
The Impact of Concomitant Proton Pump Inhibitors on Immunotherapy Efficacy among Patients with Urothelial Carcinoma: A Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategies
2.2. Data Extraction and Quality Assessment
- -
- Population: metastatic UC patients;
- -
- Intervention: concomitant PPIs and ICIs;
- -
- Control: ICIs;
- -
- Outcome: OS and PFS.
2.3. Statistical Design
2.4. Primary and Secondary Endpoints
- To assess PFS in UC patients treated with concomitant PPIs and ICIs;
- To assess OS in UC patients treated with concomitant PPIs and ICIs.
3. Results
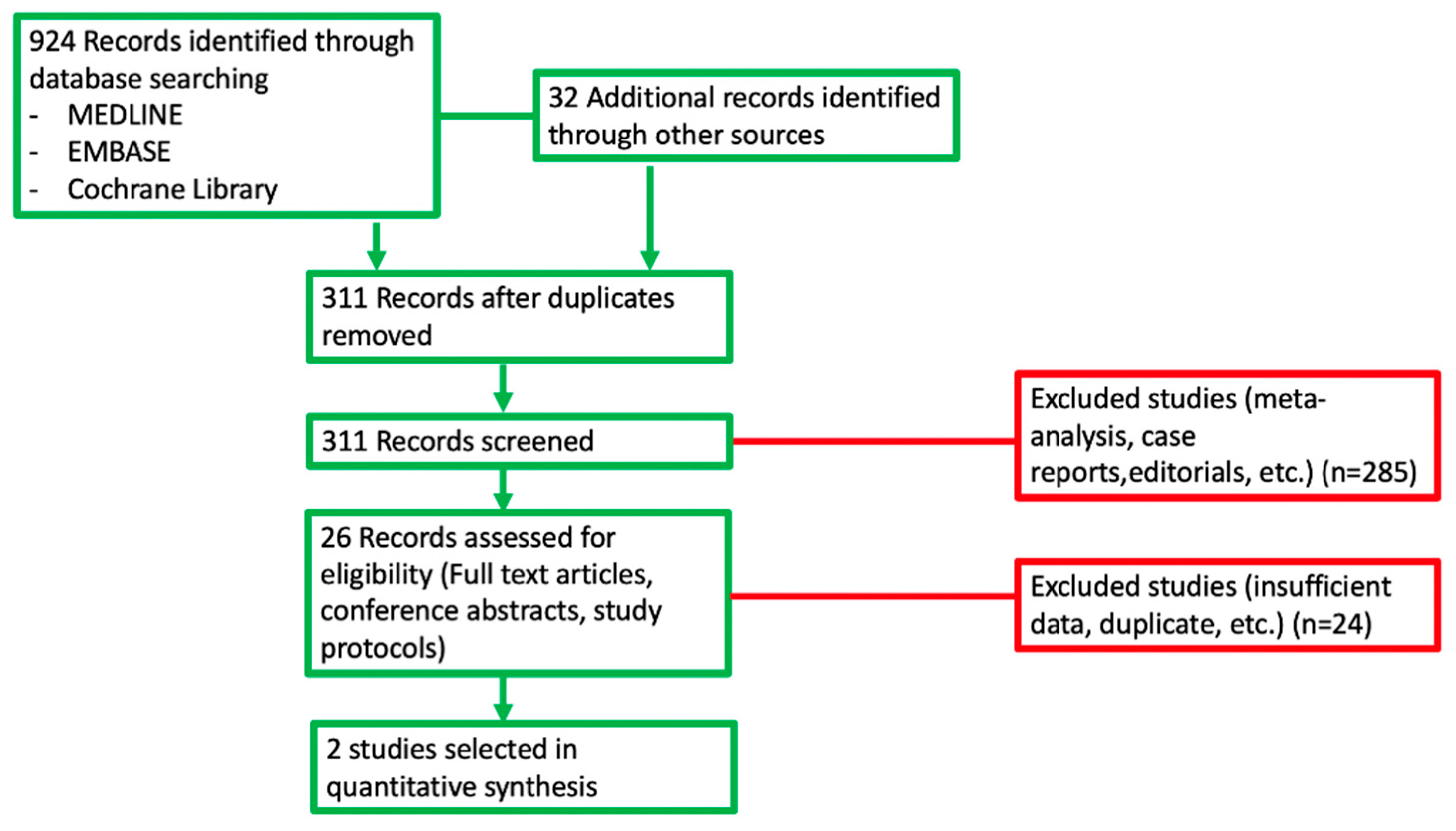
3.1. Search Results
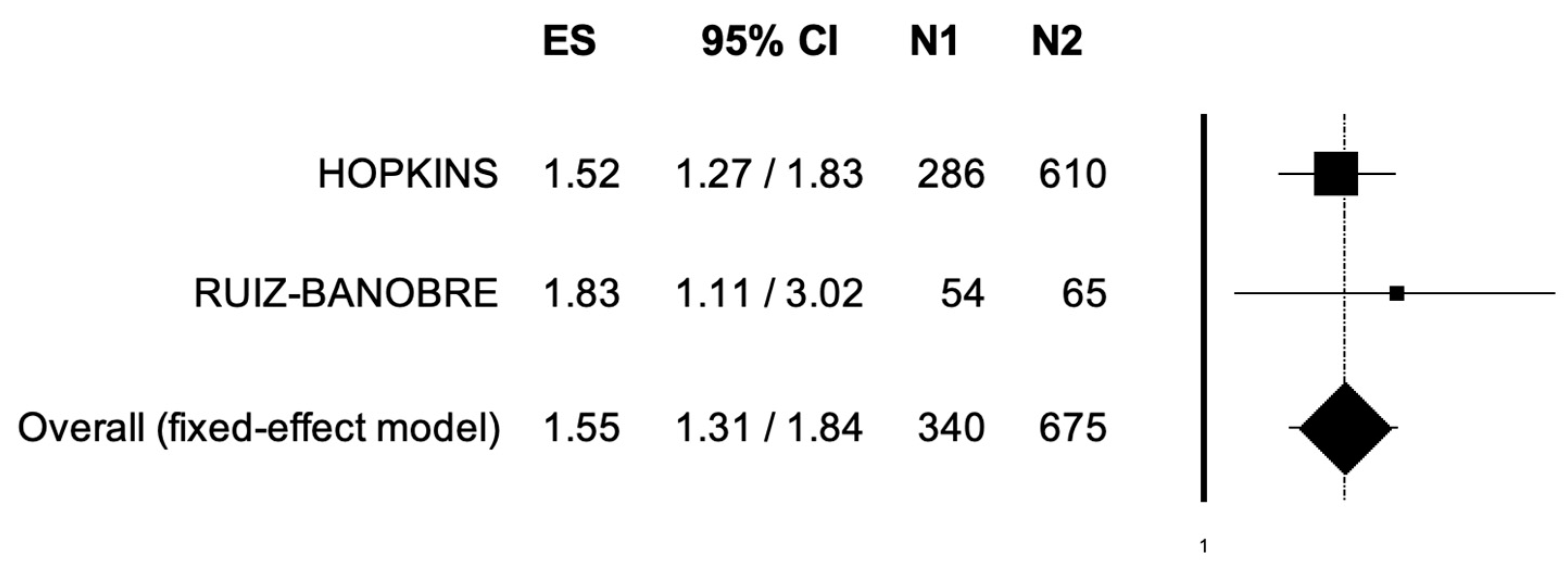
3.2. Overall Survival
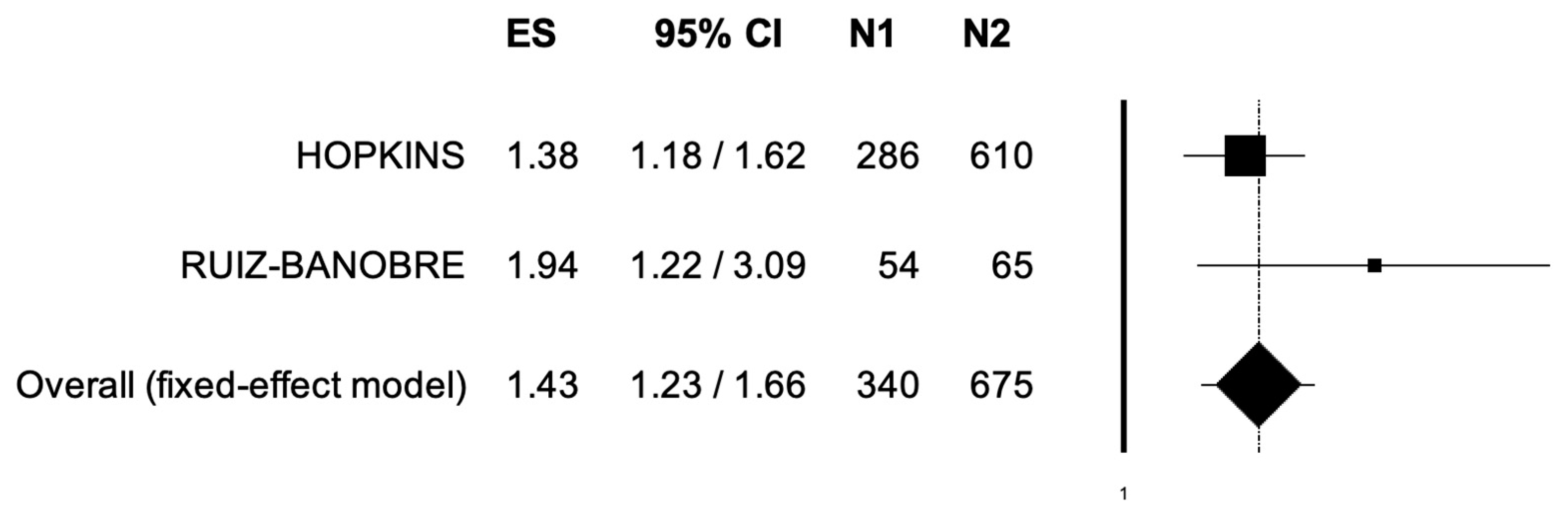
3.3. Progression-Free Survival
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef]
- Smith, A.B.; Deal, A.M.; Woods, M.E.; Wallen, E.M.; Pruthi, R.S.; Chen, R.C.; Milowsky, M.I.; Nielsen, M.E. Muscle-invasive bladder cancer: Evaluating treatment and survival in the National Cancer Data Base. BJU Int. 2014, 114, 719–726. [Google Scholar] [CrossRef]
- Godwin, J.L.; Hoffman-Censits, J.; Plimack, E. Recent developments in the treatment of advanced bladder cancer. Urol. Oncol. 2018, 36, 109–114. [Google Scholar] [CrossRef]
- Mollica, V.; Rizzo, A.; Montironi, R.; Cheng, L.; Giunchi, L.; Schiavina, R.; Santoni, M.; Fiorentino, M.; Lopez-Beltran, A.; Brnocilla, E.; et al. Current Strategies and Novel Therapeutic Approaches for Metastatic Urothelial Carcinoma. Cancers 2020, 12, 1449. [Google Scholar] [CrossRef]
- Hanna, K.S. Updates and novel treatments in urothelial carcinoma. J. Oncol. Pharm. Pract. 2019, 25, 648–656. [Google Scholar] [CrossRef]
- Powles, T.; Smith, K.; Stenzl, A.; Bedke, J. Immune checkpoint inhibition in metastatic urothelial cancer. Eur. Urol. 2017, 72, 477–481. [Google Scholar] [CrossRef]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalafonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef]
