
Effects of Inositol Hexaphosphate and Myo-Inositol Administration in Breast Cancer Patients during Adjuvant Chemotherapy

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Intervention
2.3. Blood Sample Collection
2.4. Quality-of-Life
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Blood Parameters and Quality of Life between Inositol Group and Control Group at Baseline (T0)
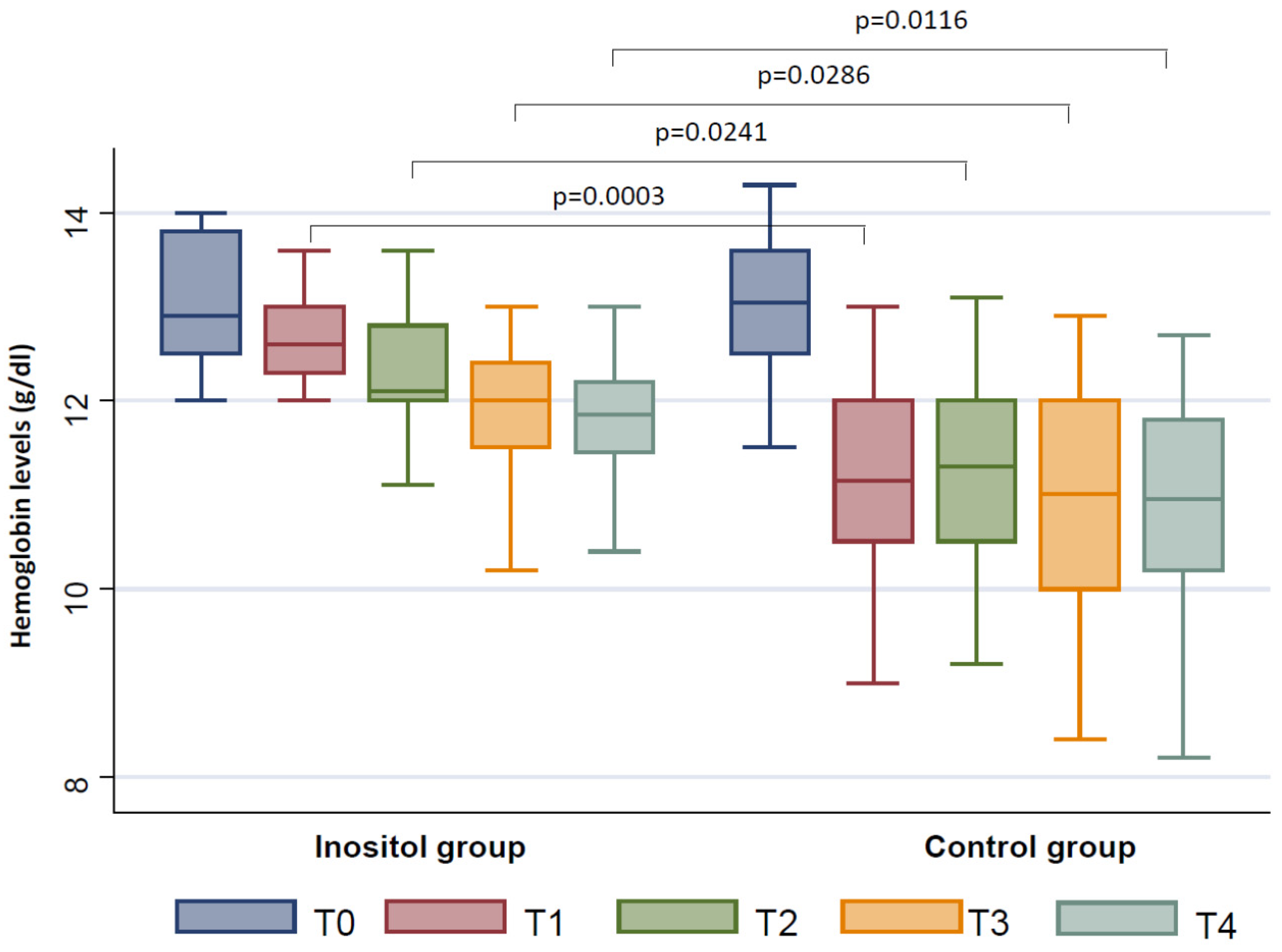
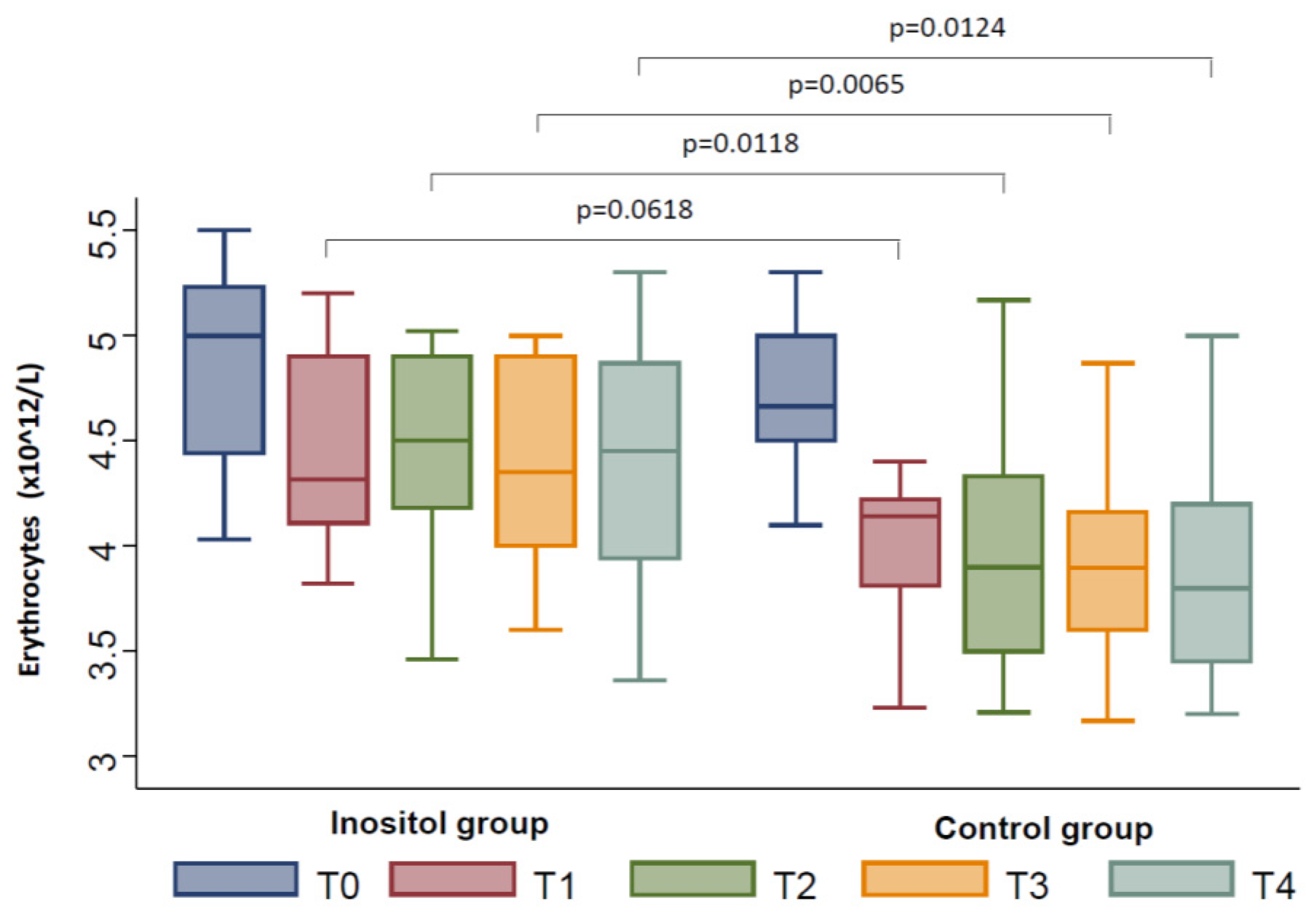
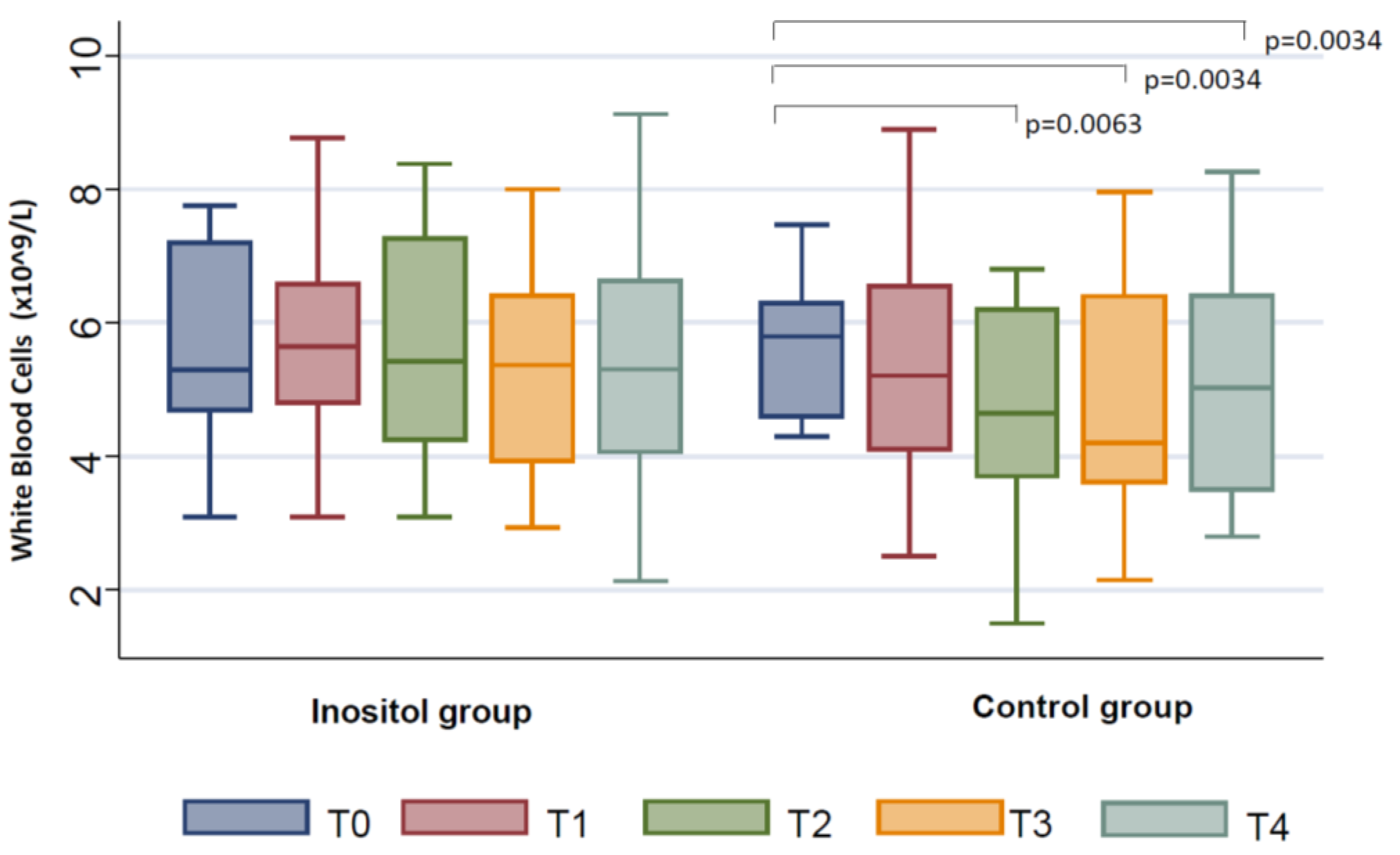
3.3. Changes from Baseline in Blood Parameters between Inositol Group and Control Group during the Follow-Up (T1–T4)
3.4. Changes from Baseline in EORTC Questionnaire Scores in the Inositol Group and in the Control Group during the Follow-Up (T1-T4)
3.5. Differences between Inositol Group and Control Group during the Follow-Up (T1–T4) in EORTC Questionnaire Scores
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Breast Cancer. Available online: https://www.wcrf.org/dietandcancer/breast-cancer (accessed on 12 April 2021).
