
Molecular Mechanisms Underlying the Pain-Relieving Effects of Extracorporeal Shock Wave Therapy: A Focus on Fascia Nociceptors

 , , ,
, , ,
Abstract
:1. Introduction
2. Physiology and Biology of ESWT
2.1. Mechanism of Action: Technical Aspect
2.2. Types of ESWT: Focused vs. Radial Extracorporeal Shock Waves
2.3. Biological and Molecular Effects of ESWT on Bones and Soft Tissues
3. A Brief Overview of the Human Fascial System and Its Role as a Pain Generator in Musculoskeletal Dysfunctions
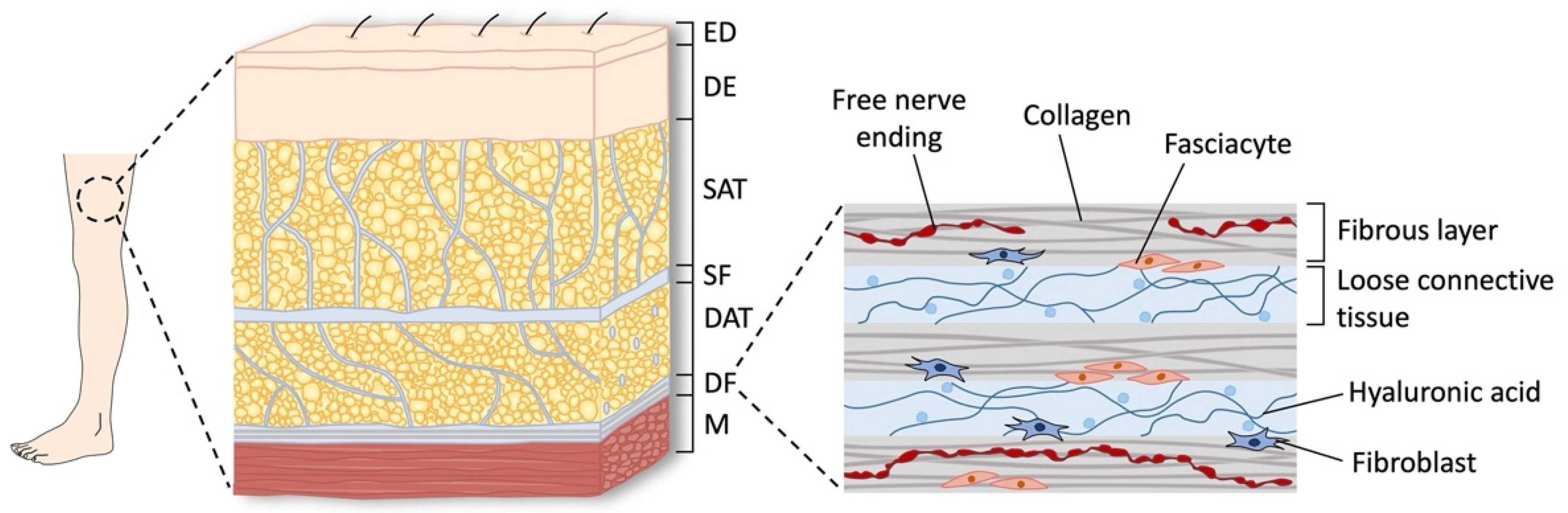
3.1. Anatomy and Function of the Fascial and Musculoskeletal System
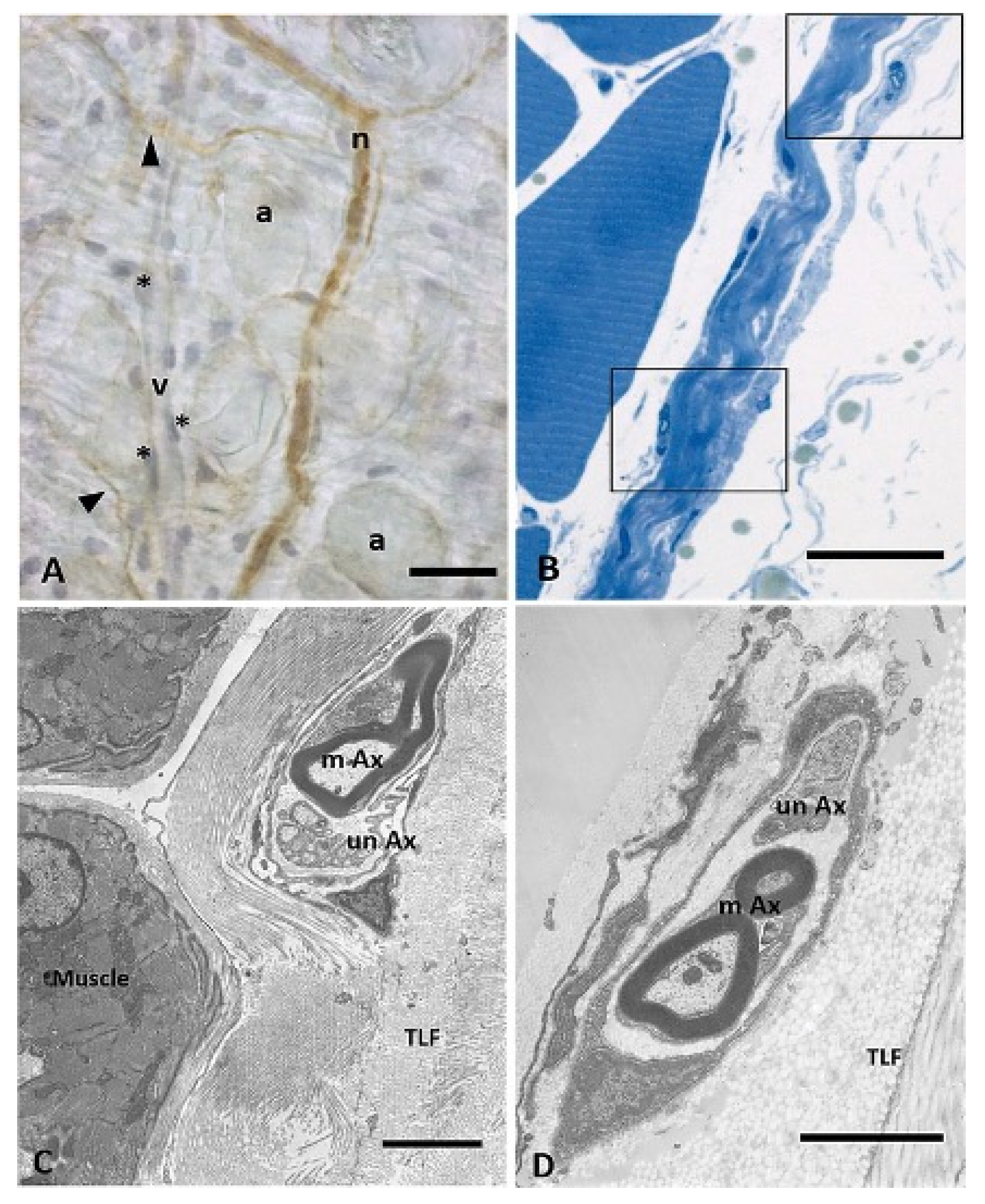
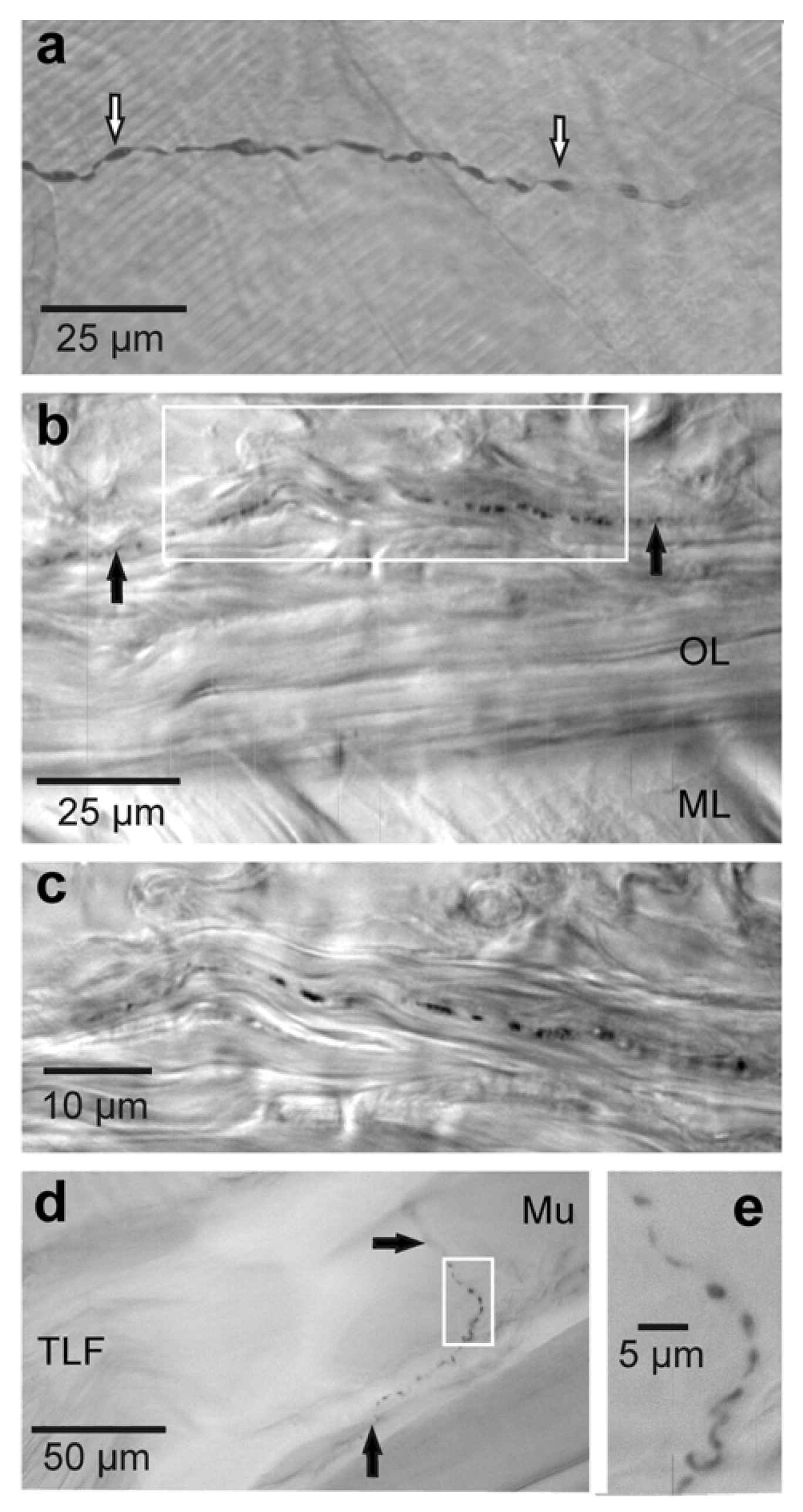
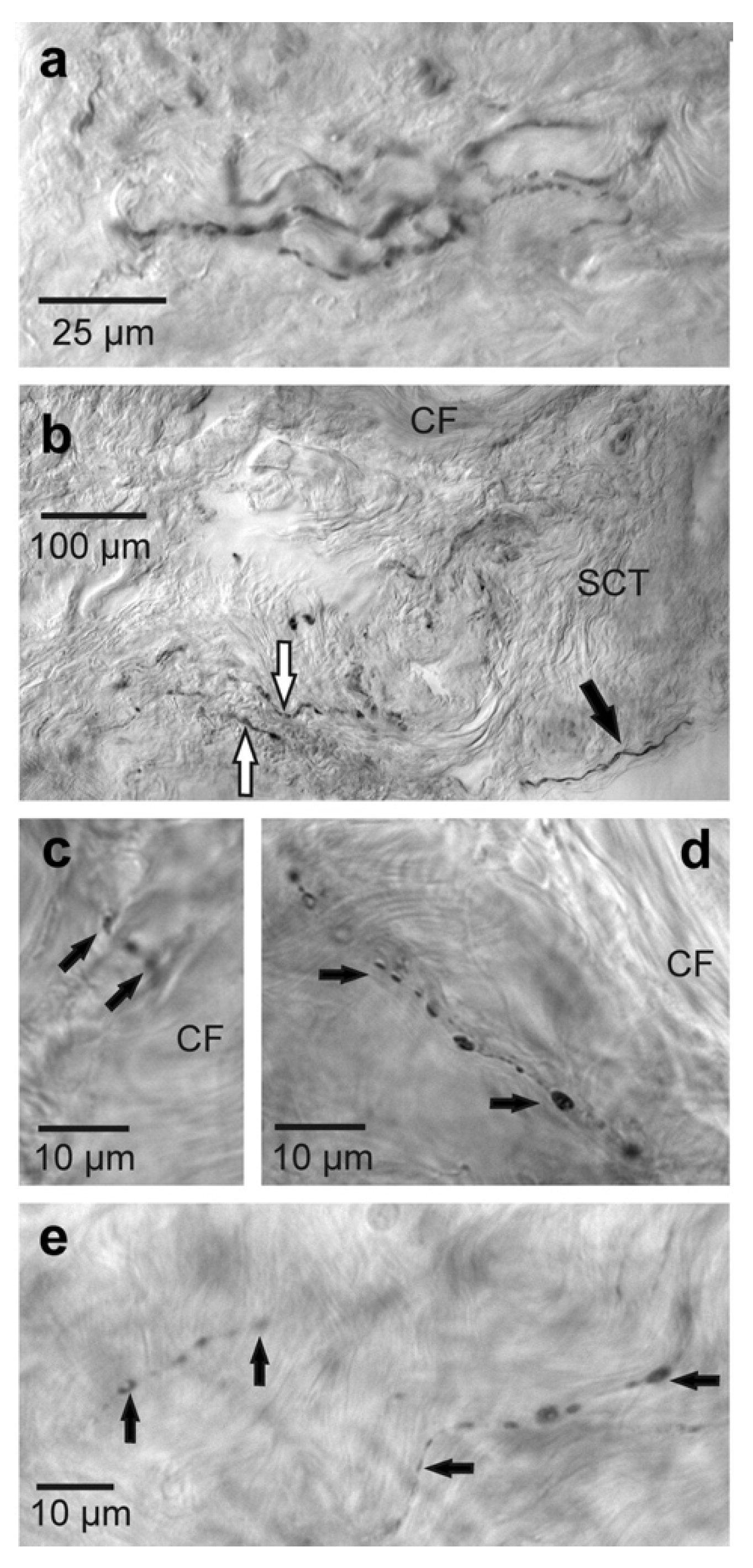
3.2. Sensory Innervation of the Deep Fascia: The Role of Nociceptive Fibers
3.3. The Deep Fascia as a Source of Pain in Musculoskeletal Disorders
4. Possible Molecular Mechanisms Underlying Pain-Relieving Effects of ESWT in the Musculoskeletal System
5. Conclusions and Future Research Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ATF3 | activating transcription factor 3 |
| ATP | adenosine triphosphate |
| BMP-2 | bone morphogenetic protein-2 |
| CGRP | calcitonin gene-related peptide |
| DAT | deep adipose tissue |
| EFD | energy flux density |
| eNOS | endothelial nitric oxide synthase |
| ERK; Erk1/2 | extracellular-signal-regulated kinase |
| ESWT | extracorporeal shock wave therapy |
| FAK | focal adhesion kinase |
| fESWT | focused shock wave therapy |
| FNEs | free nerve endings |
| fSW | focused shock waves |
| GSK-3β | glycogen synthase kinase 3 beta |
| HA | hyaluronic acid |
| HMW | high-molecular-weight |
| IGF-I | insulin-like growth factor-I |
| MNT | mechanical nociceptive threshold |
| MPa | megaPascal |
| MPS | myofascial pain syndrome |
| MTrPs | myofascial trigger points |
| PAG | periaqueductal grey |
| PCNA | proliferating cell nuclear antigen |
| PERK | protein kinase R-like endoplasmic reticulum kinase |
| PF | plantar fasciitis |
| PTLF | posterior layer of the thoracolumbar fascia |
| RCTs | randomized controlled trials |
| rESWT | radial shock wave therapy |
| rSW | radial shock waves |
| SAT | superficial adipose tissue |
| SP | substance P |
| TGF-β1 | transforming growth factor-beta 1 |
| TLF | thoracolumbar fascia |
| TLR3 | toll-like receptor 3 |
| TRPV1 | transient receptor potential cation channel subfamily V member 1 |
| VAS | visual analog scale |
| VEGF | vascular endothelial growth factor |
References
- Reilly, J.M.; Bluman, E.; Tenforde, A.S. Effect of Shockwave Treatment for Management of Upper and Lower Extremity Musculoskeletal Conditions: A Narrative Review. PM R 2018, 10, 1385–1403. [Google Scholar] [CrossRef] [PubMed]
- Chaussy, C.; Schmiedt, E.; Jocham, D.; Brendel, W.; Forssmann, B.; Walther, V. First clinical experience with extracorporeally induced destruction of kidney stones by shock waves. J. Urol. 1982, 127, 417–420. [Google Scholar] [CrossRef]
- Lawler, A.C.; Ghiraldi, E.M.; Tong, C.; Friedlander, J.I. Extracorporeal Shock Wave Therapy: Current Perspectives and Future Directions. Curr. Urol. Rep. 2017, 18, 25. [Google Scholar] [CrossRef] [PubMed]
- Moya, D.; Ramón, S.; Schaden, W.; Wang, C.J.; Guiloff, L.; Cheng, J.H. The Role of Extracorporeal Shockwave Treatment in Musculoskeletal Disorders. J. Bone Jt. Surg. Am. 2018, 100, 251–263. [Google Scholar] [CrossRef] [Green Version]
- Loew, M.; Jurgowski, W. Erste Erfahrungen mit der Extrakorporalen Stosswellen-Lithotripsie (ESWL) in der Behandlung der Tendinosis calcarea der Schulter [Initial experiences with extracorporeal shockwave lithotripsy (ESWL) in treatment of tendinosis calcarea of the shoulder]. Z. Orthop. Ihre Grenzgeb. 1993, 131, 470–473. [Google Scholar] [CrossRef]
