
SEM-EDX Study of the Degradation Process of Two Xenograft Materials Used in Sinus Lift Procedures

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Results
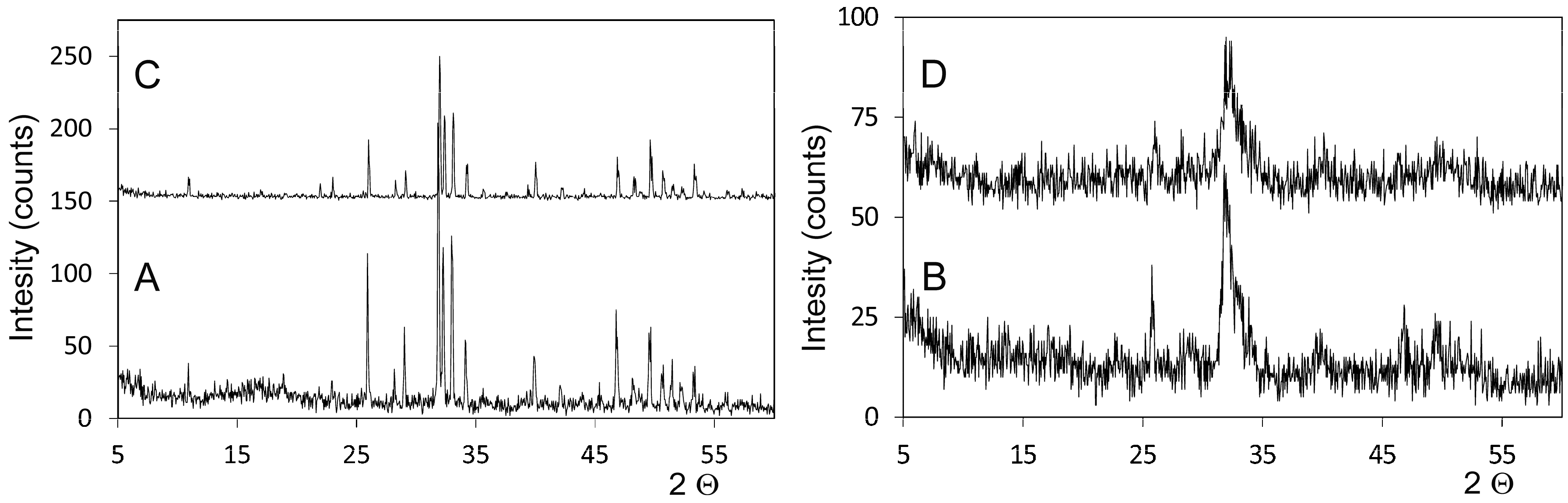
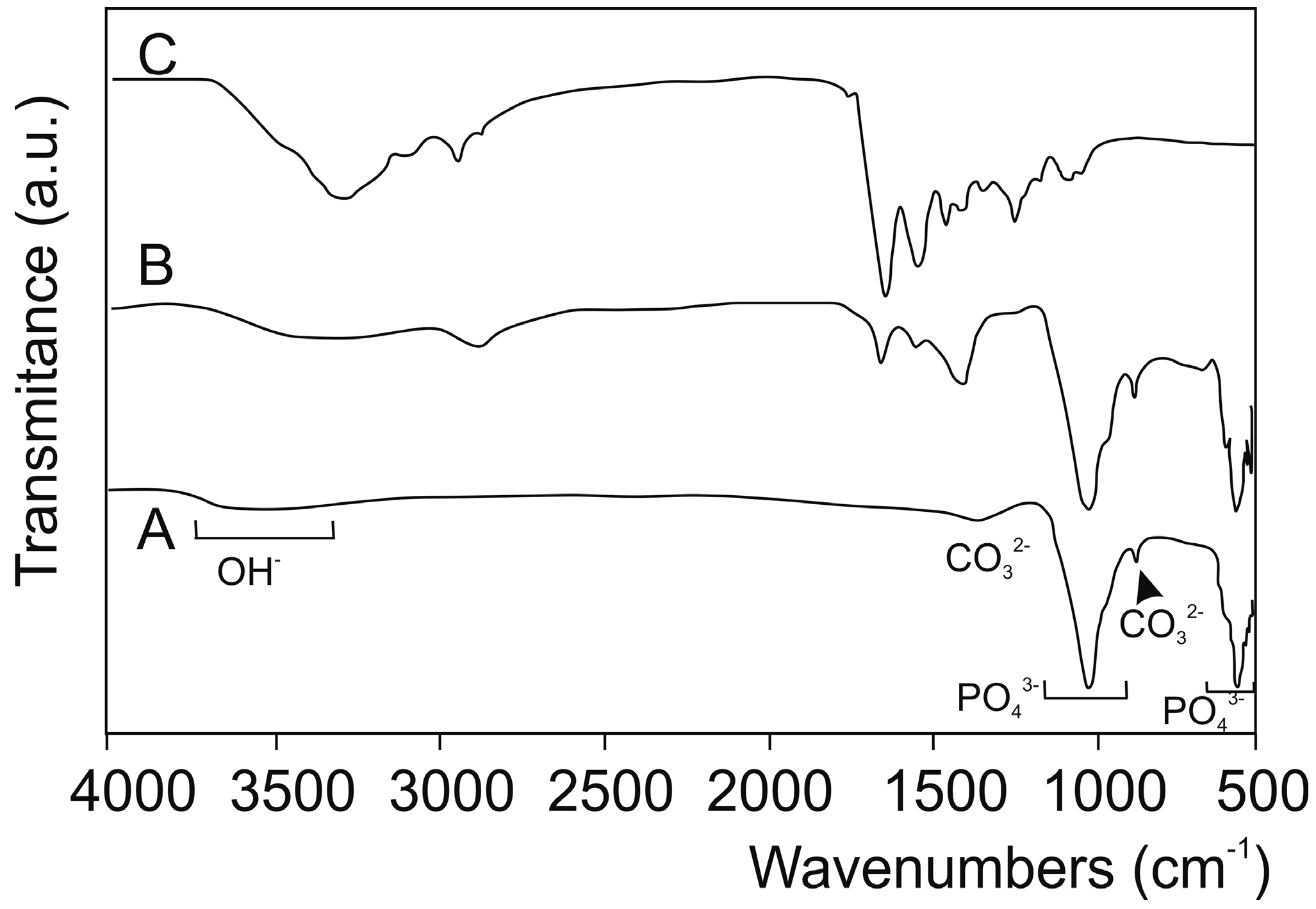
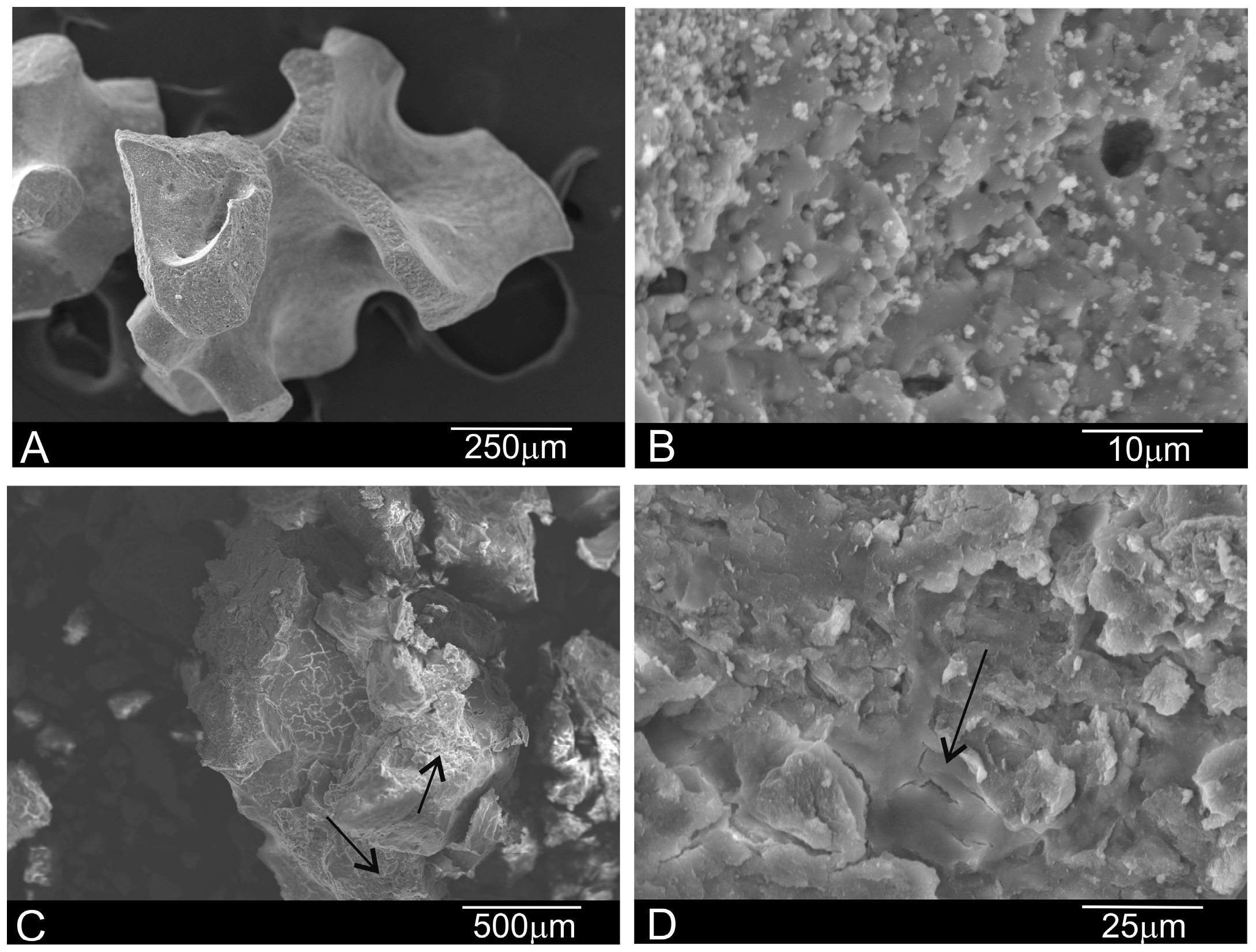
2.1. Characterization of Deproteinized Hydroxyapatite Materials
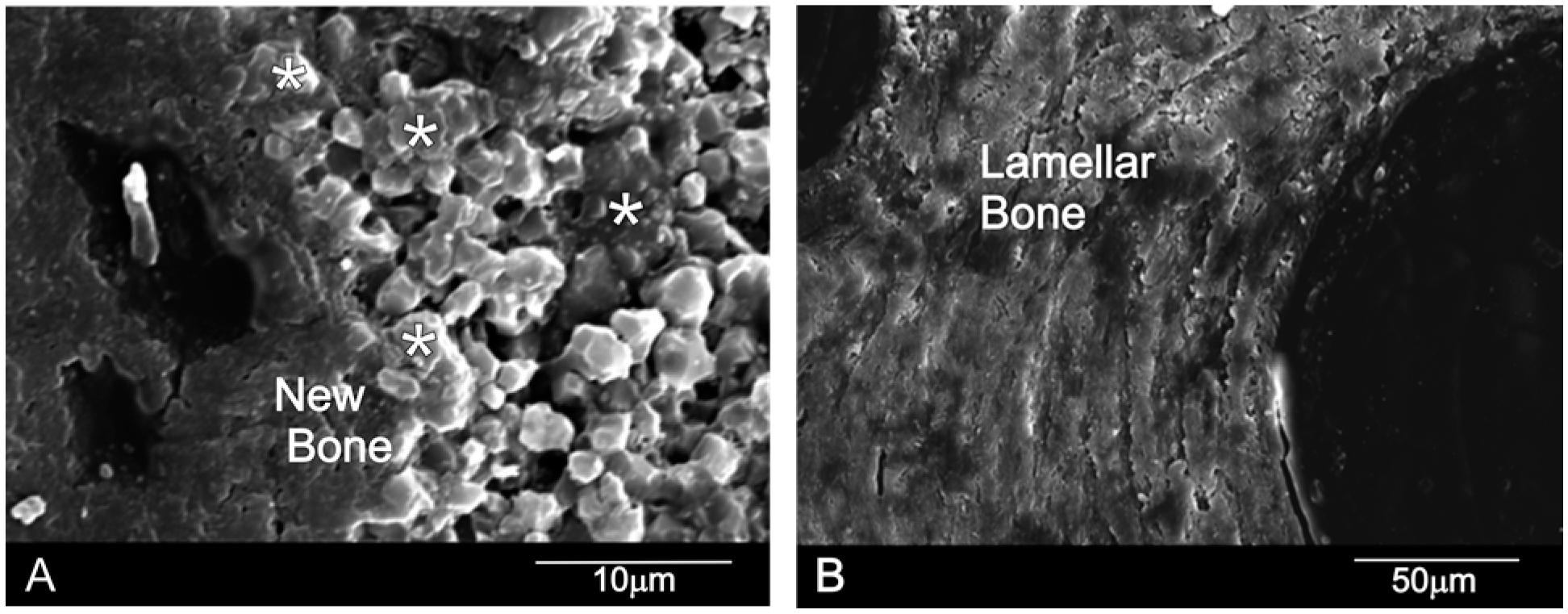
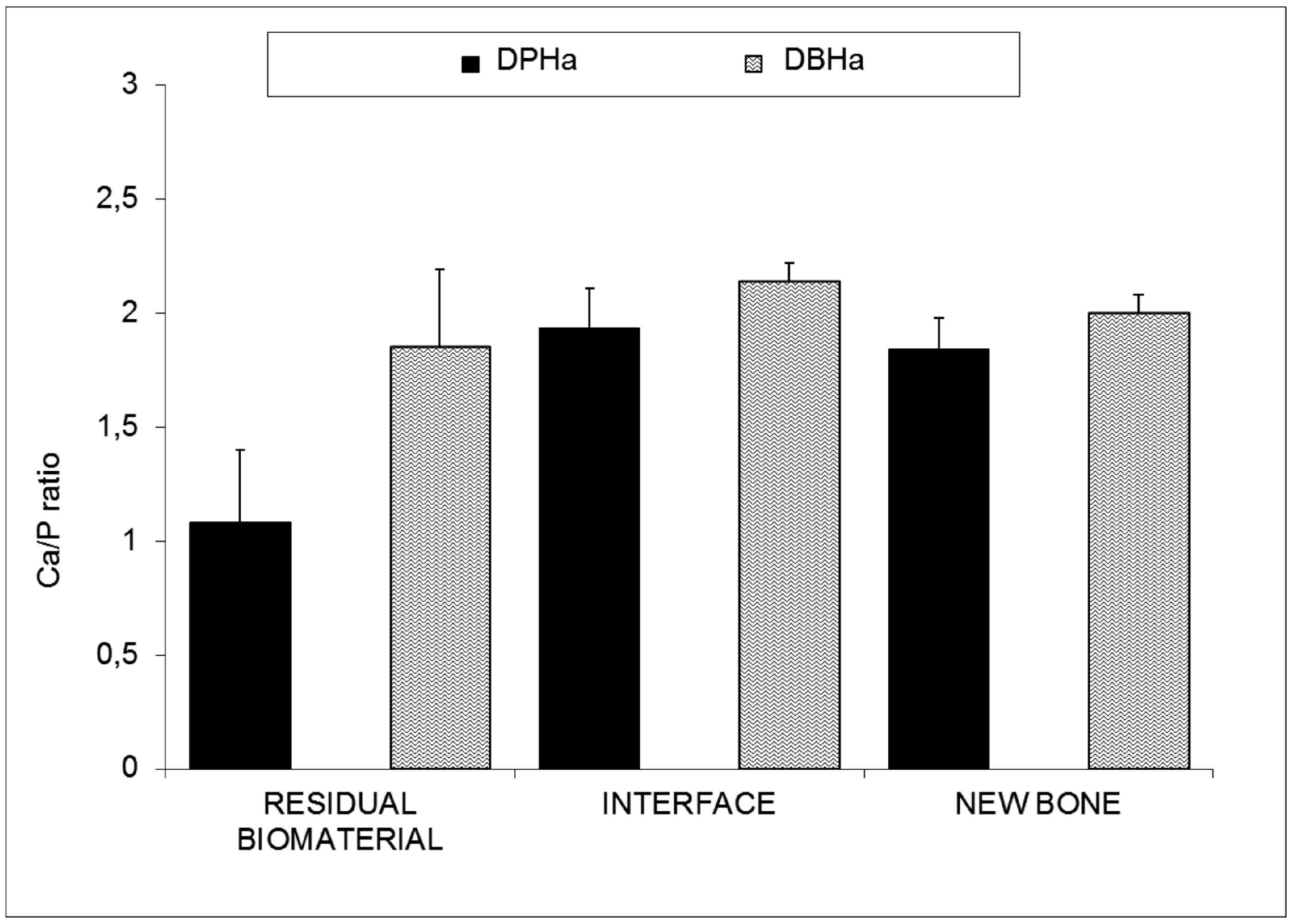
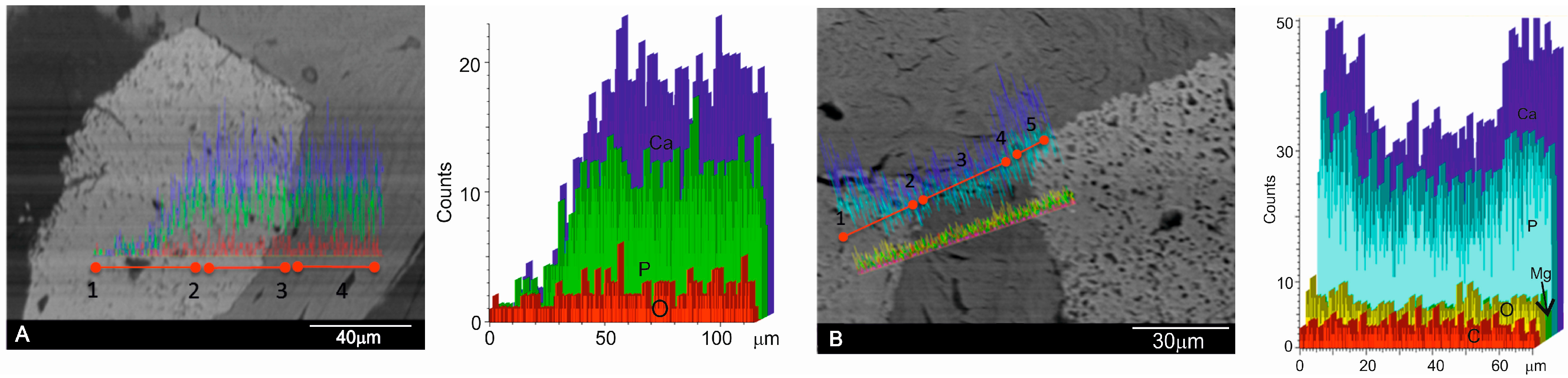
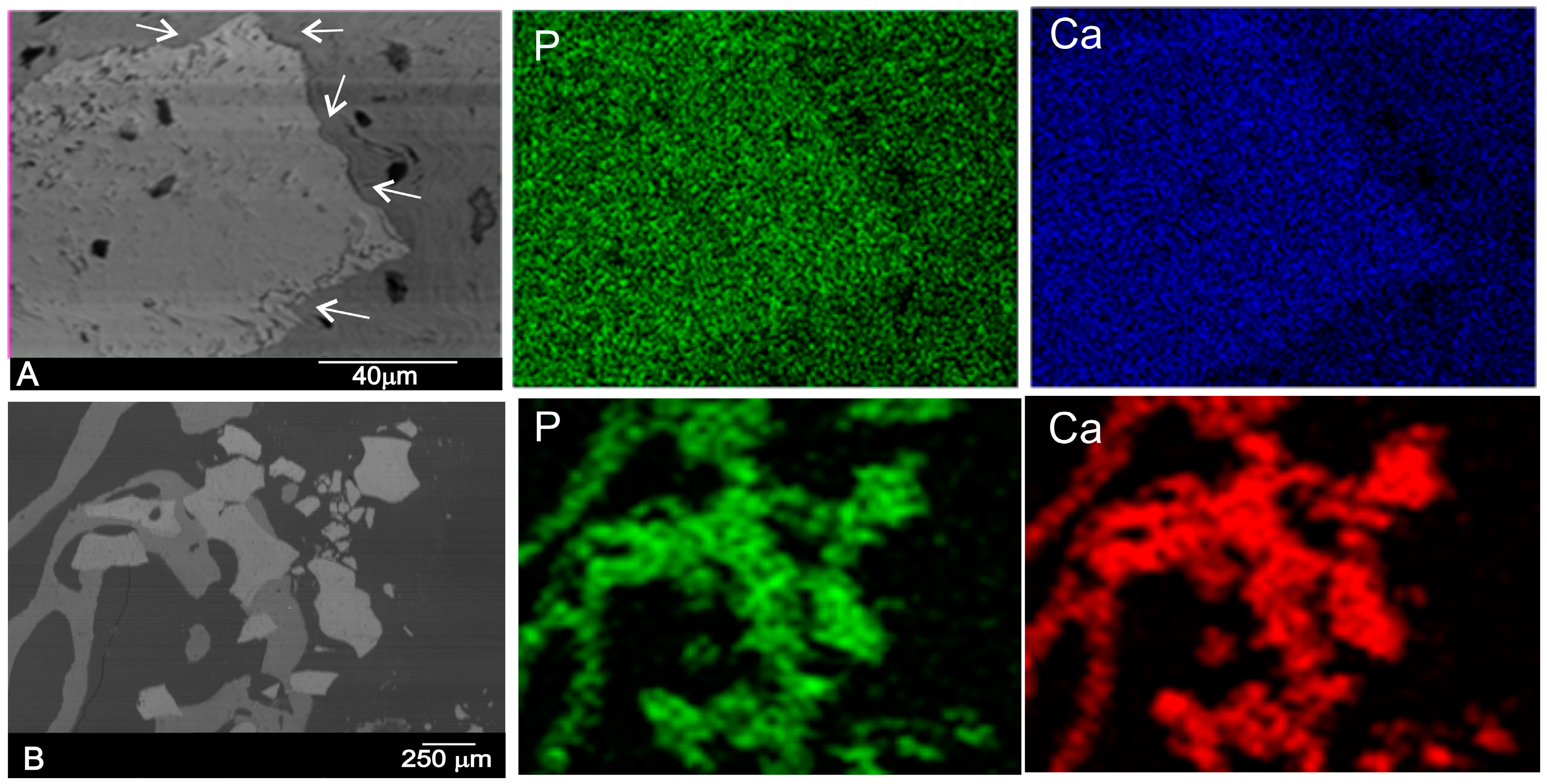
2.2. Results of Retrieved Bone Biopsies
3. Discussion
4. Materials and Methods
4.1. Deprotenized Hydroxyapatite Materials
4.2. Surgery and Bone Retrieval
4.3. Specimen Preparation and Analysis
