
Acute Inflammation in Cerebrovascular Disease: A Critical Reappraisal with Focus on Human Studies


1
Department of Neurology, Centro Hospitalar Universitário São João, 4200-319 Porto, Portugal
2
Department of Neurology, Hospital Central do Funchal, 9000-177 Funchal, Portugal
3
Department of Clinical Neurosciences and Mental Health, Faculty of Medicine, University of Porto, 4200-319 Porto, Portugal
4
Cardiovascular R & D Unit, Faculty of Medicine, University of Porto, 4200-319 Porto, Portugal
*
Author to whom correspondence should be addressed.
Life 2021, 11(10), 1103; https://0-doi-org.brum.beds.ac.uk/10.3390/life11101103
Submission received: 2 September 2021
/
Revised: 6 October 2021
/
Accepted: 12 October 2021
/
Published: 17 October 2021
(This article belongs to the Special Issue Innovative Stroke Diagnostic and Treatment Strategies)
Abstract
:Recent attention has been focused on the field of inflammatory biomarkers associated with vascular disorders, regarding diagnosis, prognosis, and possible therapeutical targets. In this study, we aimed to perform a comprehensive review of the literature regarding the use of inflammatory biomarkers in stroke patients. We searched studies that evaluated inflammation biomarkers associated with Cerebrovascular Disease (CVD), namely, ischemic Stroke (IS), Intracerebral Hemorrhage (ICH) and Cerebral Venous Thrombosis (CVT). As of today, neutrophil–lymphocyte ratio (NLR) seems the be the most widely studied and accepted biomarker for cerebrovascular disease due to its easy access and availability. Although demonstrated as a prognostic risk factor, in IS, ICH and CVT, its diagnostic role is still under investigation. Several other prognostic factors could be used or even combined together into a diagnostic or prognostic index. Multiple inflammatory biomarkers appear to be involved in IS, ICH, and CVT. Blood inflammatory cells, easily measured and accessible at admission may provide information regarding accurate diagnosis and prognosis. Although not yet a reality, increasing evidence exists to suggest that these may become potential therapeutic targets, likely influencing or mitigating complications of CVD and improving prognosis. Nevertheless, further larger, well-designed randomized clinical trials are still needed to follow up this hypothesis.
1. Introduction
Cerebrovascular disorders (CVD) are a leading cause of death and disability worldwide [1]. Most consist of acute arterial events, with around 80% being ischemic strokes (IS) [2]. Intracerebral spontaneous hemorrhages (ICH) are also a common cause of stroke, leading to higher mortality [3]. Cerebral venous thrombosis (CVT), although infrequent, affect a younger population, leading to long-term morbidity [4].
Acute stroke occurs suddenly, and the few initial therapeutic options have proven to be efficacious at this phase. In acute IS, the chemical (thrombolysis) or mechanical (thrombectomy) removal of the thrombus are examples [5]. In ICH, Acute blood pressure lowering, and surgery do not reach high levels of evidence [6]. Currently, considerable investigation efforts are being devoted to further elucidating secondary damage after the initial acute insult. Recent attention has been focused on the field of inflammatory biomarkers associated with vascular disorders, regarding diagnosis, prognosis, and possible therapeutic targets [7].
Prognosis of CVD is not always easy to assess and predict. In the case of IS, prognosis improved in developed countries, due to the success of thrombolytic clinical trials and the mechanical thrombectomy (MT), namely with the extension of the therapeutic window in recent guidelines. This prevents further brain damage due to hypoperfusion during the acute stage, and possibly disrupts inflammatory pathways, decreasing mortality and morbidity [2,5]. In ICH, besides primary hemorrhagic damage, activation of inflammatory cells may contribute to a secondary neuronal damage. In CVT, coagulation and inflammatory disorders may be a potential cause of thromboembolism, besides contributing to additional damage [8]. Detecting and measuring biomarkers involved in those pathways may allow for a better prediction of prognosis of CVD.
Inflammatory pathways could theoretically be therapeutic targets against the secondary injury associated with inflammation after CVD. However, apart from vasculitis, the use of steroids failed to demonstrate a benefit in IS [2]. In the case of ICH and CVT, no studies were performed. There is a need to elucidate inflammatory pathways associated with CVD, to develop possible novel therapeutic targets.
In this study, we aimed to perform a comprehensive review of the literature regarding inflammation and stroke.
2. Materials and Methods
Studies were identified using a search strategy in two English-language databases (PubMed and Web of Science) published up to August of 2021 and in the Clinical Trials Database (ClinicalTrials.gov). Search terms used were previously selected by co-authors and included the following mesh terms: IS, ICH, CVT, inflammation and inflammatory biomarkers. Clinical Trials were also searched for ongoing or published trials. References of the selected articles were screened for additional relevant articles, including revision and animal studies to facilitate the explanation of some biochemical mechanisms.
The inclusion criteria for studies were: 1—Clinical studies in humans, 2—Reporting results on biomarkers associated with diagnosis treatment and prognosis; 3—Published in the last 5 years. The formulated exclusion criteria were: 1—non-human studies and 2—non-English-language publications.
Articles’ abstracts were reviewed by co-authors and selected on the basis of their relevance to the topic.
From a total of 439 papers included, 304 papers were excluded according to the defined criteria. Finally, 135 papers were reviewed.
The data extracted from the retrieved studies were: (1) specific research objectives; (2) type and number of stroke patients included; (3) selected inflammatory biomarkers tested; (4) main results and conclusions; (5) relationship between inflammatory biomarkers tested and diagnosis, treatment and prognostic outcomes; and (6) important limitations of the study.
All the important data were summarized in a table for easier access.
To orient the reader as to the full scope of the data included, we will briefly discuss the main inflammatory cells involved in CVD, followed by markers associated with endothelial cells and blood–brain barrier (BBB), and acute phase biomarkers and their use as diagnostic, therapeutic and prognostic markers. Finally, other less-studied biomarkers are mentioned. All inflammatory biomarkers mentioned in each section contain separate paragraphs related to the 3 main CVD, namely IS, ICH and CVT.
3. Results
3.1. Inflammatory Cells Involved in Cvd
Several studies have demonstrated the involvement of neurons, glial and vascular cells in the pathogenesis of CVD and secondary injury (Figure 1) [9,10].
3.1.1. Leukocytes
Increased leukocytes are a marker of inflammatory response [9]. Soon after IS, neutrophil concentration rises in a stroke-severity-dependent manner, undergoing conformational changes, improving endothelial adhesion, and migrating towards the ischemic site through chemokines concentration gradients [9,10]. Neutrophils are usually only seen in the ischemic cortical parenchyma 12 h after ischemia onset, remaining in the neurovascular unit and leptomeningeal spaces in the first hours. Neutrophil activation contributes to the resolution of inflammation, scar formation, and neo-angiogenesis. However, by releasing pro-inflammatory cytokines, reactive oxygen species, and proteases, they induce secondary brain injury, contributing to BBB impairment and cerebral edema [9,10]. Blood-derived macrophages are recruited into the ischemic brain tissue 3–4 h after onset. Nevertheless, during the first 24 h, the brain resident macrophages, microglia dominate the infarction region, declining and giving rise to blood-derived macrophages around day 7 [9]. T cells are detected in the infarction boundary zones early within 24 h after reperfusion, accumulating until day 7 and reducing after 14 days [10]. Both CD4+ and CD8+ lymphocytes seem to play a harmful role in the infarcted parenchyma. Nevertheless, regulatory T cells seem to have a neuroprotective effect, producing anti-inflammatory cytokines such as IL-10 and TGF-B [10]. B cells effects are mainly in the ischemic/reperfusion injury related to the production of autoantibodies. Regulatory B cells seem capable of reducing inflammation and neurological deficits in mouse models [10].
In ICH, primary brain lesion occurs in the first hours after ICH due to hematoma or edema. Polymorphonuclear activation occurs soon after ictus, contributing to secondary injury. Neutrophils are the first leukocytes to migrate to the brain in the first hours, contributing to a granular and friable tissue formation. Subsequent infiltrating leukocytes release inflammatory and cytotoxic mediators, causing an increased capillary permeability and BBB disfunction, contributing to an increased peri-lesional edema and secondary damage [11,12]. Due to the hematoma and edema expansion, mass effect and increased intracranial pressure can lead to herniation and death [11].
In CVT, venous obstruction can be complicated by venous infarction or hemorrhage. This leads to a local disruption of the BBB, causing microvascular damage, and infiltration of inflammatory cells and leukocyte adhesion [13,14]. Additionally, vasogenic edema occurs earlier in venous stroke, due to an increase in venous pressure related to the occlusion [13,15]. In an acute phase, there is a rise in neutrophil counts with lower lymphocyte, followed by a rise of monocytes in a subacute phase, and an increase of lymphocytes and neutrophil reduction in chronic phase [16].
3.1.2. Absolute Neutrophil Count and Neutrophil-to-Lymphocyte Ratio (NLR)
NLR consists of the total number of neutrophils divided by lymphocytes. It is a marker of inflammation and infection used in several fields, including in many cerebrovascular disorders [15].
Several studies have approached the role of the NLR in arterial stroke as a possible prognostic predictor [17]. Neutrophils are significantly increased in stroke patients, and are higher in dead patients, with an average specificity for mortality prediction when superior to a ratio of 4.1 [18]. High NLR predicts stroke-associated pneumonia [19]. NLR also seems to differ between different stroke treatment groups—in a pilot study, patients submitted to intravenous thrombolysis (IVT) and MT, NLR was markedly higher than in other treatment groups, which was associated with increased severity of the disease [20,21]. Additionally, NLR levels may predict outcome and treatment response—higher levels 24 h post MT associated with worse functional outcome when controlling for confounders, but not pretreatment NLR [22,23]. High NLR also predicts hemorrhagic transformation after stroke [24]. Specifically in stroke due to large vessel occlusion, high NLR correlated with early neurological deterioration, although only patients with in situ thrombosis had high NLR levels [25]. Additionally, high NLR levels at admission correlated with increased post-stroke depression [26,27]. Recently, in a cohort of 553 patients, post-reperfusion NLR was shown to be the best predictor of severe grades of cerebral edema with an area under the curve around 0.7. NLR ≥ 7 had an accuracy, sensitivity, and specificity around 60%, which is encouraging for investigators who consider the inflammatory pathways as routes to the prevention of brain secondary damage early after reperfusion therapy in stroke [28].
In ICH, higher ratios seem to be associated with larger hematoma volume at admission and hydrocephalus and are associated with a worse National Institutes of Health Stroke Scale (NIHSS) score and lower Glasgow Coma Scale (GCS) score at admission. It may also help predict worse neurological outcomes, assess risk of deterioration, and evaluate outcomes in patients submitted to surgical treatment. Regarding outcome, NLR was independently associated with 30-day poor outcome and mortality after ICH, with a study establishing 7.35 as the best predictive NLR cutoff. This association was not confirmed in relation to the 3-month outcome. However, depression at 3 months, an important comorbidity, may be related to higher NLR, suggesting that NLR may be a significant depression predictor. It is interesting to notice that NLR, as in IS, an immediate and intense systemic inflammatory response reduces the likelihood of a better functional outcome at 90 days, which is more likely to be explained by perihematomal edema growth than due to a significant hematoma expansion [29].