- DeSantis, C.E.; Ma, J.; Gaudet, M.M.; Newman, L.A.; Miller, K.D.; Goding Sauer, A.; Jemal, A.; Siegel, R.L. Breast cancer statistics. CA Cancer J. Clin. 2019, 69, 438–451. [Google Scholar] [CrossRef] [PubMed]
- De Luca, A.; Frusone, F.; Buzzacchino, F.; Amabile, M.I.; Taffurelli, M.; Del Mastro, L.; Rutgers, E.J.T.; Sacchini, V.; Caruso, F.; Minelli, M.; et al. First Surgical National Consensus Conference of the Italian Breast Surgeons association (ANISC) on breast cancer management in neoadjuvant setting: Results and summary. Eur. J. Surg. Oncol. 2021, 47, 1913–1919. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Liu, Z.; Du, S.; Li, J.; Ma, L.; Li, L. Diagnosis and Treatment of Breast Cancer in the Precision Medicine Era. Methods Mol. Biol. 2020, 2204, 53–61. [Google Scholar] [CrossRef]
- Erickson, V.S.; Pearson, M.L.; Ganz, P.A.; Adams, J.; Kahn, K.L. Arm edema in breast cancer patients. J. Natl. Cancer Inst. 2001, 93, 96–111. [Google Scholar] [CrossRef] [Green Version]
- Hidding, J.T.; Beurskens, C.H.; van der Wees, P.J.; van Laarhoven, H.W.; Nijhuis-van der Sanden, M.W. Treatment related impairments in arm and shoulder in patients with breast cancer: A systematic review. PLoS ONE 2014, 9, e96748. [Google Scholar] [CrossRef] [PubMed]
- De Luca, A.; Tripodi, D.; Frusone, F.; Leonardi, B.; Cerbelli, B.; Botticelli, A.; Vergine, M.; D’Andrea, V.; Pironi, D.; Sorrenti, S.; et al. Retrospective Evaluation of the Effectiveness of a Synthetic Glue and a Fibrin-Based Sealant for the Prevention of Seroma Following Axillary Dissection in Breast Cancer Patients. Front. Oncol. 2020, 10, 1061. [Google Scholar] [CrossRef] [PubMed]
- Groenvold, M. Health-related quality of life in early breast cancer. Dan. Med. Bull. 2010, 57, B4184. [Google Scholar] [PubMed]
- Beaulac, S.M.; McNair, L.; Scott, T.; Lamorte, W.W.; Kavanah, M.T. Lymphedema and quality of life in survivors of early-stage breast cancer. Arch. Surg. 2002, 137, 1253–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rietman, J.; Dijkstra, P.; Hoekstra, H.; Eisma, W.; Szabo, B.; Groothoff, J.; Geertzen, J. Late morbidity after treatment of breast cancer in relation to daily activities and quality of life: A systematic review. Eur. J. Surg. Oncol. 2003, 29, 229–238. [Google Scholar] [CrossRef] [Green Version]
- Gunasekaran, G.H.; Hassali, M.A.B.A.; Sabri, W.M.A.B.W.; Bin Rahman, M.T. Impact of chemotherapy schedule modification on breast cancer patients: A single-centre retrospective study. Int. J. Clin. Pharm. 2020, 42, 642–651. [Google Scholar] [CrossRef]
- Graf, E.; Eaton, J.W. Antioxidant functions of phytic acid. Free Radic. Biol. Med. 1990, 8, 61–69. [Google Scholar] [CrossRef]
- Bizzarri, M.; Dinicola, S.; Bevilacqua, A.; Cucina, A. Broad Spectrum Anticancer Activity of Myo-Inositol and Inositol Hexakisphosphate. Int. J. Endocrinol. 2016, 2016, 5616807. [Google Scholar] [CrossRef] [Green Version]
- Lamarre, Y.; Bourgeaux, V.; Pichon, A.; Hardeman, M.R.; Campion, Y.; Hardeman-Zijp, M.; Martin, C.; Richalet, J.-P.; Bernaudin, F.; Driss, F.; et al. Effect of inositol hexaphosphate-loaded red blood cells (RBCs) on the rheology of sickle RBCs. Transfusion 2013, 53, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.P.; Agarwal, C.; Agarwal, R. Inositol hexaphosphate inhibits growth, and induces G1 arrest and apoptotic death of prostate carcinoma DU145 cells: Modulation of CDKI-CDK-cyclin and pRb-related protein-E2F complexes. Carcinogenesis 2003, 24, 555–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minini, M.; Senni, A.; Unfer, V.; Bizzarri, M. The Key Role of IP6K: A Novel Target for Anticancer Treatments? Molecules. 2020, 25, 4401. [Google Scholar] [CrossRef]