- Rompe, J.D.; Rumler, F.; Hopf, C.; Nafe, B.; Heine, J. Extracorporal shock wave therapy for calcifying tendinitis of the shoulder. Clin. Orthop. Relat. Res. 1995, 321, 196–201. [Google Scholar] [CrossRef]
- Wang, C.J.; Ko, J.Y.; Chen, H.S. Treatment of calcifying tendinitis of the shoulder with shock wave therapy. Clin. Orthop. 2001, 387, 83–89. [Google Scholar] [CrossRef]
- Cacchio, A.; Paoloni, M.; Barile, A.; Don, R.; de Paulis, F.; Calvisi, V.; Ranavolo, A.; Frascarelli, M.; Santilli, V.; Spacca, G. Effectiveness of radial shock-wave therapy for calcific tendinitis of the shoulder: Single-blind, randomized clinical study. Phys. Ther. 2006, 86, 672–682. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.J.; Wang, D.Y.; Tseng, K.F.; Fong, Y.C.; Hsu, H.C.; Jim, Y.F. Extracorporeal shock wave therapy for calcifying tendinitis of the shoulder. J. Shoulder Elb. Surg. 2008, 17, 55–59. [Google Scholar] [CrossRef]
- Wang, C.J.; Yang, K.D.; Wang, F.S.; Chen, H.H.; Wang, J.W. Shock wave therapy for calcific tendinitis of the shoulder: A prospective clinical study with two-year follow-up. Am. J. Sports Med. 2003, 31, 425–430. [Google Scholar] [CrossRef]
- Ogden, J.A.; Alvarez, R.; Levitt, R.; Cross, G.L.; Marlow, M. Shock wave therapy for chronic proximal plantar fasciitis. Clin. Orthop. Relat. Res. 2001, 387, 47–59. [Google Scholar] [CrossRef]
- Rompe, J.D.; Schoellner, C.; Nafe, B. Evaluation of low-energy extracorporeal shock-wave application for treatment of chronic plantar fasciitis. J. Bone Jt. Surg. Am. 2002, 84, 335–341. [Google Scholar] [CrossRef]
- Sun, J.; Gao, F.; Wang, Y.; Sun, W.; Jiang, B.; Li, Z. Extracorporeal shock wave therapy is effective in treating chronic plantar fasciitis: A meta-analysis of RCTs. Medicine 2017, 96, e6621. [Google Scholar] [CrossRef]
- Wang, F.S.; Yang, K.D.; Chen, R.F.; Wang, C.J.; Sheen-Chen, S.M. Extracorporeal shock wave promotes growth and differentiation of bone marrow stromal cells towards osteoprogenitors associated with induction of TGF-β1. J. Bone Jt. Surg. Br. 2002, 84, 457–461. [Google Scholar] [CrossRef]
- Wang, C.; Wang, F.; Yang, K. Shock wave therapy induces neovascularization at the tendon-bone junction. A study in rabbits. J. Orthop. Res. 2003, 21, 984–989. [Google Scholar] [CrossRef]
- Mariotto, S.; Cavalieri, E.; Amelio, E.; Ciampa, A.R.; de Prati, A.C.; Marlinghaus, E.; Russo, S.; Suzuki, H. Extracorporeal shock waves: From lithotripsy to anti-inflammatory action by NO production. Nitric Oxide 2005, 12, 89–96. [Google Scholar] [CrossRef]
- Frairia, R.; Berta, L. Biological effects of extracorporeal shock waves on fibroblasts. A review. Muscles Ligaments Tendons J. 2012, 1, 138–147. [Google Scholar]
- D’Agostino, M.C.; Craig, K.; Tibalt, E.; Respizzi, S. Shock wave as biological therapeutic tool: From mechanical stimulation to recovery and healing, through mechanotransduction. Int. J. Surg. 2015, 24, 147–153. [Google Scholar] [CrossRef]
- Basoli, V.; Chaudary, S.; Cruciani, S.; Santaniello, S.; Balzano, F.; Ventura, C.; Redl, H.; Dungel, P.; Maioli, M. Mechanical Stimulation of Fibroblasts by Extracorporeal Shock Waves: Modulation of Cell Activation and Proliferation through a Transient Proinflammatory Milieu. Cell Transplant. 2020, 29, 0963689720916175. [Google Scholar] [CrossRef] [Green Version]
- Weihs, A.M.; Fuchs, C.; Teuschl, A.H.; Hartinger, J.; Slezak, P.; Mittermayr, R.; Redl, H.; Junger, W.G.; Sitte, H.H.; Rünzler, D. Shock wave treatment enhances cell proliferation and improves wound healing by ATP release-coupled extracellular signal-regulated kinase (ERK) activation. J. Biol. Chem. 2014, 289, 27090–27104. [Google Scholar] [CrossRef] [Green Version]