Data regarding NLR involvement in other cerebrovascular disorders, such as CVT, are still scarce. When compared to reference populational values, CVT patients present increased NLR [30]. Clinical studies also suggest an evolution of the neutrophil and NLR according to the temporal stage of CVT, with higher neutrophil absolute count and NLR in acute CVT, and lower NLR in the chronic stage, suggesting an earlier infiltration of neutrophils [16,31]. NLR also seems to have prognostic implications. Retrospective studies have shown a positive correlation between NLR and baseline degree of disability and NIHSS. Different studies have also shown that NLR is an independent risk factor for poor prognosis in patients with Cerebral Venous Sinus Thrombosis (CVST), significantly associated with a high risk of poor outcome at discharge and unfavorable functional outcome at 90 days, although no relation to brain lesion outcomes or recanalization was found [32,33,34]. Therapeutic data are still lacking, with only a preclinical study supporting neutropenia and neutralization of leukocyte adhesion molecules in effectively reducing blood–brain damage and brain edema [15].
3.1.3. Absolute Lymphocyte Count and Lymphocyte-to-Monocyte Ratio (LMR)
LMR is the ratio between total lymphocyte and monocyte count, and its utility as a biomarker for stroke has been explored in recent studies. In the case of infarct or hemorrhage, a local disruption of the BBB occurs, causing microvascular damage. Leukocytes may contribute to such a phenomenon; a preclinical murine study demonstrated that brain edema and BBB disruption depended on leukocyte adhesion [13].
In IS, low LMR seems to increase the risk of hemorrhagic transformation [35]. Indeed, a study showed that low LMR levels were independently correlated with stroke severity [36]. It may also help predict functional outcome after thrombolysis and MT, with lower LMR significantly associated with poor functional outcome in both treatments [23,37,38]. Low LMR also seems to be more frequent in stroke patients with concomitant infections, with stroke inducing a possible immunosuppression [39]. In a stroke cohort, decreased LMR also seems to relate to post stroke depression and its severity [40].
In ICH, leukocytes are recruited due to the production of M1 chemokines, perpetuating inflammatory response [41]. In ICH, higher white blood cells (WBC) count at admission is related to GCS score and clot volume, as well as 6-month survival, helping to identify more severe clinical pictures and prognosis. However, in a prospective study, higher admission WBC count was associated with lower risk of hematoma expansion [42]. LMR cutoffs of 2.21 and 2.19 predicted neurological deterioration and 90-day mortality, respectively [43].
In CVT, a retrospective cohort showed that LMR was higher in the chronic presentation setting [16]. Although there was no leukopenia in the acute phase, a tendency to lower lymphocyte count in the acute phase, with higher lymphocytes and decreased neutrophils in the chronic phase was observed [16]. The acute group exhibited the lowest absolute lymphocyte counts, leading investigators to hypothesize lymphocyte migration and adhesion as possible contributors. In this model, higher LMR predicted the presence of chronic CVT with high specificity and sensitivity. This last theory is supported by case–control studies, which associated lower LMR with worse clinical outcomes [32,44,45].
3.1.4. Platelet Count (PLT) and Mean Platelet Volume (MPV) and Platelet-to-Lymphocyte Ratio (PLR)
Platelet size has been demonstrated to reflect platelet activity and seems to be a useful predictive and prognostic biomarker of cardiovascular events. Increased MPV was observed in cardiovascular diseases [46]. Platelets are important for tissue remodeling after injury has been inflicted to the endothelial barrier and to the subendothelial tissue [47].
In IS, preclinical studies with mice lacking CD84 receptor on platelets or T cells, impairing activation, displayed reduced cerebral CD4+ T-cell infiltration and thrombotic activity following experimental stroke resulting in reduced neurological damage. Clinically, high platelet CD84 expression levels were associated with poor outcome in patients with stroke [48] PLR was inferior to NLR as predictor of outcome and severe neurological complications such as edema in a larger cohort study [28]. Nevertheless, in patients with stroke, namely those submitted to IVT, higher PLR was independently associated with unfavorable outcome and death at 3 months after thrombolysis, correlating with NIHSS and GCS [49,50,51,52]. Regarding psychiatric impairment, higher PLR was associated with post-stroke disorder, and depression 6 months after stroke [53].
Regarding ICH, PLR data are limited, with only a retrospective study showing high PLT levels (>100) in patients admitted to ICU correlated with worse GCS [54]. One study of 135 patients with ICH showed that higher PLR was associated with independence at 90 days although this effect was not due to significant midline shift or hematoma expansion. Again, PLR was inferior to NLR in prognostic performance [29].
In CVT, case–control studies described a reduction of PLR [55]. Another retrospective study theorized that PLR could predict in-hospital adverse events [45]. Platelet counts were also slightly higher in the acute and subacute settings when compared to chronic [16]. A 2018 case–control study did not find an increased risk of CVT with high PLR; however, they found that high PLR values increased the risk of provoked CVT and interaction with thrombophilia patients [55].
3.1.5. Systemic Immune-Inflammatory Index (SII)
The SII is an indicator composed of platelet, neutrophil, and lymphocyte counts, whose formula is: platelet counts × neutrophil counts/lymphocyte counts. It has shown possible prognostic prediction abilities in malignant tumors, coronary artery disease, and acute IS [56,57,58].
In stroke, a retrospective study showed no difference in SII values upon admission between acute IS patients with neurological recovery and acute IS patients with no improvement at 1, 3, 6, and 12 months poststroke [59]. Conversely, in patients with large artery occlusion, decreased SII was associated with favorable clinical outcomes after MT [60].
In ICH, patients with supratentorial spontaneous ICH early SII index was an independent predictor of poor outcome at time of hospital discharge [58,61]. In another study, SII was associated with 90-day functional outcome [62]. In patients submitted to IVT, an increased 24-h SII was associated with poor functional outcome [63].
In CVT, a case–control study showed that SII was an independent risk factor for poor prognosis in CVT [33]. Another 270 CVT cohort with a 22-month follow-up showed that patients with higher SII presented with lower survival rates, and a subgroup analysis demonstrated that SII was an important predictor of poor outcomes in acute/subacute CVT, especially in pregnancy/puerperium female patients [64].
3.1.6. Microglia
There are no human studies directly related to microglia biomarkers, despite their major role as resident innate immune cells of the brain [9]. Microglia are activated minutes following injury, including in IS, releasing several immunomodulatory molecules namely cytokines, chemokines, and free radicals [9,65].
In response to injury, microglia become active and differentiate into M1 or M2. Soon after IS, nuclear factor kappa-light-chain-enhancer of activated B cells (NF-kB) is activated within microglia promoting differentiation into M1 phenotype and release of proinflammatory cytokines [65]. M2 microglia are activated through upregulation of peroxisome proliferator-activated receptor Y (PPARy), following IS, promoting the release of anti-inflammatory cytokines [65]. The M1/M2 microglia phenotype changes dynamically post-injury, thought to exhibit an early beneficial M2 phenotype, followed around 7 days by a majority of a detrimental M1 phenotype [65,66]. The detrimental effects of microglia are thought to be by BBB disruption and upregulation of endothelial cell adhesion molecules promoting leukocyte infiltration [66].
In ICH, primary brain lesion occurs in the first hours after ICH due to hematoma or edema. The inflammation is firstly mediated by microglia, which are among the first non-neuronal cells activated during the innate immune response. As in IS, the development of either M1-like (proinflammatory) or alternative M2-like (anti-inflammatory) phenotypes is very well documented [41,67]. In the subacute and chronic phase (~7 days from ictus), an M2 (anti-inflammatory) phenotype develops, contributing to phagocytosis of cell debris, tissue healing, and hematoma clearance [67].
3.1.7. Interleukin (IL)
IL are substances with proinflammatory properties that modulate brain injury and can be potential therapeutic targets. Multiple IL are involved in stroke pathways.
Most studies focus on IL-6. IL-6 is an inflammatory factor produced by endothelial cells and may regulate acute phase response negatively. In IS, IL-6 levels rise in serum and cerebrospinal fluid (CSF) after injury. Elevated levels are associated with stroke severity, neurological worsening, infarct volume and clinical outcome [68]. In IS, IL-10 rs1800896 polymorphism was significantly associated with individual susceptibility to IS, especially for cerebral infarction [69]. IL-18 was higher in stroke patients than in controls, and was negatively associated with the NIHSS scale [70].
In ICH, higher IL-6 levels correlated with higher 30-day mortality, higher volume, and mass effect [71].
Other IL may have a role as possible biomarkers. In ICH, IL-10 was associated with rebleeding [72]. Additionally in ICH, CSF IL-11 levels were higher in patients with hydrocephalus occurring after ICH onset and were also associated with high mortality [73].
In CVT, IL-6 was shown to be significantly associated with an unfavorable functional outcome at 90 days, defining a cut point of 2.7 pg/mL for a specificity of 81% and sensitivity of 78% [32].
3.2. Endothelial Cells and BBB
Endothelial cells are one of the components of the neurovascular unit, having tight junction proteins that are the major interface with the blood [9]. Pericytes, which are macrophage-like cells contiguous with the basal lamina that surrounds endothelial cells, have a role in protecting the neuronal microenvironment [9]. Following IS, pericytes migrate from the basement membrane leading to BBB permeability. However, animal models have shown that 7 days after IS, pericytes accumulate in the peri-infarct area, which might support vascular repair [9]. The human studies in BBB is out of the scope of this article but human imaging studies are nicely reviewed elsewhere [74].
3.2.1. Matrix Metalloproteinase-9 (MMP-9)
MMP-9 is a gelatinase that degrades major components of the basal lamina, whose expression is upregulated after cerebral ischemia and has been associated with blood–brain disruption. Blood levels of MMP-9 correlate with disease severity and infarct volume in the hyperacute phase and late hemorrhagic infarction. MMP-9 can also be a prognostic factor for IS, as MMP-9 levels have also been associated with increased risk of mortality and major disability, and higher infarct volume. Additionally, MMP-9 predicts the development of hemorrhagic transformation in patients with IS and specifically in patients submitted to thrombolysis [75]. MMP-9 might be a potential therapeutic target. In a preclinical study, MMP-9 inhibition decreased the degree of brain edema, reduced the risk and gravity of intracerebral hemorrhage, and improved neurological outcome [76].
In ICH, although MMP-9 has shown some association with the development of aneurysms and arteriovenous malformations and with the increase risk of ICH, as a marker of unstable vasculature, in spontaneous ICH these findings have been few [77,78]. A study associated specific MMP-9 haplotypes, such as rs2250889 and haplotype 3 in younger males, as protectors of spontaneous ICH [79]. Another study identified that, in intracerebral hemorrhage induced by cerebral amyloid angiopathy, Aβ induced expression and activation of MMP-9 in cerebral vessels of amyloid precursor protein (APP) transgenic mice, and, in postmortem brain tissues of human cerebral amyloid angiopathy (CAA) cases, MMP-9 co-localized with CAA, correlated with the severity of the vascular pathology, and was detected in proximity to microbleeds, suggesting that inhibition of MMP-9 may be a potential preventive strategy for CAA-associated hemorrhage [80]. Additionally, an ICH preclinical study found that the neuropathological features of ICH such as inflammatory cell activation were reduced in MMP-9 null mice compared with wild-type controls, suggesting that MMP-9 inhibition may prevent neurotoxic actions and increased injury [81].
In CVT, a prospective case–control study found that patients with parenchymal brain lesions had higher baseline concentrations when compared to controls [32]. Additionally, patients with venous recanalization showed an early decline of circulating MMP-9 and significantly lower levels on day 8 [32]. A higher MMP-9 on day 8 was associated with persistent venous occlusion [82]. In another study, MMP-9 was not detected in the CSF of any patient [83]. Although venous parenchymal hemorrhage is commonly seen in patients with venous infarction, serum MMP-9 levels were not significantly different between patients with hemorrhagic and non-hemorrhagic lesions [82]. Although, in arterial infarction, hypoxia in ischemic regions likely increases the expression of MMP-9, in venous infarction the hypoxic state is not as significant, which may explain lower MMP-9 in this CVD.
3.2.2. Astrocytes
Astrocytes are key elements of the neurovascular unit function [65].
