Screening, Linkage to Care and Treatment of Hepatitis C Infection in Primary Care Setting in the South of Italy

 , ,
, ,
Abstract
:1. Introduction
2. Methods
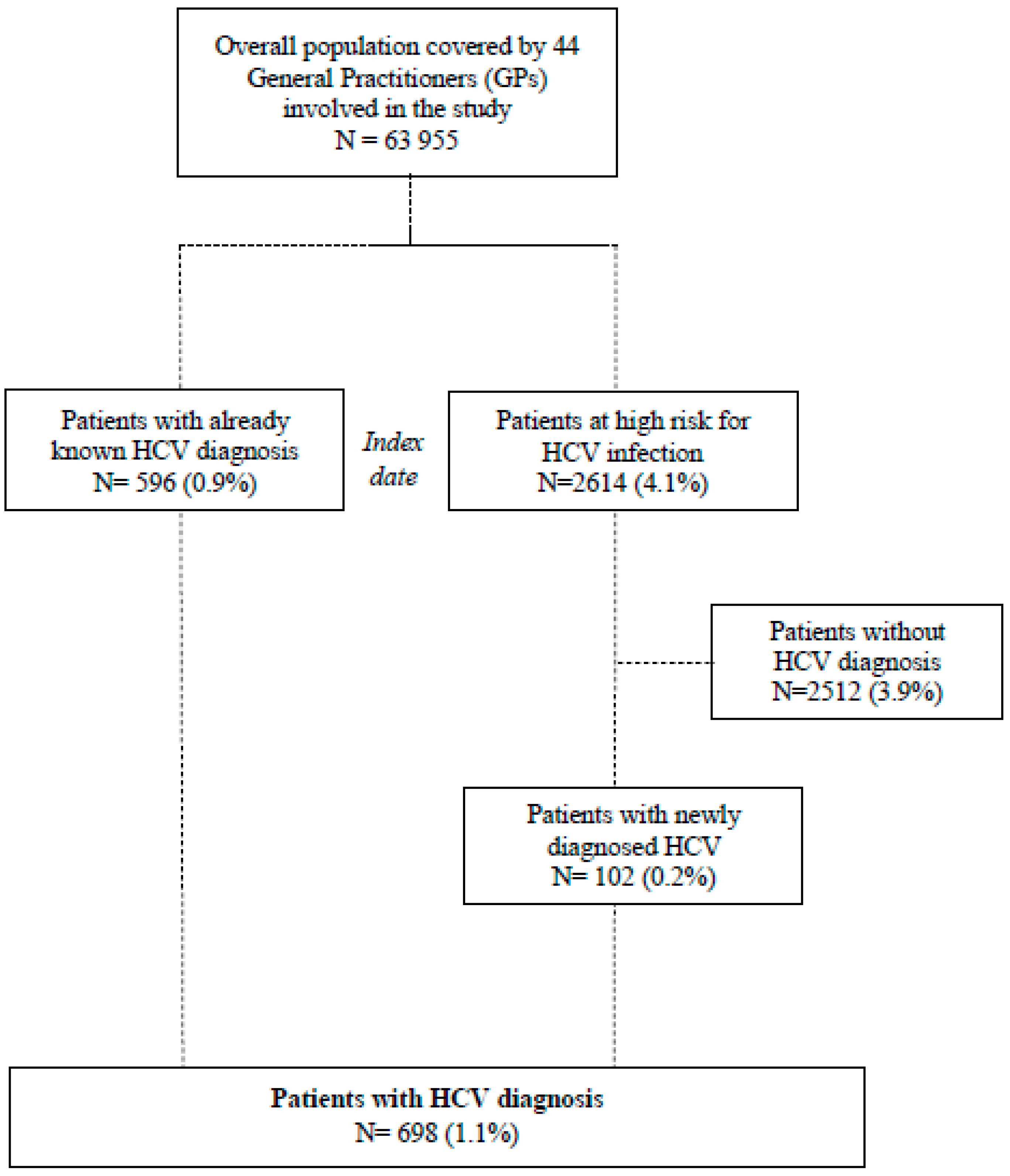
2.1. Study Population and Data Collection
2.2. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- El Khoury, A.C.; Wallace, C.; Klimack, W.K.; Razavi, H. Economic burden of hepatitis C-associated diseases: Europe, Asia Pacific, and the Americas. J. Med. Econ. 2012, 15, 887–896. [Google Scholar] [CrossRef]
- Polaris Observatory, H.C.V.C. Global prevalence and genotype distribution of hepatitis C virus infection in 2015: A modelling study. Lancet. Gastroenterol. Hepatol. 2017, 2, 161–176. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.H.; Yang, H.I.; Yuan, Y.; L’Italien, G.; Chen, C.J. Epidemiology and natural history of hepatitis C virus infection. World J. Gastroenterol. 2014, 20, 9270–9280. [Google Scholar] [CrossRef]
- Leone, N.; Rizzetto, M. Natural history of hepatitis C virus infection: From chronic hepatitis to cirrhosis, to hepatocellular carcinoma. Minerva Gastroenterol. Dietol. 2005, 51, 31–46. [Google Scholar]
