
DeepBiomarker: Identifying Important Lab Tests from Electronic Medical Records for the Prediction of Suicide-Related Events among PTSD Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Method
2.1. Data Source
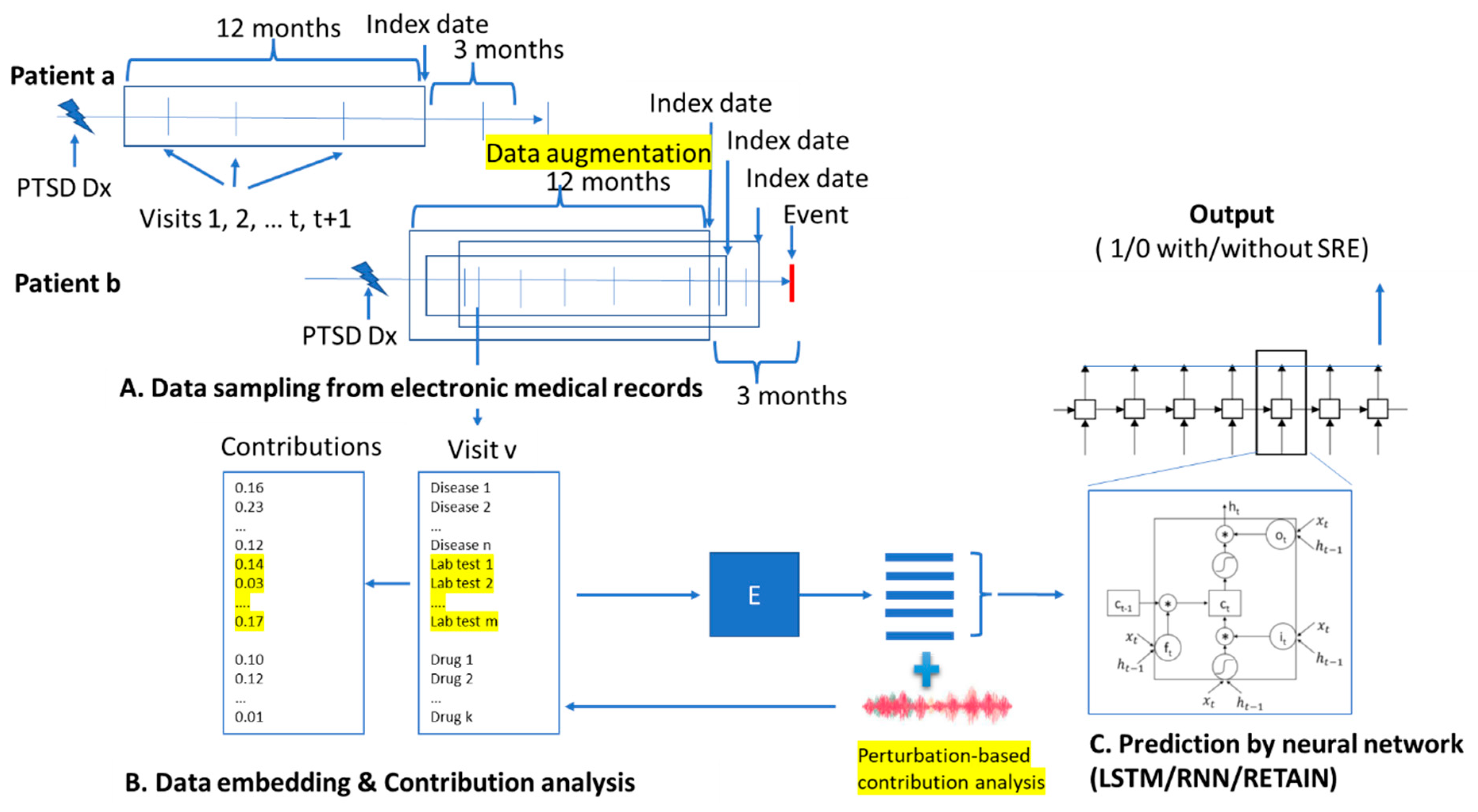
2.2. Data Preparation
2.3. Data Augmentation
2.4. Dataset Splitting
2.5. DeepBiomarker
2.6. Assessment of Importance of the Clinical Factors for Predicting Suicide-Related Events
2.7. Assessment of Model Performance
3. Results
3.1. The Performance of DeepBiomarker on SRE Prediction
3.2. Important Indicators for SRE Prediction
3.3. Effect of Medication use and Comorbidities on PTSD for SRE Prediction
3.4. Overall Lab Test-Based Indicators of Comorbidities and Disease Burdens for SRE Prediction
4. Discussion
4.1. Biomarkers Closely Related to PTSD and SREs
4.2. New Hypothesis on SREs in PTSD
4.3. Biomarkers for Personalized Treatment for PTSD to Reduce the Risk of SRE
5. Limitation of Our Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Diagnosis Codes
- PTSD: 309.81, F43.10, F43.11, F43.12.
- Suicide Related Events/behaviors: V62.84,R45.851,E950.3,E956,E950.4,E950.0,E958.8,T14.91,E950.9,E958.9,T14.91XA,E950.5,E950.2,E953.0,E958.1,E953.8,E950.1,E950.7,E952.0,E958.0,E957.1,E957.0,E958.5,E952.1,E955.4,T14.91XD,E950.6,E953.9,E955.0,E957.9,E958.7,E958.3,E954,T14.91XS,E951.0,E951.8,E952.8,E953.1,E955.1,E958.6,E958.2,E955.9,E955.2,X83.8XXA,T42.4 × 2A,T43.592A,T39.1X2A,X78.8XXA,X78.9XXD,T42.6X2A,X78.9XXA,T43.222A,T50.902A,X83.8XXD,T39.312A,T43.212A,T45.0X2A,X78.1XXA,X78.8XXD,T50.992A,T40.2X2A,T43.292A,T43.012A,T39.012A,T42.8X2A,X78.0XXA,T51.0X2A,T40.5X2A,T40.4X2A,T40.1X2A,T44.7X2A,T38.3X2A,T44.6X2A,T48.1X2A,T46.5X2A,T71.162A,T48.3X2A,T43.022A,T44.3X2A,T50.902D,X79.XXXA,T65.92XA,X78.1XXD,T51.92XA,T42.1X2A,T65.892A,T56.892A,T43.622A,X80.XXXA,T42.4X2D,X78.0XXD,T42.72XA,T43.3X2A,X76.XXXD,T48.4X2A,T51.2X2A,T46.4X2A,T39.1X2D,T40.7X2A,T54.92XA,T40.602A,T45.512A,X76.XXXA,T43.222D,T39.392A,T47.1X2A,T50.902S,X74.9XXD,T39.092A,T38.1X2A,X74.9XXA,T39.312D,T38.892A,T43.612A,X82.8XXA,T42.6X2D,T43.632A,T46.1X2A,T45.0X2D,T50.992D,T54.2X2A,T40.3X2A,T39.012D,T43.4X2A,T58.02XA,T43.592D,X81.0XXA,T43.202A,T43.8X2A,T44.992A,T45.2X2A,T40.1X2D,T41.292A,T50.2X2A,T48.6X2A,T50.7X2A,T49.0X2A,T46.3X2A,T42.0X2A,T36.1X2A,T36.0X2A,X74.9XXS,X72.XXXD,T43.012D,T51.8X2A,T51.0X2D,T54.92XS,T54.3X2A,T65.892D,T65.92XD,T65.222D,T50.3X2A,T48.5X2A,T47.0X2A,T46.6X2A,T65.92XS,T54.1X2A,T52.4X2A,T52.0X2A,T55.1X2A,T59.892A,T42.4X2S,T42.3X2A,T36.3X2A,T37.8X2A,T38.2X2A,T38.3X2D,T40.992A,T40.8X2A,T44.4X2A,T43.692A,T45.2X2D,T44.7X2D,T43.502A,T71.192A,X79.XXXD,X83.2XXA,X83.8XXS,X72.XXXA,X71.9XXA,T48.202A,T40.2X2D,X74.8XXS,T48.3X2D,T39.8X2A,T47.4X2A,T47.6X2A,T50.6X2A,T49.6X2D,T43.3X2D,T50.5X2A,X74.01XA,X73.0XXA,T49.6X2A,X72.XXXS,X78.9XXS,T39.92XA,X80.XXXD,X81.8XXA,T39.4X2A,X77.8XXA,T50.2X2D,T43.622D,T43.292D,T45.4X2A,T46.0X2A,T41.3X2A,T42.5X2A,T42.6X2,T46.7X2A,T46.8X2A,T46.5X2D,T43.1X2A,T43.92XA,T40.5X2D,X71.0XXS,X71.3XXA,X71.8XXA,T43.212D,T46.2X2A,T40.8X2D,T40.602D,T43.022D,T44.1X2A,T46.4X2D,T65.222S,T62.0X2A,T71.162D,T51.1X2A,T51.2X2D,T51.2X2S,T52.8X2A,T51.92XD,T50.8X2A,T56.892D,T58.92XA,T54.3X2S,T54.3X2D,T54.0X2A,T55.0X2A,T36.0X2D,T36.4X2A,T38.5X2A,T36.8X2A,T37.5X2A.