Following ischemia, cytokines from neurons and glial cells lead to astrocyte increased reactivity, forming a glial scar in the peri-infarct region, limiting the diffusion of neuroinflammation [9,65]. Like microglia, astrocyte proliferation follows two routes A1 a A2 reactive astrocytes. A1 reactive astrocytosis leads to the release of inflammatory factors, namely IL-6, tumor necrosis factor alfa (TNF-alfa), IL-1alfa, IL-1B and interferon gamma (IFNy) and free radicals. Post-stroke, due to failure of the Na+K+ pump, astrocytes swell, leading to increased intracranial pressure and cerebral hypoperfusion [9,66]. A2 reactive astrocytes upregulate neurotrophic factors, playing an important role in neuroprotection [9,65]. Disconnection of the astrocyte endfeet and endothelial cells is involved in BBB damage and the influx of peripheral inflammatory cells [9]. In animal models, ischemic cerebral insult induce extensive astroglial response in the lesions core from 4 h to 1 day, peaking at day 4 and persisting until 28 days after [9].
3.2.3. Calcium-Binding Proteins S100B
S100B refers to a protein characterized by its solubility in a 100% saturated solution of ammonium sulfide [84]. Intracellularly, it is a calcium-sensor protein and although involved in a variety of functions, it is still unclear what its main function is [84]. S100B has been traditionally associated with astrocyte dysfunction and a marker of BBB dysfunction [84] in various pathologies [10].
In IS, serum levels of S100B are increased 8–10 h after symptom onset, reaching a peak at 72 h and dropping at 96 h, and although studies failed to demonstrate its role as a diagnostic marker, it showed potential as a predictor of hemorrhagic transformation and long-term functional outcome [10,85]. Indeed, a few studies in IS patients demonstrated a correlation between infarct size, but not stroke severity and levels of serum S100B on the 3rd day after stroke [86,87]. Nevertheless, levels measured at 8 h after onset showed no correlation with the functional outcome, implying the possible use of S100B as a prognostic but not diagnostic marker in acute IS patients [88]. Levels of S100B have also been shown to be increased in patients with transient ischemic attacks (TIA) and intracerebral hemorrhage when compared with patients with IS or healthy controls, potentially being able to discriminate IS from TIA and ICH [88,89,90].
In CVT, S100B was undetectable in the serum of most patients, except for two patients with large-volume venous infarcts and brain herniation—however, no CSF levels were measured [83]. In ICH, S100B levels on admission were negatively correlated with GCS values and positively correlated with bleeding volume and NIHSS in the patient group, acting as a potential biomarker for severity of brain injury after poor prognosis [91].
Regarding S100A, in ICH, concentrations increased compared to control subjects and also correlated with NIHSS score, ICH volume, blood glucose concentrations [91]. Additionally, Serum S100A12 concentrations significantly discriminated patients at risk of 30-day mortality and its predictive value was equivalent to those of NIHSS score and hematoma volume [91]. Moreover, higher serum S100A12 concentrations showed a significantly higher risk for 30-day mortality and overall survival, blood WBC count and plasma C-reactive protein (CRP) concentrations [91].
3.3. Acute Phase Biomarkers
3.3.1. C-Reactive Protein (CRP)
CRP is a protein synthesized in the liver in response to IL-6 secretion by macrophages and T-cells [92]. High sensitivity CRP (Hs-CRP) is more sensitive and can more accurately detect low-grade inflammation. It correlates with cardiovascular risk in the general population and is an inflammatory biomarker frequently associated with all stages of IS [93,94].
CRP has been shown to be associated with an increased risk of all-cause mortality in patients with acute IS, predicts further ischemic events in patients with transient ischemic attack, lacunar stroke or IS in general [93,94,95]. Nevertheless, an increase of CRP occurs in IS but also in several other inflammatory conditions, reflecting its poor specificity and sensitivity [10]. CRP is probably more informative with respect to acute indolent inflammatory status that very acute changes in stroke.
In the case of ICH, CRP levels correlate with outcome [96]. CRP levels in the short follow-up (between 3rd and 7th day) were higher among patients with poor outcomes (NIHSS > 15) and associated with larger ICH volume [96]. Additionally, a prospective study showed a correlation between higher CRP and higher mortality, aiding in mortality prediction when added to the ICH score [96].
In CVT, the evidence shows that CVT patients have higher CRP levels than controls and that hs-CRP levels are higher in the acute and subacute stage of CVT, decreasing in the chronic stage, which can support acute CVT diagnosis [16,97]. CVT clinical syndrome and prognosis are also connected to CRP. In a study, hs-CRP level was positively correlated with the baseline occurrence of seizure in CVT [97]. Priority-CVT, a multicenter prospective cohort of recently diagnosed CVT, however, did not show a relation between CRP levels and brain lesion outcomes or recanalization [32]. Regarding outcome, increased CRP baseline concentrations had a significant association with the unfavorable functional outcome at 90 days [32]. A cutoff of 3.3 mg/dL had low sensitivity (0.5) but high specificity (0.9) when predicting unfavorable outcome at 90 days [32].
3.3.2. Procalcitonin (PCT)
PCT is a prohormone of calcitonin and is produced by C-cells and the thyroid gland [98]. Overall, there have been fewer studies than those on other biomarkers like CRP, reflecting its less frequent use in current practice.
PCT has been demonstrated to be elevated after first-ever acute IS and is an independent risk factor for stroke [98]. It has also been shown to be a prognostic marker both for mortality in 30 days and for functional outcome after IS in a Chinese population [99].
In ICH, serum PCT correlate with outcome, with higher PCR levels at admission being independently associated with unfavorable clinical outcome [100]. Another study combined albumin and PCT to uncover a ratio, where albumin/PCT ratio could be an additional diagnostic predictor for nosocomial infection in patients with ICH [101]. The role of PCT in CVT has not been investigated.
3.3.3. D-Dimers
3.3.4. Erythrocyte Sedimentation Rate (ESR)
ESR is another acute-phase inflammatory biomarker.
In IS, an association of ESR has been linked more to chronic atherosclerosis and marker of more severe carotid atherosclerosis [105,106,107]. In the acute stage, higher ESR might be linked to early ischemic changes in computed tomography (CT) of IS patients at admission [108,109]. Another study found that high ESR levels were significantly correlated with higher in-hospital death rate and/or poor condition at discharge [110].
In ICH, this biomarker has not been explored.
3.3.5. Iron, Ferritin Levels and Erythropoietin (EPO)
Iron has an important role in several processes, including erythropoiesis. EPO is a cytokine mediating erythropoiesis Ferritin, besides its importance in iron absorption, and additionally intervenes as an acute inflammatory biomarker, and can be activated in several disorders.
In IS, higher iron status was associated with increased stroke risk and, in particular, cardioembolic stroke [111]. Ferritin reduction is related to cerebral ischemia-induced hippocampal ferroptosis [112]. A study found that increased serum ferritin levels correlate with severity of stroke and size of the lesion [113,114]. Additionally, elevated serum ferritin levels at admission were associated with post-stroke depression [115].
In a preclinical ICH study, ICH + EPO showed better functional recovery with a lower hemorrhage volume [116]. In this study, treatment with EPO increased endothelial nitric oxide synthase (eNOS), among other substances [116]. There might be a therapeutic role for EPO, inducing a better functional recovery with reducing perihematomal inflammation and apoptosis. The ICH Score and NIHSS were correlated with high ferritin levels measured at 7 days post ictus [117]. This could explain the worse functional outcome.
In CVT, the role of ferritin has not been explored.
3.3.6. Other Acute Phase Biomarkers
Several other biomarkers have been explored, on a smaller scale, and not systematically in all disorders.
Neutrophil gelatinase-associated lipocalin (NGAL) is an acute-phase protein and is implicated in acute brain injury. A case–control study in ICH showed that patients had significantly raised serum NGAL levels, correlating with blood glucose levels, GCS score, NIHSS score, ICH score, and ICH volume, and predicting an unfavorable outcome at 90 days, intimately correlating with a worse prognosis [118]. Substance P (SP) is also involved in brain inflammation. In a 106 ICH patient study, poor outcome patients had higher serum SP concentrations, with serum SP concentrations > 449 pg/mL predicting poor outcome with 63.0% sensitivity and 78.9% specificity, suggesting that serum SP could be an inflammatory prognostic factor for ICH [119].
3.4. Oxidative Stress Biomarkers
There is already evidence of oxidative stress having a major role in the pathogenesis of ischemic and reperfusion-related injury mediated through free radicals and lipide peroxidation [120].
To assess oxidative stress in the plasma, usual biomarkers include the accumulation of malondialdehyde (MDA), an end-product of peroxidative decomposition of polyenoic fatty acids in the lipid peroxidation process, measured as thiobarbituric acid-reactive substances (TBARS) [121].
TBARS and MDA have been identified as predictors of poor neurological outcomes; however, they lack the specificity needed for an IS biomarker, not allowing its distinction from their easily confounding mimickers [10].
F2-isoprostanes (F2-isoPs) are products of noncyclooxygenase free radical-induced neuronal arachidonic acid peroxidation of membrane phospholipids and lipoproteins capable of being detected in human plasma, urine and CSF [120]. Plasma levels increase in the first 8 h after IS but not at 24 h, indicating a possible oxidative stress mechanism in the hyperacute phase of IS, potentially before irreversible damage [120]. Indeed, it has been demonstrated that plasma levels of F2-isoPs are independent molecular predictors of radiographic evidence of ischemic penumbra in patients with acute IS evaluated within 9 h of symptom onset [120].
Several oxidative biomarkers have been researched.
Heart-type fatty acid-binding protein (H-FABP) is a small cytoplasmatic protein (15 kDa) that is involved in active fatty acid metabolism where it transport fatty acids from cell membrane to mitochondria for oxidation [122]. H-FABP is mainly present in the myocardium and neuronal cell body in the central nervous system (CNS), being released from tissue to peripheral blood following the ischemic event and myocardial infarction [122]. H-FABP is increased during the acute phase (<24 h) after IS, correlating with clinical severity and long-term follow-up; however, its clinical applicability is not yet recommended [10,122,123]. H-FABP has not been explored in CVT or ICH.
Damage-associated molecular patterns (DAMPs) appear critical for the promotion of altered BBB permeability, leukocytes infiltration, tissue edema, and brain injury [124]. They are released after ischemic lesion, activating different pathways including toll-like receptors (TLR) and inflammasomes, thus exacerbating ischemic damage [124].
Leptin and adiponectin (APN) mediate proatherogenic and antiatherogenic responses, respectively, and hence, determining the plasma or serum levels of leptin and adiponectin alone or in combination may act as a novel prognostic biomarker for inflammation and atherosclerosis in stroke [125]. APN has also been shown to be a crucial mediator of acute cerebral ischemia [125]. Serum leptin is associated with first-ever acute IS, lesion size, and stroke severity in a Chinese cohort [125].
Plasma total homocysteine (tHcy) is an independent risk factor for vascular disorders, with several studies demonstrating a deleterious effect of Hcy in the vascular system. It has not been explored in stroke or ICH. In CVT, a case–control study showed that fasting plasma tHcy, S-adenosylhomocysteine, and S-adenosylmethionine were significantly higher in CVT patients, with elevated S-adenosylhomocysteine having a higher sensitivity and specificity as risk predictor [126].
3.5. Immunoglobulin A (IgA), Immunoglobulin M (IgM), and Immunoglobulin G (IgG)
In IS and ICH, a study identified a transient IgG reduction in patients with substantial ischemic or hemorrhagic brain injuries, with subsequent increase in infections [127]. In CVT, a case–control study had a positive relation between CSF IgM and baseline degree of disability, while baseline CSF IgA (r = 0.615, p < 0.001), CSF IgM (r = 0.752, p < 0.001), and CSF IgG (r = 0.248, p = 0.015) levels were positively associated with NIHSS, a significant correlation between inflammation and CVT severity [97]. Ig A, IgM, and IgG CSF levels were also higher in the acute and subacute phases, indicating a variation in the degree of inflammation during the course of the disease [97].
