
Role of Metformin in Morbidity and Mortality Associated with Urinary Tract Infections in Patients with Type 2 Diabetes

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
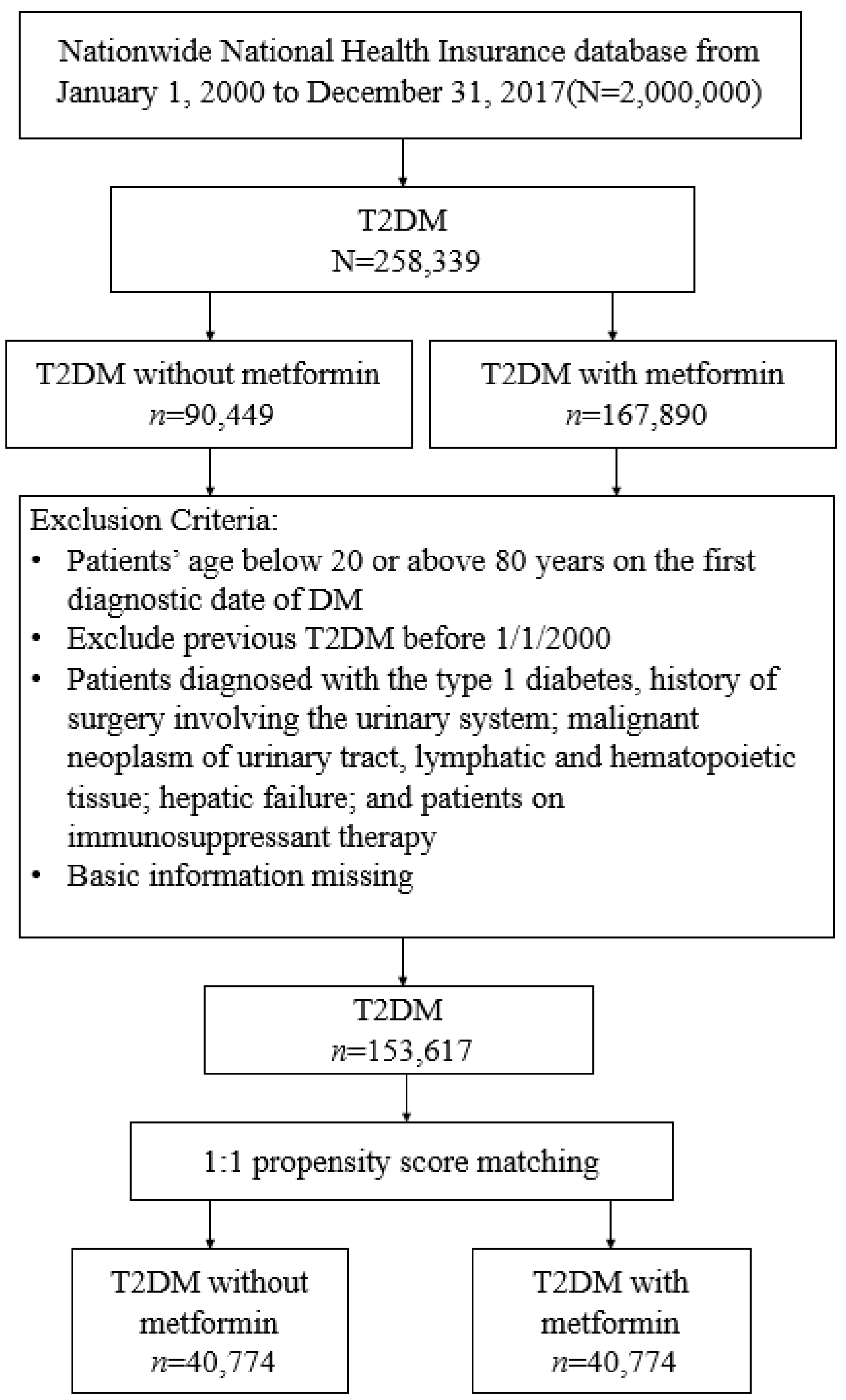
2.1. Study Population
2.2. Study Design
2.3. Procedures
2.4. Main Outcomes
2.5. Statistical Analysis
3. Results
3.1. Participants
3.2. Main Outcomes
3.3. Subgroup Analysis
3.4. Cumulative Duration of Metformin Use
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bell, J.I.; Hockaday, T.D.R. Diabetes mellitus. In Oxford Textbook of Medicine; Wetherall, D.J., Ledingham, J.G.G., Warrell, D.A., Eds.; Oxford University Press: Oxford, UK, 1996; pp. 1448–1504. [Google Scholar]
- Luk, A.O.Y.; Wu, H.; Lau, E.S.H.; Yang, A.; So, W.Y.; Chow, E.; Kong, A.P.S.; Hui, D.S.C.; Ma, R.C.W.; Chan, J.C.N. Temporal trends in rates of infection-related hospitalisations in Hong Kong people with and without diabetes, 2001–2016: A retrospective study. Diabetologia 2021, 64, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Pozzilli, P.; Leslie, R.D. Infections and diabetes: Mechanisms and prospects for prevention. Diabet. Med. 1994, 11, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Bertoni, A.G.; Saydah, S.; Brancati, F.L. Diabetes and the risk of infection-related mortality in the US. Diabetes Care 2001, 24, 1044–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harding, G.K.; Zhanel, G.G.; Nicolle, L.E.; Cheang, M.; Manitoba Diabetes Urinary Tract Infection Study Group. Antimicrobial treatment in diabetic women with asymptomatic bacteriuria. N. Engl. J. Med. 2002, 347, 1576–1583. [Google Scholar] [CrossRef] [PubMed]
- Joshi, N.; Caputo, G.M.; Weitekamp, M.R.; Karchmer, A.W. Infections in patients with diabetes mellitus. N. Engl. J. Med. 1999, 341, 1906–1912. [Google Scholar] [CrossRef] [PubMed]
- Boyko, E.J.; Fihn, S.D.; Scholes, D.; Chen, C.L.; Normand, E.H.; Yarbro, P. Diabetes and the risk of acute urinary tract infection among postmenopausal women. Diabetes Care 2002, 25, 1778–1783. [Google Scholar] [CrossRef] [Green Version]
- Thomsen, R.W.; Hundborg, H.H.; Lervang, H.H.; Johnsen, S.P.; Schønheyder, H.C.; Sørensen, H.T. Diabetes mellitus as a risk and prognostic factor for community-acquired bacteremia due to enterobacteria: A 10-year, population-based study among adults. Clin. Infect. Dis. 2005, 40, 628–631. [Google Scholar] [CrossRef] [Green Version]
- Bailey, C.J. Metformin: Historical overview. Diabetologia 2017, 60, 1566–1576. [Google Scholar] [CrossRef] [Green Version]