- Duncan, A.M. The role of nutrition in the prevention of breast cancer. AACN Clin. Issues 2004, 15, 119–135. [Google Scholar] [CrossRef]
- Molfino, A.; Amabile, M.I.; Mazzucco, S.; Biolo, G.; Farcomeni, A.; Ramaccini, C.; Antonaroli, S.; Monti, M.; Muscaritoli, M. Effect of Oral Docosahexaenoic Acid (DHA) Supplementation on DHA Levels and Omega-3 Index in Red Blood Cell Membranes of Breast Cancer Patients. Front. Physiol. 2017, 8, 549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamsuddin, A.M.; Yang, G.Y.; Vucenik, I. Novel anti-cancer functions of IP6: Growth inhibition and differentiation of human mammary cancer cell lines in vitro. Anticancer Res. 1996, 16, 3287–3292. [Google Scholar] [PubMed]
- Tantivejkul, K.; Vucenik, I.; Eiseman, J.; Shamsuddin, A.M. Inositol hexaphosphate (IP6) enhances the anti-proliferative effects of adriamycin and tamoxifen in breast cancer. Breast Cancer Res. Treat. 2003, 79, 301–312. [Google Scholar] [CrossRef]
- Bacić, I.; Druzijanić, N.; Karlo, R.; Skifić, I.; Jagić, S. Efficacy of IP6 + inositol in the treatment of breast cancer patients receiving chemotherapy: Prospective, randomized, pilot clinical study. J. Exp. Clin. Cancer Res. 2010, 29, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proietti, S.; Pasta, V.; Cucina, A.; Aragona, C.; Palombi, E.; Vucenik, I.; Bizzarri, M. Inositol hexaphosphate (InsP6) as an effective topical treatment for patients receiving adjuvant chemotherapy after breast surgery. Eur. Rev. Med. Pharmacol. Sci. 2017, 21 (Suppl. 2), 43–50. [Google Scholar] [PubMed]
- Shamsuddin, A.M.; Ullah, A.; Chakravarthy, A.K. Inositol and inositol hexaphosphate suppress cell proliferation and tumor formation in CD-1 mice. Carcinogenesis 1989, 10, 1461–1463. [Google Scholar] [CrossRef]
- Vucenik, I.; Yang, G.Y.; Shamsuddin, A.M. Inositol hexaphosphate and inositol inhibit DMBA-induced rat mammary cancer. Carcinogenesis 1995, 16, 1055–1058. [Google Scholar] [CrossRef] [PubMed]
- Grases, F.; Isern, B.; Perelló, J.; Sanchis, P.; Prieto, R.M. Absorption of myo-inositol hexakisphosphate (InsP6) through the skin: Study of the matrix effects. Mechanism of phytate topical absorption. Front. Biosci. 2005, 10, 799–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grases, F.; Isern, B.; Perelló, J.; Sanchis, P.; Prieto, R.M.; Costa-Bauzà, A. Absorption of myo-inositol hexakisphosphate (InsP6) through the skin in humans. Pharmazie 2006, 61, 652. [Google Scholar]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The Europen Organisation for Research and Treatment of Cancer QLQC30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Fayers, P.M.; Aaronson, N.K.; Bjordal, K.; Groenvold, M.; Curran, D.; Bottomley, A. The EORTC QLQ-C30 Scoring Manual. European Organisation for Research and Treatment of Cancer; European Organisation for Research and Treatment of Cancer: Brussels, Belgium, 2001. [Google Scholar]
- Bourgeaux, V.; Aufradet, E.; Campion, Y.; De Souza, G.; Horand, F.; Bessaad, A.; Chevrier, A.-M.; Canet-Soulas, E.; Godfrin, Y.; Martin, C. Efficacy of homologous inositol hexaphosphate-loaded red blood cells in sickle transgenic mice. Br. J. Haematol. 2012, 157, 357–369. [Google Scholar] [CrossRef]
- Vucenik, I. Anticancer Properties of Inositol Hexaphosphate and Inositol: An Overview. J. Nutr. Sci. Vitaminol. 2019, 65, S18–S22. [Google Scholar] [CrossRef] [Green Version]
- Wyatt, G.; Sikorskii, A.; Tesnjak, I.; Victorson, D.; Srkalovic, G. Chemotherapy interruptions in relation to symptom severity in advanced breast cancer. Support. Care Cancer 2015, 23, 3183–3191. [Google Scholar] [CrossRef] [Green Version]
- Kimura, M.; Usami, E.; Yoshimura, T. Association between severe neutropenia and progression-free survival in patients with advanced or recurrent breast cancer treated with palbociclib. Pharmazie 2020, 75, 662–665. [Google Scholar] [CrossRef]