References
- Patton, G.C.; Coffey, S.M.C.; Sawyer, S.M.; Viner, R.M.; Haller, D.; Bose, K.; Vos, T.; Ferguson, J.; Mathers, C.D. Global patterns of mortality in young people: A systematic analysis of population health data. Lancet 2009, 374, 881–892. [Google Scholar] [CrossRef] [PubMed]
- W.H.O. Figures and Facts About Suicide; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Woolf, S.H.; Schoomaker, H. Life Expectancy and Mortality Rates in the United States, 1959–2017. JAMA J. Am. Med. Assoc. 2019, 322, 1996–2016. [Google Scholar] [CrossRef]
- Fan, P.X.; Guo, X.; Qi, X.; Matharu, M.; Patel, R.; Sakolsky, D.; Kirisci, L.; Silverstein, J.C.; Wang, L. Prediction of Suicide-Related Events by Analyzing Electronic Medical Records from PTSD Patients with Bipolar Disorder. Brain Sci. 2020, 10, 784. [Google Scholar] [CrossRef]
- Fox, V.; Dalman, C.; Dal, H.; Hollander, A.-C.; Kirkbride, J.B.; Pitman, A. Suicide risk in people with post-traumatic stress disorder: A cohort study of 3.1 million people in Sweden. J. Affect. Disord. 2021, 279, 609–616. [Google Scholar] [CrossRef]
- Williams, M.B.; Poijula, S. The Ptsd Workbook: Simple, Effective Techniques for Overcoming Traumatic Stress Symptoms; 5674 Shattuck Ave; New Harbinger Publications: Oakland, CA, USA, 2016. [Google Scholar]
- Mutz, J.; Edgcumbe, D.R.; Brunoni, A.R.; Fu, C.H. Efficacy and acceptability of non-invasive brain stimulation for the treatment of adult unipolar and bipolar depression: A systematic review and meta-analysis of randomised sham-controlled trials. Neurosci. Biobehav. Rev. 2018, 92, 291–303. [Google Scholar] [CrossRef] [Green Version]
- Borgomaneri, S.; Battaglia, S.; Sciamanna, G.; Tortora, F.; Laricchiuta, D. Memories are not written in stone: Re-writing fear memories by means of non-invasive brain stimulation and optogenetic manipulations. Neurosci. Biobehav. Rev. 2021, 127, 334–352. [Google Scholar] [CrossRef] [PubMed]
- Kan, R.L.D.; Zhang, B.B.B.; Zhang, J.J.Q.; Kranz, G.S. Non-invasive brain stimulation for posttraumatic stress disorder: A systematic review and meta-analysis. Transl. Psychiatry 2020, 10, 168. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, B. Neurobiological advances of learned fear in humans. Adv. Clin. Exp. Med. 2022, 31. [Google Scholar] [CrossRef]
- Tanaka, M.; Tóth, F.; Polyák, H.; Szabó, Á.; Mándi, Y.; Vécsei, L. Immune Influencers in Action: Metabolites and Enzymes of the Tryptophan-Kynurenine Metabolic Pathway. Biomedicines 2021, 9, 734. [Google Scholar] [CrossRef]
- Tanaka, M.; Toldi, J.; Vécsei, L. Exploring the Etiological Links behind Neurodegenerative Diseases: Inflammatory Cytokines and Bioactive Kynurenines. Int. J. Mol. Sci. 2020, 21, 2431. [Google Scholar] [CrossRef] [Green Version]
- Jiang, S.; Postovit, L.; Cattaneo, A.; Binder, E.B.; Aitchison, K.J. Epigenetic Modifications in Stress Response Genes Associated with Childhood Trauma. Front. Psychiatry 2019, 10, 808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowirrat, A.; Chen, T.J.; Blum, K.; Madigan, M.; Bailey, J.A.; Chen, A.L.C.; Downs, B.W.; Braverman, E.R.; Radi, S.; Waite, R.L.; et al. Neuro-psychopharmacogenetics and Neurological Antecedents of Posttraumatic Stress Disorder: Unlocking the Mysteries of Resilience and Vulnerability. Curr. Neuropharmacol. 2010, 8, 335–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, T.; Saab, B.; Mansuy, I.M. Neural Mechanisms of Stress Resilience and Vulnerability. Neuron 2012, 75, 747–761. [Google Scholar] [CrossRef] [Green Version]
- El-Sayed, A.M.; Haloossim, M.R.; Galea, S.; Koenen, K.C. Epigenetic modifications associated with suicide and common mood and anxiety disorders: A systematic review of the literature. Biol. Mood Anxiety Disord. 2012, 2, 1–14. [Google Scholar] [CrossRef]
- Shalev, A.Y.; Peri, T.; Brandes, D.; Freedman, S.; Orr, S.P.; Pitman, R.K. Auditory Startle Response in Trauma Survivors with Posttraumatic Stress Disorder: A Prospective Study. Am. J. Psychiatry 2000, 157, 255–261. [Google Scholar] [CrossRef]
- Segman, R.H.; Goltser-Dubner, S.N.T.; Friedman, N.; Kaminski, N.; Shalev, A.Y. Peripheral blood mononuclear cell gene expression profiles identify emergent post-traumatic stress disorder among trauma survivors. Mol. Psychiatry 2005, 10, 500–513. [Google Scholar]
- Marmar, C.R.; Weiss, D.S.; E Schlenger, W.; A Fairbank, J.; Jordan, B.K.; A Kulka, R.; Hough, R.L. Peritraumatic dissociation and posttraumatic stress in male Vietnam theater veterans. Am. J. Psychiatry 1994, 151, 902–907. [Google Scholar] [CrossRef]
- Shalev, A.Y.; Peri, T.; Canetti, L.; Schreiber, S. Predictors of PTSD in injured trauma survivors: A prospective study. Am. J. Psychiatry 1996, 153, 219–225. [Google Scholar] [CrossRef] [Green Version]
- Dwivedi, Y. The Neurobiological Basis of Suicide; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2012. [Google Scholar]
- Wang, H.; Raj, B. On the origin of deep learning. arXiv 2017, arXiv:1702.07800. [Google Scholar]
- Pham, T.; Tran, T.; Phung, D.; Venkatesh, S. DeepCare: A Deep Dynamic Memory Model for Predictive Medicine. In Proceedings of the Human-Computer Interaction. Towards Mobile and Intelligent Interaction Environments; Springer: Berlin/Heidelberg, Germany, 2016; pp. 30–41. [Google Scholar]
- Dernoncourt, F.; Lee, J.Y.; Uzuner, O.; Szolovits, P. De-identification of patient notes with recurrent neural networks. J. Am. Med. Inform. Assoc. 2017, 24, 596–606. [Google Scholar] [CrossRef]
- Che, Z.; Purushotham, S.; Khemani, R.; Liu, Y. Distilling knowledge from deep networks with applications to healthcare domain. arXiv 2015, arXiv:1512.03542. [Google Scholar]