3.6. Treatment and Ongoing Trials
3.6.1. Uric Acid, NCT00860366
To target oxidative damage, the use of oxidative stress scavengers has been studied. URICOICTUS, NCT00860366, a phase 2b/3 trial confirmed the safety of the combination of uric acid and alteplase (started within 4.5 h of symptom onset) in patients with acute IS.
Although no difference in functional outcome was seen, uric acid did reduce the incidence of early clinical worsening, and more patients treated with uric acid obtained full independence at follow-up than those who received placebo [128]. Other clinical trials looked at different antioxidant drugs, such as edaravone, but evidence in its efficacy is not consistent [129,130].
3.6.2. Edaravone and D-Borneol, NCT04950920
Phase III Clinical Trial of Y-2 Sublingual Tablets in the Treatment of Acute Ischemic Stroke. Edaravone is a free radical scavenger and inflammatory protein expression inhibitor [131]. It can clear hydroxyl free radical (COH), nitric oxide free radical (no) and peroxynitrite ion (onoa), and inhibit the expression of tumor necrosis factor-A (TNF-a), interleukin IP (IL-1 (3), cyclooxygenase-2 (COX-2) and inducible nitric oxide synthase (iNOS) and other inflammatory related proteins induced by cerebral ischemia [131]. By clearing the excessive free radicals produced in the brain tissue during ischemia and reperfusion and inhibiting the secondary inflammatory reaction, we can reduce the damage of free radicals and inflammatory reaction to the brain tissue [131].
3.6.3. Butylphthalide, NCT03539445
3.6.4. Vinpocetine, NCT02878772
In a multi-center study (NCT02878772), 60 patients with anterior cerebral circulation occlusion and onset of stroke that had exceeded 4.5 h but lasted less than 48 h were recruited [133]. Vinpocetine treatment associated with serum markers of NF-kB inhibition. Compared to controls, patients treated with vinpocetine had a better recovery of neurological function and improved clinical outcomes during the acute phase and at 3-month follow-up [133].
3.6.5. ApTOLL, NCT04734548
ApTOLL is a Toll-like receptor 4 (TLR4) antagonist, a receptor that is involved in innate immune responses, but also responds to tissue damage, and is therefore directly involved in a large number of diseases in which the inflammatory response is involved [134]. ApTOLL has demonstrated specific binding to human TLR4 as well as a TLR4 antagonistic effect, reducing inflammation and improving outcome after different disease models [134]. This is a multicenter Phase 1/2 trial registration of ApTOLL together with endovascular therapy in acute IS patients with confirmed Large Vessel Occlusion (LVO) who are candidates to receive reperfusion therapies including endovascular treatment with or without iv rt-PA (recombinant tissue Plasminogen Activator) studying safety and efficacy [134].
3.6.6. Colchicine, NCT02898610
Colchicine for Prevention of Vascular Inflammation in Non-Cardio Embolic Stroke (CONVINCE), NCT02898610, is a phase 3 trial that evaluates the use of colchicine in patients who have suffered an ischemic stroke or transient ischemic attack not caused by cardiac embolism or other defined causes [135]. Patients will be randomized to 0.5 mg/day of Colchicine plus usual care, or to usual care alone. Primary targets are stroke recurrence, but secondary analysis will be performed to evaluate functional outcome at 3 months, which might give clues about anti-inflammatory effects in patients randomized in the first days [135].
3.6.7. Fingolimod, NCT04629872
For inflammation, fingolimod, an agonist of sphingosine-1-phosphate receptors, used on multiple sclerosis, that prevents the egress of lymphocytes from lymph nodes, was studied in stroke. Preclinical studies using several rodent models of brain ischemia showed that fingolimod can reduce infarct size, neurological deficit, edema, and the number of dying cells in the core and peri-infarct area [136]. Currently, a phase 2 trial is ongoing, to assess a possible role for fingolimod in attenuating brain inflammation and improving clinical outcomes in patients with acute IS, and also if fingolimod enhances the action of endovascular therapy [137]. In ICH, a pilot trial is also evaluating fingolimod in patients with primary spontaneous intracerebral hemorrhage, as a treatment for cerebral edema [138].
3.6.8. Natalizumab
3.6.9. Rapamycin
In ICH, there are some studies focusing on neuroprotective effects through microglia phenotype modelling. Low dose rapamycin increased levels of anti-inflammatory cytokines (il10 and TGFbeta) [141]. Sinomenine, a dextrorotatorymorphinan analogue used clinically for treating rheumatoid arthritis in China, was shown to reduce levels of proinflammatory cytokines IL-1β, IL-6 and TNF in ICH-exposed BV-2 microglia198 and increased levels of M2-like markers IL-10 and Arg1 in primary microglia exposed to erythrocyte lysate, in vitro and in mice [142,143].
3.6.10. Interferon ~Beta-1, NCT00097318
Safety Study of Interferon Beta 1a to for Acute Stroke, NCT00097318, was finished but results not published [144].
3.6.11. Canakinumab
Anti-inflammatory Therapy with Canakinumab for Atherosclerotic Disease.
A randomized, double-blind trial of canakinumab, a therapeutic monoclonal antibody targeting interleukin-1β, involving 10,061 patients with previous myocardial infarction and hs-CRP level of 2 mg or more per liter was conducted [145]. The trial compared three doses of canakinumab (50 mg, 150 mg, and 300 mg, administered subcutaneously every 3 months) with placebo [145]. The primary efficacy end point was nonfatal myocardial infarction, nonfatal stroke, or cardiovascular death [145]. Stroke recurrence was reduced but not significantly (p = 0.17) [145]. Functional outcome was not assessed.
3.6.12. Anakinra, NCT03737344
Phase 2 trial Phase II Trial of Interleukin-1 Receptor Antagonist in Intracerebral Hemorrhage: BLOcking the Cytokine IL-1 in ICH to reduce edema at 72 h is not recruiting yet [146].
In CVT, a possible role for immunosuppression as a therapeutical agent has not been yet studied.
4. Conclusions
Multiple inflammatory biomarkers appear to be involved in IS, ICH, and CVT (Table 1). Blood inflammatory cells, easily measured and accessible at admission, are potential diagnostic tools in CVD. However, their role in inflammatory pathways leading to added secondary injury also make them great prognostic markers. The combination of several biomarkers related to their time of activation may in the future become the diagnostic and prognostic tools needed for the next step in CVD. Although not yet a reality, there is increasing evidence supporting the notion that these may become potential therapeutic targets, likely influencing, or mitigating complications of CVD and improving prognosis. Nevertheless, further larger, well-designed randomized clinical trials are still needed to follow-up this hypothesis.
Author Contributions
Conceptualization, R.A.D., P.C.; methodology, R.A.D., L.D.; validation, R.A.D., L.D., P.C., E.A.; investigation, R.A.D., L.D., P.C.; writing—original draft preparation, R.A.D., L.D.; writing—review and editing, R.A.D., P.C., E.A.; supervision, E.A., P.C.; project administration, R.A.D., P.C.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Krishnamurthi, R.V.; Ikeda, T.; Feigin, V.L. Global, Regional and Country-Specific Burden of Ischaemic Stroke, Intracerebral Haemorrhage and Subarachnoid Haemorrhage: A Systematic Analysis of the Global Burden of Disease Study 2017. Neuroepidemiology 2020, 54, 171–179. [Google Scholar] [CrossRef]
- Shekhar, S.; Cunningham, M.W.; Pabbidi, M.R.; Wang, S.; Booz, G.W.; Fan, F. Targeting vascular inflammation in ischemic stroke: Recent developments on novel immunomodulatory approaches. Eur. J. Pharmacol. 2018, 833, 531–544. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.; Biller, J. Recent advances in spontaneous intracerebral hemorrhage. F1000Research 2019, 8, 302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silvis, S.M.; de Sousa, D.A.; Ferro, J.M.; Coutinho, J.M. Cerebral venous thrombosis. Nat. Rev. Neurol. 2017, 13, 555–565. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [CrossRef] [PubMed]
- McGurgan, I.J.; Ziai, W.C.; Werring, D.J.; Salman, R.A.-S.; Parry-Jones, A.R. Acute intracerebral haemorrhage: Diagnosis and management. Pr. Neurol. 2021, 21, 128–136. [Google Scholar] [CrossRef]
- Tamhane, U.U.; Aneja, S.; Montgomery, D.; Rogers, E.-K.; Eagle, K.A.; Gurm, H.S. Association Between Admission Neutrophil to Lymphocyte Ratio and Outcomes in Patients with Acute Coronary Syndrome. Am. J. Cardiol. 2008, 102, 653–657. [Google Scholar] [CrossRef]
- Aronowski, J.; Zhao, X. Molecular Pathophysiology of Cerebral Hemorrhage. Stroke 2011, 42, 1781–1786. [Google Scholar] [CrossRef]
- Jayaraj, R.L.; Azimullah, S.; Beiram, R.; Jalal, F.Y.; Rosenberg, G.A. Neuroinflammation: Friend and foe for ischemic stroke. J. Neuroinflamm. 2019, 16, 142. [Google Scholar] [CrossRef] [Green Version]
- Bonaventura, A.; Liberale, L.; Vecchié, A.; Casula, M.; Carbone, F.; Dallegri, F.; Montecucco, F. Update on Inflammatory Biomarkers and Treatments in Ischemic Stroke. Int. J. Mol. Sci. 2016, 17, 1967. [Google Scholar] [CrossRef]
- Wang, J.; Doré, S. Inflammation after Intracerebral Hemorrhage. Br. J. Pharmacol. 2007, 27, 894–908. [Google Scholar] [CrossRef] [Green Version]
- Mracsko, E.; Javidi, E.; Na, S.-Y.; Kahn, A.; Liesz, A.; Veltkamp, R. Leukocyte Invasion of the Brain After Experimental Intracerebral Hemorrhage in Mice. Stroke 2014, 45, 2107–2114. [Google Scholar] [CrossRef] [Green Version]
- Vosko, M.R.; Friedl, B.; Kloss, C.U.A.; Hamann, G.F. Microvascular damage following experimental sinus-vein thrombosis in rats. Acta Neuropathol. 2003, 106, 501–505. [Google Scholar] [CrossRef]
- Nagai, M.; Terao, S.; Yilmaz, G.; Yilmaz, C.E.; Esmon, C.T.; Watanabe, E.; Granger, D.N. Roles of Inflammation and the Activated Protein C Pathway in the Brain Edema Associated With Cerebral Venous Sinus Thrombosis. Stroke 2010, 41, 147–152. [Google Scholar] [CrossRef]