- Wee, Y.; Yang, C.H.; Chen, S.K.; Yen, Y.C.; Wang, C.S. Inositol hexaphosphate modulates the behavior of macrophages through alteration of gene expression involved in pathways of pro- and anti-inflammatory responses, and resolution of inflammation pathways. Food Sci. Nutr. 2021, 9, 3240–3249. [Google Scholar] [CrossRef] [PubMed]
- Chatree, S.; Thongmaen, N.; Tantivejkul, K.; Sitticharoon, C.; Vucenik, I. Role of Inositols and Inositol Phosphates in Energy Metabolism. Molecules 2020, 25, 5079. [Google Scholar] [CrossRef]
- Pasta, V.; Dinicola, S.; Giuliani, A.; Harrath, A.H.; Alwasel, S.H.; Tartaglia, F.; Cucina, A.; Bizzarri, M. A Randomized Pilot Study of Inositol in Association with Betaine and Boswellia in the Management of Mastalgia and Benign Breast Lump in Premenopausal Women. Breast Cancer 2016, 10, 37–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasta, V.; Gullo, G.; Giuliani, A.; Harrath, A.H.; Alwasel, S.H.; Tartaglia, F.; Cucina, A.; Bizzarri, M. An association of boswellia, betaine and myo-inositol (Eumastós) in the treatment of mammographic breast density: A randomized, double-blind study. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 4419–4426. [Google Scholar]
- Onomi, S.; Okazaki, Y.; Katayama, T. Effect of dietary level of phytic acid on hepatic and serum lipid status in rats fed a high-sucrose diet. Biosci. Biotechnol. Biochem. 2004, 68, 1379–1381. [Google Scholar] [CrossRef]
- Kamp, D.W.; Israbian, V.A.; Yeldandi, A.V.; Panos, R.J.; Graceffa, P.; Weitzman, S.A. Phytic acid, an iron chelator, attenuates pulmonary inflammation and fibrosis in rats after intratracheal instillation of asbestos. Toxicol. Pathol. 1995, 23, 689–695. [Google Scholar] [CrossRef]
- Di Sabatino, A.; Jackson, C.; Pickard, K.M.; Buckley, M.J.; Rovedatti, L.; Leakey, N.A.B.; Picariello, L.; Cazzola, P.; Monteleone, G.; Tonelli, F.; et al. Transforming growth factor beta signalling and matrix metalloproteinases in the mucosa overlying Crohn’s disease strictures. Gut 2009, 58, 777–789. [Google Scholar] [CrossRef]
- Chhetri, D.R. Myo-Inositol and Its Derivatives: Their Emerging Role in the Treatment of Human Diseases. Front. Pharmacol. 2019, 10, 1172. [Google Scholar] [CrossRef] [Green Version]
- Urrila, A.S.; Hakkarainen, A.; Castaneda, A.; Paunio, T.; Marttunen, M.; Lundbom, N. Frontal cortex Myo-inositol is associated with sleep and depression in adolescents: A proton magnetic resonance spectroscopy study. Neuropsychobiology 2017, 75, 21–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molfino, A.; Gioia, G.; Rossi Fanelli, F.; Laviano, A. Contribution of Neuroinflammation to the Pathogenesis of Cancer Cachexia. Mediat. Inflamm. 2015, 2015, 801685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molfino, A.; de van der Schueren, M.A.; Sánchez-Lara, K.; Milke, P.; Amabile, M.I.; Imbimbo, G.; Di Lazzaro, L.; Cavuto, S.; Ronzani, G.; Snegovoy, A.; et al. Cancer-associated anorexia: Validity and performance overtime of different appetite tools among patients at their first cancer diagnosis. Clin. Nutr. 2021, 40, 4037–4042. [Google Scholar] [CrossRef] [PubMed]
- Amabile, M.I.; Frusone, F.; De Luca, A.; Tripodi, D.; Imbimbo, G.; Lai, S.; D’Andrea, V.; Sorrenti, S.; Molfino, A. Locoregional Surgery in Metastatic Breast Cancer: Do Concomitant Metabolic Aspects Have a Role on the Management and Prognosis in this Setting? J. Pers. Med. 2020, 10, 227. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Participants N = 36 | Inositol Group N = 18 | Control Group N = 18 |
|---|---|---|
| Age, years | 52.0 (48.0; 62.0) | 58.0 (53.0; 69.0) |
| Body weight, kg | 65.0 (63.0; 77.0) | 64.00 (62.0; 70.0) |
| BMI, weight (kg)/height2 (m) | 25.1 (23.4; 27.9) | 25.3 (23.9; 26.8) |