- Mbara, K.C.; Mofo Mato, P.E.; Driver, C.; Nzuza, S.; Mkhombo, N.T.; Gcwensa, S.K.; Mcobothi, E.N.; Owira, P.M. Metformin turns 62 in pharmacotherapy: Emergence of non-glycaemic effects and potential novel therapeutic applications. Eur. J. Pharmacol. 2021, 898, 173934. [Google Scholar] [CrossRef]
- Yang, A.; Shi, M.; Wu, H.; Lau, E.S.H.; Ma, R.C.W.; Kong, A.P.S.; So, W.Y.; Luk, A.O.Y.; Chan, J.C.N.; Chow, E. Long-term metformin use and risk of pneumonia and related death in type 2 diabetes: A registry-based cohort study. Diabetologia 2021, 64, 1760–1765. [Google Scholar] [CrossRef]
- Pan, S.W.; Yen, Y.F.; Kou, Y.R.; Chuang, P.H.; Su, V.Y.; Feng, J.Y.; Chan, Y.J.; Su, W.J. The risk of TB in patients with type 2 diabetes initiating metformin vs sulfonylurea treatment. Chest 2018, 153, 1347–1357. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.J.; Wu, Y.L.; Chao, P.W.; Kuo, S.C.; Yang, C.Y.; Li, S.Y.; Ou, S.M.; Chen, Y.T. Association between use of oral anti-diabetic drugs and the risk of sepsis: A nested case-control study. Sci. Rep. 2015, 5, 15260. [Google Scholar] [CrossRef] [Green Version]
- Patorno, E.; Garry, E.M.; Patrick, A.R.; Schneeweiss, S.; Gillet, V.G.; Zorina, O.; Bartels, D.B.; Seeger, J.D. Addressing limitations in observational studies of the association between glucose-lowering medications and all-cause mortality: A review. Drug Saf. 2015, 38, 295–310. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.M. Taiwan’s new national health insurance program: Genesis and experience so far. Health Aff. 2003, 22, 61–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.C.; Lai, M.S.; Syu, C.Y.; Chang, S.C.; Tseng, F.Y. Accuracy of diabetes diagnosis in health insurance claims data in Taiwan. J. Formos. Med. Assoc. 2005, 104, 157–163. [Google Scholar]
- Meduru, P.; Helmer, D.; Rajan, M.; Tseng, C.L.; Pogach, L.; Sambamoorthi, U. Chronic illness with complexity: Implications for performance measurement of optimal glycemic control. J. Gen. Intern. Med. 2007, 22, 408–418. [Google Scholar] [CrossRef] [Green Version]
- Young, B.A.; Lin, E.; Von Korff, M.; Simon, G.; Ciechanowski, P.; Ludman, E.J.; Everson-Stewart, S.; Kinder, L.; Oliver, M.; Boyko, E.J.; et al. Diabetes complications severity index and risk of mortality, hospitalization, and health care utilization. Am. J. Manag. Care 2008, 14, 15–23. [Google Scholar]