- Gotoh, M.; Ohmoto, T.; Kuyama, H. Experimental study of venous circulatory disturbance by dural sinus occlusion. Acta Neurochir. 1993, 124, 120–126. [Google Scholar] [CrossRef]
- Dias, L.; Pinto, M.J.; Castro, P.; Carvalho, M. Inflammatory Biomarkers Correlate with Time Evolution in Cerebral Venous Thrombosis. J. Stroke Cerebrovasc. Dis. 2021, 30, 105844. [Google Scholar] [CrossRef] [PubMed]
- Tokgoz, S.; Kayrak, M.; Akpinar, Z.; Seyithanoğlu, A.; Güney, F.; Yürüten, B. Neutrophil Lymphocyte Ratio as a Predictor of Stroke. J. Stroke Cerebrovasc. Dis. 2013, 22, 1169–1174. [Google Scholar] [CrossRef] [PubMed]
- Celikbilek, A.; Ismailogullari, S.; Zararsiz, G. Neutrophil to Lymphocyte Ratio Predicts Poor Prognosis in Ischemic Cerebrovascular Disease. J. Clin. Lab. Anal. 2014, 28, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Nam, K.-W.; Kim, T.J.; Lee, J.S.; Kwon, H.-M.; Lee, Y.-S.; Ko, S.-B.; Yoon, B.-W. High Neutrophil-to-Lymphocyte Ratio Predicts Stroke-Associated Pneumonia. Stroke 2018, 49, 1886–1892. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Arima, H.; Bertmar, C.; Clarke, S.; Herkes, G.; Krause, M. Neutrophil to lymphocyte ratio and early clinical outcomes in patients with acute ischemic stroke. J. Neurol. Sci. 2018, 387, 115–118. [Google Scholar] [CrossRef]
- Pektezel, M.Y.; Yilmaz, E.; Arsava, E.M.; Topcuoglu, M.A. Neutrophil-to-Lymphocyte Ratio and Response to Intravenous Thrombolysis in Patients with Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 1853–1859. [Google Scholar] [CrossRef] [PubMed]
- Kömürcü, H.F.; Gözke, E.; Ak, P.D.; Aslan, I.K.; Salt, I.; Bi, Ç.I.Ö. Changes in neutrophil, lymphocyte, platelet ratios and their relationship with NIHSS after rtPA and/or thrombectomy in ischemic stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 105004. [Google Scholar] [CrossRef] [PubMed]
- Lux, D.; Alakbarzade, V.; Bridge, L.; Clark, C.; Clarke, B.; Zhang, L.; Khan, U.; Pereira, A.C. The association of neutrophil-lymphocyte ratio and lymphocyte-monocyte ratio with 3-month clinical outcome after mechanical thrombectomy following stroke. J. Neuroinflamm. 2020, 17, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Wu, X.; Hu, W.; Zhao, L.; Zhao, S.; Zhang, J.; Chu, Z.; Xu, Y. Neutrophil-to-lymphocyte ratio predicts hemorrhagic transformation in ischemic stroke: A meta-analysis. Brain Behav. 2019, 9, e01382. [Google Scholar] [CrossRef]
- Goyal, N.; Tsivgoulis, G.; Chang, J.J.; Malhotra, K.; Pandhi, A.; Ishfaq, M.F.; Alsbrook, D.; Arthur, A.S.; Elijovich, L.; Alexandrov, A.V. Admission Neutrophil-to-Lymphocyte Ratio as a Prognostic Biomarker of Outcomes in Large Vessel Occlusion Strokes. Stroke 2018, 49, 1985–1987. [Google Scholar] [CrossRef]
- Chen, H.; Luan, X.; Zhao, K.; Qiu, H.; Liu, Y.; Tu, X.; Tang, W.; He, J. The association between neutrophil-to-lymphocyte ratio and post-stroke depression. Clin. Chim. Acta 2018, 486, 298–302. [Google Scholar] [CrossRef]
- Hu, J.; Zhou, W.; Zhou, Z.; Han, J.; Dong, W. Elevated neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios predict post-stroke depression with acute ischemic stroke. Exp. Ther. Med. 2020, 19, 2497–2504. [Google Scholar] [CrossRef] [Green Version]
- Ferro, D.; Matias, M.; Neto, J.; Dias, R.; Moreira, G.; Petersen, N.; Azevedo, E.; Castro, P. Neutrophil-to-Lymphocyte Ratio Predicts Cerebral Edema and Clinical Worsening Early after Reperfusion Therapy in Stroke. Stroke 2021, 52, 859–867. [Google Scholar] [CrossRef]
- Fonseca, S.; Costa, F.; Seabra, M.; Dias, R.; Soares, A.; Dias, C.; Azevedo, E.; Castro, P. Systemic inflammation status at admission affects the outcome of intracerebral hemorrhage by increasing perihematomal edema but not the hematoma growth. Acta Neurol. 2021, 121, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Fest, J.; Ruiter, R.; Ikram, M.A.; Voortman, T.; Van Eijck, C.H.J.; Stricker, B.H. Reference values for white blood-cell-based inflammatory markers in the Rotterdam Study: A population-based prospective cohort study. Sci. Rep. 2018, 8, 1–7. [Google Scholar] [CrossRef]
- Tekesin, A.; Tunç, A. Inflammatory markers are beneficial in the early stages of cerebral venous thrombosis. Arq. Neuro-Psiquiatria 2019, 77, 101–105. [Google Scholar] [CrossRef] [PubMed]
- De Sousa, D.A.; Pereira-Santos, M.C.; Serra-Caetano, A.; Neto, L.L.; Sousa, A.L.; Gabriel, D.; Correia, M.; Gil-Gouveia, R.; Oliveira, R.; Penas, S.; et al. Blood biomarkers associated with inflammation predict poor prognosis in cerebral venous thrombosis. Eur. J. Neurol. 2021, 28, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Karahan, S.Z.; Gazioglu, S.; Dilaver, I.; Boz, C. The Role of Thrombo-Inflammatory Biomarkers in the Prognosis of Cerebral Venous Sinus Thrombosis. Curr. Neurovascular Res. 2021, 18, 1. [Google Scholar] [CrossRef]
- Zhao, J.; Liu, K.; Li, S.; Gao, Y.; Zhao, L.; Liu, H.; Fang, H.; Song, B.; Xu, Y. Neutrophil-to-lymphocyte ratio predicts the outcome of cerebral venous thrombosis. Curr. Neurovascular Res. 2021, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Song, Q.; Pan, R.; Jin, Y.; Wang, Y.; Cheng, Y.; Liu, J.; Wu, B.; Liu, M. Lymphocyte-to-monocyte ratio and risk of hemorrhagic transformation in patients with acute ischemic stroke. Neurol. Sci. 2020, 41, 2511–2520. [Google Scholar] [CrossRef]
- Ren, H.; Liu, X.; Wang, L.; Gao, Y. Lymphocyte-to-Monocyte Ratio: A Novel Predictor of the Prognosis of Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2017, 26, 2595–2602. [Google Scholar] [CrossRef] [Green Version]
- Ren, H.; Han, L.; Liu, H.; Wang, L.; Liu, X.; Gao, Y. Decreased Lymphocyte-to-Monocyte Ratio Predicts Poor Prognosis of Acute Ischemic Stroke Treated with Thrombolysis. Med. Sci. Monit. 2017, 23, 5826–5833. [Google Scholar] [CrossRef] [Green Version]
- Świtońska, M.; Słomka, A.; Korbal, P.; Piekuś-Słomka, N.; Sinkiewicz, W.; Sokal, P.; Żekanowska, E. Association of Neutrophil-to-Lymphocyte Ratio and Lymphocyte-to-Monocyte Ratio with Treatment Modalities of Acute Ischaemic Stroke: A Pilot Study. Medicina 2019, 55, 342. [Google Scholar] [CrossRef] [Green Version]
- Cheng, H.-R.; Song, J.-Y.; Zhang, Y.-N.; Chen, Y.-B.; Lin, G.-Q.; Huang, G.-Q.; He, J.-C.; Wang, Z. High Monocyte-to-Lymphocyte Ratio Is Associated with Stroke-Associated Pneumonia. Front. Neurol. 2020, 11, 575809. [Google Scholar] [CrossRef]
- Wijeratne, T.; Sales, C. Understanding Why Post-Stroke Depression May Be the Norm Rather Than the Exception: The Anatomical and Neuroinflammatory Correlates of Post-Stroke Depression. J. Clin. Med. 2021, 10, 1674. [Google Scholar] [CrossRef] [PubMed]
- Tschoe, C.; Bushnell, C.D.; Duncan, P.W.; Alexander-Miller, M.A.; Wolfe, S.Q. Neuroinflammation after Intracerebral Hemorrhage and Potential Therapeutic Targets. J. Stroke 2020, 22, 29–46. [Google Scholar] [CrossRef] [Green Version]
- Morotti, A.; Phuah, C.-L.; Anderson, C.D.; Jessel, M.J.; Schwab, K.; Ayres, A.M.; Pezzini, A.; Padovani, A.; Gurol, E.; Viswanathan, A.; et al. Leukocyte Count and Intracerebral Hemorrhage Expansion. Stroke 2016, 47, 1473–1478. [Google Scholar] [CrossRef] [Green Version]
- Qi, H.; Wang, D.; Deng, X.; Pang, X. Lymphocyte-to-Monocyte Ratio Is an Independent Predictor for Neurological Deterioration and 90-Day Mortality in Spontaneous Intracerebral Hemorrhage. Med. Sci. Monit. 2018, 24, 9282–9291. [Google Scholar] [CrossRef]
- Li, S.; Liu, K.; Zhang, R.; Gao, Y.; Fang, H.; Liu, X.; Pei, L.; Chou, L.-Y.R.; Guan, S.; Guo, X.; et al. Lower lymphocyte to monocyte ratio is a potential predictor of poor outcome in patients with cerebral venous sinus thrombosis. Stroke Vasc. Neurol. 2018, 4, 148–153. [Google Scholar] [CrossRef] [Green Version]
- Akboga, Y.E.; Bektas, H.; Anlar, O. Usefulness of platelet to lymphocyte and neutrophil to lymphocyte ratios in predicting the presence of cerebral venous sinus thrombosis and in-hospital major adverse cerebral events. J. Neurol. Sci. 2017, 380, 226–229. [Google Scholar] [CrossRef]
- Korniluk, A.; Koper-Lenkiewicz, O.M.; Kamińska, J.; Kemona, H.; Dymicka-Piekarska, V. Mean Platelet Volume (MPV): New Perspectives for an Old Marker in the Course and Prognosis of Inflammatory Conditions. Mediat. Inflamm. 2019, 2019, 1–14. [Google Scholar] [CrossRef]
- Mezger, M.; Nording, H.; Sauter, R.; Graf, T.; Heim, C.; Von Bubnoff, N.; Ensminger, S.M.; Langer, H.F. Platelets and Immune Responses during Thromboinflammation. Front. Immunol. 2019, 10, 1731. [Google Scholar] [CrossRef] [PubMed]
- Schuhmann, M.K.; Stoll, G.; Bieber, M.; Vögtle, T.; Hofmann, S.; Klaus, V.; Kraft, P.; Seyhan, M.; Kollikowski, A.M.; Papp, L.; et al. CD84 Links T Cell and Platelet Activity in Cerebral Thrombo-Inflammation in Acute Stroke. Circ. Res. 2020, 127, 1023–1035. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.-H.; He, X.-W.; Li, Q.; Liu, J.-R.; Zhuang, M.-T.; Huang, F.-F.; Bao, G.-S. Higher Platelet-to-Lymphocyte Ratio Is Associated with Worse Outcomes after Intravenous Thrombolysis in Acute Ischaemic Stroke. Front. Neurol. 2019, 10, 1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Yang, P.; Wang, J. Peripheral Blood Platelet to Lymphocyte Ratio as Potential Diagnostic and Prognostic Markers of Acute Cerebral Infarction and its Clinical Significance. Clin. Lab. 2019, 65. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Gu, L.; Chen, L.; Hu, W.; Feng, X.; Qiu, F.; Fan, Z.; Chen, Q.; Qiu, J.; Shao, B. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio as Potential Predictors of Prognosis in Acute Ischemic Stroke. Front. Neurol. 2021, 11, 525621. [Google Scholar] [CrossRef]
- Sharma, D.; Gandhi, N. Role of Platelet to Lymphocyte Ratio (PLR) and its Correlation with NIHSS (National Institute of Health Stroke Scale) for Prediction of Severity in Patients of Acute Ischemic Stroke. J. Assoc. Physicians India 2021, 69, 56–60. [Google Scholar] [PubMed]