| RBC, ×1012/L | 5.0 (4.44; 5.23) | 4.7 (4.54; 5.0) |
| Hb levels, g/dL | 12.9 (12.5; 13.8) | 13.05 (12.5; 13.6) |
| WBC, ×109/L | 5.3 (4.7; 7.2) | 5.8 (4.6; 6.3) |
| Comorbidities: | ||
| Diabetes mellitus (y/no) | 0/18 | 0/18 |
| Arterial hypertensione (y/no) | 4/14 | 4/14 |
| Hyperlipidemia (y/no) | 2/16 | 3/15 |
| Type of breast surgery | ||
| Breast conserving surgery/ | ||
| Mastectomy, n | 6/12 | 7/11 |
| Type of axillary surgery | ||
| SLN biopsy/ALND, n | 10/8 | 11/7 |
| Tumor diameter, cm | 2.0 (1.2; 2.24) | 1.6 (1.23; 2.5) |
| Removed axillary lymph nodes, n | 5.0 (3.0; 6.0) | 4.0 (2.0; 11.0) |
| All Participants N = 36 | Inositol Group N = 18 | p Value | Control Group N = 18 | p Value | |
|---|---|---|---|---|---|
| QLQ-BR23 Functional scales | |||||
| Body image | T0 (baseline) | 83.3 (66.7; 91.7) | 79.2 (66.7; 91.7) | ||
| T1–T0 | 0.0 (−8.3; 8.3) | >0.99 | −8.3 (−25.0; 0.0) | 0.0007 | |
| T2–T0 | −8.3 (−25.0; 0.0) | 0.1484 | −8.3 (−33.3; 0.0) | 0.001 | |
| T3–T0 | −16.7 (−33.3; 0.0) | 0.0085 | −8.3 (−58.3; 0.0) | 0.0065 | |
| T4–T0 | −16.7 (−33.3; 0.0) | 0.0175 | −8.3 (−58.3; 0.0) | 0.0044 | |
| QLQ-BR23 Symptom scales | |||||
| Systemic therapy side effects T0 | 4.8 (0.0; 14.3) | 4.7 (0.0; 14.3) | |||
| T1–T0 | 19.1 (9.5; 3.8) | 0.001 | 38.1 (19.1; 52.4) | <0.0001 | |
| T2–T0 | 14.3 (4.8; 28.6) | 0.0002 | 33.3 (16.7; 52.4) | <0.0001 | |
| T3–T0 | 19.1 (7.1; 40.5) | 0.0002 | 42.9 (23.8; 52.4) | <0.0001 | |
| T4–T0 | 28.6 (14.3; 57.1) | 0.0001 | 52.4 (30.9; 69.1) | <0.0001 | |
| Breast symptoms | T0 (baseline) | 16.7 (8.3; 25.0) | 8.3 (0.0; 41.7) | ||
| T1–T0 | 0.0 (−16.7; 0.0) | 0.1465 | 0.0 (0.0; 8.3) | 0.418 | |
| T2–T0 | −4.2 (−16.7; 0.0) | 0.1216 | 0.0 (−8.3; 8.3) | 0.4906 | |
| T3–T0 | 0.0 (−16.7; 0.0) | 0.0569 | 0.0 (0.0; 8.3) | 0.8218 | |
| T4–T0 | −8.3 (−16.7; 0.0) | 0.0215 | 0.0 (−8.3; 16.7) | 0.9971 | |
| Arm symptoms | T0 (baseline) | 16.7 (0.0; 22.2) | 22.2 (11.1; 33.3) | ||
| T1–T0 | 0.0 (−11.1; 0.0) | 0.2949 | 0.0 (0.0; 22.2) | 0.0195 | |
| T2–T0 | 0.0 (−11.1; 0.0) | 0.4023 | 5.6 (−11.1; 22.2) | 0.0947 | |
| T3–T0 | 0.0 (−11.1; 22.2) | 0.5778 | 11.1 (0.0; 33.3) | 0.0221 | |
| T4–T0 | 0.0 (−22.2; 0.0) | >0.99 | 11.1 (11.1; 33.3) | <0.0001 |
| All Participants N = 36 | Inositol Group N = 18 | p Value | Control Group N = 18 | p Value | ||
|---|---|---|---|---|---|---|
| QLQ-C30 Functional scales | ||||||
| Quality of life | T0 (baseline) | 54.2 (33.3; 58.3) | 66.7 (66.7; 83.3) | |||
| T1–T0 | 0.0 (0.0; 16.7) | 0.2168 | −33.3 (−41.7; −8,33) | 0.0001 | ||
| T2–T0 | 0.0 (−8.3; 16.7) | 0.5757 | −25.0 (−33.3; 0.0) | 0.0007 | ||
| T3–T0 | 0.0 (−16.7; 8.3) | 0.6797 | −33.3 (−50.0; −16.7) | 0.0001 | ||
| T4–T0 | 0.0 (−16.7; 16.7) | 0.9314 | −25.0 (−50.0; −16.7) | <0.0001 | ||
| Physical functioning | T0 (baseline) | 86.7 (73.3; 86.7) | 86.7 (80.0; 100.0) | |||
| T1–T0 | −3.3 (−20.0; 6.7) | 0.2507 | −26.7 (−40.0; −6.7) | <0.0001 | ||
| T2–T0 | 0.0 (−13.3; 20.0) | 0.7024 | −26.7 (−46.7; −6.7) | 0.0002 | ||
| T3–T0 | −10.0 (−26.7; 13.3) | 0.3068 | −43.3 (−46.7; −13.3) | <0.0001 | ||
| T4–T0 | −10.0 (−26.7; 13.3) | 0.106 | −46.7 (−66.7; −26.7) | <0.0001 | ||
| Role functioning | T0 (baseline) | 66.7 (50.0; 83.3) | 75.0 (66.7; 100.0) | |||
| T1–T0 | 0.0 (−16.7; 33.3) | 0.9204 | −16.7 (−33.3; 0.0) | 0.001 | ||
| T2–T0 | 0.0 (−16.7; 33.3) | 0.7852 | −16.7 (−33.3; 16.7) | 0.0347 | ||
| T3–T0 | −16.7 (−33.3; 16.7) | 0.3326 | −33.3 (−50.0; 0.0) | 0.0033 | ||
| T4–T0 | −16.7 (−33.3; 0.0) | 0.2574 | −33.3 (−66.7; −16.7) | 0.0003 | ||
| Cognitive functioning | T0 (baseline) | 83.3 (50.0; 100.0) | 100.0 (83.3; 100.0) | |||
| T1–T0 | 0.0 (−16.7; 16.7) | 0.9258 | −16.7 (−66.7; 0.0) | 0.002 | ||
| T2–T0 | 0.0 (−16.7; 0.0) | 0.4307 | 0.0 (−50.0; 0.0) | 0.0195 | ||