- Simplicio, C.L.; Purita, J.; Murrell, W.; Santos, G.S.; Dos Santos, R.G.; Lana, J.F.S.D. Extracorporeal shock wave therapy mechanisms in musculoskeletal regenerative medicine. J. Clin. Orthop. Trauma 2020, 11, S309–S318. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.-R.; Wang, C.-T.; Wang, F.-S.; Chiang, Y.-C.; Wang, C.-J. Extracorporeal shock-wave therapy enhanced wound healing via increasing topical blood perfusion and tissue regeneration in a rat model of STZ-induced diabetes. Wound Repair Regen. 2009, 17, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Mariotto, S.; De Prati, A.C.; Cavalieri, E.; Amelio, E.; Marlinghaus, E.; Suzuki, H. Extracorporeal Shock Wave Therapy in Inflammatory Diseases: Molecular Mechanism that Triggers Anti-Inflammatory Action. Curr. Med. Chem. 2009, 16, 2366–2372. [Google Scholar] [CrossRef] [PubMed]
- Sukubo, N.G.; Tibalt, E.; Respizzi, S.; Locati, M.; D’Agostino, M. Effect of shock waves on macrophages: A possible role in tissue regeneration and remodeling. Int. J. Surg. 2015, 24, 124–130. [Google Scholar] [CrossRef]
- Sun, D.; Junger, W.G.; Yuan, C.; Zhang, W.; Bao, Y.; Qin, D.; Wang, C.; Tan, L.; Qi, B.; Zhu, D.; et al. Shockwaves induce osteogenic differentiation of human mesenchymal stem cells through ATP release and activation of P2X7 receptors. Stem Cells 2013, 31, 1170–1180. [Google Scholar] [CrossRef] [Green Version]
- Catalano, M.G.; Marano, F.; Rinella, L.; de Girolamo, L.; Bosco, O.; Fortunati, N.; Berta, L.; Frairia, R. Extracorporeal shockwaves (ESWs) enhance the osteogenic medium-induced differentiation of adipose-derived stem cells into osteoblast-like cells. J. Tissue Eng. Regen. Med. 2017, 11, 390–399. [Google Scholar] [CrossRef] [Green Version]
- Leone, L.; Raffa, S.; Vetrano, M.; Ranieri, D.; Malisan, F.; Scrofani, C.; Vulpiani, M.C.; Ferretti, A.; Torrisi, M.R.; Visco, V. Extracorporeal Shock Wave Treatment (ESWT) enhances the in vitro-induced differentiation of human tendon-derived stem/progenitor cells (hTSPCs). Oncotarget 2016, 7, 6410–6423. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Kang, N.; Yu, X.; Ma, Y.; Pang, X. Radial Extracorporeal Shock Wave Therapy Enhances the Proliferation and Differentiation of Neural Stem Cells by Notch, PI3K/AKT, and Wnt/β-catenin Signaling. Sci. Rep. 2017, 7, 15321. [Google Scholar] [CrossRef] [Green Version]
- Aqil, A.; Siddiqui, M.R.; Solan, M.; Redfern, D.J.; Gulati, V.; Cobb, J.P. Extracorporeal shock wave therapy is effective in treating chronic plantar fasciitis: A meta-analysis of RCTs. Clin. Orthop. Relat. Res. 2013, 471, 3645–3652. [Google Scholar] [CrossRef] [Green Version]
- Melese, H.; Alamer, A.; Getie, K.; Nigussie, F.; Ayhualem, S. Extracorporeal shock wave therapy on pain and foot functions in subjects with chronic plantar fasciitis: Systematic review of randomized controlled trials. Disabil. Rehabiltation 2021, 1928775. [Google Scholar] [CrossRef]
- Ji, H.M.; Kim, H.J.; Han, S.J. Extracorporeal shock wave therapy in myofascial pain syndrome of upper trapezius. Ann. Rehabil. Med. 2012, 36, 675–680. [Google Scholar] [CrossRef] [Green Version]
- Jeon, J.H.; Jung, Y.J.; Lee, J.Y.; Choi, J.S.; Mun, J.H.; Park, W.Y.; Seo, C.H.; Jang, K.U. The effect of extracorporeal shock wave therapy on myofascial pain syndrome. Ann. Rehabil. Med. 2012, 36, 665–674. [Google Scholar] [CrossRef]
- Yoo, J.I.; Oh, M.K.; Chun, S.W.; Lee, S.U.; Lee, C.H. The effect of focused extracorporeal shock wave therapy on myofascial pain syndrome of trapezius: A systematic review and meta-analysis. Medicine 2020, 99, e19085. [Google Scholar] [CrossRef]
- Simons, D.G.; Travel, J.G.; Simons, L.S. Myofascial Pain and Dysfunction: The Trigger Point Manual, 2nd ed.; Williams and Wilkins: Philadelphia, PA, USA; Lippincott: Baltimore, MD, USA, 1999. [Google Scholar]
- Ramon, S.; Gleitz, M.; Hernandez, L.; Romero, L.D. Update on the efficacy of extracorporeal shockwave treatment for myofascial pain syndrome and fibromyalgia. Int. J. Surg. 2015, 24, 201–206. [Google Scholar] [CrossRef]