- Huang, G.; Chen, H.; Wang, Q.; Hong, X.; Hu, P.; Xiao, M.; Shu, M.; He, J. High platelet-to-lymphocyte ratio are associated with post-stroke depression. J. Affect. Disord. 2019, 246, 105–111. [Google Scholar] [CrossRef]
- Zhang, W.; Shen, Y. Platelet-to-Lymphocyte Ratio as a New Predictive Index of Neurological Outcomes in Patients with Acute Intracranial Hemorrhage: A Retrospective Study. Med. Sci. Monit. 2018, 24, 4413–4420. [Google Scholar] [CrossRef] [PubMed]
- Artoni, A.; Abbattista, M.; Bucciarelli, P.; Gianniello, F.; Scalambrino, E.; Pappalardo, E.; Peyvandi, F.; Martinelli, I. Platelet to Lymphocyte Ratio and Neutrophil to Lymphocyte Ratio as Risk Factors for Venous Thrombosis. Clin. Appl. Thromb. 2017, 24, 808–814. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Tian, W.; Zhao, F.; Li, M.; Ye, Q.; Wei, Y.; Li, T.; Xie, K. Systemic immune-inflammation index, SII, for prognosis of elderly patients with newly diagnosed tumors. Oncotarget 2018, 9, 35293–35299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, G.; Zhang, Y.; Xiao, R.; Zhang, T.; Gong, B. Systemic immune-inflammation index as a promising predictor of mortality in patients with acute coronary syndrome: A real-world study. J. Int. Med. Res. 2021, 49, 3000605211016274. [Google Scholar] [CrossRef] [PubMed]
- Hou, D.; Wang, C.; Luo, Y.; Ye, X.; Han, X.; Feng, Y.; Zhong, P.; Wu, D. Systemic immune-inflammation index (SII) but not platelet-albumin-bilirubin (PALBI) grade is associated with severity of acute ischemic stroke (AIS). Int. J. Neurosci. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Li, L.-H.; Chen, C.-T.; Chang, Y.-C.; Chen, Y.-J.; Lee, I.-H.; How, C.-K. Prognostic role of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and systemic immune inflammation index in acute ischemic stroke. Medicine 2021, 100, e26354. [Google Scholar] [CrossRef] [PubMed]
- Yi, H.J.; Sung, J.H.; Lee, D.H. Systemic Inflammation Response Index and Systemic Immune-Inflammation Index Are Associated with Clinical Outcomes in Patients Treated with Mechanical Thrombectomy for Large Artery Occlusion. World Neurosurg. 2021, 153, e282–e289. [Google Scholar] [CrossRef]
- Trifan, G.; Testai, F.D. Systemic Immune-Inflammation (SII) index predicts poor outcome after spontaneous supratentorial intracerebral hemorrhage. J. Stroke Cerebrovasc. Dis. 2020, 29, 105057. [Google Scholar] [CrossRef]
- Li, Y.; Wen, D.; Cui, W.; Chen, Y.; Zhang, F.; Yuan, M.; Xiao, H.; Li, H.; Ma, L.; Hu, X.; et al. The Prognostic Value of the Acute Phase Systemic Immune–Inflammation Index in Patients with Intracerebral Hemorrhage. Front. Neurol. 2021, 12, 628557. [Google Scholar] [CrossRef]
- Topcuoglu, M.A.; Pektezel, M.Y.; Yilmaz, E.; Arsava, E.M. Systemic Inflammation Indices in Patients with Acute Ischemic Stroke Treated with Intravenous Tissue Plasminogen Activator: Clinical Yield and Utility. Angiology 2021, 72, 279–284. [Google Scholar] [CrossRef]
- Li, S.; Liu, K.; Gao, Y.; Zhao, L.; Zhang, R.; Fang, H.; Tao, Y.; Liu, H.; Zhao, J.; Xia, Z.; et al. Prognostic value of systemic immune–inflammation index in acute/subacute patients with cerebral venous sinus thrombosis. Stroke Vasc. Neurol. 2020, 5, 368–373. [Google Scholar] [CrossRef]
- Jiang, C.; Wu, W.; Deng, Y.; Ge, J. Modulators of microglia activation and polarization in ischemic stroke (Review). Mol. Med. Rep. 2020, 21, 2006–2018. [Google Scholar] [CrossRef] [Green Version]
- Xu, S.; Lu, J.; Shao, A.; Zhang, J.H.; Zhang, J. Glial Cells: Role of the Immune Response in Ischemic Stroke. Front. Immunol. 2020, 11, 294. [Google Scholar] [CrossRef] [PubMed]
- Lan, X.; Han, X.; Li, Q.; Yang, Q.-W.; Wang, J. Modulators of microglial activation and polarization after intracerebral haemorrhage. Nat. Rev. Neurol. 2017, 13, 420–433. [Google Scholar] [CrossRef] [Green Version]
- Tso, A.R.; Merino, J.G.; Warach, S. Interleukin-6—174G/C Polymorphism and Ischemic Stroke. Stroke 2007, 38, 3070–3075. [Google Scholar] [CrossRef] [Green Version]
- Lv, K.; Yang, Y. Relationship between interleukin-10 polymorphisms and susceptibility to ischemic stroke: A Meta-analysis. Scand. J. Clin. Lab. Investig. 2019, 80, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Ding, J.; Hong, R.; Bai, S.; Wang, Z.; Mo, C.; Hu, Q.; Li, Z.; Guan, Y. Increased interleukin-18 level contributes to the development and severity of ischemic stroke. Aging 2019, 11, 7457–7472. [Google Scholar] [CrossRef] [PubMed]
- Dziedzic, T.; Bartus, S.; Klimkowicz, A.; Motyl, M.; Slowik, A.; Szczudlik, A. Intracerebral hemorrhage triggers interleukin-6 and interleukin-10 release in blood. Stroke 2002, 33, 2334–2335. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.-W.; Cho, C.-L.; Chen, H.-J.; Liang, C.-L.; LiLiang, P.-C.; Tsai, Y.-D.; Wang, H.-K.; Lu, K. Molecular Biomarker of Inflammatory Response Is Associated with Rebleeding in Spontaneous Intracerebral Hemorrhage. Eur. Neurol. 2011, 66, 322–327. [Google Scholar] [CrossRef]
- Fang, H.-Y.; Ko, W.-J.; Lin, C.-Y. Plasma interleukin 11 levels correlate with outcome of spontaneous intracerebral hemorrhage. Surg. Neurol. 2005, 64, 511–517. [Google Scholar] [CrossRef]
- Heye, A.K.; Culling, R.D.; Hernández, M.D.C.V.; Thrippleton, M.J.; Wardlaw, J.M. Assessment of blood–brain barrier disruption using dynamic contrast-enhanced MRI. A systematic review. NeuroImage Clin. 2014, 6, 262–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yi, X.; Sui, G.; Zhou, Q.; Wang, C.; Lin, J.; Chai, Z.; Zhou, J. Variants in matrix metalloproteinase-9 gene are associated with hemorrhagic transformation in acute ischemic stroke patients with atherothrombosis, small artery disease, and cardioembolic stroke. Brain Behav. 2019, 9, e01294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Copin, J.-C.; Merlani, P.; Sugawara, T.; Chan, P.H.; Gasche, Y. Delayed matrix metalloproteinase inhibition reduces intracerebral hemorrhage after embolic stroke in rats. Exp. Neurol. 2008, 213, 196–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, T.; Wen, G.; Lawton, M.T.; Boudreau, N.J.; Bollen, A.W.; Yang, G.-Y.; Barbaro, N.M.; Higashida, R.T.; Dowd, C.F.; Halbach, V.V.; et al. Abnormal Expression of Matrix Metalloproteinases and Tissue Inhibitors of Metalloproteinases in Brain Arteriovenous Malformations. Stroke 2003, 34, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Todor, D.R.; Lewis, I.; Bruno, G.; Chyatte, D. Identification of a serum gelatinase associated with the occurrence of cerebral aneurysms as pro-matrix metalloproteinase-2. Stroke 1998, 29, 1580–1583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, W.-M.; Chen, C.-M.; Lee, Y.-S.; Chang, K.-H.; Chen, H.-W.; Chen, S.-T.; Chen, Y.-C. Association of MMP-9 Haplotypes and TIMP-1 Polymorphism with Spontaneous Deep Intracerebral Hemorrhage in the Taiwan Population. PLoS ONE 2015, 10, e0125397. [Google Scholar] [CrossRef]
- Zhao, L.; Arbel-Ornath, M.; Wang, X.; Betensky, R.A.; Greenberg, S.M.; Frosch, M.P.; Bacskai, B.J. Matrix metalloproteinase 9–mediated intracerebral hemorrhage induced by cerebral amyloid angiopathy. Neurobiol. Aging 2015, 36, 2963–2971. [Google Scholar] [CrossRef] [Green Version]
- Xue, M.; Hollenberg, M.D.; Yong, V.W. Combination of Thrombin and Matrix Metalloproteinase-9 Exacerbates Neurotoxicity in Cell Culture and Intracerebral Hemorrhage in Mice. J. Neurosci. 2006, 26, 10281–10291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Sousa, D.A.; Pereira-Santos, M.C.; Serra-Caetano, A.; Neto, L.L.; Sousa, A.L.; Gabriel, D.; Correia, M.; Gil-Gouveia, R.; Oliveira, R.; Penas, S.; et al. Matrix Metalloproteinase-9 Levels are Associated with Brain Lesion and Persistent Venous Occlusion in Patients with Cerebral Venous Thrombosis. Thromb. Haemost. 2021. [Google Scholar] [CrossRef]
- Duan, J.; Leng, X.; Han, Z.; Cai, Y.; Wang, C.; Rajah, G.; Song, H.; Ding, Y.; Ji, X. Identifying Biomarkers Associated with Venous Infarction in Acute/Subacute Cerebral Venous Thrombosis. Aging Dis. 2021, 12, 93–101. [Google Scholar] [CrossRef]
- Michetti, F.; D’Ambrosi, N.; Toesca, A.; Puglisi, M.A.; Serrano, A.; Marchese, E.; Corvino, V.; Geloso, M.C. The S100B story: From biomarker to active factor in neural injury. J. Neurochem. 2018, 148, 168–187. [Google Scholar] [CrossRef] [Green Version]
- Rahmati, M.; Azarpazhooh, M.R.; Ehteram, H.; Ferns, G.A.; Ghayour-Mobarhan, M.; Ghannadan, H.; Mobarra, N. The elevation of S100B and downregulation of circulating miR-602 in the sera of ischemic stroke (IS) patients: The emergence of novel diagnostic and prognostic markers. Neurol. Sci. 2020, 41, 2185–2192. [Google Scholar] [CrossRef]
- Selçuk, Ö.; Yayla, V.; Çabalar, M.; Güzel, V.; Uysal, S.; Gedikbasi, A. The Relationship of Serum S100B Levels with Infarction Size and Clinical Outcome in Acute Ischemic Stroke Patients. Arch. Neuropsychiatry 2014, 51, 395–400. [Google Scholar] [CrossRef]
- Weglewski, A.; Ryglewicz, D.; Mular, A.; Juryńczyk, J. Changes of protein S100B serum concentration during ischemic and hemorrhagic stroke in relation to the volume of stroke lesion. Neurol. Neurochir. Pol. 2005, 39, 310–317. [Google Scholar]
- Nielsen, H.H.; Soares, C.B.; Høgedal, S.S.; Madsen, J.S.; Hansen, R.B.; Christensen, A.A.; Madsen, C.; Clausen, B.H.; Frich, L.H.; Degn, M.; et al. Acute Neurofilament Light Chain Plasma Levels Correlate with Stroke Severity and Clinical Outcome in Ischemic Stroke Patients. Front. Neurol. 2020, 11, 448. [Google Scholar] [CrossRef] [PubMed]
- Montaner, J.; Mendioroz, M.; Delgado, P.; García-Berrocoso, T.; Giralt, D.; Merino, C.; Ribo, M.; Rosell, A.; Penalba, A.; Fernandez-Cade, I.; et al. Differentiating ischemic from hemorrhagic stroke using plasma biomarkers: The S100B/RAGE pathway. J. Proteom. 2012, 75, 4758–4765. [Google Scholar] [CrossRef] [PubMed]
- Glushakova, O.Y.; Glushakov, A.; Miller, E.R.; Valadka, A.B.; Hayes, R.L. Biomarkers for acute diagnosis and management of stroke in neurointensive care units. Brain Circ. 2016, 2, 28–47. [Google Scholar] [CrossRef]