| T3–T0 | −8.3 (−33.3; 16.7) | 0.1913 | −25.0 (−50.0; 0.0) | 0.0029 | ||
| T4–T0 | 0.0 (−33.3; 16.7) | 0.2955 | −16.7 (−50.0; 0.0) | 0.001 | ||
| Social functioning | T0 (baseline) | 75.0 (66.7; 100.0) | 83.3 (66.7; 100.0) | |||
| T1–T0 | −8.3 (−16.7; 0.0) | 0.0508 | −16.7 (−33.3; 0.0) | 0.0005 | ||
| T2–T0 | −8.3 (−33.3; 0.0) | 0.1011 | 0.0 (−16.7; 0.0) | 0.0444 | ||
| T3–T0 | −16.7 (−50.0; 0.0) | 0.1653 | −25.0 (−50.0; 0.0) | 0.0034 | ||
| T4–T0 | −16.7 (−50.0; 0.0) | 0.139 | −33.3 (−50.0; 0.0) | 0.0017 | ||
| QLQ-C30 Symptom scales | ||||||
| Fatigue | T0 (baseline) | 33.3 (11.1; 44.4) | 16.7 (0.0; 33.3) | |||
| T1–T0 | 0.0 (−11.1; 33.3) | 0.2867 | 44.4 (0.0; 55.6) | 0.0002 | ||
| T2–T0 | 0.0 (−11.1; 33.3) | 0.2771 | 38.9 (0.0; 55.6) | 0.0007 | ||
| T3–T0 | 22.2 (−11.1; 33,.3) | 0.1015 | 44.4 (22.2; 66.7) | <0.0001 | ||
| T4–T0 | 16.7 (0.0; 33.3) | 0.0854 | 66.7 (22.2; 77.8) | <0.0001 | ||
| Nausea and vomiting | T0 (baseline) | 0.0 (0.0; 16.7) | 0.0 (0.0; 0.0) | |||
| T1–T0 | 0.0 (0.0; 33.3) | 0.2227 | 16.7 (0.0; 50.0) | 0.0059 | ||
| T2–T0 | 0.0 (0.0; 16.7) | 0.7070 | 8.3 (0.0; 33.3) | 0.0059 | ||
| T3–T0 | 0.0 (0.0; 16.7) | 0.9609 | 8.3 (0.0; 50.0) | 0.0322 | ||
| T4–T0 | 0.0 (−16.7; 0.0) | 0.6230 | 25.0 (0.0; 66.7) | 0.0022 | ||
| Dispnoea | T0 (baseline) | 0.0 (0.0; 33.3) | 0.0 (0.0; 33.3) | |||
| T1–T0 | 0.0 (0.0; 33.3) | 0.0625 | 0.0 (0.0; 33.3) | 0.0078 | ||
| T2–T0 | 0.0 (0.0; 33.3) | 0.0625 | 16.7 (0.0; 33.3) | 0.0137 | ||
| T3–T0 | 0.0 (0.0; 33.3) | 0.0156 | 33.3 (0.0; 33.3) | 0.002 | ||
| T4–T0 | 16.7 (0.0; 33.3) | 0.0215 | 33.3 (0.0; 33.3) | 0.0013 | ||
| Insomnia | T0 (baseline) | 0.0 (0.0; 66.7) | 33.3 (0.0; 33.3) | |||
| T1–T0 | 0.0 (0.0; 0.0) | 0.5703 | 16.7 (0.0; 66.7) | 0.0117 | ||
| T2–T0 | 0.0 (−33.3; 33.3) | 0.5820 | 16.7 (0.0; 66.7) | 0.0059 | ||
| T3–T0 | 0.0 (−33.3; 33.3) | 0.8621 | 0.0 (0.0; 66.7) | 0.0078 | ||
| T4–T0 | 0.0 (−33.3; 33.3) | 0.8267 | 33.3 (0.0; 66.7) | 0.0007 | ||
| Appetite loss | T0 (baseline) | 0.0 (0.0; 0.0) | 0.0 (0.0; 0.0) | |||
| T1–T0 | 0.0 (0.0; 33.3) | 0.6719 | 33.3 (0.0; 33.3) | 0.0471 | ||
| T2–T0 | 0.0 (0.0; 33.3) | 0.8281 | 0.0 (0.0; 33.3) | 0.2734 | ||
| T3–T0 | 0.0 (0.0; 0.0) | 0.8438 | 16.7 (0.0; 66.7) | 0.0156 | ||
| T4–T0 | 0.0 (0.0; 0.0) | 0.8828 | 50.0 (0.0; 66.7) | 0.0037 | ||
| All Participants N = 36 | Inositol Group N = 18 | Control Group N = 18 | p Value | |
|---|---|---|---|---|
| QLQ-BR23 Functional scales | ||||
| Body image | ||||
| T1–T0 | 83.3 (66.7; 83.3) | 66.7 (33.3; 83.3) | 0.0422 | |
| T2–T0 | 66.7 (66.7; 83.3) | 66.7 (33.3; 66.7) | 0.1461 | |
| T3–T0 | 66.7 (66.7; 75.0) | 58.3 (8.3; 100.0) | 0.5191 | |
| T4–T0 | 66.7 (58.3; 66.7) | 62.5 (8.3; 75.0) | 0.4971 | |
| QLQ-BR23 Symptom scales | ||||
| Systemic therapy side effects | ||||
| T1–T0 | 23.8 (19.1; 33.3) | 38.1 (33.3; 57.1) | 0.0028 | |
| T2–T0 | 28.6 (14.3; 38.1) | 40.5 (21.4; 61.9) | 0.0823 | |
| T3–T0 | 33.3 (19.1; 42.9) | 47.6 (28.6; 66.7) | 0.0429 | |
| T4–T0 | 38.1 (19.1; 57.1) | 57.1 (40.5; 71.4) | 0.0193 | |
| Breast symptoms | ||||
| T1–T0 | 8.3 (0.0; 16.7) | 16.7 (8.3; 33.3) | 0.0296 | |
| T2–T0 | 8.3 (0.0; 16.7) | 12.5 (0.0; 33.3) | 0.1788 | |
| T3–T0 | 8.3 (0.0; 16.7) | 16.7 (8.3; 33.3) | 0.1003 | |
| T4–T0 | 4.2 (0.0; 16.7) | 16.7 (8.3; 33.3) | 0.0396 | |
| Arm symptoms | ||||
| T1–T0 | 0.0 (0.0; 22.2) | 27.8 (22.2; 55.6) | 0.0015 | |
| T2–T0 | 0.0 (0.0; 22.2) | 22.2 (11.1; 55.6) | 0.0053 | |
| T3–T0 | 11.1 (0.0; 22.2) | 33.3 (11.1; 66.7) | 0.0079 | |
| T4–T0 | 0.0 (0.0; 22.2) | 50.0 (33.3; 66.7) | <0.0001 |
| All Participants N = 36 | Inositol Group N = 18 | Control Group N = 18 | p Value | |
|---|---|---|---|---|
| QLQ-C30 Functional scales | ||||
| Quality of life | ||||
| T1–T0 | 50.0 (41.7; 66.7) | 37.5 (33.3; 50.0) | 0.052 | |
| T2–T0 | 50.0 (50.0; 58.3) | 50.0 (33.3; 66.7) | 0.6291 | |