- Cheng, Y.; Wang, F.; Zhang, P.; Hu, J. Risk Prediction with Electronic Health Records: A Deep Learning Approach. In Proceedings of the 2016 SIAM International Conference on Data Mining; Society for Industrial & Applied Mathematics (SIAM), Miami, FL, USA, 5–7 May 2016; pp. 432–440. [Google Scholar]
- Choi, Y.; Chiu, C.Y.-I.; Sontag, D. Learning Low-Dimensional Representations of Medical Concepts. AMIA Jt. Summits Transl. Sci. 2016, 2016, 41–50. [Google Scholar]
- Shickel, B.; Tighe, P.J.; Bihorac, A.; Rashidi, P. Deep EHR: A Survey of Recent Advances in Deep Learning Techniques for Electronic Health Record (EHR) Analysis. IEEE J. Biomed. Health Inform. 2017, 22, 1589–1604. [Google Scholar] [CrossRef] [PubMed]
- Karstoft, K.-I.; For Members of the Jerusalem Trauma Outreach and Prevention Study (J-TOPS) Group; Galatzer-Levy, I.R.; Statnikov, A.; Li, Z.; Shalev, A.Y. Bridging a translational gap: Using machine learning to improve the prediction of PTSD. BMC Psychiatry 2015, 15, 30. [Google Scholar] [CrossRef] [Green Version]
- Rasmy, L.; Zhu, J.; Li, Z.; Hao, X.; Tran, H.T.; Zhou, Y.; Tiryaki, F.; Xiang, Y.; Xu, H.; Zhi, D. Simple recurrent neural networks is all we need for clinical events predictions using ehr data. arXiv 2021, arXiv:2110.00998. [Google Scholar]
- Guan, C.; Wang, X.; Zhang, Q.; Chen, R.; He, D.; Xie, X. Towards a deep and unified understanding of deep neural models in nlp. In Proceedings of the International Conference on Machine Learning, Long Beach, CA, USA, 9–15 June 2019; pp. 2454–2463. [Google Scholar]
- Visweswaran, S.; McLay, B.; Cappella, N.; Morris, M.; Milnes, J.T.; E Reis, S.; Silverstein, J.C.; Becich, M.J. An atomic approach to the design and implementation of a research data warehouse. J. Am. Med Inform. Assoc. 2021, 29, 601–608. [Google Scholar] [CrossRef]
- Gilbert, M.; La, A.D.; Delapaz, N.R.; Hor, W.K.; Fan, P.; Qi, X.; Guo, X.; Ying, J.; Wang, L. An Emulation of Randomized Trials of Administrating Benzodiazepines in PTSD Patients for Outcomes of Suicide-Related Events. J. Clin. Med. 2020, 9, 3492. [Google Scholar] [CrossRef]
- Wang, H.; Huang, Z.; Wu, X.; Xing, E.P. Squared ℓ2 norm as consistency loss for leveraging augmented data to learn robust and invariant representations. arXiv 2020, arXiv:2011.13052. [Google Scholar]
- Delapaz, N.; Hor, W.; Gilbert, M.; La, A.; Liang, F.; Fan, P.; Qi, X.; Guo, X.; Ying, J.; Sakolsky, D.; et al. An Emulation of Randomized Trials of Administrating Antipsychotics in PTSD Patients for Outcomes of Suicide-Related Events. J. Pers. Med. 2021, 11, 178. [Google Scholar] [CrossRef]
- Shorten, C.; Khoshgoftaar, T.M. A survey on Image Data Augmentation for Deep Learning. J. Big Data 2019, 6, 60. [Google Scholar] [CrossRef]
- Reitermanova, Z. Data Splitting. In Proceedings of the Presented at WDS, Prague, Czech Republic, 1–4 June 2010; pp. 31–36. [Google Scholar]
- Chang, S.; Zhang, Y.; Han, W.; Yu, M.; Guo, X.; Tan, W.; Cui, X.; Witbrock, M.; Hasegawa-Johnson, M.A.; Huang, T.S. Dilated recurrent neural networks. Adv. Neural Inf. Process. Syst. 2017, 30, 76–86. [Google Scholar]
- Bradbury, J.; Merity, S.; Xiong, C.; Socher, R. Quasi-recurrent neural networks. arXiv 2016, arXiv:1611.01576. [Google Scholar]
- Pham, T.; Tran, T.; Phung, D.; Venkatesh, S. Predicting healthcare trajectories from medical records: A deep learning approach. J. Biomed. Inform. 2017, 69, 218–229. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.; Li, Y.; Ramakrishnan, R.; Hassaine, A.; Canoy, D.; Zhu, Y.; Salimi-Khorshidi, G.; Rahimi, K. BEHRT-HF: An interpretable transformer-based, deep learning model for prediction of incident heart failure. Eur. Hear. J. 2020, 41, 3553. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. How to obtain the P value from a confidence interval. BMJ 2011, 343, d2304. [Google Scholar] [CrossRef] [Green Version]
- Bonferroni, C. Teoria Statistica Delle Classi e Calcolo Delle Probabilita; Pubblicazioni del R Istituto Superiore di Scienze Economiche e Commericiali di Firenze: Firenze, Italy, 1936. [Google Scholar]
- Fraunfelder, F.W. Epinastine hydrochloride for atopic disease. Drugs Today 2004, 40, 677–683. [Google Scholar] [CrossRef]
- Tzeng, N.-S.; Chang, H.-A.; Chung, C.-H.; Kao, Y.-C.; Chang, C.-C.; Yeh, H.-W.; Chiang, W.-S.; Chou, Y.-C.; Chang, S.-Y.; Chien, W.-C. Increased Risk of Psychiatric Disorders in Allergic Diseases: A Nationwide, Population-Based, Cohort Study. Front. Psychiatry 2018, 9, 133. [Google Scholar] [CrossRef] [Green Version]
- Amritwar, A.U.; Lowry, C.A.; A Brenner, L.; Hoisington, A.J.; Stiller, J.W.; Hamilton, R.; Postolache, T.T. Mental Health in Allergic Rhinitis: Depression and Suicidal Behavior. Curr. Treat. Options Allergy 2017, 4, 71–97. [Google Scholar] [CrossRef] [Green Version]
- Jung, S.J.; Kang, J.H.; Roberts, A.L.; Nishimi, K.; Chen, Q.; Sumner, J.A.; Kubzansky, L.; Koenen, K.C. Posttraumatic stress disorder and incidence of thyroid dysfunction in women. Psychol. Med. 2019, 49, 2551–2560. [Google Scholar] [CrossRef]
- Sunyecz, J. The use of calcium and vitamin D in the management of osteoporosis. Ther. Clin. Risk Manag. 2008, 4, 827–836. [Google Scholar] [CrossRef] [Green Version]
- Weber, T.; Eberle, J.; Messelhäuser, U.; Schiffmann, L.; Nies, C.; Schabram, J.; Zielke, A.; Holzer, K.; Rottler, E.; Henne-Bruns, D. Parathyroidectomy, elevated depression scores, and suicidal ideation in patients with primary hyperparathyroidism: Results of a prospective multicenter study. JAMA Surg. 2013, 148, 109–115. [Google Scholar] [PubMed]