- D’Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Geerlings, S.E.; Meiland, R.; van Lith, E.C.; Brouwer, E.C.; Gaastra, W.; Hoepelman, A.I. Adherence of type 1-fimbriated Escherichia coli to uroepithelial cells: More in diabetic women than in control subjects. Diabetes Care 2002, 25, 1405–1409. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.J.; Ha, K.H.; Kim, D.J.; Choi, Y.H. Diabetes and the risk of infection: A national cohort study. Diabetes Metab. J. 2019, 43, 804–814. [Google Scholar] [CrossRef]
- Bramante, C.T.; Ingraham, N.E.; Murray, T.A.; Marmor, S.; Hovertsen, S.; Gronski, J.; McNeil, C.; Feng, R.; Guzman, G.; Abdelwahab, N.; et al. Metformin and risk of mortality in patients hospitalised with COVID-19: A retrospective cohort analysis. Lancet Healthy Longev. 2021, 2, e34–e41. [Google Scholar] [CrossRef]
- Liang, H.; Ding, X.; Li, L.; Wang, T.; Kan, Q.; Wang, L.; Sun, T. Association of preadmission metformin use and mortality in patients with sepsis and diabetes mellitus: A systematic review and meta-analysis of cohort studies. Crit. Care 2019, 23, 50. [Google Scholar] [CrossRef] [Green Version]
- Ursini, F.; Russo, E.; Pellino, G.; D’Angelo, S.; Chiaravalloti, A.; De Sarro, G.; Manfredini, R.; De Giorgio, R. Metformin and autoimmunity: A “new deal” of an old drug. Front. Immunol. 2018, 9, 1236. [Google Scholar] [CrossRef] [Green Version]
- Salvatore, T.; Pafundi, P.C.; Galiero, R.; Gjeloshi, K.; Masini, F.; Acierno, C.; Di Martino, A.; Albanese, G.; Alfano, M.; Rinaldi, L.; et al. Metformin: A potential therapeutic tool for rheumatologists. Pharmaceuticals 2020, 13, 234. [Google Scholar] [CrossRef]
- Saenwongsa, W.; Nithichanon, A.; Chittaganpitch, M.; Buayai, K.; Kewcharoenwong, C.; Thumrongwilainet, B.; Butta, P.; Palaga, T.; Takahashi, Y.; Ato, M.; et al. Metformin-induced suppression of IFN-α via mTORC1 signalling following seasonal vaccination is associated with impaired antibody responses in type 2 diabetes. Sci. Rep. 2020, 10, 3229. [Google Scholar] [CrossRef]
- Maniar, K.; Moideen, A.; Mittal, A.; Patil, A.; Chakrabarti, A.; Banerjee, D. A story of metformin-butyrate synergism to control various pathological conditions as a consequence of gut microbiome modification: Genesis of a wonder drug? Pharmacol. Res. 2017, 117, 103–128. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | T2DM without Metformin | T2DM with Metformin | p | ||
|---|---|---|---|---|---|
| (N = 40,774) | (N = 40,774) | ||||
| n | % | n | % | ||
| Sex | 0.123 | ||||
| female | 18,942 | 46.46 | 19,162 | 47.00 | |
| male | 21,832 | 53.54 | 21,612 | 53.00 | |
| Age | 0.164 | ||||
| 20–40 | 5049 | 12.38 | 5228 | 12.82 | |
| 41–60 | 19,158 | 46.99 | 19,093 | 46.83 | |
| 61–80 | 16,567 | 40.63 | 16,453 | 40.35 | |
