croce, C.M.; Coukos, G.; Zhang, L. Mechanisms of microRNA deregulation in human cancer. Cell Cycle 2008, 7, 2643–2646. [Google Scholar] [CrossRef] [PubMed]
- Bartel, D.P. MicroRNAs: Target Recognition and Regulatory Functions. Cell 2009, 136, 215–233. [Google Scholar] [CrossRef] [Green Version]
- Djebali, S.; Davis, C.A.; Merkel, A.; Dobin, A.; Lassmann, T.; Mortazavi, A.; Tanzer, A.; Lagarde, J.; Lin, W.; Schlesinger, F.; et al. Landscape of transcription in human cells. Nature 2012, 489, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Gutschner, T.; Diederichs, S. The hallmarks of cancer: A long non-coding RNA point of view. RNA Biol. 2012, 9, 703–719. [Google Scholar] [CrossRef] [Green Version]
- Galamb, O.; Barták, B.K.; Kalmár, A.; Nagy, Z.B.; Szigeti, K.A.; Tulassay, Z.; Igaz, P.; Molnár, B. Diagnostic and prognostic potential of tissue and circulating long non-coding RNAs in colorectal tumors. World J. Gastroenterol. 2019, 25, 5026–5048. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Castellano, J.J.; Moreno, I.; Martínez-Rodenas, F.; Hernandez, R.; Canals, J.; Diaz, T.; Han, B.; Muñoz, C.; Biete, A.; et al. LincRNA-p21 Levels Relates to Survival and Post-Operative Radiotherapy Benefit in Rectal Cancer Patients. Life 2020, 10, 172. [Google Scholar] [CrossRef]
- Necsulea, A.; Soumillon, M.; Warnefors, M.; Liechti, A.; Daish, T.; Zeller, U.; Baker, J.C.; Grützner, F.; Kaessmann, H. The evolution of lncRNA repertoires and expression patterns in tetrapods. Nat. Cell Biol. 2014, 505, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Washietl, S.; Kellis, M.; Garber, M. Evolutionary dynamics and tissue specificity of human long noncoding RNAs in six mammals. Genome Res. 2014, 24, 616–628. [Google Scholar] [CrossRef] [Green Version]
- Yan, X.; Hu, Z.; Feng, Y.; Hu, X.; Yuan, J.; Zhao, S.D.; Zhang, Y.; Yang, L.; Shan, W.; He, Q.; et al. Comprehensive Genomic Characterization of Long Non-coding RNAs across Human Cancers. Cancer Cell 2015, 28, 529–540. [Google Scholar] [CrossRef] [Green Version]
- Huarte, M.; Guttman, M.; Feldser, D.; Garber, M.; Koziol, M.J.; Kenzelmann-Broz, D.; Khalil, A.M.; Zuk, O.; Amit, I.; Rabani, M.; et al. A Large Intergenic Noncoding RNA Induced by p53 Mediates Global Gene Repression in the p53 Response. Cell 2010, 142, 409–419. [Google Scholar] [CrossRef] [Green Version]
- Castellano, J.J.; Navarro, A.; Vinõlas, N.; Marrades, R.M.; Moises, J.; Santanach, A.C.; Saco, A.; Muñoz, C.; Fuster, D.; Molins, L.; et al. LincRNA-p21 Impacts Prognosis in Resected Non-Small Cell Lung Cancer Patients through Angiogenesis Regulation. J. Thorac. Oncol. 2016, 11, 2173–2182. [Google Scholar] [CrossRef]
- Yang, F.; Zhang, H.; Mei, Y.; Wu, M. Reciprocal Regulation of HIF-1α and LincRNA-p21 Modulates the Warburg Effect. Mol. Cell 2014, 53, 88–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, G.; Li, Z.; Zhao, Q.; Zhu, Y.; Zhao, C.; Li, X.; Ma, Z.; Li, X.; Zhang, Y. LincRNA-p21 enhances the sensitivity of radiotherapy for human colorectal cancer by targeting the Wnt/β-catenin signaling pathway. Oncol. Rep. 2014, 31, 1839–1845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhai, H.; Fesler, A.; Schee, K.; Fodstad, Ø.; Flatmark, K.; Ju, J. Clinical Significance of Long Intergenic Noncoding RNA-p21 in Colorectal Cancer. Clin. Color. Cancer 2013, 12, 261–266. [Google Scholar]
- Dworak, O.; Keilholz, L.; Hoffmann, A. Pathological features of rectal cancer after preoperative radiochemotherapy. Int. J. Color. Dis. 1997, 12, 19–23. [Google Scholar] [CrossRef]
- Campayo, M.; Navarro, A.; Benítez, J.C.; Santasusagna, S.; Ferrer, C.; Monzó, M.; Cirera, L. miR-21, miR-99b and miR-375 combination as predictive response signature for preoperative chemoradiotherapy in rectal cancer. PLoS ONE 2018, 13, e0206542. [Google Scholar] [CrossRef]
- Robin, X.A.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Muller, M.J. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Camp, R.L.; Dolled-Filhart, M.; Rimm, D.L. X-tile: A new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin. Cancer Res. 2004, 10, 7252–7259. [Google Scholar] [CrossRef] [Green Version]