- Qian, S.-Q.; He, S.-R.; Li, B.-B.; Qian, J.; Zheng, X.-D. Serum S100A12 and 30-day mortality after acute intracerebral hemorrhage. Clin. Chim. Acta 2018, 477, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.; Pepys, M.B.; Wood, S.P. The physiological structure of human C-reactive protein and its complex with phosphocholine. Structure 1999, 7, 169–177. [Google Scholar] [CrossRef]
- Mengozzi, M.; Kirkham, F.A.; Girdwood, E.E.R.; Bunting, E.; Drazich, E.; Timeyin, J.; Ghezzi, P.; Rajkumar, C. C-Reactive Protein Predicts Further Ischemic Events in Patients with Transient Ischemic Attack or Lacunar Stroke. Front. Immunol. 2020, 11, 1403. [Google Scholar] [CrossRef]
- Yu, B.; Yang, P.; Xu, X.; Shao, L. C-reactive protein for predicting all-cause mortality in patients with acute ischemic stroke: A meta-analysis. Biosci. Rep. 2019, 39. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Han, W.; Gong, D.; Man, C.; Fan, Y. Hs-CRP in stroke: A meta-analysis. Clin. Chim. Acta 2016, 453, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Di Napoli, M.; Godoy, D.A.; Campi, V.; del Valle, M.; Piñero, G.; Mirofsky, M.; Popa-Wagner, A.; Masotti, L.; Papa, F.; Rabinstein, A.A. C-Reactive Protein Level Measurement Improves Mortality Prediction When Added to the Spontaneous Intracerebral Hemorrhage Score. Stroke 2011, 42, 1230–1236. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Duan, J.; Bian, T.; Meng, R.; Wu, L.; Zhang, Z.; Zhang, X.; Wang, C.; Ji, X. Inflammation is correlated with severity and outcome of cerebral venous thrombosis. J. Neuroinflammation 2018, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Tian, D.; Zhang, S.; He, X.; Liu, H. Serum procalcitonin as a diagnostic marker in acute ischemic stroke. NeuroReport 2015, 26, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Wang, S.; Xu, L.; Zhang, Z.; Liao, P. Procalcitonin as a prognostic marker of patients with acute ischemic stroke. J. Clin. Lab. Anal. 2020, 34, e23301. [Google Scholar] [CrossRef] [Green Version]
- He, D.; Zhang, Y.; Zhang, B.; Jian, W.; Deng, X.; Yang, Y.; Xiao, T.; Yu, H.; Wen, S.; Huang, K. Serum Procalcitonin Levels are Associated with Clinical Outcome in Intracerebral Hemorrhage. Cell. Mol. Neurobiol. 2017, 38, 727–733. [Google Scholar] [CrossRef]
- Deng, S.; Gao, J.; Zhao, Z.; Tian, M.; Li, Y.; Gong, Y. Albumin/Procalcitonin Ratio Is a Sensitive Early Marker of Nosocomial Blood Stream Infection in Patients with Intra-Cerebral Hemorrhage. Surg. Infect. 2019, 20, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Meng, R.; Wang, X.; Hussain, M.; Dornbos, D., III; Meng, L.; Liu, Y.; Wu, Y.; Ning, M.; Buonanno, F.S.; Lo, E.H.; et al. Evaluation of plasma D-dimer plus fibrinogen in predicting acute CVST. Int. J. Stroke 2013, 9, 166–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misra, U.K.; Kalita, J.; Bansal, V. D-dimer is useful in the diagnosis of cortical venous sinus thrombosis. Neurol. India 2009, 57, 50–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talbot, K.; Wright, M.; Keeling, D. Normal d-dimer levels do not exclude the diagnosis of cerebral venous sinus thrombosis. J. Neurol. 2002, 249, 1603–1604. [Google Scholar] [CrossRef]
- Singh, A.S.; Atam, V.; Yathish, B.E.; Das, L.; Koonwar, S. Role of erythrocyte sedimentation rate in ischemic stroke as an inflammatory marker of carotid atherosclerosis. J. Neurosci. Rural. Pr. 2014, 5, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Perez, F.J.; Castelo-Branco, M.; Alvarez-Sabin, J. Usefulness of measurement of fibrinogen, D-dimer, D-dimer/fibrinogen ratio, C reactive protein and erythrocyte sedimentation rate to assess the pathophysiology and mechanism of ischaemic stroke. J. Neurol. Neurosurg. Psychiatry 2011, 82, 986–992. [Google Scholar] [CrossRef] [Green Version]
- Xie, D.; Hu, D.; Zhang, Q.; Sun, Y.; Li, J.; Zhang, Y. Increased high-sensitivity C-reactive protein, erythrocyte sedimentation rate and lactic acid in stroke patients with internal carotid artery occlusion. Arch. Med. Sci. 2016, 3, 546–551. [Google Scholar] [CrossRef]
- Chamorro, A.; Vila, N.; Ascaso, C.; Saiz, A.; Montalvo, J.; Alonso, P.; Tolosa, E. Early Prediction of Stroke Severity. Stroke 1995, 26, 573–576. [Google Scholar] [CrossRef]
- Zaremba, J.; Skrobański, P.; Losy, J. Acute ischaemic stroke increases the erythrocyte sedimentation rate, which correlates with early brain damage. Folia Morphol. 2004, 63, 373–376. [Google Scholar]
- Nikanfar, M.; Shaafi, S.; Hashemilar, M.; Oskouii, D.S.; Goldust, M. Evaluating Role of Leukocytosis and High Sedimentation Rate as Prognostic Factors in Acute Ischemic Cerebral Strokes. Pak. J. Biol. Sci. 2012, 15, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Gill, D.; Monori, G.; Tzoulaki, I.; Dehghan, A. Iron Status and Risk of Stroke. Stroke 2018, 49, 2815–2821. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.; Jiang, L.; Hu, Y.; Tang, N.; Liang, N.; Li, X.-F.; Chen, Y.-W.; Qin, H.; Wu, L. Ferritin reduction is essential for cerebral ischemia-induced hippocampal neuronal death through p53/SLC7A11-mediated ferroptosis. Brain Res. 2021, 1752, 147216. [Google Scholar] [CrossRef]
- Erdemoglu, A.K.; Ozbakır, S. Serum ferritin levels and early prognosis of stroke. Eur. J. Neurol. 2002, 9, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Kaur, S.; Garg, R.; Aravind, S.; Chawla, S.P.S.; Aggarwal, S.; Goyal, G. Role of serum ferritin as a prognostic marker in acute ischemic stroke: A preliminary observation. Ann. Afr. Med. 2020, 19, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Han, B.; Wang, L.; Chang, Y.; Ren, W.; Gu, Y.; Yan, M.; Wu, C.; Zhang, X.Y.; He, J. The association between serum ferritin levels and post-stroke depression. J. Affect. Disord. 2016, 190, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-T.; Chu, K.; Sinn, D.-I.; Jung, K.-H.; Kim, E.-H.; Kim, S.-J.; Kim, J.-M.; Ko, S.-Y.; Kim, M.; Roh, J.-K. Erythropoietin reduces perihematomal inflammation and cell death with eNOS and STAT3 activations in experimental intracerebral hemorrhage. J. Neurochem. 2006, 96, 1728–1739. [Google Scholar] [CrossRef] [PubMed]
- Garton, A.L.; Gupta, V.; Christophe, B.R.; Connolly, E.S. Biomarkers of Functional Outcome in Intracerebral Hemorrhage: Interplay between Clinical Metrics, CD163, and Ferritin. J. Stroke Cerebrovasc. Dis. 2017, 26, 1712–1720. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Chen, X.-C.; Lou, X.-H.; Qian, S.-Q.; Ruan, Z.-W. Determination of serum neutrophil gelatinase-associated lipocalin as a prognostic biomarker of acute spontaneous intracerebral hemorrhage. Clin. Chim. Acta 2019, 492, 72–77. [Google Scholar] [CrossRef]
- Wang, G.; He, C.-J.; Liang, X.-S.; Zhou, Y.-F.; Chen, S.-H. Potential role of serum substance P as a favorable biomarker of functional outcome in acute spontaneous intracerebral hemorrhage. Clin. Chim. Acta 2020, 510, 111–116. [Google Scholar] [CrossRef]
- Lorenzano, S.; Rost, N.S.; Khan, M.; Li, H.; Batista, L.M.; Chutinet, A.; Green, R.E.; Thankachan, T.K.; Thornell, B.; Muzikansky, A.; et al. Early molecular oxidative stress biomarkers of ischemic penumbra in acute stroke. Neurology 2019, 93, e1288–e1298. [Google Scholar] [CrossRef]
- Tsai, N.-W.; Chang, Y.-T.; Huang, C.-R.; Lin, Y.-J.; Lin, W.-C.; Cheng, B.-C.; Su, C.-M.; Chiang, Y.-F.; Chen, S.-F.; Huang, C.-C.; et al. Association between Oxidative Stress and Outcome in Different Subtypes of Acute Ischemic Stroke. BioMed Res. Int. 2014, 2014, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Park, S.-Y.; Kim, M.-H.; Kim, O.-J.; Ahn, H.-J.; Song, J.-Y.; Jeong, J.-Y.; Oh, S.-H. Plasma heart-type fatty acid binding protein level in acute ischemic stroke: Comparative analysis with plasma S100B level for diagnosis of stroke and prediction of long-term clinical outcome. Clin. Neurol. Neurosurg. 2013, 115, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-Y.; Kim, J.; Kim, O.-J.; Kim, J.-K.; Song, J.; Shin, D.-A.; Oh, S.-H. Predictive value of circulating interleukin-6 and heart-type fatty acid binding protein for three months clinical outcome in acute cerebral infarction: Multiple blood markers profiling study. Crit. Care 2013, 17, R45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanzione, R.; Forte, M.; Cotugno, M.; Bianchi, F.; Marchitti, S.; Rubattu, S. Role of DAMPs and of Leukocytes Infiltration in Ischemic Stroke: Insights from Animal Models and Translation to the Human Disease. Cell. Mol. Neurobiol. 2020, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Gairolla, J.; Kler, R.; Modi, M.; Khurana, D. Leptin and adiponectin: Pathophysiological role and possible therapeutic target of inflammation in ischemic stroke. Rev. Neurosci. 2017, 28, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Bharatkumar, V.P.; Rudreshkumar, K.J.; Nagaraja, D.; Christopher, R. Plasma S-adenosylhomocysteine: A potential risk marker for cerebral venous thrombosis. Clin. Chim. Acta 2016, 458, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Liesz, A.; Roth, S.; Zorn, M.; Sun, L.; Hofmann, K.; Veltkamp, R. Acquired Immunoglobulin G deficiency in stroke patients and experimental brain ischemia. Exp. Neurol. 2015, 271, 46–52. [Google Scholar] [CrossRef]
- Chamorro, Á.; Amaro, S.; Castellanos, M.; Segura, T.; Arenillas, J.; Martí-Fábregas, J.; Gellego, J.; Krupinski, J.; Gomis, M.; Canovas, D.; et al. Safety and efficacy of uric acid in patients with acute stroke (URICO-ICTUS): A randomised, double-blind phase 2b/3 trial. Lancet Neurol. 2014, 13, 453–460. [Google Scholar] [CrossRef]
- Yang, Q.-W.; Liu, M.; Zhang, S.-H.; Wu, B. Edaravone for acute cerebral infarction: A systematic review. Chin. J. Evid. Based Med. 2006, 1, 18–22. [Google Scholar]
- Feng, S.; Yang, Q.; Liu, M.; Li, W.; Yuan, W.; Zhang, S.; Wu, B.; Li, J. Edaravone for acute ischemic stroke. Cochrane Database Syst. Rev. 2011, 12, CD007230. [Google Scholar] [CrossRef]
- Phase III Clinical Trial of Y-2 Sublingual Tablets in the Treatment of Acute Ischemic Stroke, Identifier: NCT04950920, (n.d.). Available online: https://clinicaltrials.gov/ct2/show/NCT04950920 (accessed on 19 September 2021).