- Nadal, R.; Bellmunt, J. Management of metastatic bladder cancer. Cancer Treat. Rev. 2019, 76, 10–21. [Google Scholar] [CrossRef]
- Tripathi, A.; Plimack, E.R. Immunotherapy for Urothelial Carcinoma: Current Evidence and Future Directions. Curr. Urol. Rep. 2018, 19, 109. [Google Scholar] [CrossRef]
- Rizzo, A.; Mollica, V.; Massari, F. Expression of Programmed Cell Death Ligand 1 as a Predictive Biomarker in Metastatic Urothelial Carcinoma Patients Treated with First-line Immune Checkpoint Inhibitors versus Chemotherapy: A Systematic Review and Meta-analysis. Eur. Urol. Focus 2022, 8, 152–159. [Google Scholar] [CrossRef]
- Nadal, R.; Apolo, A.B.; Girardi, D.M.; Hahn, N.M.; Bellmunt, J. Systemic therapy issues: Immunotherapy in nonmetastatic urothelial cancer. Urol. Oncol. Semin. Orig. Investig. 2020; in press. [Google Scholar] [CrossRef]
- Rey-Cárdenas, M.; Guerrero-Ramos, F.; Gómez de Liaño Lista, A.; Carretero-González, A.; Bote, H.; Herrera-Juárez, M.; Carril-Ajuria, L.; Martín-Soberón, M.; Sepulveda, J.M.; Billalabeitia, E.G.; et al. Recent advances in neoadjuvant immunotherapy for urothelial bladder cancer: What to expect in the near future. Cancer Treat. Rev. 2021, 93, 102142. [Google Scholar] [CrossRef]
- Cortellini, A.; Tucci, M.; Adamo, V.; Stucci, L.S.; Russo, A.; Tanda, E.T.; Spagnolo, F.; Rastelli, F.; Bisonni, R.; Santini, D.; et al. Integrated analysis of concomitant medications and oncological outcomes from PD-1/PD-L1 checkpoint inhibitors in clinical practice. J. Immunother. Cancer 2020, 8, e001361. [Google Scholar] [CrossRef]
- Mukherjee, S.; Ibrahimi, S.; Khalid, B.; Roman, D.; Zhao, D.; Aljumaily, R. Do proton pump inhibitors modulate the efficacy of anti-PD-1/PD-L1 therapy? A retrospective study. J. Oncol. Pharm. Pract. 2019, 25, 762–764. [Google Scholar] [CrossRef]
- Chalabi, M.; Cardona, A.; Nagarkar, D.R.; Dhawahir Scala, A.; Gandara, D.R.; Rittmeyer, A.; Albert, M.L.; Powles, T.; Kok, M.; Herrera, F.G.; et al. Efficacy of chemotherapy and atezolizumab in patients with non-small-cell lung cancer receiving antibiotics and proton pump inhibitors: Pooled post hoc analyses of the OAK and POPLAR trials. Ann. Oncol. 2020, 31, 525–531. [Google Scholar] [CrossRef] [Green Version]