- Simons, D.G. Clinical and Etiological Update of Myofascial Pain from Trigger Points. J. Musculoskelet. Pain 1996, 4, 93–122. [Google Scholar] [CrossRef]
- Dommerholt, J.; Simons, D.G. Myofascial pain syndrome-trigger points. J. Musculoskelet. Pain 2008, 16, 211–228. [Google Scholar] [CrossRef]
- Suputtitada, A. Update of extracorporeal shockwave therapy in myofascial pain syndrome. Int. Phys. Med. Rehab. J. 2017, 1, 82–86. [Google Scholar] [CrossRef] [Green Version]
- Dommerholt, J.; Mayoral del Moral, O.; Grobli, C. Trigger point dry needling. J. Man. Manip. Ther. 2006, 14, 70–87. [Google Scholar] [CrossRef]
- Rickards, L.D. The effectiveness of non-invasive treatments for active myofascial trigger point pain: A systematic review of the literature. Int. J. Osteopath. Med. 2006, 9, 120–136. [Google Scholar] [CrossRef]
- Vázquez-Delgado, E.; Cascos-Romero, J.; Gay-Escoda, C. Myofascial pain syndrome associated with trigger points: A literature review. (I): Epidemiology, clinical treatment and etiopathogeny. Med. Oral Patol. Oral Cir. Bucal 2009, 14, 494–498. [Google Scholar] [CrossRef] [Green Version]
- Tough, E.A.; White, A.R.; Cummings, T.M.; Richards, S.H.; Campbell, J.L. Acupuncture and dry needling in the management of myofascial trigger point pain: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Pain 2009, 13, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Gerber, L.H.; Shah, J.; Rosenberger, W.; Armstrong, K.; Turo, D.; Otto, P.; Heimur, J.; Thaker, N.; Sikdar, S. Dry needling alters trigger points in the upper trapezius muscle and reduces pain in subjects with chronic myofascial pain. PM R 2015, 7, 711–718. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.F.; Liu, L.; Wang, B.B.; Liu, X.; Li, P. Evidence for kinesio taping in management of myofascial pain syndrome: A systematic review and meta-analysis. Clin. Rehabil. 2019, 33, 865–874. [Google Scholar] [CrossRef]
- Desai, M.J.; Saini, V.; Saini, S. Myofascial pain syndrome: A treatment review. Pain Ther. 2013, 2, 21–36. [Google Scholar] [CrossRef] [Green Version]
- Loew, M.; Daecke, W.; Kusnierczak, D.; Rahmanzadeh, M.; Ewerbeck, V. Shock-wave therapy is effective for chronic calcifying tendinitis of the shoulder. J. Bone Jt. Surg. Br. 1999, 81, 863–867. [Google Scholar] [CrossRef]
- Takahashi, N.; Ohtori, S.; Saisu, T.; Moriya, H.; Wada, Y. Second application of low-energy shock waves has a cumulative effect on free nerve endings. Clin. Orthop. Relat. Res. 2006, 443, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Rompe, J.D.; Furia, J.; Weil, L.; Maffulli, N. Shock wave therapy for chronic plantar fasciopathy. Br. Med. Bull. 2007, 81–82, 183–208. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.J.; Wang, F.S.; Yang, K.D.; Weng, L.H.; Ko, J.Y. Long-term results of extracorporeal shockwave treatment for plantar fasciitis. Am. J. Sports Med. 2006, 34, 592–596. [Google Scholar] [CrossRef]
- Dizon, J.N.; Gonzalez-Suarez, C.; Zamora, M.T.; Gambito, E.D. Effectiveness of extracorporeal shock wave therapy in chronic plantar fasciitis: A meta-analysis. Am. J. Phys. Med. Rehabil. 2013, 92, 606–620. [Google Scholar] [CrossRef]
- Ohtori, S.; Inoue, G.; Mannoji, C.; Saisu, T.; Takahashi, K.; Mitsuhashi, S.; Wada, Y.; Takahashi, K.; Yamagata, M.; Moriya, H. Shock wave application to rat skin induces degeneration and reinnervation of sensory nerve fibres. Neurosci. Lett. 2001, 315, 57–60. [Google Scholar] [CrossRef]
- Maier, M. Selective Loss of Unmyelinated and Small Myelinated Fibres within the Femoral Nerve and Reduction in Substance P Production in Dorsal Root Ganglia L5 to L7 Following High-Energy Extracorporeal Shock Wave Application to the Ventral Side of the Distal Femur of Rabbits. DIGEST Award, Baden-Baden. 2004. Available online: https://0-academic-oup-com.brum.beds.ac.uk/bmb/article/81-82/1/183/282933 (accessed on 8 April 2022).