- Bucci, L.; Garuti, F.; Lenzi, B.; Pecorelli, A.; Farinati, F.; Giannini, E.G.; Granito, A.; Ciccarese, F.; Rapaccini, G.L.; Di Marco, M.; et al. The evolutionary scenario of hepatocellular carcinoma in Italy: An update. Liver Int. 2017, 37, 259–270. [Google Scholar] [CrossRef]
- Kieran, J.A.; Norris, S.; O’Leary, A.; Walsh, C.; Merriman, R.; Houlihan, D.; McCormick, P.A.; McKiernan, S.; Bergin, C.; Barry, M. Hepatitis C in the era of direct-acting antivirals: Real-world costs of untreated chronic hepatitis C; a cross-sectional study. BMC Infect. Dis. 2015, 15, 471. [Google Scholar] [CrossRef] [Green Version]
- Lavanchy, D. Evolving epidemiology of hepatitis C virus. Clin. Microbiol. Infect. 2011, 17, 107–115. [Google Scholar] [CrossRef] [Green Version]
- Kohli, A.; Shaffer, A.; Sherman, A.; Kottilil, S. Treatment of hepatitis C: A systematic review. JAMA 2014, 312, 631–640. [Google Scholar] [CrossRef]
- Terrault, N.A.; Hassanein, T.I. Management of the patient with SVR. J. Hepatol. 2016, 65, S120–S129. [Google Scholar] [CrossRef] [Green Version]
- WHO. Global Health Sector Strategy on Viral Hepatitis, 2016–2021; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Registri AIFA per il Monitoraggio dei Farmaci Anti-HCV. Available online: www.aifa.gov.it/aggiornamento-epatite-c (accessed on 30 September 2020).