- Hussain, N.; Naeem, M.; Pinato, D.J. Concomitant medications and immune checkpoint inhibitor therapy for cancer: Causation or association? Hum. Vaccines Immunother. 2021, 17, 55–61. [Google Scholar] [CrossRef]
- Fessler, J.; Matson, V.; Gajewski, T.F. Exploring the emerging role of the microbiome in cancer immunotherapy. J. Immunother. Cancer 2019, 7, 108. [Google Scholar] [CrossRef]
- Imhann, F.; Bonder, M.J.; Vich Vila, A.; Fu, J.; Mujagic, Z.; Vork, L.; Tigchelaar, E.F.; Jankipersadsing, S.A.; Cenit, M.C.; Harmsen, H.J.; et al. Proton pump inhibitors affect the gut microbiome. Gut 2016, 65, 740–748. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, S.; Pandey, M.; Ammannagari, N.; Wang, C.; Bucsek, M.J.; Hamad, L.; Repasky, E.; Ernstoff, M.S. Impact of concomitant medication use and immune-related adverse events on response to immune checkpoint inhibitors. Immunotherapy 2020, 12, 141–149. [Google Scholar] [CrossRef]
- Mollica, V.; Santoni, M.; Matrana, M.R.; Basso, U.; De Giorgi, U.; Rizzo, A.; Maruzzo, M.; Marchetti, A.; Rosellini, M.; Bleve, S.; et al. Concomitant Proton Pump Inhibitors and Outcome of Patients Treated with Nivolumab Alone or Plus Ipilimumab for Advanced Renal Cell Carcinoma. Target. Oncol. 2022, 17, 61–68. [Google Scholar] [CrossRef]
- Gaucher, L.; Adda, L.; Séjourné, A.; Joachim, C.; Guillaume, C.; Poulet, C.; Liabeuf, S.; Gras-Champel, V.; Masmoudi, K.; Houessinon, A.; et al. Associations between dysbiosis-inducing drugs, overall survival and tumor response in patients treated with immune checkpoint inhibitors. Ther. Adv. Med. Oncol. 2021, 13, 17588359211000591. [Google Scholar] [CrossRef]
- Iglesias-Santamaría, A. Impact of antibiotic use and other concomitant medications on the efficacy of immune checkpoint inhibitors in patients with advanced cancer. Clin. Transl. Oncol. 2020, 22, 1481–1490. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [Green Version]