- Murata, R.; Ohtori, S.; Ochiai, N.; Takahashi, N.; Saisu, T.; Moriya, H.; Takahashi, K.; Wada, Y. Extracorporeal shockwaves induce the expression of ATF3 and GAP-43 in rat dorsal root ganglion neurons. Auton. Neurosci. 2006, 128, 96–100. [Google Scholar] [CrossRef]
- Rompe, J.D.; Meurer, A.; Nafe, B.; Hoffman, A.; Gerdesmeyer, L. Repetitive low-energy shock wave application without local anesthesia is more efficient than repetitive low-energy shock wave application with local anesthesia in the treatment of chronic plantar fasciitis. J. Orthop. Res. 2005, 23, 931–941. [Google Scholar] [CrossRef]
- Hausdorf, J.; Schmitz, C.; Averbeck, B.; Maier, M. Molekulare Grundlagen zur schmerzvermittelnden Wirkung extrakorporaler Stosswellen [Molecular basis for pain mediating properties of extracorporeal shock waves]. Schmerz 2004, 18, 492–497. (In German) [Google Scholar] [CrossRef]
- Hausdorf, J.; Lemmens, M.A.; Heck, K.D.; Grolms, N.; Korr, H.; Kertschanska, S.; Steinbusch, H.W.; Schmitz, C.; Maier, M. Selective loss of unmyelinated nerve fibers after extracorporeal shockwave application to the musculoskeletal system. Neuroscience 2008, 155, 138–144. [Google Scholar] [CrossRef]
- Barry, C.M.; Kestell, G.; Gillan, M.; Haberberger, R.V.; Gibbins, I.L. Sensory nerve fibers containing calcitonin gene-related peptide in gastrocnemius, latissimus dorsi and erector spinae muscles and thoracolumbar fascia in mice. Neuroscience 2015, 291, 106–117. [Google Scholar] [CrossRef]
- Schilder, A.; Magerl, W.; Klein, T.; Treede, R.D. Assessment of pain quality reveals distinct differences between nociceptive innervation of low back fascia and muscle in humans. Pain Rep. 2018, 3, e662. [Google Scholar] [CrossRef]
- Fede, C.; Petrelli, L.; Guidolin, D.; Porzionato, A.; Pirri, C.; Fan, C.; De Caro, R.; Stecco, C. Evidence of a new hidden neural network into deep fasciae. Sci. Rep. 2021, 11, 12623. [Google Scholar] [CrossRef]
- Stecco, A.; Gesi, M.; Stecco, C.; Stern, R. Fascial components of the myofascial pain syndrome. Curr. Pain Headache Rep. 2013, 17, 352. [Google Scholar] [CrossRef]
- Klingler, W.; Velders, M.; Hoppe, K.; Pedro, M.; Schleip, R. Clinical relevance of fascial tissue and dysfunctions. Curr. Pain Headache Rep. 2014, 18, 439. [Google Scholar] [CrossRef]
- Wilke, J.; Schleip, R.; Klingler, W.; Stecco, C. The Lumbodorsal Fascia as a Potential Source of Low Back Pain: A Narrative Review. Biomed Res. Int. 2017, 2017, 5349620. [Google Scholar] [CrossRef] [Green Version]
- Dommerholt, J. How have the views on myofascial pain and its treatment evolved in the past 20 years? From spray and stretch and injections to pain science, dry needling and fascial treatments. Pain Manag. 2020, 10, 63–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langevin, H.M. Fascia Mobility, Proprioception, and Myofascial Pain. Life 2021, 11, 668. [Google Scholar] [CrossRef] [PubMed]
- Notarnicola, A.; Moretti, B. The biological effects of extracorporeal shock wave therapy (eswt) on tendon tissue. Muscles Ligaments Tendons J. 2012, 2, 33–37. [Google Scholar] [PubMed]
- Yalcin, E.; Keskin Akca, A.; Selcuk, B.; Kurtaran, A.; Akyuz, M. Effects of extracorporal shock wave therapy on symptomatic heel spurs: A correlation between clinical outcome and radiologic changes. Rheumatol. Int. 2012, 32, 343–347. [Google Scholar] [CrossRef]
- Ogden, J.A.; Toth-Kischkat, A.; Schultheiss, R. Principles of shock wave therapy. Clin. Orthop. Relat. Res. 2001, 387, 8–17. [Google Scholar] [CrossRef]
- McClure, S.; Dorfmüller, C. Extracorporeal shock wave therapy: Theory and equipment. Clin. Tech. Equine Pract. 2003, 2, 348–357. [Google Scholar] [CrossRef] [Green Version]
- Ciampa, A.R.; de Prati, A.C.; Amelio, E.; Cavalieri, E.; Persichini, T.; Colasanti, M.; Musci, G.; Marlinghaus, E.; Suzuki, H.; Mariotto, S. Nitric oxide mediates anti-inflammatory action of extracorporeal shock waves. FEBS Lett. 2005, 579, 6839–6845. [Google Scholar] [CrossRef]
- Wang, C.; Wang, F.; Yang, K. Biological effects of extracorporeal shockwave in bone healing: A study in rabbits. Arch. Orthop. Trauma Surg. 2008, 128, 879–884. [Google Scholar] [CrossRef]
- Wang, C.J.; Yang, Y.J.; Huang, C.C. The effects of shockwave on systemic concentrations of nitric oxide level, angiogenesis and osteogenesis factors in hip necrosis. Rheumatol. Int. 2011, 31, 871–877. [Google Scholar] [CrossRef]
- Chen, Y.J.; Wang, C.J.; Yang, K.D.; Kuo, Y.R.; Huang, H.C.; Huang, Y.T.; Sun, Y.C.; Wang, F.S. Extracorporeal shock waves promote healing of collagenase-induced Achilles tendinitis and increase TGF-beta1 and IGF-I expression. J. Orthop. Res. 2004, 22, 854–861. [Google Scholar] [CrossRef]
- Zhang, D.; Kearney, C.J.; Cheriyan, T.; Schmid, T.M.; Spector, M. Extracorporeal shockwave-induced expression of lubricin in tendons and septa. Cell Tissue Res. 2011, 346, 255–262. [Google Scholar] [CrossRef]
- Zhang, H.; Li, Z.L.; Yang, F.; Zhang, Q.; Su, X.Z.; Li, J.; Zhang, N.; Liu, C.H.; Mao, N.; Zhu, H. Radial shockwave treatment promotes human mesenchymal stem cell self-renewal and enhances cartilage healing. Stem Cell Res. Ther. 2018, 9, 54. [Google Scholar] [CrossRef]
- Wang, F.S.; Wang, C.J.; Sheen-Chen, S.M.; Kuo, Y.R.; Chen, R.F.; Yang, K.D. Superoxide mediates shock wave induction of ERK-dependent osteogenic transcription factor (CBFA I) and mesenchymal cell differentiation toward osteoprogenitors. J. Biol. Chem. 2002, 277, 10931–10937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, F.S.; Yang, K.D.; Kuo, Y.R.; Wang, C.J.; Sheen-Chen, S.M.; Huang, H.C.; Chen, Y.J. Temporal and spatial expression of bone morphogenetic proteins in extracorporeal shock wave-promoted healing of segmental defect. Bone 2003, 32, 387–396. [Google Scholar] [CrossRef]
- Suhr, F.; Delhasse, Y.; Bungartz, G.; Schmidt, A.; Pfannkuche, K.; Bloch, W. Cell biological effects of mechanical stimulations generated by focused extracorporeal shock wave applications on cultured human bone marrow stromal cells. Stem Cell Res. 2013, 11, 951–964. [Google Scholar] [CrossRef] [Green Version]
- Vetrano, M.; D’Alessandro, F.; Torrisi, M.R.; Ferretti, A.; Vulpiani, M.C.; Visco, V. Extracorporeal shock wave therapy promotes cell proliferation and collagen synthesis of primary cultured human tenocytes. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Aschermann, I.; Noor, S.; Venturelli, S.; Sinnberg, T.; Mnich, C.D.; Busch, C. Extracorporal Shock Waves Activate Migration, Proliferation and Inflammatory Pathways in Fibroblasts and Keratinocytes, and Improve Wound Healing in an Open-Label, Single-Arm Study in Patients with Therapy-Refractory Chronic Leg Ulcers. Cell. Physiol. Biochem. 2017, 41, 890–906. [Google Scholar] [CrossRef]