| mean, (SD) † | 56.62 | 13.03 | 56.43 | 13.09 | 0.040 |
| Comorbidities | |||||
| Hypertension | 22,445 | 55.05 | 23,020 | 56.46 | <0.001 |
| Dyslipidemia | 23,577 | 57.82 | 23,990 | 58.84 | 0.003 |
| Coronary artery disease | 10,963 | 26.89 | 10,964 | 26.89 | 0.994 |
| Stroke | 3645 | 8.94 | 3719 | 9.12 | 0.366 |
| Atrial fibrillation | 41 | 0.10 | 44 | 0.11 | 0.745 |
| Heart failure | 2715 | 6.66 | 2765 | 6.78 | 0.484 |
| PAOD | 1401 | 3.44 | 1363 | 3.34 | 0.462 |
| CKD | 2028 | 4.97 | 1867 | 4.58 | 0.008 |
| Retinopathy | 2752 | 6.75 | 2687 | 6.59 | 0.362 |
| COPD | 10,570 | 25.92 | 10,728 | 26.31 | 0.208 |
| Rheumatoid arthritis | 729 | 1.79 | 699 | 1.71 | 0.423 |
| Systemic lupus erythematosus | 69 | 0.17 | 67 | 0.16 | 0.864 |
| Hepatitis B or C infection | 3493 | 8.57 | 3411 | 8.37 | 0.302 |
| Liver cirrhosis | 859 | 2.11 | 868 | 2.13 | 0.827 |
| Urolithiasis | 3890 | 9.54 | 3856 | 9.46 | 0.685 |
| Cancers | 1389 | 3.41 | 1377 | 3.38 | 0.816 |
| Psychosis | 832 | 2.04 | 880 | 2.16 | 0.241 |
| Depression | 13,147 | 32.24 | 13,148 | 32.25 | 0.994 |
| Dementia | 1136 | 2.79 | 1120 | 2.75 | 0.733 |
| Obesity | 883 | 2.17 | 898 | 2.20 | 0.719 |
| Smoking | 1073 | 2.63 | 1093 | 2.68 | 0.663 |
| Alcoholic diseases | 2309 | 5.66 | 2397 | 5.88 | 0.186 |
| CCI | <0.001 | ||||
| 1 | 9406 | 23.07 | 8924 | 21.89 | |
| 2–3 | 20,808 | 51.03 | 21,396 | 52.47 | |
| >3 | 10,560 | 25.90 | 10,454 | 25.64 | |
| DCSI | 0.082 | ||||
| 0 | 16,557 | 40.61 | 16,286 | 39.94 | |
| 1 | 7649 | 18.76 | 7851 | 19.25 | |
| ≥2 | 16,568 | 40.63 | 16,637 | 40.80 | |
| Medication | |||||
| SU | 4342 | 10.65 | 4487 | 11.00 | 0.102 |
| TZD | 364 | 0.89 | 369 | 0.91 | 0.853 |
| DPP-4i | 406 | 1.00 | 402 | 0.99 | 0.888 |
| AGI | 926 | 2.27 | 949 | 2.33 | 0.591 |
| OAD drugs | 0.503 | ||||
| 1 | 40,132 | 98.43 | 40,096 | 98.34 | |
| 2–3 | 633 | 1.55 | 671 | 1.65 | |
| >3 | 9 | 0.02 | 7 | 0.02 | |
| Insulin | 13,624 | 33.41 | 13,838 | 33.94 | 0.113 |
| Corticosteroid | 422 | 1.04 | 411 | 1.01 | 0.702 |
| Statin | 12,358 | 30.31 | 12,364 | 30.32 | 0.964 |
| NSAIDs | 39,998 | 98.10 | 40,315 | 98.87 | <0.001 |
| Aspirin | 14,514 | 35.60 | 14,611 | 35.83 | 0.478 |
| Outcome | T2DM without Metformin | T2DM with Metformin | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | PY | IR | n | PY | IR | cHR | (95% CI) | p-Value | aHR† | (95% CI) | p-Value | |
| UTI | 1084 | 186,381 | 5.82 | 1293 | 210,672 | 6.14 | 1.06 | (0.98, 1.15) | 0.1728 | 1.06 | (0.98, 1.15) | 0.1732 |