- Efficacy and Safety of Butylphthalide for Acute Ischemic Stroke Patients Receiving Intravenous Thrombolysis or Endovascular Treatment, Identifier: NCT03539445, (n.d.). Available online: https://clinicaltrials.gov/ct2/show/NCT03539445 (accessed on 19 September 2021).
- Zhang, F.; Yan, C.; Wei, C.; Yao, Y.; Ma, X.; Gong, Z.; Liu, S.; Zang, D.; Chen, J.; Shi, F.-D.; et al. Vinpocetine Inhibits NF-κB-Dependent Inflammation in Acute Ischemic Stroke Patients. Transl. Stroke Res. 2018, 9, 174–184. [Google Scholar] [CrossRef]
- Phase Ib/IIa Clinical Study of ApTOLL for the Treatment of Acute Ischemic Stroke, Identifier: NCT04734548, (n.d.). Available online: https://clinicaltrials.gov/show/NCT04734548 (accessed on 1 September 2021).
- Mater Misericordia, Colchicine for Prevention of Vascular Inflammation in Non-Cardio Embolic Stroke, Identifier: NCT02898610, (n.d.). Available online: https://clinicaltrials.gov/show/NCT02898610 (accessed on 1 September 2021).
- Liu, J.; Zhang, C.; Tao, W.; Liu, M. Systematic Review and Meta-Analysis of the Efficacy of Sphingosine-1-Phosphate (S1P) Receptor Agonist FTY720 (Fingolimod) in Animal Models of Stroke. Int. J. Neurosci. 2012, 123, 163–169. [Google Scholar] [CrossRef]
- Wang, N. Fingolimod in Endovascular Treatment of Ischemic Stroke. 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT04629872?term=treatment&cond=stroke%2C+inflammation&draw=2&rank=1 (accessed on 1 September 2021).
- Wendy Jenkins, K.H. Fingolimod as a Treatment of Cerebral Edema After Intracerebral Hemorrhage (FITCH), Clin. Identifier NCT04088630. 2019. Available online: https://clinicaltrials.gov/ct2/show/NCT04088630 (accessed on 1 September 2021).
- Langhauser, F.; Kraft, P.; Gob, E.; Leinweber, J.; Schumann, M.K.; Lorenz, K.; Gelderblom, M.; Bittner, S.; Meuth, S.G.; Wiendl, H.; et al. Blocking of α4 integrin does not protect from acute ischemic stroke in mice. Stroke 2014, 45, 1799–1806. [Google Scholar] [CrossRef] [Green Version]
- Llovera, G.; Hofmann, K.; Roth, S.; Salas-Perdomo, A.; Ferrer-Ferrer, M.; Perego, C.; Zanier, E.R.; Mamrak, U.; Rex, A.; Party, H.; et al. Results of a preclinical randomized controlled multicenter trial (pRCT): Anti-CD49d treatment for acute brain ischemia. Sci. Transl. Med. 2015, 7, 299ra121. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.-P.; Zhang, M.-Y. Role for Target of Rapamycin (mTOR) Signal Pathway in Regulating Neuronal Injury after Intracerebral Hemorrhage. Cell. Physiol. Biochem. 2017, 41, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Liu, Y.; Yuan, F.; Li, Z.; Huang, S.; Shen, H.; Yuan, B. Sinomenine inhibits microglia activation and attenuates brain injury in intracerebral hemorrhage. Mol. Immunol. 2014, 60, 109–114. [Google Scholar] [CrossRef]
- Shi, H.; Zheng, K.; Su, Z.; Su, H.; Zhong, M.; He, X.; Zhou, C.; Chen, H.; Xiong, Q.; Zhang, Y. Sinomenine enhances microglia M2 polarization and attenuates inflammatory injury in intracerebral hemorrhage. J. Neuroimmunol. 2016, 199, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Safety Study of Interferon Beta 1a to for Acute Stroke, Identifier: NCT00097318, (n.d.). Available online: https://clinicaltrials.gov/show/NCT00097318%0D%0A (accessed on 1 September 2021).
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- BLOC-ICH: Interleukin-1 Receptor Antagonist in Intracerebral Haemorrhage, Identifier: NCT03737344, (n.d.). Available online: https://clinicaltrials.gov/show/NCT03737344 (accessed on 1 September 2021).
Figure 1.
Inflammatory biomarkers in cerebrovascular disorders.


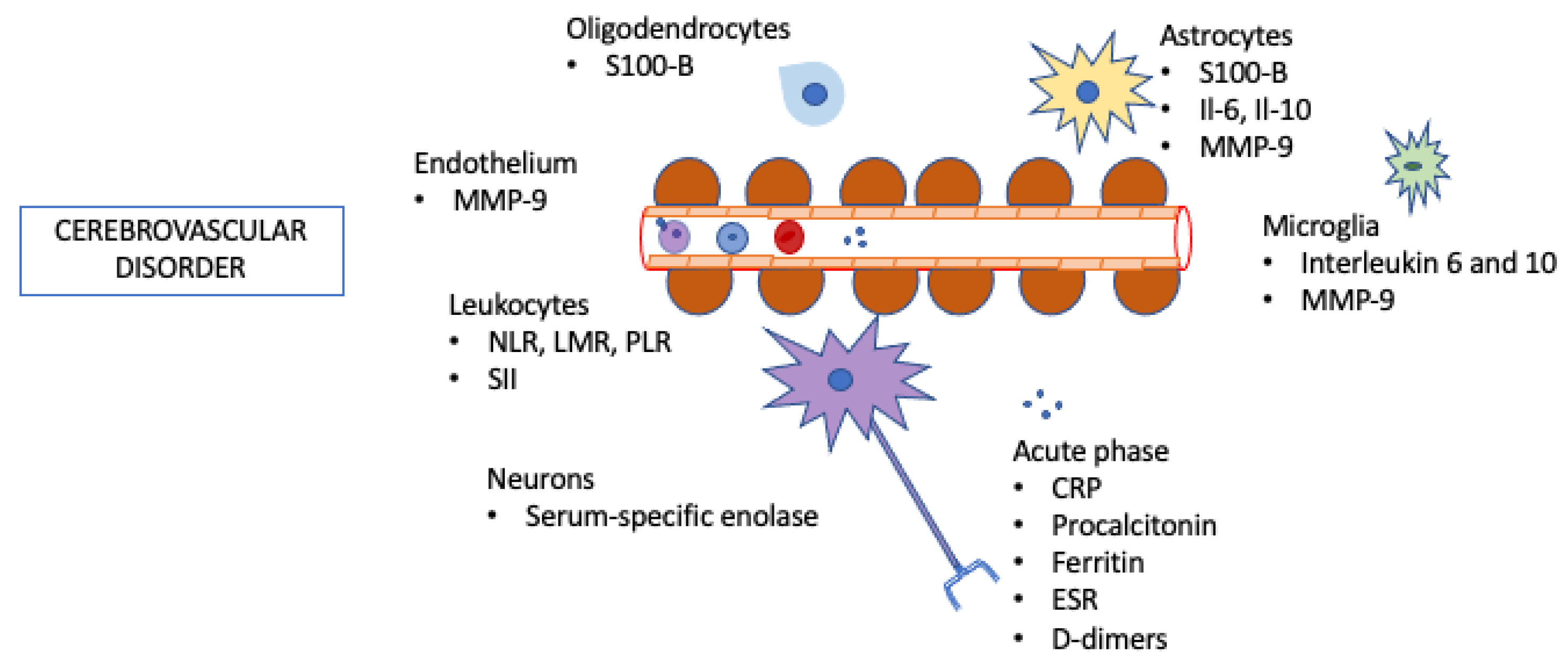{kind=link}
Table 1.
Summary of inflammatory biomarkers related to cerebrovascular disease and the application in which they are currently being evaluated.
Table 1.
Summary of inflammatory biomarkers related to cerebrovascular disease and the application in which they are currently being evaluated.
| Biomarker | Ischemic Stroke | ICH | CVT |
|---|---|---|---|
| NLR | - Hemorrhagic transformation - Cerebral Edema Grade - Mechanical thrombectomy outcome - Post-stroke depression - Mortality | - Clinical outcome (GCS, severity) - ICH volume - Post-stroke depression - Mortality | - Diagnosis - Clinical outcome (NIHSS) - Disability |
| LMR | - Hemorrhagic transformation - Outcome - Post-stroke depression | - Possible ICH Volume - Mortality | - Possible diagnosis - Outcome |
| PLR | - Functional Outcome - Post-stroke depression - Mortality | - Clinical outcome (GCS) - Functional Outcome | - In-hospital adverse events |
| SII | - Outcome in mechanical thrombectomy | - Functional Outcome | - Functional Outcome - Mortality |
| Interleukin | - Diagnosis - Clinical outcome - Ischemic volume | - ICH volume - Mortality | - Functional Outcome |
| MMP-9 | - Severity - Ischemic volume - Hemorrhagic transformation - Mortality | - Hemorrhage due to beta-amyloid angiopathy | - CVT recanalization |
| Calcium-binding proteins | - Hemorrhagic transformation - Functional Outcome | - Clinical outcome (GCS, severity) - ICH volume | - Severity |
| CRP | - Risk of stroke after TIA - Mortality | - Functional Outcome | - Seizure - Outcome |
| Procalcitonin | - Risk factor - Mortality | - Outcome | - |
| ESR | - Mortality - Large vessel disorder | - | - |
| Iron, Ferritin, EPO | - Cardioembolic stroke | - Outcome | - |
NLR—Neutrophil-to-lymphocyte ratio; LMR—lymphocyte-to-monocyte ratio; PLR—latelet-to lymphocyte ratio; SII—systemic immune-inflammatory index; MMP-9—matrix metalloproteinase-9; CRP—C-reactive protein; ESR—erythrocyte sedimentation rate.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Dias, R.A.; Dias, L.; Azevedo, E.; Castro, P. Acute Inflammation in Cerebrovascular Disease: A Critical Reappraisal with Focus on Human Studies. Life 2021, 11, 1103. https://0-doi-org.brum.beds.ac.uk/10.3390/life11101103
AMA Style
Dias RA, Dias L, Azevedo E, Castro P. Acute Inflammation in Cerebrovascular Disease: A Critical Reappraisal with Focus on Human Studies. Life. 2021; 11(10):1103. https://0-doi-org.brum.beds.ac.uk/10.3390/life11101103
Chicago/Turabian StyleDias, Rafael Azevedo, Leonor Dias, Elsa Azevedo, and Pedro Castro. 2021. "Acute Inflammation in Cerebrovascular Disease: A Critical Reappraisal with Focus on Human Studies" Life 11, no. 10: 1103. https://0-doi-org.brum.beds.ac.uk/10.3390/life11101103
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.