- Liu, T.; Shindel, A.W.; Lin, G.; Lue, T.F. Cellular signaling pathways modulated by low-intensity extracorporeal shock wave therapy. Int. J. Impot. Res. 2019, 31, 170–176. [Google Scholar] [CrossRef]
- Adstrum, S.; Hedley, G.; Schleip, R.; Stecco, C.; Yucesoy, C.A. Defining the fascial system. J. Bodyw. Mov. Ther. 2017, 21, 173–177. [Google Scholar] [CrossRef]
- Fede, C.; Pirri, C.; Fan, C.; Petrelli, L.; Guidolin, D.; De Caro, R.; Stecco, C. A Closer Look at the Cellular and Molecular Components of the Deep/Muscular Fasciae. Int. J. Mol. Sci. 2021, 22, 1411. [Google Scholar] [CrossRef]
- Natale, G.; Condino, S.; Soldani, P.; Fornai, F.; Mattioli Belmonte, M.; Gesi, M. Natale et.al.’s response to Stecco’s fascial nomenclature editorial. J. Bodyw. Mov. Ther. 2014, 18, 588–590. [Google Scholar] [CrossRef] [PubMed]
- Stecco, C.; Porzionato, A.; Lancerotto, L.; Stecco, A.; Macchi, V.; Day, J.A.; De Caro, R. Histological study of the deep fasciae of the limbs. J. Bodyw. Mov. Ther. 2008, 12, 225–230. [Google Scholar] [CrossRef]
- Stecco, C.; Macchi, V.; Porzionato, A.; Duparc, F.; De Caro, R. The fascia: The forgotten structure. Ital. J. Anat. Embryol. 2011, 116, 127–138. [Google Scholar]
- Amir, A.; Kim, S.; Stecco, A.; Jankowski, M.P.; Raghavan, P. Hyaluronan homeostasis and its role in pain and muscle stiffness. PM R 2022. [Google Scholar] [CrossRef]
- Pratt, R.L. Hyaluronan and the fascial frontier. Int. J. Mol. Sci. 2021, 22, 6845. [Google Scholar] [CrossRef]
- Weiss, K.; Kalichman, L. Deep fascia as a potential source of pain: A narrative review. J. Bodyw. Mov. Ther. 2021, 28, 82–86. [Google Scholar] [CrossRef]
- Langevin, H.M.; Fox, J.R.; Koptiuch, C.; Badger, G.J.; Greenan-Naumann, A.C.; Bouffard, N.A.; Konofagou, E.E.; Lee, W.N.; Triano, J.J.; Henry, S.M. Reduced thoracolumbar fascia shear strain in human chronic low back pain. BMC Musculoskelet. Disord. 2011, 12, 203. [Google Scholar] [CrossRef]
- Stecco, C.; Pirri, C.; Fede, C.; Fan, C.; Giordani, F.; Stecco, L.; Foti, C.; De Caro, R. Dermatome and fasciatome. Clin. Anat. 2019, 32, 896–902. [Google Scholar] [CrossRef]
- Mense, S. Innervation of the thoracolumbar fascia. Eur. J. Transl. Myol. 2019, 29, 8297. [Google Scholar] [CrossRef]
- Stilwell, D.L. Regional variations in the innervation of deep fasciae and aponeuroses. Anat. Rec. 1957, 127, 635–653. [Google Scholar] [CrossRef]
- Hirsch, C.; Ingelmark, B.E.; Miller, M. The anatomical basis for low back pain. Studies on the presence of sensory nerve endings in ligamentous, capsular and intervertebral disc structures in the human lumbar spine. Acta Orthop. Scand. 1963, 33, 1–17. [Google Scholar] [CrossRef]
- Yahia, L.; Rhalmi, S.; Newman, N.; Isler, M. Sensory innervation of human thoracolumbar fascia. An immunohistochemical study. Acta Orthop. Scand. 1992, 63, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Stecco, C.; Gagey, O.; Belloni, A.; Pozzuoli, A.; Porzionato, A.; Macchi, V.; Aldegheri, R.; De Caro, R.; Delmas, V. Anatomy of the deep fascia of the upper limb. Second part: Study of innervation. Morphologie 2007, 91, 38–43. [Google Scholar] [CrossRef]
- Tesarz, J.; Hoheisel, U.; Wiedenhöfer, B.; Mense, S. Sensory innervation of the thoracolumbar fascia in rats and humans. Neuroscience 2011, 194, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Mense, S.; Hoheisel, U. Evidence for the existence of nociceptors in rat thoracolumbar fascia. J. Bodyw. Mov. Ther. 2016, 20, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, T.; Yasui, M.; Kubo, A.; Abe, M.; Kiyama, H.; Yamanaka, A.; Mizumura, K. Nociception originating from the crural fascia in rats. Pain 2013, 154, 1103–1114. [Google Scholar] [CrossRef] [PubMed]
- Hoheisel, U.; Rosner, J.; Mense, S. Innervation changes induced by inflammation of the rat thoracolumbar fascia. Neuroscience 2015, 300, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Corey, S.M.; Vizzard, M.A.; Badger, G.J.; Langevin, H.M. Sensory innervation of the nonspecialized connective tissues in the low back of the rat. Cells Tissues Organs 2011, 194, 521–530. [Google Scholar] [CrossRef] [Green Version]
- Basbaum, A.I.; Bautista, D.M.; Scherrer, G.; Julius, D. Cellular and molecular mechanisms of pain. Cell 2009, 139, 267–284. [Google Scholar] [CrossRef] [Green Version]
- Fede, C.; Porzionato, A.; Petrelli, L.; Fan, C.; Pirri, C.; Biz, C.; De Caro, R.; Stecco, C. Fascia and soft tissues innervation in the human hip and their possible role in post-surgical pain. J. Orthop. Res. 2020, 38, 1646–1654. [Google Scholar] [CrossRef]
- Marpalli, S.; Rao, K.G.; Venkatesan, P.; George, B.M. The morphological and microscopical characteristics of posterior layer of human thoracolumbar fascia; A potential source of low back pain. Morphologie 2021, 105, 308–315. [Google Scholar] [CrossRef]
- Gibson, W.; Arendt-Nielsen, L.; Taguchi, T.; Mizumura, K.; Graven-Nielsen, T. Increased pain from muscle fascia following eccentric exercise: Animal and human findings. Exp. Brain Res. 2009, 194, 299–308. [Google Scholar] [CrossRef]
- Schilder, A.; Hoheisel, U.; Magerl, W.; Benrath, J.; Klein, T.; Treede, R.D. Sensory findings after stimulation of the thoracolumbar fascia with hypertonic saline suggest its contribution to low back pain. Pain 2014, 155, 222–231. [Google Scholar] [CrossRef]
- Schilder, A.; Magerl, W.; Hoheisel, U.; Klein, T.; Treede, R.D. Electrical high-frequency stimulation of the human thoracolumbar fascia evokes long-term potentiation-like pain amplification. Pain 2016, 157, 2309–2317. [Google Scholar] [CrossRef]
- Vogel, S.; Magerl, W.; Treede, R.-D.; Schilder, A. Dose-Dependent Pain and Pain Radiation after Chemical Stimulation of the Thoracolumbar Fascia and Multifidus Muscle: A Single-Blinded, Cross-Over Study Revealing a Higher Impact of Fascia Stimulation. Life 2022, 12, 340. [Google Scholar] [CrossRef]
- Bednar, D.A.; Orr, F.W.; Simon, G.T. Observations on the pathomorphology of the thoracolumbar fascia in chronic mechanical back pain. A microscopic study. Spine 1995, 20, 1161–1164. [Google Scholar] [CrossRef]
- Sanchis-Alfonso, V.; Roselló-Sastre, E. Immunohistochemical analysis for neural markers of the lateral retinaculum in patients with isolated symptomatic patellofemoral malalignment. A neuroanatomic basis for anterior knee pain in the active young patient. Am. J. Sports Med. 2000, 28, 725–731. [Google Scholar] [CrossRef]
- Stecco, C.; Macchi, V.; Barbieri, A.; Tiengo, C.; Porzionato, A.; De Caro, R. Hand fasciae innervation: The palmar aponeurosis. Clin. Anat. 2018, 31, 677–683. [Google Scholar] [CrossRef]