- Petitti, D.B. Approaches to heterogeneity in meta-analysis. Stat. Med. 2001, 20, 3625–3633. [Google Scholar] [CrossRef]
- Hopkins, A.M.; Kichenadasse, G.; Karapetis, C.S.; Rowland, A.; Sorich, M.J. Concomitant Proton Pump Inhibitor Use and Survival in Urothelial Carcinoma Treated with Atezolizumab. Clin. Cancer Res. 2020, 26, 5487–5493. [Google Scholar] [CrossRef]
- Ruiz-Bañobre, J.; Molina-Díaz, A.; Fernández-Calvo, O.; Fernández-Núñez, N.; Medina-Colmenero, A.; Santomé, L.; Lázaro-Quintela, M.; Mateos-González, M.; García-Cid, N.; López-López, R.; et al. Rethinking prognostic factors in locally advanced or metastatic urothelial carcinoma in the immune checkpoint blockade era: A multicenter retrospective study. ESMO Open 2021, 6, 100090. [Google Scholar] [CrossRef]
- Bin Riaz, I.; Khan, A.M.; Catto, J.W.; Hussain, S.A. Bladder cancer: Shedding light on the most promising investigational drugs in clinical trials. Expert Opin. Investig. Drugs 2021, 30, 837–855. [Google Scholar] [CrossRef]
- Bandini, M.; Ross, J.S.; Raggi, D.; Gallina, A.; Colecchia, M.; Lucianò, R.; Giannatempo, P.; Farè, E.; Pederzoli, F.; Bianchi, M.; et al. Predicting the Pathologic Complete Response after Neoadjuvant Pembrolizumab in Muscle-Invasive Bladder Cancer. J. Natl. Cancer Inst. 2021, 113, 48–53. [Google Scholar] [CrossRef]
- Rouanne, M.; Bajorin, D.F.; Hannan, R.; Galsky, M.D.; Williams, S.B.; Necchi, A.; Sharma, P.; Powles, T. Rationale and Outcomes for Neoadjuvant Immunotherapy in Urothelial Carcinoma of the Bladder. Eur. Urol. Oncol. 2020, 3, 728–738. [Google Scholar] [CrossRef] [PubMed]
- Renner, A.; Burotto, M.; Valdes, J.M.; Roman, J.C.; Walton-Diaz, A. Neoadjuvant immunotherapy for muscle invasive urothelial bladder carcinoma: Will it change current standards? Ther. Adv. Urol. 2021, 13, 17562872211029779. [Google Scholar] [CrossRef]