- Ehelepola, N.D.B.; Sathkumara, S.M.B.Y.; Bandara, H.M.P.A.G.S.; Kalupahana, K.L.R. Atorvastatin-Diltiazem Combination Induced Rhabdomyolysis Leading to Diagnosis of Hypothyroidism. Case Rep. Med. 2017, 2017, 8383251. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, G.; Bingefors, K.; Ranstam, J.; Råstam, L.; Melander, A. Use of calcium channel blockers and risk of suicide: Ecological findings confirmed in population based cohort study. BMJ 1998, 316, 741–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biriell, C.; McEwen, J.; Sanz, E. Depression associated with diltiazem. BMJ 1989, 299, 796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arai, T.; Kogi, K.; Honda, Y.; Suzuki, T.; Kawai, K.; Okamoto, M.; Fujioka, T.; Murata, N. Lorazepam as a Cause of Drug-Induced Liver Injury. Case Rep. Gastroenterol. 2018, 12, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Gray, M.A.; Chao, C.-Y.; Staudacher, H.; Kolosky, N.A.; Talley, N.J.; Holtmann, G. Anti-TNFα therapy in IBD alters brain activity reflecting visceral sensory function and cognitive-affective biases. PLoS ONE 2018, 13, e0193542. [Google Scholar] [CrossRef]
- Jain, A.; Marrie, R.A.; Shafer, L.A.; A Graff, L.; Patten, S.B.; El-Gabalawy, R.; Sareen, J.; Bolton, J.M.; Fisk, J.D.; Bernstein, C.N. Incidence of Adverse Psychiatric Events During Treatment of Inflammatory Bowel Disease with Biologic Therapies: A Systematic Review. Crohn’s Colitis 360 2020, 2, otz053. [Google Scholar] [CrossRef] [Green Version]
- Cham, S.; Koslik, H.J.; Golomb, B.A. Mood, Personality, and Behavior Changes During Treatment with Statins: A Case Series. Drug Saf.-Case Rep. 2016, 3, 1. [Google Scholar] [CrossRef] [Green Version]
- Rana, A.; Musto, A.E. The role of inflammation in the development of epilepsy. J. Neuroinflamm. 2018, 15, 144. [Google Scholar] [CrossRef]
- Dai, C.-Y.; Ho, C.-K.; Huang, J.-F.; Hsieh, M.-Y.; Hou, N.-J.; Lin, Z.-Y.; Chen, S.-C.; Wang, L.-Y.; Chang, W.-Y.; Yu, M.-L.; et al. Hepatitis C virus viremia and low platelet count: A study in a hepatitis B & C endemic area in Taiwan. J. Hepatol. 2010, 52, 160–166. [Google Scholar] [CrossRef]
- Hill, A.R.; Spencer-Segal, J.L. Glucocorticoids and the Brain after Critical Illness. Endocrinology 2021, 162, 242. [Google Scholar] [CrossRef]
- Kenna, H.A.; Poon, A.W.; Angeles, C.P.D.L.; Koran, L.M. Psychiatric complications of treatment with corticosteroids: Review with case report. Psychiatry Clin. Neurosci. 2011, 65, 549–560. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, K.; Harigai, M.; Omori, M.; Sato, E.; Hara, M. Blood-brain barrier damage as a risk factor for corticosteroid-induced psychiatric disorders in systemic lupus erythematosus. Psychoneuroendocrinology 2008, 33, 395–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagao, T.; Hirokawa, M. Diagnosis and treatment of macrocytic anemias in adults. J. Gen. Fam. Med. 2017, 18, 200–204. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, E.H. Folic acid, ageing, depression, and dementia. BMJ 2002, 324, 1512–1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, B.; Conradty, M.; Grohmann, R.; Rüther, E.; Witzgall, H.; Londong, V. A case of immune complex hemolytic anemia, thrombocytopenia, and acute renal failure associated with doxepin use. J. Clin. Psychiatry 1989, 50, 99–100. [Google Scholar]
- O’Brien, C.L.; Allison, G.E.; Grimpen, F.; Pavli, P. Impact of Colonoscopy Bowel Preparation on Intestinal Microbiota. PLoS ONE 2013, 8, e62815. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.T.T.; Tsujiguchi, H.; Kambayashi, Y.; Hara, A.; Miyagi, S.; Yamada, Y.; Nakamura, H.; Shimizu, Y.; Hori, D.; Suzuki, F.; et al. Relationship between Vitamin Intake and Depressive Symptoms in Elderly Japanese Individuals: Differences with Gender and Body Mass Index. Nutrients 2017, 9, 1319. [Google Scholar] [CrossRef] [Green Version]
- Rao, T.S.S.; Asha, M.R.; Ramesh, B.N.; Rao, K.S.J. Understanding nutrition, depression and mental illnesses. Indian J. Psychiatry 2008, 50, 77–82. [Google Scholar] [CrossRef]
- Tardy, A.-L.; Pouteau, E.; Marquez, D.; Yilmaz, C.; Scholey, A. Vitamins and Minerals for Energy, Fatigue and Cognition: A Narrative Review of the Biochemical and Clinical Evidence. Nutrients 2020, 12, 228. [Google Scholar] [CrossRef] [Green Version]
- Evron, E.; Juhasz, M.; Babadjouni, A.; Mesinkovska, N.A. Natural Hair Supplement: Friend or Foe? Saw Palmetto, a Systematic Review in Alopecia. Ski. Appendage Disord. 2020, 6, 329–337. [Google Scholar] [CrossRef]
- Siwakoti, A.; Potukuchi, P.K.; Thomas, F.; Gaipov, A.; Talwar, M.; Balaraman, V.; Cseprekal, O.; Yazawa, M.; Streja, E.; Eason, J.D.; et al. History of posttraumatic stress disorder and outcomes after kidney transplantation. Am. J. Transplant. 2019, 19, 2294–2305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bersani, G.; Marino, P.; Valeriani, G.; Cuoco, V.; Zitelli, C.; Melcore, C.; Bersani, F.S. Manic-Like Psychosis Associated with Elevated Trough Tacrolimus Blood Concentrations 17 Years after Kidney Transplant. Case Rep. Psychiatry 2013, 2013, 926395. [Google Scholar] [CrossRef]
- Robertson, H.T.; Allison, D.B. Drugs Associated with More Suicidal Ideations Are also Associated with More Suicide Attempts. PLoS ONE 2009, 4, e7312. [Google Scholar] [CrossRef]
- Muzik, M.; McGinnis, E.W.; Bocknek, E.; Morelen, D.; Rosenblum, K.L.; Liberzon, I.; Seng, J.; Abelson, J.L. Ptsd symptoms across pregnancy and early postpartum among women with lifetime ptsd diagnosis. Depress. Anxiety 2016, 33, 584–591. [Google Scholar] [CrossRef] [Green Version]
- Rybakowski, J.K.; Ainiyet, B. Suicidal Behavior in Schizophrenia may be Related to Low Lipid Levels. Med Sci. Monit. 2014, 20, 1486–1490. [Google Scholar] [CrossRef] [Green Version]