- Schubert, T.E.; Weidler, C.; Borisch, N.; Schubert, C.; Hofstädter, F.; Straub, R.H. Dupuytren’s contracture is associated with sprouting of substance P positive nerve fibres and infiltration by mast cells. Ann. Rheum. Dis. 2006, 65, 414–415. [Google Scholar] [CrossRef] [Green Version]
- Hoheisel, U.; Taguchi, T.; Treede, R.D.; Mense, S. Nociceptive input from the rat thoracolumbar fascia to lumbar dorsal horn neurones. Eur. J. Pain 2011, 15, 805–810. [Google Scholar] [CrossRef]
- Hoheisel, U.; Mense, S. Inflammation of the thoracolumbar fascia excites and sensitizes rat dorsal horn neurons. Eur. J. Pain 2015, 19, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Hoheisel, U.; Koch, K.; Mense, S. Functional reorganization in the rat dorsal horn during an experimental myositis. Pain 1994, 59, 111–118. [Google Scholar] [CrossRef]
- Taguchi, T.; Hoheisel, U.; Mense, S. Dorsal horn neurons having input from low back structures in rats. Pain 2008, 138, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Rompe, J.D.; Hopf, C.; Nafe, B.; Burger, R. Low-energy extracorporeal shock wave therapy for painful heel: A prospective controlled single-blind study. Arch. Orthop. Trauma Surg. 1996, 115, 75–91. [Google Scholar] [CrossRef]
- Rompe, J.D.; Hope, C.; Küllmer, K.; Heine, J.; Bürger, R. Analgesic effect of extracorporeal shock-wave therapy on chronic tennis elbow. J. Bone Jt. Surg. Br. 1996, 78, 233–237. [Google Scholar] [CrossRef] [Green Version]
- Buch, M.; Knorr, U.; Fleming, L.; Theodore, G.; Amendola, A.; Bachmann, C.; Zingas, C.; Siebert, W.E. Extracorporeal shockwave therapy in plantar fasciitis—3 months results of a multicentre prospective randomised double blind placebo controlled trial. Orthopäde 2002, 31, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Muller-Ehrenberg, H.; Licht, G. Diagnosis and therapy of myofascial pain syndrome with focused shock waves. Med. Orthop. Tech. 2005, 5, 1–6. [Google Scholar]
- Seok, H.; Kim, S.H. The effectiveness of extracorporeal shock wave therapy vs. local steroid injection for management of carpal tunnel syndrome: A randomized controlled trial. Am. J. Phys. Med. Rehabil. 2013, 92, 327–334. [Google Scholar] [CrossRef]
- Zheng, Z.; Gao, Q.; Wang, J. Effect of pneumatically ballistic extracorporeal shockwave on chronic nonspecific low back pain. Chin. J. Rehabil. Theory Pract. 2013, 19, 666–668. [Google Scholar]
- Gür, A.; Koca, I.; Karagüllü, H.; Altindag, O.; Madenci, E.; Tutoglu, A.; Boyaci, A.; Isik, M. Comparison of the effectiveness of two different extracorporeal shock wave therapy regimens in the treatment of patients with myofascial pain syndrome. Arch. Rheumatol. 2014, 29, 186–193. [Google Scholar] [CrossRef] [Green Version]
- Walewicz, K.; Taradaj, J.; Rajfur, K.; Ptaszkowski, K.; Kuszewski, M.T.; Sopel, M.; Dymarek, R. The effectiveness of radial extracorporeal shock wave therapy in patients with chronic low back pain: A prospective, randomized, single-blinded pilot Study. Clin. Interv. Aging 2019, 14, 1859–1869. [Google Scholar] [CrossRef] [Green Version]
- Leão, R.G.; Azuma, M.M.; Ambrosio, G.H.C.; Faloppa, F.; Takimoto, E.S.; Tamaoki, M.J.S. Effectiveness of shockwave therapy in the treatment of plantar fasciitis. Acta Ortop. Bras. 2020, 28, 7–11. [Google Scholar] [CrossRef]
- Guo, X.; Li, L.; Yan, Z.; Li, Y.; Peng, Z.; Yang, Y.; Zhang, Y.; Schmitz, C.; Feng, Z. Efficacy and safety of treating chronic nonspecific low back pain with radial extracorporeal shock wave therapy (rESWT), rESWT combined with celecoxib and eperisone (C + E) or C + E alone: A prospective, randomized trial. J. Orthop. Surg. Res. 2021, 16, 705. [Google Scholar] [CrossRef]
- Rompe, J.D.; Decking, J.; Schoellner, C.; Nafe, B. Shock wave application for chronic plantar fasciitis in running athletes. A prospective, randomized, placebo-controlled trial. Am. J. Sports Med. 2003, 31, 268–275. [Google Scholar] [CrossRef]
- Rompe, J.D.; Kirkpatrick, C.J.; Küllmer, K.; Schwitalle, M.; Krischek, O. Dose-related effects of shock waves on rabbit tendo Achillis. A sonographic and histological study. J. Bone Jt. Surg. Br. 1998, 80, 546–552. [Google Scholar] [CrossRef]
- Takahashi, N.; Wada, Y.; Ohtori, S.; Saisu, T.; Moriya, H. Application of shock waves to rat skin decreases calcitonin gene-related peptide immunoreactivity in dorsal root ganglion neurons. Auton. Neurosci. 2003, 107, 81–84. [Google Scholar] [CrossRef]
- Maier, M.; Averbeck, B.; Milz, S.; Refior, H.J.; Schmitz, C. Substance P and prostaglandin E2 release after shock wave application to the rabbit femur. Clin. Orthop. Relat. Res. 2003, 406, 237–245. [Google Scholar] [CrossRef]
- Bolt, D.M.; Burba, D.J.; Hubert, J.D.; Strain, G.M.; Hosgood, G.L.; Henk, W.G.; Cho, D.-Y. Determination of functional and morphologic changes in palmar digital nerves after nonfocused extracorporeal shock wave treatment in horses. Am. J. Vet. Res. 2004, 65, 1714–1718. [Google Scholar] [CrossRef]
- Trager, L.R.; Funk, R.A.; Clapp, K.S.; Dahlgren, L.A.; Werre, S.R.; Hodgson, D.R.; Pleasant, R.S. Extracorporeal shockwave therapy raises mechanical nociceptive threshold in horses with thoracolumbar pain. Equine Vet. J. 2020, 52, 250–257. [Google Scholar] [CrossRef]
- Hausdorf, J.; Lemmens, M.A.M.; Kaplan, S.; Marangoz, C.; Milz, S.; Odaci, E.; Korr, H.; Schmitz, C.; Maier, M. Extracorporeal shockwave application to the distal femur of rabbits diminishes the number of neurons immunoreactive for substance P in dorsal root ganglia L5. Brain Res. 2008, 1207, 96–101. [Google Scholar] [CrossRef]
- Ochiai, N.; Ohtori, S.; Sasho, T.; Nakagawa, K.; Takahashi, K.; Takahashi, N.; Murata, R.; Takahashi, K.; Moriya, H.; Wada, Y.; et al. Extracorporeal shock wave therapy improves motor dysfunction and pain originating from knee osteoarthritis in rats. Osteoarthr. Cartil. 2007, 15, 1093–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueberle, F. Shock wave technology. In Extracorporeal Shock Waves in Orthopaedics, 1st ed.; Siebert, W., Buch, M., Eds.; Springer: Berlin/Heidelberg, Germany, 1998; pp. 59–87. [Google Scholar]
- Haake, M.; Thon, A.; Bette, M. Absence of spinal response to extracorporeal shock waves on the endogenous opioid systems in the rat. Ultrasound Med. Biol. 2001, 27, 279–284. [Google Scholar] [CrossRef]
- Haake, M.; Thon, A.; Bette, M. No influence of low-energy extracorporeal shock wave therapy (ESWT) on spinal nociceptive systems. J. Orthop. Sci. 2002, 7, 97–101. [Google Scholar] [CrossRef]
- Klonschinski, T.; Ament, S.J.; Schlereth, T.; Rompe, J.D.; Birklein, F. Application of local anesthesia inhibits effects of low-energy extracorporeal shock wave treatment (ESWT) on nociceptors. Pain Med. 2011, 12, 1532–1537. [Google Scholar] [CrossRef] [PubMed]