- Petrelli, F.; Iaculli, A.; Signorelli, D.; Ghidini, A.; Dottorini, L.; Perego, G.; Ghidini, M.; Zaniboni, A.; Gori, S.; Inno, A. Survival of Patients Treated with Antibiotics and Immunotherapy for Cancer: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 1458. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, H.; Chen, S.; Li, Z.; Chen, J.; Li, W. The effect of concomitant use of statins, NSAIDs, low-dose aspirin, metformin and beta-blockers on outcomes in patients receiving immune checkpoint inhibitors: A systematic review and meta-analysis. Oncoimmunology 2021, 10, 1957605. [Google Scholar] [CrossRef]
- Maier, L.; Pruteanu, M.; Kuhn, M.; Zeller, G.; Telzerow, A.; Anderson, E.E.; Brochado, A.R.; Fernandez, K.C.; Dose, H.; Mori, H.; et al. Extensive impact of non-antibiotic drugs on human gut bacteria. Nature 2018, 555, 623–628. [Google Scholar] [CrossRef]
- Lee, K.A.; Shaw, H.M.; Bataille, V.; Nathan, P.; Spector, T.D. Role of the Gut Microbiome for Cancer Patients Receiving Immunotherapy: Dietary and Treatment Implications. Eur. J. Cancer 2020, 138, 149–155. [Google Scholar] [CrossRef]
- Buti, S.; Bersanelli, M.; Perrone, F.; Bracarda, S.; Di Maio, M.; Giusti, R.; Nigro, O.; Cortinovis, D.L.; Aerts, J.G.J.V.; Guaitoli, G.; et al. Predictive Ability of a Drug-Based Score in Patients with Advanced Non-Small-Cell Lung Cancer Receiving First-Line Immunotherapy. Eur. J. Cancer 2021, 150, 224–231. [Google Scholar] [CrossRef]
- Bruno, G.; Zaccari, P.; Rocco, G.; Scalese, G.; Panetta, C.; Porowska, B.; Pontone, S.; Severi, C. Proton pump inhibitors and dysbiosis: Current knowledge and aspects to be clarified. World J. Gastroenterol. 2019, 25, 2706–2719. [Google Scholar] [CrossRef]
- Laheij, R.J.; Sturkenboom, M.C.; Hassing, R.J.; Dieleman, J.; Stricker, B.H.; Jansen, J.B. Risk of community-acquired pneumonia and use of gastric acid-suppressive drugs. JAMA 2004, 292, 1955–1960. [Google Scholar] [CrossRef]
- Aybay, C.; Imir, T.; Okur, H. The effect of omeprazole on human natural killer cell activity. Gen. Pharmacol. 1995, 26, 1413–1418. [Google Scholar] [CrossRef]