- Gokalp, G. The association between low vitamin d levels and suicide attempts in adolescents. Ann. Clin. Psychiatry: Off. J. Am. Acad. Clin. Psychiatr. 2020, 32, e1–e8. [Google Scholar]
- Singh, V.; Khatana, S.; Gupta, P. Blood gas analysis for bedside diagnosis. Natl. J. Maxillofac. Surg. 2013, 4, 136–141. [Google Scholar] [CrossRef] [Green Version]
- Pongmanee, W.; Vattanavanit, V. Can base excess and anion gap predict lactate level in diagnosis of septic shock? Open Access Emerg. Med. 2017, 10, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Zante, B.; Reichenspurner, H.; Kubik, M.; Kluge, S.; Schefold, J.C.; Pfortmueller, C. Base excess is superior to lactate-levels in prediction of ICU mortality after cardiac surgery. PLoS ONE 2018, 13, e0205309. [Google Scholar] [CrossRef] [Green Version]
- Xiong, W.; Xu, M.; Zhao, Y.; Wu, X.; Pudasaini, B.; Liu, J.-M. Can we predict the prognosis of COPD with a routine blood test? Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 615–625. [Google Scholar] [CrossRef] [Green Version]
- Lindqvist, D.; Mellon, S.H.; Dhabhar, F.S.; Yehuda, R.; Grenon, S.M.; Flory, J.D.; Bierer, L.M.; Abu-Amara, D.; Coy, M.; Makotkine, I.; et al. Increased circulating blood cell counts in combat-related ptsd: Associations with inflammation and ptsd severity. Psychiatry Res. 2017, 258, 330–336. [Google Scholar] [PubMed]
- Huang, Y.; Wang, J.; Shen, J.; Ma, J.; Miao, X.; Ding, K.; Jiang, B.; Hu, B.; Fu, F.; Huang, L.; et al. Relationship of Red Cell Index with the Severity of Chronic Obstructive Pulmonary Disease. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 825–834. [Google Scholar] [CrossRef]
- Pedersen, K.M.; Çolak, Y.; Ellervik, C.; Hasselbalch, H.C.; Bojesen, S.E.; Nordestgaard, B.G. Smoking and Increased White and Red Blood Cells. Arter. Thromb. Vasc. Biol. 2019, 39, 965–977. [Google Scholar] [CrossRef]
- Orum, M.H.; Kara, M.Z.; Egilmez, O.B. Mean platelet volume and neutrophil to lymphocyte ratio as parameters to indicate the severity of suicide attempt. J. Immunoass. Immunochem. 2018, 39, 647–659. [Google Scholar] [CrossRef]
- Evstatiev, R.; Bukaty, A.; Jimenez, K.; Kulnigg-Dabsch, S.; Surman, L.; Schmid, W.; Eferl, R.; Lippert, K.; Scheiber-Mojdehkar, B.; Kvasnicka, H.M.; et al. Iron deficiency alters megakaryopoiesis and platelet phenotype independent of thrombopoietin. Am. J. Hematol. 2014, 89, 524–529. [Google Scholar] [CrossRef] [Green Version]
- Fletcher-Sandersjöö, A.; Thelin, E.P.; Maegele, M.; Svensson, M.; Bellander, B.-M. Time Course of Hemostatic Disruptions after Traumatic Brain Injury: A Systematic Review of the Literature. Neurocrit. Care 2021, 34, 635–656. [Google Scholar] [CrossRef]
- Öztürk, A.; Şahan, E.; Mirçik, A.B.; Deveci, E.; Yilmaz, O.; Kirpinar, I. Mean platelet volume and neutrophil to lymphocyte ratio decrease in patients with depression with antidepressant treatment. Arch. Clin. Psychiatry 2019, 46, 9–13. [Google Scholar] [CrossRef] [Green Version]
- Fan, Z.; Lu, X.; Long, H.; Li, T.; Zhang, Y. The association of hemocyte profile and obstructive sleep apnea. J. Clin. Lab. Anal. 2019, 33, e22680. [Google Scholar] [CrossRef] [Green Version]
- Center, I.M. Link between Red Cell Distribution Width Levels, Depression. ScienceDaily. Available online: www.sciencedaily.com/releases/2013/11/131118111750.htm (accessed on 10 November 2021).
- Kang, C.; Park, I.S.; Kim, D.H.; Kim, S.C.; Jeong, J.H.; Lee, S.H.; Lee, S.B.; Jung, S.M.; Kang, T.-S.; Lee, K.-W. Red cell distribution width as a predictor of mortality in organophosphate insecticide poisoning. Am. J. Emerg. Med. 2014, 32, 743–746. [Google Scholar] [CrossRef]
- Ransing, R.S.; Patil, S.; Pevekar, K.; Mishra, K.; Patil, B. Unrecognized Prevalence of Macrocytosis among the Patients with First Episode of Psychosis and Depression. Indian J. Psychol. Med. 2018, 40, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Aguglia, A.; Amerio, A.; Asaro, P.; Caprino, M.; Conigliaro, C.; Giacomini, G.; Parisi, V.M.; Trabucco, A.; Amore, M.; Serafini, G. High-lethality of suicide attempts associated with platelet to lymphocyte ratio and mean platelet volume in psychiatric inpatient setting. World J. Biol. Psychiatry 2021, 22, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Kalinova, D.; Kukushev, G.; Kolarov, Z.; Rashkov, R. Severe mononeuritis multiplex in a patient with eosinophilic granulomatosis with polyangiitis. Reumatology 2019, 57, 288–291. [Google Scholar] [CrossRef] [Green Version]
- Sharma, S.; Hashmi, M.H.; Aggarwal, S. Hyperchloremic Acidosis; Stat pearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Mistry, K. Dialysis disequilibrium syndrome prevention and management. Int. J. Nephrol. Renov. Dis. 2019, 12, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Kolmodin, L.; Sekhon, M.S.; Henderson, W.R.; Turgeon, A.F.; Griesdale, D.E. Hypernatremia in patients with severe traumatic brain injury: A systematic review. Ann. Intensiv. Care 2013, 3, 35. [Google Scholar] [CrossRef] [Green Version]
- Romero, S.; Pintor, L.; Serra, M.; Plana, T.; Navarro, V.; Gastó, C.; Goldstein, B. Syndrome of inappropriate secretion of antidiuretic hormone due to citalopram and venlafaxine. Gen. Hosp. Psychiatry 2007, 29, 81–84. [Google Scholar] [CrossRef]
- Brunner, J. Vasopressin in CSF and plasma in depressed suicide attempters: Preliminary results. Eur. Neuropsychopharmacol. 2002, 12, 489–494. [Google Scholar] [CrossRef]
- Yang, P.-W.; Lin, K.-H.; Lo, S.-H.; Wang, L.-M.; Lin, H.-D. Successful Treatment of Severe Lactic Acidosis Caused by a Suicide Attempt with a Metformin Overdose. Kaohsiung J. Med. Sci. 2009, 25, 93–97. [Google Scholar] [CrossRef] [Green Version]