4.4. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Jang, H.Y.; Kim, H.C.; Lee, S.C.; Lee, J.Y. Choice of Graft Material in Relation to Maxillary Sinus Width in Internal Sinus Floor Augmentation. J. Oral Maxillofac. Surg. 2010, 68, 1859–1868. [Google Scholar] [CrossRef] [PubMed]
- Szpalski, C.; Wetterau, M.; Barr, J.; Warren, S.M. Bone tissue engineering: Current strategies and techniques–part I: Scaffolds. Tissue Eng. Part B Rev. 2012, 18, 246–257. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.S.; Aaboe, M.; Janner, S.F.; Saulacic, N.; Bornstein, M.M.; Bosshardt, D.D.; Buser, D. Influence of particle size of deproteinized bovine bone mineral on new bone formation and implant stability after simultaneous sinus floor elevation: A histomorphometric study in minipigs. Clin. Implant Dent. Relat. Res. 2015, 17, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Danesh-Sani, S.A.; Engebretson, S.P.; Janal, M.N. Histomorphometric results of different grafting materials and effect of healing time on bone maturation after sinus floor augmentation: A systematic review and meta-analysis. J. Periodontal. Res. 2016. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Shimizu, Y.; Asai, S.; Ooya, K. Experimental sinus grafting with the use of deproteinized bone particles of different sizes. Clin. Oral Implants Res. 2003, 14, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Burg, K.J.; Porter, S.; Kellam, J.F. Biomaterials development for bone tissue engineering. Biomaterials 2000, 21, 2347–2359. [Google Scholar] [CrossRef]
- De Aza, P.N.; De Aza, A.H.; De Aza, S. Crystalline bioceramic materials. Bol. Soc. Esp. Ceram. Vidr. 2005, 44, 135–145. [Google Scholar] [CrossRef]