- Manganotti, P.; Amelio, E.; Guerra, C. Shock wave over hand muscles: A neurophysiological study on peripheral conduction nerves in normal subjects. Muscles Ligaments Tendons J. 2012, 2, 104–107. [Google Scholar]
- Dahmen, G.P.; Meiss, L.; Nam, V.C.; Skruodies, B. Extrakorporale Stosswellentherapie (ESWT) im knochennahen Weichteilbereich an der Schulter. Extr. Orthop. 1992, 11, 25–27. (In German) [Google Scholar]
- Mokhtar, M.; Singh, P. Neuroanatomy, Periaqueductal Gray. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Physical Characteristics | fSW | rSW |
|---|---|---|
| Wave propagation | Focused | Radial |
| Pressure | Up to 100 MPa | 0.1 to 1 MPa |
| Pulse duration | Does not exceed 2 μs | 1 to 5 ms |
| Penetration power | Up to 10–12 cm | Less than 3 cm |
| Force of impact | 0.001–0.4 mJ/mm EFD4 > 0.1 mJ/mm (low-energy shock waves) EFD of 0.2 to 0.4 mJ/mm2 (high-energy shock waves) | 0.02–0.06 mJ/mm2 |
| Energy profile | Rapid rise and fall of the pressure wave | Slower rise and fall of pressure |
| Target | Skin, muscles, bones | Skin, muscles |
| Pathological Condition (s) | n | Main Finding (s) | Ref. |
|---|---|---|---|
| Chronic proximal PF * | 302 patients | Successful result by all four of the evaluation criteria (pain assessment, subject’s self-assessment of pain on first walking in the morning, subject’s self-assessment of activity, use of pain medications) in 56% more of the treated patients 3 months after one treatment | [11] |
| Chronic PF | 112 patients | Decrease in score for pain caused by manual pressure (VAS score from 77 points before treatment to 19 points at 6 months); 25/49 patients able to walk completely without pain | [12] |
| MPS ‡ in upper trapezius | 22 patients | Significant decrease in VAS score from 4.91 ± 1.76 to 2.27 ± 1.27; significant increase in pressure threshold from 40.4 ± 9.94 N to 61.2 ± 12.16 N in the treated group | [31] |
| Painful heel associated with calcaneal spurs | 30 patients | Significant alleviation of pain and improvement of function at all follow-ups in treatment group (improvement rating 72.9% at 6 weeks, and 77.4% at 24 weeks) | [116] |
| Chronic tennis elbow | 100 patients | Significant alleviation of pain and improvement of function after treatment, with a good or excellent outcome in 48% and an acceptable result in 42% at 24 weeks | [117] |
| MTrPs # | 30 patients | Significant decrease in VAS score after 3 months’ treatment in 95% of patients (from 3.6 prior to therapy to 1.7 after therapy) | [119] |
| Carpal tunnel syndrome | 36 patients | Significant reduction in VAS and symptom severity score on the Levine Self-assessment Questionnaire at 1 and 3 months after treatment | [120] |
| Chronic nonspecific low back pain | 66 patients | Significant reduction in the VAS score after 2 weeks of therapy (from 6.32 ± 1.12 prior to therapy to 2.96 ± 1.00 after therapy) | [121] |
| Active myofascial trigger points in the trapezius muscle | 64 patients | Statistically significant improvements in the number of trigger points, pain, quality of life, and anxiety scores of patients in both groups (i.e., group I = patients undergoing a single session of low-energy; group II = patients undergoing three sessions of ESWT with the same energy density, with one-week intervals) at 3 and 12 weeks after treatment | [122] |
| Chronic Low Back Pain | 52 patients | An extremely strong analgesic effect in the group treated with rESWT and stabilization training (pain reduction in VAS scale from 4.4 to 2.7 points, on average, at one months and 2.0 points at three months after treatment) | [123] |
| PF | 56 patients | Progressive improvement in the three outcomes evaluated, assessed pain, function, and quality of life (VAS, AOFAS, and SF-36, respectively), at 3, 6, and 12 weeks | [124] |
| Chronic nonspecific low back pain | 140 patients | Significant lower mean numerical rating scale (NRS) values in patients treated with rESWT at 1, 3, and 4 weeks after treatment | [125] |
| Chronic PF | 45 running athletes | Significant reduction of self-reported pain on first walking in the morning, from an average of 6.9 to 2.1 points on a VAS † score after 6 months; further reduction of pain to an average 1.5 points after 12 months | [126] |
| Animal Model | Site of Application | Effect (s) | Ref. |
|---|---|---|---|
| Rat | Foot pad | Amplification of ESWT-induced denervation and pain relief following a repetitive application | [47] |
| Rat | Plantar skin of hind paw | Nearly complete degeneration of epidermal nerve fibers, as indicated by the significant loss of PGP9.5 and CGRP immunoreactivity | [51] |
| Rat | Skin of footpads (corresponding to L4 and L5 dermatomes) | Injury of sensory nerve fibers, as indicated by the significant increase in the number of ATF3-ir * DRG § neurons | [53] |
| Rabbit | Distal femur | Decrease in substance P release from the periosteum of the femur 6 weeks after ESWT application | [55] |
| Rabbit | Ventral side of the right distal femur | Selective and substantial loss of unmyelinated nerve fibers within the femoral nerve of treated hind limb | [56] |
| Rat | Foot pad of hind paw | Reduced CGRP expression in DRG neurons (the percentage of FG † -labeled CGRP-ir DRG neurons decreased to 18% in treated group) | [128] |
| Horse | Left forelimb | Significant lower SNCV ‡ in treated medial and lateral palmar digital nerves along with a severe disruption of myelin sheath | [130] |
| Horse | Skin from T12 to L5 | Three treatments of ESWT 2 weeks apart raised MNT # over a 56-day period in horses with back pain | [131] |
| Rabbit | Ventral side of the right distal femur | Significant decrease in the mean number of SP-ir neurons within DRG L5 | [132] |
| Rat | Hindlimb | Reduction of CGRP-ir DRG neurons innervating the knee in the osteoarthritis model | [133] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryskalin, L.; Morucci, G.; Natale, G.; Soldani, P.; Gesi, M. Molecular Mechanisms Underlying the Pain-Relieving Effects of Extracorporeal Shock Wave Therapy: A Focus on Fascia Nociceptors. Life 2022, 12, 743. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050743
Ryskalin L, Morucci G, Natale G, Soldani P, Gesi M. Molecular Mechanisms Underlying the Pain-Relieving Effects of Extracorporeal Shock Wave Therapy: A Focus on Fascia Nociceptors. Life. 2022; 12(5):743. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050743
Chicago/Turabian StyleRyskalin, Larisa, Gabriele Morucci, Gianfranco Natale, Paola Soldani, and Marco Gesi. 2022. "Molecular Mechanisms Underlying the Pain-Relieving Effects of Extracorporeal Shock Wave Therapy: A Focus on Fascia Nociceptors" Life 12, no. 5: 743. https://0-doi-org.brum.beds.ac.uk/10.3390/life12050743