- Forman, J.P.; Rifas-Shiman, S.L.; Taylor, E.N.; Lane, K.; Gillman, M.W. Association between the serum anion gap and blood pressure among patients at Harvard Vanguard Medical Associates. J. Hum. Hypertens. 2007, 22, 122–125. [Google Scholar] [CrossRef]
- Nowotny, B.; Cavka, M.; Herder, C.; Löffler, H.; Poschen, U.; Joksimovic, L.; Kempf, K.; Krug, A.W.; Koenig, W.; Martin, S.; et al. Effects of Acute Psychological Stress on Glucose Metabolism and Subclinical Inflammation in Patients with Post-traumatic Stress Disorder. Horm. Metab. Res. 2010, 42, 746–753. [Google Scholar] [CrossRef]
- Batty, G.D.; Kivimaki, M.; Park, I.S.; Jee, S.H. Diabetes and raised blood glucose as risk factors for future suicide: Cohort study of 1 234 927 Korean men and women: Table 1. J. Epidemiol. Community Heal. 2012, 66, 650–652. [Google Scholar] [CrossRef]
- Lehto, S.M.; Niskanen, L.; Tolmunen, T.; Hintikka, J.; Viinamäki, H.; Heiskanen, T.; Honkalampi, K.; Kokkonen, M.; Koivumaa-Honkanen, H. Low serum HDL-cholesterol levels are associated with long symptom duration in patients with major depressive disorder. Psychiatry Clin. Neurosci. 2010, 64, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Bachawati, M. Anticoagulation and psychotropic medications. Curr Psychiatry Rep. 2010, 12, 265–271. [Google Scholar]
- Norton, J.Q.E. Mirtazapine-induced warfarin toxicity. Prim Psychiatry 2002, 9, 30–31. [Google Scholar]
- Sansone, R.A.; Sansone, L. Warfarin and antidepressants: Happiness without hemorrhaging. Psychiatry 2009, 6, 24–29. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC2728939/pdf/PE_6_07_24.pdf (accessed on 9 November 2021). [PubMed]
- Madden, T.; Grentzer, J.M.; Secura, G.M.; Allsworth, J.; Peipert, J.F. Risk of Bacterial Vaginosis in Users of the Intrauterine Device. Sex. Transm. Dis. 2012, 39, 217–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nansel, T.R.; Riggs, M.A.; Yu, K.-F.; Andrews, W.W.; Schwebke, J.R.; Klebanoff, M.A. The association of psychosocial stress and bacterial vaginosis in a longitudinal cohort. Am. J. Obstet. Gynecol. 2006, 194, 381–386. [Google Scholar] [CrossRef] [Green Version]
- Araklitis, G.; Robinson, D.; Cardozo, L. Cognitive Effects of Anticholinergic Load in Women with Overactive Bladder. Clin. Interv. Aging 2020, 15, 1493–1503. [Google Scholar]
- Gosling, P.; Sutcliffe, A.J. Proteinuria following Trauma. Ann. Clin. Biochem. Int. J. Lab. Med. 1986, 23, 681–685. [Google Scholar] [CrossRef]
- Canakis, A.; Haroon, M.; Weber, H.C. Irritable bowel syndrome and gut microbiota. Curr. Opin. Endocrinol. Diabetes Obes. 2020, 27, 28–35. [Google Scholar] [CrossRef]
- Bufler, P.; Groß, M.; Uhlig, H.H. Recurrent Abdominal Pain in Childhood. Dtsch. Ärzteblatt Int. 2011, 108, 295–304. [Google Scholar] [CrossRef]
- Michopoulos, V.; Vester, A.; Neigh, G. Posttraumatic stress disorder: A metabolic disorder in disguise? Exp. Neurol. 2016, 284, 220–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lihua, M.; Tao, Z.; Hongbin, M.; Hui, W.; Caihong, J.; Xiaolian, J. Metabolic syndrome risk in relation to posttraumatic stress disorder among trauma-exposed civilians in Gansu Province, China. Medicine 2020, 99, e18614. [Google Scholar] [CrossRef] [PubMed]
- Heppner, P.S.; Crawford, E.F.; A Haji, U.; Afari, N.; Hauger, R.L.; A Dashevsky, B.; Horn, P.S.; E Nunnink, S.; Baker, D.G. The association of posttraumatic stress disorder and metabolic syndrome: A study of increased health risk in veterans. BMC Med. 2009, 7, 1. [Google Scholar] [CrossRef] [Green Version]
- Gupta, M.A.; Jarosz, P. Obstructive Sleep Apnea Severity is Directly Related to Suicidal Ideation in Posttraumatic Stress Disorder. J. Clin. Sleep Med. 2018, 14, 427–435. [Google Scholar] [CrossRef]
- Young, S. Elevated incidence of suicide in people living at altitude, smokers and patients with chronic obstructive pulmonary disease and asthma: Possible role of hypoxia causing decreased serotonin synthesis. J. Psychiatry Neurosci. 2013, 38, 423–426. [Google Scholar] [CrossRef] [Green Version]
- Liao, Y.; Liu, P.; Guo, F.; Zhang, Z.-Y.; Zhang, Z. Oxidative Burst of Circulating Neutrophils Following Traumatic Brain Injury in Human. PLoS ONE 2013, 8, e68963. [Google Scholar] [CrossRef]
- Von Kanel, R.; Hepp, U.; Buddeberg, C.; Keel, M.; Mica, L.; Aschbacher, K.; Schnyder, U. Altered Blood Coagulation in Patients with Posttraumatic Stress Disorder. Psychosom. Med. 2006, 68, 598–604. [Google Scholar] [CrossRef]
- Sinagra, E.; Utzeri, E.; Morreale, G.C.; Fabbri, C.; Pace, F.; Anderloni, A. Microbiota-gut-brain axis and its affect inflammatory bowel disease: Pathophysiological concepts and insights for clinicians. World J. Clin. Cases 2020, 8, 1013–1025. [Google Scholar] [CrossRef]
- Liu, C.-H.; Zhang, G.-Z.; Li, B.; Li, M.; Woelfer, M.; Walter, M.; Wang, L. Role of inflammation in depression relapse. J. Neuroinflammation 2019, 16, 90. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Whole Dataset (Diagnosis + Medication + Lab Test) | ||||
|---|---|---|---|---|
| Valid AUC | Test AUC | Valid AUC std | Test AUC std | |
| RNN | 0.921 | 0.931 | 0.002 | 0.003 |
| DRNN | 0.929 | 0.930 | 0.002 | 0.001 |
| QRNN | 0.933 | 0.929 | 0.001 | 0.001 |
| TLSTM | 0.933 | 0.929 | 0.001 | 0.001 |
| RETAIN | 0.935 | 0.932 | 0.001 | 0.002 |
| Dataset without lab tests (diagnosis + medication) | ||||
| Valid AUC | Test AUC | Valid AUC std | Test AUC std | |
| RNN | 0.915 | 0.912 | 0.002 | 0.002 |
| DRNN | 0.917 | 0.913 | 0.001 | 0.002 |
| QRNN | 0.918 | 0.91 | 0.001 | 0.001 |
| TLSTM | 0.920 | 0.910 | 0.001 | 0.001 |