- Hollande, C.; Parlati, L.; Pol, S. Micro-elimination of hepatitis C virus. Liver Int. 2020, 40, 67–71. [Google Scholar] [CrossRef] [Green Version]
- Masarone, M.; Caruso, R.; Aglitti, A.; Izzo, C.; de Matteis, G.; Attianese, M.R.; Pagano, A.M.; Persico, M. Hepatitis C virus infection in jail: Difficult-to-reach, not to-treat. Results of a point-of-care screening and treatment program. Dig. Liver Dis. 2020, 52, 541–546. [Google Scholar] [CrossRef]
- Persico, M.; Masarone, M.; Aglitti, A.; Armenante, C.; Giordano, A.; Guardiola, A.; Raimondi, G.; Contaldi, C.; Nigro, C.; Marena, G.; et al. HCV point-of-care screening programme and treatment options for people who use drugs in a metropolitan area of Southern Italy. Liver Int. 2019, 39, 1845–1851. [Google Scholar] [CrossRef]
- Bartholomew, T.S.; Grosgebauer, K.; Huynh, K.; Cos, T. Integration of hepatitis C treatment in a primary care federally qualified health center; Philadelphia, Pennsylvania, 2015–2017. Infect. Dis. 2019, 12. [Google Scholar] [CrossRef] [Green Version]
- Drainoni, M.L.; Litwin, A.H.; Smith, B.D.; Koppelman, E.A.; McKee, M.D.; Christiansen, C.L.; Gifford, A.L.; Weinbaum, C.M.; Southern, W.N. Effectiveness of a risk screener in identifying hepatitis C virus in a primary care setting. Am. J. Public Health 2012, 102, e115–e121. [Google Scholar] [CrossRef]
- Datta, S.; Horwood, J.; Hickman, M.; Sharp, D. Case-finding for hepatitis C in primary care: A mixed-methods service evaluation. Br. J. Gen. Pract. 2014, 64, e67–e74. [Google Scholar] [CrossRef] [Green Version]
- Thomson, M.; Konerman, M.A.; Choxi, H.; Lok, A.S. Primary care physician perspectives on hepatitis C management in the era of direct-acting antiviral therapy. Dig. Dis. Sci. 2016, 61, 3460–3468. [Google Scholar] [CrossRef]
- Andriulli, A.; Stroffolini, T.; Mariano, A.; Valvano, M.R.; Grattagliano, I.; Ippolito, A.M.; Grossi, A.; Brancaccio, G.; Coco, C.; Russello, M.; et al. Declining prevalence and increasing awareness of HCV infection in Italy: A population-based survey in five metropolitan areas. Eur. J. Intern. Med. 2018, 53, 79–84. [Google Scholar] [CrossRef]
- Lombardi, A.; Colaneri, M.; Vijayagopal, K.A.; Sambo, M.; Legnazzi, P.; Sacchi, P.; Zuccaro, V.; Maiocchi, L.; Maserati, R.; Gulminetti, R.; et al. Patients with chronic hepatitis C receiving treatment with direct acting antivirals: How is this population changing? Dig. Liver Dis. 2020. [Google Scholar] [CrossRef]