- LeGeros, R.Z. Strategies to affect bone remodeling: Osteointegration. J. Bone Mineral Res. 1993, 8, 583–596. [Google Scholar] [CrossRef] [PubMed]
- Conz, M.B.; Granjeiro, J.M.; de Almeida Soares, G. Hydroxyapatite crystallinity does not affect the repair of critical size bone defects. J. Appl. Oral Sci. 2011, 19, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Guirado, J.L.; Ramirez-Fernandez, M.P.; Delgado-Ruiz, R.A.; Mate-Sanchez de Val, J.E.; Velasquez, P.; de Aza, P.N. Influence of biphasic α-TCP with and without the use of collagen membranes on bone healing of surgically critical size defects. A radiological, histological and histomorphometric study. Clin. Oral Implants Res. 2014, 25, 1228–1238. [Google Scholar] [CrossRef] [PubMed]
- Fulmer, M.T.; Ison, I.C.; Hankermayer, C.R.; Constantz, B.R.; Ross, J. Measurements of the solubilities and dissolution rates of several hydroxyapatite. Biomaterials 2002, 23, 751–755. [Google Scholar] [CrossRef]
- Mate-Sanchez de Val, J.E.; Calvo-Guirado, J.L.; Gomez Moreno, G.; Perez Albacete-Martinez, C.; Mazón, P.; de Aza, P.N. Influence of hydroxyapatite granule size, porosity and crystallinity on tissue reaction in vivo. Part A: Synthesis, characterization of the materials and SEM analysis. Clin. Oral Implants Res. 2016, 27, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Nkenke, E.; Stelzle, F. Clinical outcomes of sinus or augmentation for implant placement using autogenous bone or bone substitutes: A systematic review. Clin. Oral Implants Res. 2009, 20, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T.; Schou, S.; Stavropoulos, A.; Terheyden, H.; Holmstrup, P. Maxillary sinus floor augmentation