| RETAIN | 0.920 | 0.910 | 0.001 | 0.002 |
| Dataset without lab tests and medication (diagnosis only) | ||||
| Valid AUC | Test AUC | Valid AUC std | Test AUC std | |
| RNN | 0.919 | 0.911 | 0.001 | 0.002 |
| DRNN | 0.92 | 0.909 | 0.001 | 0.002 |
| QRNN | 0.919 | 0.908 | 0.002 | 0.002 |
| TLSTM | 0.919 | 0.910 | 0.001 | 0.001 |
| RETAIN | 0.919 | 0.910 | 0.001 | 0.002 |
| Feature Name | Relative Contribution | CI95up | CI95down | FDR_Q | p Value (Bonferroni Adjusted) |
|---|---|---|---|---|---|
| Glucose | 1.45 | 1.51 | 1.38 | 9.19 × 10−52 | 7.35 × 10−51 |
| Chloride | 1.41 | 1.49 | 1.35 | 1.58 × 10−36 | 2.21 × 10−35 |
| RDW | 1.52 | 1.63 | 1.42 | 2.38 × 10−30 | 3.81 × 10−29 |
| MCH | 1.50 | 1.61 | 1.40 | 3.55 × 10−27 | 7.45 × 10−26 |
| HGB | 1.39 | 1.47 | 1.32 | 9.40 × 10−27 | 2.16 × 10−25 |
| HCT | 1.38 | 1.46 | 1.31 | 2.54 × 10−26 | 6.36 × 10−25 |
| MCV | 1.50 | 1.61 | 1.39 | 1.52 × 10−23 | 4.56 × 10−22 |
| WBC | 1.37 | 1.45 | 1.29 | 9.61 × 10−23 | 3.08 × 10−21 |
| Anion Gap | 1.44 | 1.55 | 1.34 | 1.45 × 10−18 | 5.66 × 10−17 |
| Blood−Urine | 1.29 | 1.35 | 1.22 | 1.51 × 10−18 | 6.05 × 10−17 |
| ABS Neutrophils | 1.29 | 1.36 | 1.22 | 1.48 × 10−17 | 6.21 × 10−16 |
| Glucose−Urine | 1.69 | 1.89 | 1.51 | 6.40 × 10−17 | 2.82 × 10−15 |
| Glucose (Bedside test) | 1.38 | 1.49 | 1.28 | 6.23 × 10−15 | 3.43 × 10−13 |
| ABS Basophils | 1.35 | 1.45 | 1.26 | 2.62 × 10−14 | 1.60 × 10−12 |
| RBC | 1.27 | 1.34 | 1.20 | 3.61 × 10−14 | 2.24 × 10−12 |
| Potassium | 1.28 | 1.35 | 1.20 | 7.41 × 10−14 | 4.81 × 10−12 |
| INR | 1.96 | 2.31 | 1.66 | 4.61× 10−13 | 3.32 × 10−11 |
| Ionized Calcium, ISTAT | 1.66 | 1.88 | 1.46 | 1.65 × 10−12 | 1.24 × 10−10 |
| Ionized Calcium | 0.498 | 0.598 | 0.415 | 9.33 × 10−12 | 7.47 × 10−10 |
| Bacteria | 1.23 | 1.30 | 1.16 | 9.21 × 10−11 | 8.01 × 10−9 |
| Base excess | 0.460 | 0.573 | 0.370 | 3.80 × 10−10 | 3.57 × 10−8 |
| Total protein | 1.24 | 1.32 | 1.17 | 1.16 × 10−9 | 1.10 × 10−7 |
| Calcium | 1.20 | 1.27 | 1.14 | 1.32 × 10−9 | 1.27 × 10−7 |
| Red blood cells−Urine | 1.22 | 1.29 | 1.15 | 2.09 × 10−9 | 2.03 × 10−7 |
| Sodium | 1.26 | 1.35 | 1.18 | 2.67 × 10−9 | 2.67 × 10−7 |
| Prothrombin Time | 1.75 | 2.06 | 1.48 | 2.71 × 10−9 | 2.74 × 10−7 |
| MPV | 3.84 | 5.77 | 2.56 | 6.06 × 10−9 | 6.19 × 10−7 |
| Platelets | 1.29 | 1.39 | 1.19 | 1.03 × 10−8 | 1.10 × 10−6 |
| Feature Name | Relative Contribution | CI95up | CI95down | FDR_Q | p Value (Bonferroni Adjusted) |
|---|---|---|---|---|---|
| Epinastine HCL 0.05% Eye drops | 2.76 | 3.02 | 2.532 | 6.09 × 10−99 | 1.83 × 10−98 |
| Vitamin D2 1.25 mg (50,000 Unit) | 0.673 | 0.740 | 0.611 | 1.33 × 10−13 | 9.19 × 10−12 |
| Tacrolimus Cap 1 mg | 0.415 | 0.520 | 0.332 | 3.63 × 10−12 | 2.76 × 10−10 |
| Mephyton 5 mg tablet | 0.248 | 0.361 | 0.171 | 3.39 × 10−11 | 2.88 × 10−9 |
| Mycophenolate 250 mg capsules | 0.330 | 0.449 | 0.243 | 1.89 × 10−10 | 1.72 × 10−8 |
| Cartia XT (Diltiazem) 240 mg Capsule | 1.82 | 2.18 | 1.53 | 2.10 × 10−9 | 2.06 × 10−7 |
| Cephalexin 500 mg Capsule | 0.816 | 0.869 | 0.767 | 8.62 × 10−9 | 8.97 × 10−7 |
| Vol−plus tab (Multivitamin) | 0.794 | 0.852 | 0.739 | 9.33 × 10−9 | 9.80 × 10−7 |
| Stelara (Ustekinumab) 90 mg/mL syringe | 3.05 | 4.30 | 2.17 | 1.02 × 10−8 | 1.08 × 10−6 |
| Monurol (Fosfomycin) 3 gm Sachet | 0.344 | 0.479 | 0.247 | 1.78 × 10−8 | 1.98 × 10−6 |
| Trospium Chloride ER 60 mg Capsule | 2.25 | 2.91 | 1.74 | 2.70 × 10−8 | 3.13 × 10−6 |
| Vitamin B12 500 mcg Tablet | 0.755 | 0.826 | 0.690 | 4.03 × 10−8 | 4.71 × 10−6 |
| Saw Palmetto 160 mg Capsule | 0.403 | 0.540 | 0.300 | 6.10 × 10−8 | 7.32 × 10−6 |
| Mycopgenolic Acid 180 mg Tb | 0.295 | 0.443 | 0.197 | 1.46 × 10−7 | 1.93 × 10−5 |
| Prednisone tablet 10 mg | 0.835 | 0.886 | 0.786 | 1.60 × 10−7 | 2.12 × 10−5 |
| Suprep Bowel Prep Kit | 0.848 | 0.897 | 0.802 | 2.61 × 10−7 | 3.63 × 10−5 |
| Zenatane (Isotretinoin) 20 mg Capsule | 3.77 | 6.06 | 2.35 | 1.24 × 10−6 | 0.000185 |
| Tobramycin-dexamethasone Suspension | 0.665 | 0.771 | 0.573 | 2.06 × 10−6 | 0.000314 |
| Torsemide 10 mg tablets | 3.71 | 5.98 | 2.30 | 2.34 × 10−6 | 0.000360 |
| Rosuvastatin 10 Mg Tablet | 1.71 | 2.10 | 1.40 | 4.42 × 10−6 | 0.000730 |
| Feature Name | Relative Contribution | CI95up | CI95down | FDR_Q | p Value (Bonferroni Adjusted) |
|---|---|---|---|---|---|
| Esophageal reflux | 1.72 | 1.79 | 1.65 | 1.10 × 10−128 | 2.20 × 10−128 |
| Major depressive disorder, single episode, unspecified | 1.58 | 1.65 | 1.52 | 6.99 × 10−87 | 2.80 × 10−86 |
| Nicotine dependence, cigarettes, uncomplicated | 1.52 | 1.58 | 1.46 | 1.58 × 10−80 | 7.90 × 10−80 |
| Personal history of transient ischemic attack (TIA), and cerebral infarction without residual deficits | 1.82 | 1.93 | 1.72 | 2.21 × 10−77 | 1.33 × 10−76 |
| Anxiety state, unspecified | 1.50 | 1.56 | 1.44 | 7.55 × 10−74 | 5.29 × 10−73 |
| Periumbilical pain | 1.88 | 2.04 | 1.74 | 5.25 × 10−49 | 4.72 × 10−48 |
| Bipolar disorder, unspecified | 1.74 | 1.86 | 1.62 | 6.88 × 10−46 | 6.88 × 10−45 |
| Unspecified asthma with (acute) exacerbation | 1.49 | 1.58 | 1.42 | 2.51 × 10−43 | 2.76 × 10−42 |
| Epilepsy, unspecified, without mention of intractable epilepsy | 1.86 | 2.03 | 1.71 | 2.08 × 10−41 | 2.50 × 10−40 |
| Migraine, unspecified, without mention of intractable migraine without mention of status migrainosus | 1.53 | 1.63 | 1.45 | 5.85 × 10−41 | 7.61 × 10−40 |
| Irritable bowel syndrome | 1.89 | 2.09 | 1.72 | 5.50 × 10−32 | 8.25 × 10−31 |
| Mononeuritis of unspecified site | 1.45 | 1.54 | 1.37 | 5.31 × 10−30 | 9.03 × 10−29 |
| Unspecified essential hypertension | 1.73 | 1.89 | 1.58 | 2.36 × 10−29 | 4.25 × 10−28 |
| Personal history of tobacco use | 1.33 | 1.40 | 1.27 | 4.27 × 10−28 | 8.11 × 10−27 |