| T3–T0 | 54.2 (41.7; 58.3) | 37.5 (16.7; 50.0) | 0.0243 | |
| T4–T0 | 58.3 (33.3; 66.7) | 33.3 (16.7; 58.3) | 0.0431 | |
| Physical functioning | ||||
| T1–T0 | 76.7 (66.7; 86.7) | 56.7 (40.0; 80.0) | 0.1012 | |
| T2–T0 | 73.3 (66.7; 86.7) | 40.0 (40.0; 86.7) | 0.0409 | |
| T3–T0 | 73.3 (66.7; 86.7) | 40.0 (33.3; 66.7) | 0.0017 | |
| T4–T0 | 73.3 (46.7; 80.0) | 33.3 (33.3; 53.3) | 0.0003 | |
| Role functioning | ||||
| T1–T0 | 66.7 (33.3; 83.3) | 50.0 (33.3; 66.7) | 0.386 | |
| T2–T0 | 66.7 (50.0; 100.0) | 50.0 (50.0; 83.3) | 0.5828 | |
| T3–T0 | 50.0 (33.3; 66.7) | 50.0 (33.3; 83.3) | 0.6873 | |
| T4–T0 | 33.3 (33.3; 83.3) | 33.3 (33.3; 50.0) | 0.2841 | |
| Cognitive functioning | ||||
| T1–T0 | 83.3 (50.0; 100.0) | 66.7 (33.3; 83.3) | 0.1538 | |
| T2–T0 | 75.0 (50.0; 83.3) | 83.3 (33.3; 100.0) | 0.6604 | |
| T3–T0 | 66.7 (33.3; 100.0) | 66.7 (33.3; 83.3) | 0.6999 | |
| T4–T0 | 66.7 (50.0; 100.0) | 66.7 (33.3; 83.3) | 0.2949 | |
| Social functioning | ||||
| T1–T0 | 66.7 (50.0; 83.3) | 66.7 (50.0; 66.7) | 0.5794 | |
| T2–T0 | 58.3 (50.0; 83.3) | 66.7 (66.7; 100.0) | 0.1503 | |
| T3–T0 | 50.0 (33.3; 83.3) | 66.7 (33.3; 66.7) | 0.8187 | |
| T4–T0 | 58.3 (33.3; 83.3) | 33.3 (33.3; 66.7) | 0.5849 | |
| QLQ-C30 Symptom scales | ||||
| Fatigue | ||||
| T1–T0 | 33.3 (33.3; 55.6) | 55.6 (44.4; 66.7) | 0.077 | |
| T2–T0 | 44.4 (33.3; 66.7) | 44.4 (33.3; 55.6) | 0.0714 | |
| T3–T0 | 50.0 (33.3; 66.7) | 61.1 (44.4; 88.9) | 0.0883 | |
| T4–T0 | 55.6 (33.3; 66.7) | 72.2 (66.7; 88.9) | 0.0092 | |
| Nausea and vomiting | ||||
| T1–T0 | 16.7 (0.0; 33.3) | 16.7 (0.0; 50.0) | 0.2878 | |
| T2–T0 | 16.7 (0.0; 16.7) | 16.7 (0.0; 50.0) | 0.3178 | |
| T3–T0 | 8.3 (0.0; 16.7) | 16.7 (0.0; 50.0) | 0.1073 | |
| T4–T0 | 0.0 (0.0; 16.7) | 33.3 (0.0; 66.7) | 0.002 | |
| Dispnoea | ||||
| T1–T0 | 33.3 (0.0; 33.3) | 33.3 (0.0; 66.7) | 0.2709 | |
| T2–T0 | 33.3 (0.0; 33.3) | 33.3 (0.0; 66.7) | 0.3438 | |
| T3–T0 | 33.3 (0.0; 66.7) | 33.3 (33.3; 66.7) | 0.2529 | |
| T4–T0 | 33.3 (0.0; 33.3) | 33.3 (33.3; 66.7) | 0.043 | |
| Insomnia | ||||
| T1–T0 | 33.3 (0.0; 33.3) | 50.0 (33.3; 66.7) | 0.0442 | |
| T2–T0 | 33.3 (0.0; 33.3) | 66.7 (33.3; 66.7) | 0.0182 | |
| T3–T0 | 33.3 (0.0; 33.3) | 66.7 (33.3; 66.7) | 0.0424 | |
| T4–T0 | 33.3 (33.3; 33.3) | 66.7 (33.3; 66.7) | 0.0043 | |
| Appetite loss | ||||
| T1–T0 | 0.0 (0.0; 33.3) | 33.3 (0.0; 33.3) | 0.3689 | |
| T2–T0 | 0.0 (0.0; 33.3) | 0.0 (0.0; 33.3) | 0.8373 | |
| T3–T0 | 0.0 (0.0; 33.3) | 33.3 (0.0; 66.7) | 0.1008 | |
| T4–T0 | 0.0 (0.0; 0.0) | 50.0 (0.0; 66.7) | 0.0147 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amabile, M.I.; De Luca, A.; Tripodi, D.; D’Alberti, E.; Melcarne, R.; Imbimbo, G.; Picconi, O.; D’Andrea, V.; Vergine, M.; Sorrenti, S.; et al. Effects of Inositol Hexaphosphate and Myo-Inositol Administration in Breast Cancer Patients during Adjuvant Chemotherapy. J. Pers. Med. 2021, 11, 756. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080756
Amabile MI, De Luca A, Tripodi D, D’Alberti E, Melcarne R, Imbimbo G, Picconi O, D’Andrea V, Vergine M, Sorrenti S, et al. Effects of Inositol Hexaphosphate and Myo-Inositol Administration in Breast Cancer Patients during Adjuvant Chemotherapy. Journal of Personalized Medicine. 2021; 11(8):756. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080756
Chicago/Turabian StyleAmabile, Maria Ida, Alessandro De Luca, Domenico Tripodi, Elena D’Alberti, Rossella Melcarne, Giovanni Imbimbo, Orietta Picconi, Vito D’Andrea, Massimo Vergine, Salvatore Sorrenti, and et al. 2021. "Effects of Inositol Hexaphosphate and Myo-Inositol Administration in Breast Cancer Patients during Adjuvant Chemotherapy" Journal of Personalized Medicine 11, no. 8: 756. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm11080756