- Chaleshi, V.; Irani, S.; Alebouyeh, M.; Mirfakhraie, R.; Aghdaei, H.A. Association of lncRNA-p53 regulatory network (lincRNA-p21, lincRNA-ROR and MALAT1) and p53 with the clinicopathological features of colorectal primary lesions and tumors. Oncol. Lett. 2020, 19, 3937–3949. [Google Scholar]
- Melo, C.A.; Léveillé, N.; Rooijers, K.; Wijchers, P.J.; Geeven, G.; Tal, A.; Melo, S.A.; De Laat, W.; Agami, R. A p53-bound enhancer region controls a long intergenic noncoding RNA required for p53 stress response. Oncogene 2016, 35, 4399–4406. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.; Yang, X.; Li, J.; Yang, W.; Ma, H.; Zhang, Z. p53-targeted lincRNA-p21 acts as a tumor suppressor by inhibiting JAK2/STAT3 signaling pathways in head and neck squamous cell carcinoma. Mol. Cancer 2019, 18, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.; Kim, C.; Ku, J.-L.; Kim, W.; Yoon, S.K.; Kuh, H.-J.; Lee, J.-H.; Nam, S.W.; Lee, E.K. A long non-coding RNA snaR contributes to 5-fluorouracil resistance in human colon cancer cells. Mol. Cells 2014, 37, 540–546. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Q.; Zhan, H.; Lin, F.; Liu, Y.; Yang, K.; Gao, Q.; Ding, M.; Liu, Y.; Huang, W.; Cai, Z. LincRNA-p21 suppresses glutamine catabolism and bladder cancer cell growth through inhibiting glutaminase expression. Biosci. Rep. 2019, 39, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ning, Y.; Yong, F.; Haibin, Z.; Hui, S.; Nan, Z.; Guangshun, Y. LincRNA-p21 activates endoplasmic reticulum stress and inhibits hepatocellular carcinoma. Oncotarget 2015, 6, 28151–28163. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number of Patients (%) | TTR p-Value | OS p-Value | |
|---|---|---|---|---|
| Sex | Male | 49 (70) | 0.203 | 0.269 |
| Female | 21 (30) | |||
| Median age (range) | 66 (38–82) | |||
| <60 | 19 (27.1) | 0.679 | 0.815 | |
| >60 | 51 (72.9) | |||
| Clinical stage pre-CRT | II | 9 (12.9) | 0.585 | 0.497 |
| III | 61 (87.1) | |||
| Adjuvant therapy | No | 27 (33.8) | 0.776 | 0.130 |
| 5-FLU | 7 (8.7) | |||
| FOLFOX | 40 (50) | |||
| Other | 6 (7.5) | |||
| ypT | ypT0 | 18 (25.7) | 0.015 | 0.051 |
| ypT1–2 | 18 (25.7) | |||
| ypT3–4 | 34 (48.6) | |||
| ypN | ypN0 | 48 (68.6) | 0.003 | 0.044 |
| ypN1–2 | 22 (31.4) | |||
| Pathological stage after neoadjuvant CRT | ypT0N0 | 17 (24.2) | 0.024 | 0.133 |
| I | 16 (22.9) | |||
| II | 14 (20) | |||
| III | 23 (32.9) | |||
| Downstaging | No | 25 (35.7) | 0.001 | 0.010 |
| Yes | 45 (64.3) | |||
| Tumor regression grade (TRG) | 0–3 | 52 (74.3) | 0.324 | 0.161 |
| 4 | 18 (25.7) |
| Factors | OR (95% CI) | p-Value |
|---|---|---|
| Stage II at diagnosis | 1.703 (0.363–8.003) | 0.500 |
| Age | 0.980(0.918–1.046) | 0.549 |
| Gender male | 2.756 (0.682–11.137) | 0.155 |
| CEA at baseline | 0.930 (0.809–1.068) | 0.301 |
| LincRNA-p21 levels | 0.485 (0.237–0.992) | 0.047 |
| Constant | 0.307 | <0.001 |
| Time to Relapse | HR (95% CI) | p-Value |
| Pathological stage > I | 4.430 (1.266–15.497) | 0.020 |
| No downstaging | 1.737 (0.350–8.621) | 0.499 |
| High lincRNA-p21 | 4.458 (1.014–19.603) | 0.048 |
| Overall Survival | HR (95% CI) | p-Value |
| Pathological stage > I | 2.020 (0.362–11.273) | 0.423 |
| No downstaging | 3.512 (1.275–9.673) | 0.015 |
| High lincRNA-p21 | 1.387 (0.411–4.679) | 0.598 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benitez, J.C.; Campayo, M.; Díaz, T.; Ferrer, C.; Acosta-Plasencia, M.; Monzo, M.; Cirera, L.; Besse, B.; Navarro, A. Lincp21-RNA as Predictive Response Marker for Preoperative Chemoradiotherapy in Rectal Cancer. J. Pers. Med. 2021, 11, 420. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050420
Benitez JC, Campayo M, Díaz T, Ferrer C, Acosta-Plasencia M, Monzo M, Cirera L, Besse B, Navarro A. Lincp21-RNA as Predictive Response Marker for Preoperative Chemoradiotherapy in Rectal Cancer. Journal of Personalized Medicine. 2021; 11(5):420. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050420
Chicago/Turabian StyleBenitez, Jose Carlos, Marc Campayo, Tania Díaz, Carme Ferrer, Melissa Acosta-Plasencia, Mariano Monzo, Luis Cirera, Benjamin Besse, and Alfons Navarro. 2021. "Lincp21-RNA as Predictive Response Marker for Preoperative Chemoradiotherapy in Rectal Cancer" Journal of Personalized Medicine 11, no. 5: 420. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11050420