- Guadagnino, V.; Stroffolini, T.; Caroleo, B.; Menniti Ippolito, F.; Rapicetta, M.; Ciccaglione, A.R.; Chionne, P.; Madonna, E.; Costantino, A.; De Sarro, G.; et al. Hepatitis C virus infection in an endemic area of Southern Italy 14 years later: Evidence for a vanishing infection. Dig. Liver Dis. 2013, 45, 403–407. [Google Scholar] [CrossRef]
- Lapi, F.; Capogrosso Sansone, A.; Mantarro, S.; Simonetti, M.; Tuccori, M.; Blandizzi, C.; Rossi, A.; Corti, G.; Bartoloni, A.; Bellia, A.; et al. Hepatitis C virus infection: Opportunities for an earlier detection in primary care. Eur. J. Gastroenterol. Hepatol. 2017, 29, 271–276. [Google Scholar] [CrossRef]
- Andreone, P.; Di Marco, V.; Gaeta, G.B.; Fagiuoli, S.; Vukotic, R.; Craxi, A. Current and forthcoming perspectives in linkage to care of hepatitis C virus infection: Assessment of an Italian focus group. Dig. Liver Dis. 2019, 51, 915–921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saab, S.; Challita, Y.P.; Najarian, L.M.; Guo, R.; Saggi, S.S.; Choi, G. Hepatitis C screening: Barriers to linkage to care. J. Clin. Transl. Hepatol. 2019, 7, 226–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irving, W.L.; Smith, S.; Cater, R.; Pugh, S.; Neal, K.R.; Coupland, C.A.; Ryder, S.D.; Thomson, B.J.; Pringle, M.; Bicknell, M.; et al. Clinical pathways for patients with newly diagnosed hepatitis C—What actually happens. J. Viral Hepat. 2006, 13, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Moorman, A.C.; Gordon, S.C.; Rupp, L.B.; Spradling, P.R.; Teshale, E.H.; Lu, M.; Nerenz, D.R.; Nakasato, C.C.; Boscarino, J.A.; Henkle, E.M.; et al. Baseline characteristics and mortality among people in care for chronic viral hepatitis: The chronic hepatitis cohort study. Clin. Infect. Dis. 2013, 56, 40–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cammarota, S.; Citarella, A.; Guida, A.; Conti, V.; Iannaccone, T.; Flacco, M.E.; Bravi, F.; Naccarato, C.; Piscitelli, A.; Piscitelli, R.; et al. The inpatient hospital burden of comorbidities in HCV-infected patients: A population-based study in two Italian regions with high HCV endemicity (The BaCH study). PLoS ONE 2019, 14, e0219396. [Google Scholar] [CrossRef] [Green Version]