| Recurrence of UTI | 642 | 189,353 | 3.39 | 786 | 214,173 | 3.67 | 1.08 | (0.97, 1.2) | 0.1425 | 1.08 | (0.97, 1.2) | 0.1676 |
| Hospitalization for sepsis | 3579 | 182,854 | 19.57 | 4141 | 203,933 | 20.31 | 1.05 | (1, 1.1) * | 0.0431 | 1.01 | (0.97, 1.06) | 0.5882 |
| Death (UTI _Sepsis) | 93 | 192,448 | 0.48 | 62 | 218,118 | 0.28 | 0.6 | (0.44, 0.83) ** | 0.0019 | 0.58 | (0.42, 0.8) *** | <0.001 |
| Death (UTI_Sepsis) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-Metformin | Metformin | Univariate | Multivariate | |||||||||
| Variables | n | PY | IR | n | PY | IR | cHR | (95% CI) | p-Value | aHR† | (95% CI) | p-Value |
| Age | ||||||||||||
| 20–60 | 17 | 110,788 | 0.15 | 8 | 120,007 | 0.07 | 0.44 | (0.19, 1.02) | 0.056 | 0.42 | (0.18, 0.98) * | 0.045 |
| 61–80 | 65 | 65,371 | 0.99 | 63 | 77,931 | 0.81 | 0.81 | (0.58, 1.15) | 0.245 | 0.82 | (0.58, 1.17) | 0.277 |
| Sex | ||||||||||||
| female | 35 | 87,446 | 0.40 | 32 | 97,257 | 0.33 | 0.83 | (0.52, 1.35) | 0.454 | 0.69 | (0.42, 1.12) | 0.132 |
| male | 47 | 88,713 | 0.53 | 39 | 100,682 | 0.39 | 0.75 | (0.49, 1.15) | 0.186 | 0.8 | (0.52, 1.23) | 0.310 |
| Variables | Death (UTI or Sepsis) | ||||||
|---|---|---|---|---|---|---|---|
| N | PY | IR | cHR | (95% CI) | aHR† | (95% CI) | |
| Non-use of metformin | 93 | 192,448 | 0.48 | 1.00 | (Reference) | 1.00 | (Reference) |
| Cumulative metformin use (days) | |||||||
| <182 | 24 | 38,138 | 0.63 | 1.41 | (0.89, 2.24) | 1.17 | (0.74, 1.85) |
| 182–364 | 14 | 24,515 | 0.57 | 1.25 | (0.68, 2.29) | 1.22 | (0.69, 2.16) |
| >364 | 24 | 155,465 | 0.15 | 0.5 | (0.34, 0.74) *** | 0.31 | (0.2, 0.49) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yen, F.-S.; Wei, J.C.-C.; Shih, Y.-H.; Pan, W.-L.; Hsu, C.-C.; Hwu, C.-M. Role of Metformin in Morbidity and Mortality Associated with Urinary Tract Infections in Patients with Type 2 Diabetes. J. Pers. Med. 2022, 12, 702. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050702
Yen F-S, Wei JC-C, Shih Y-H, Pan W-L, Hsu C-C, Hwu C-M. Role of Metformin in Morbidity and Mortality Associated with Urinary Tract Infections in Patients with Type 2 Diabetes. Journal of Personalized Medicine. 2022; 12(5):702. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050702
Chicago/Turabian StyleYen, Fu-Shun, James Cheng-Chung Wei, Ying-Hsiu Shih, Wei-Lin Pan, Chih-Cheng Hsu, and Chii-Min Hwu. 2022. "Role of Metformin in Morbidity and Mortality Associated with Urinary Tract Infections in Patients with Type 2 Diabetes" Journal of Personalized Medicine 12, no. 5: 702. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050702