| Anemia, unspecified | 1.44 | 1.53 | 1.36 | 1.15 × 10−27 | 2.29 × 10−26 |
| Unspecified viral hepatitis C without hepatic coma | 2.06 | 2.32 | 1.82 | 5.20 × 10−27 | 1.14 × 10−25 |
| Supervision of normal first pregnancy | 0.459 | 0.523 | 0.402 | 9.56 × 10−27 | 2.29 × 10−25 |
| Other specified disorders of stomach and duodenum | 2.45 | 2.86 | 2.10 | 1.86 × 10−25 | 4.83 × 10−24 |
| Osteoporosis, unspecified | 2.45 | 2.88 | 2.09 | 5.31 × 10−24 | 1.43 × 10−22 |
| Lab Test | Effect on Depression | Effect on Suicide | Diagnosis | Medication Use |
|---|---|---|---|---|
| Blood: | ||||
| Auto Absolute Basophils | High EBR (Eosinophil to Basophil ratio) [79] | Poor quality of life, and suicide attempts [79] | Chronic Obstructive Pulmonary Disease (COPD) and asthma [79] | |
| Mean corpuscular hemoglobin concentration (MCHC) | Macrocytic anemia associated with folate and B12 deficiencies [62,63,64] | Anemia [62,63,64] | ||
| Red blood cell (RBC) | Increased circulating blood cells [80] | Chronic Obstructive Pulmonary Disease (COPD) [81] and nicotine use and dependence [82] | ||
| Neutrophils | High Neutrophil Lymphocyte ratio [79] | Higher NLR in violent suicide attempters [83] | Migraine, Epilepsy [57] | |
| Mean Platelet Volume (MPV) | Increased mean platelet volume (MPV) [79] | Higher MPV in violent suicide attempters [83] | ||
| Platelets | High platelet count [80] | Higher MPV in violent suicide attempters [83] | Hepatitis C [58] and iron deficiency [84] | |
| Prothrombin time (PT) | Abnormal prothrombin time (aPTT) in traumatic brain injury (TBI) patients [85] | |||
| Auto Absolute Lymphocytes | High NLR [86] | PTSD and COPD: poor quality of life, and suicide attempts [79] | COPD and asthma [79] | |
| Mean corpuscular hemoglobin (MCH) | Macrocytic anemia and major depressive disorder (MDD) associated with folate and B12 deficiencies [62,63,64] | Anemia [62,63,64] | Folate and B12 deficiencies [62,63,64] | |
| Hematocrit | Obstructive sleep apnea (OSA) and PTSD: High hemoglobin and hematocrit [87] | Higher suicidal rates among patients in higher altitudes [87] | ||
| Red cell distribution width (RDW) | High RDW [88] | RDW is a predictor of mortality in suicidal patients with organophosphate insecticide (OPI) poisoning [89] | ||
| Hemoglobin (HGB) | Higher hemoglobin [90] | |||
| Mean corpuscular volume (MCV) | High MCV [90] | |||
| White blood cell (WBC) | High WBC count in depressed patients [91] | High WBC count amongst suicide attempters [91] | Mononeuritis and Bipolar disorder [91,92] | |
| Kidney: | ||||
| Chloride | Hyperchloremia [93,94] | Chronic kidney disease (CKD) [93,94] | ||
| Sodium | Hypernatremia in traumatic brain injury [95] | High vasopressin and sodium concentrations in depressed suicide attempters [96,97] | ||
| Anion Gap | High anion gap acidosis [93,98] | Poor quality of life [94] | Hypertension [99] | |
| Metabolic syndrome: | ||||
| Glucose, POC/Glucose (Beside Test) | High blood glucose peaks and insulin levels in PTSD patients [100] | High blood glucose in suicide [101] | ||
| Cholesterol | Low serum HDL-cholesterol levels are associated with long symptom duration [102] | Abnormal cholesterol levels may cause higher suicide risk [74] | ||
| Cardiovascular: | ||||
| INR | Elevated INRs in depressed patients [103,104] | Atrial fibrillation, recurrent myocardial infarction, transient ischemic attack [105] | ||
| Potassium | Hyperkalemia in depressed patients [103,104] | Atrial fibrillation, recurrent myocardial infarction, transient ischemic attack [105] | ||
| Urine: | ||||
| Blood urine | Bacterial vaginosis increases blood urine content (BV) [106] | Poor quality of life of UTI patients increases risk of SREs [107] | Trospium chloride [108] | |
| Miscellaneous: | ||||
| Total Protein | High total protein content in trauma patients [109] | |||
| Gut microbiome (Bacteria) | High gut microbiome dysbiosis and inflammation in MDD [110] | Gut microbiome dysbiosis causes increased SREs [110] | Irritable bowel syndrome, Disorders of the stomach and duodenum, esophageal reflux, MDD, periumbilical pain [110,111] | Ustekinumab (Stelara) [54] |
| Calcium | Abnormal calcium levels, common among women, have been linked to increased risk of PTSD [47] | Abnormal calcium levels trigger the immune mediators to promote depression, anxiety, and suicidal behavior [49] | Osteoporosis and hypothyroidism, anxiety [48,49] | Diltiazem (CARTIA) [53] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miranda, O.; Fan, P.; Qi, X.; Yu, Z.; Ying, J.; Wang, H.; Brent, D.A.; Silverstein, J.C.; Chen, Y.; Wang, L. DeepBiomarker: Identifying Important Lab Tests from Electronic Medical Records for the Prediction of Suicide-Related Events among PTSD Patients. J. Pers. Med. 2022, 12, 524. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12040524
Miranda O, Fan P, Qi X, Yu Z, Ying J, Wang H, Brent DA, Silverstein JC, Chen Y, Wang L. DeepBiomarker: Identifying Important Lab Tests from Electronic Medical Records for the Prediction of Suicide-Related Events among PTSD Patients. Journal of Personalized Medicine. 2022; 12(4):524. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12040524
Chicago/Turabian StyleMiranda, Oshin, Peihao Fan, Xiguang Qi, Zeshui Yu, Jian Ying, Haohan Wang, David A. Brent, Jonathan C. Silverstein, Yu Chen, and Lirong Wang. 2022. "DeepBiomarker: Identifying Important Lab Tests from Electronic Medical Records for the Prediction of Suicide-Related Events among PTSD Patients" Journal of Personalized Medicine 12, no. 4: 524. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12040524