- Samuel, S.T.; Martinez, A.D.; Chen, Y.; Markatou, M.; Talal, A.H. Hepatitis C virus knowledge improves hepatitis C virus screening practices among primary care physicians. World J. Hepatol. 2018, 10, 319–328. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall (N = 698)% | Patients with Already Known HCV Diagnosis (N = 596)% | Patients with Newly Diagnosed HCV (N = 102)% | p Value | |
|---|---|---|---|---|
| Age Groups | ||||
| <40 | 5.2 | 5.4 | 3.5 | 0.13 |
| 40–49 | 9.7 | 10.0 | 8.0 | |
| 50–59 | 13.7 | 12.4 | 21.8 | |
| 60–69 | 21.5 | 22.4 | 16.1 | |
| ≥70 | 49.9 | 49.8 | 50.6 | |
| Gender | ||||
| Male | 48.9 | 47.4 | 57.6 | 0.06 |
| Female | 51.1 | 52.6 | 42.4 | |
| Comorbidities | ||||
| Diabetes | 14.7 | 14.3 | 16.7 | 0.54 |
| CKD | 4.9 | 4.2 | 8.8 | 0.05 |
| Obesity | 4.3 | 3.7 | 7.8 | 0.06 |
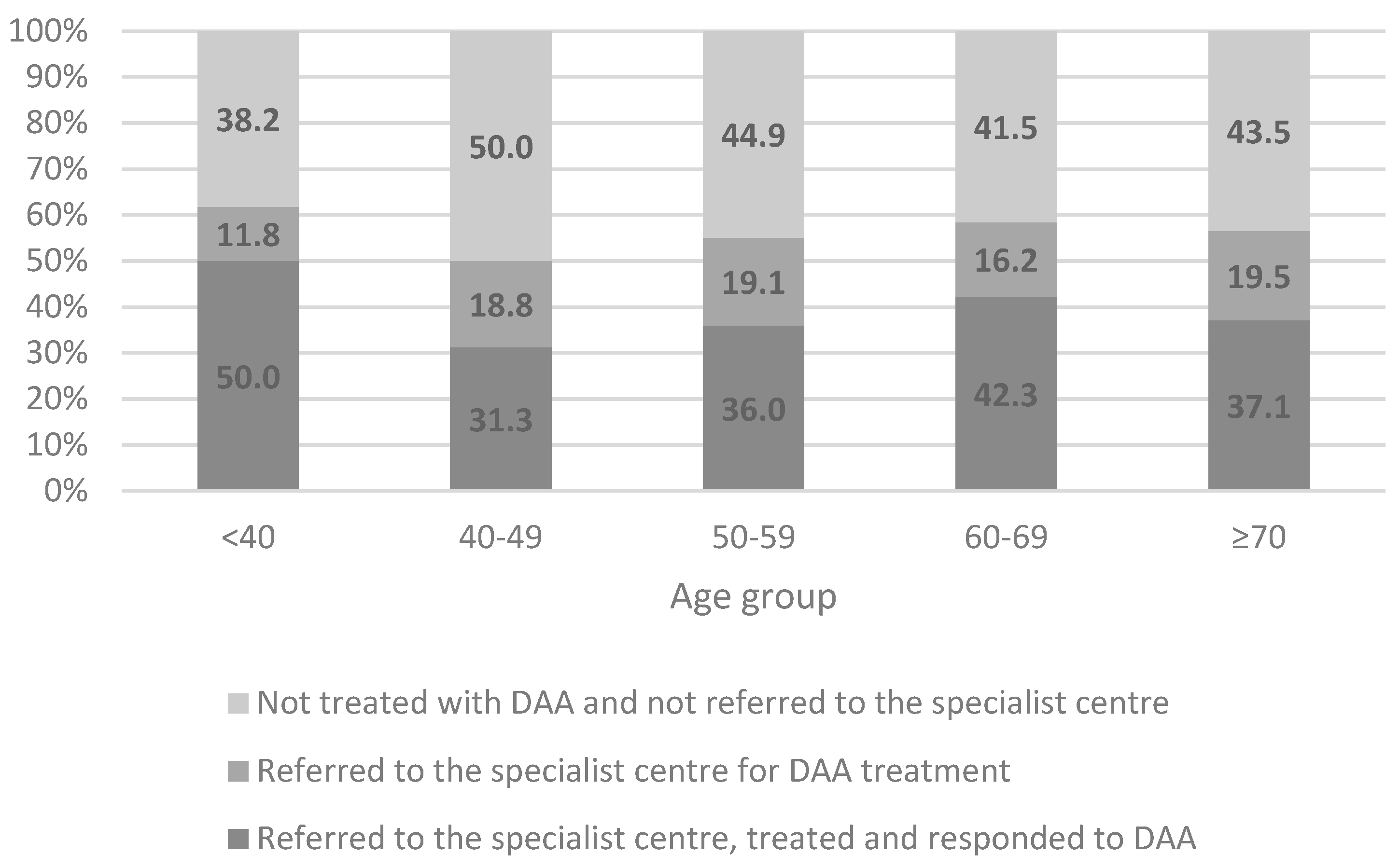
| Overall N = 698 | Patients with Already Known HCV Diagnosis N = 596 | Patients with Newly Diagnosed HCV N = 102 | p Value | ||
|---|---|---|---|---|---|
| % 1 | % 2 | % | % | ||
| Referred to the Specialist Center, Treated and Responded to DAA | 0.4 | 38.8 | 39.6 | 33.7 | 0.26 |
| Referred to the Specialist Center for DAA Treatment | 0.2 | 18.9 | 18.1 | 23.8 | 0.18 |
| Not Treated with DAA and not Referred to the Specialist Center | 0.5 | 42.3 | 42.3 | 42.5 | 0.96 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Citarella, A.; Cammarota, S.; Bernardi, F.F.; Coppola, C.; D’Antò, M.; Fogliasecca, M.; Giusto, E.; Masarone, M.; Salomone Megna, A.; Sellitto, C.; et al. Screening, Linkage to Care and Treatment of Hepatitis C Infection in Primary Care Setting in the South of Italy. Life 2020, 10, 359. https://0-doi-org.brum.beds.ac.uk/10.3390/life10120359
Citarella A, Cammarota S, Bernardi FF, Coppola C, D’Antò M, Fogliasecca M, Giusto E, Masarone M, Salomone Megna A, Sellitto C, et al. Screening, Linkage to Care and Treatment of Hepatitis C Infection in Primary Care Setting in the South of Italy. Life. 2020; 10(12):359. https://0-doi-org.brum.beds.ac.uk/10.3390/life10120359
Chicago/Turabian StyleCitarella, Anna, Simona Cammarota, Francesca F. Bernardi, Carmine Coppola, Maria D’Antò, Marianna Fogliasecca, Elio Giusto, Mario Masarone, Angelo Salomone Megna, Carmine Sellitto, and et al. 2020. "Screening, Linkage to Care and Treatment of Hepatitis C Infection in Primary Care Setting in the South of Italy" Life 10, no. 12: 359. https://0-doi-org.brum.beds.ac.uk/10.3390/life10120359