- Zedtwitz-Liebenstein, K.; Wenisch, C.; Patruta, S.; Parschalk, B.; Daxböck, F.; Graninger, W. Omeprazole treatment diminishes intra- and extracellular neutrophil reactive oxygen production and bactericidal activity. Crit. Care Med. 2002, 30, 1118–1122. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Country | Number pts PPIs/no PPIs | Median Follow-up Time | ECOG-PS 0 or 1 (Percentage) | Median Age with Range | Type of ICIs | Newcastle–Ottawa Quality Assessment Scale |
|---|---|---|---|---|---|---|---|
| Ruiz-Banobre (2021) [27] | Spain | 54/65 | 9.5 months | 83% | 69 (38–89) | Atezolizumab, Durvalumab, Nivolumab, Pembrolizumab | 7 |
| Hopkins (2020) [26] | Europe, North America, Asia—Pacific region | 286/610 | 11 and 17 months | 100% | 66 (36–84) and 67 (33–88) | Atezolizumab | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzo, A.; Santoni, M.; Mollica, V.; Ricci, A.D.; Calabrò, C.; Cusmai, A.; Gadaleta-Caldarola, G.; Palmiotti, G.; Massari, F. The Impact of Concomitant Proton Pump Inhibitors on Immunotherapy Efficacy among Patients with Urothelial Carcinoma: A Meta-Analysis. J. Pers. Med. 2022, 12, 842. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050842
Rizzo A, Santoni M, Mollica V, Ricci AD, Calabrò C, Cusmai A, Gadaleta-Caldarola G, Palmiotti G, Massari F. The Impact of Concomitant Proton Pump Inhibitors on Immunotherapy Efficacy among Patients with Urothelial Carcinoma: A Meta-Analysis. Journal of Personalized Medicine. 2022; 12(5):842. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050842
Chicago/Turabian StyleRizzo, Alessandro, Matteo Santoni, Veronica Mollica, Angela Dalia Ricci, Concetta Calabrò, Antonio Cusmai, Gennaro Gadaleta-Caldarola, Gennaro Palmiotti, and Francesco Massari. 2022. "The Impact of Concomitant Proton Pump Inhibitors on Immunotherapy Efficacy among Patients with Urothelial Carcinoma: A Meta-Analysis" Journal of Personalized Medicine 12, no. 5: 842. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm12050842