with Bio-Oss or Bio-Oss mixed with autogenous bone as graft in animals: A systematic review. Int. J. Oral Maxillofac. Surg. 2012, 41, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Arasawa, M.; Oda, Y.; Kobayashi, T.; Uoshima, K.; Nishiyama, H.; Hoshina, H.; Saito, C. Evaluation of bone volume changes after sinus floor augmentation with autogenous bone grafts. Int. J. Oral Maxillofac. Surg. 2012, 41, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Sbordone, C.; Toti, P.; Guidetti, F.; Califano, L.; Bufo, P.; Sbordone, L. Volume changes of autogenous bone after sinus lifting and grafting procedures: A 6-year computerized tomographic follow-up. J. Craniomaxillofac. Surg. 2013, 41, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.P.; Wang, K.; Liu, C.S. Crystalline structure and its effects on the degradation of linear calcium polyphosphate bone substitute. Appl. Surf. Sci. 2008, 255, 270–272. [Google Scholar] [CrossRef]
- Traini, T.; Piattelli, A.; Caputi, S.; Degidi, M.; Mangano, C.; Scarano, A.; Perrotti, V.; Iezzi, G. Regeneration of human bone using different bone substitute biomaterials. Clin. Implant Dent. Relat. Res. 2015, 17, 150–162. [Google Scholar] [CrossRef] [PubMed]
- Frenken, J.W.; Bouwman, W.F.; Bravenboer, N.; Zijderveld, S.A.; Schulten, E.A.; ten Bruggenkate, C.M. The use of Straumanns Bone Ceramic in a maxillary sinus floor elevation procedure: A clinical, radiological, histological and histomorphometric evaluation with a 6-month healing period. Clin. Oral Implants Res. 2010, 21, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.V.; Serricella, P.; Linhares, A.B.; Guerdes, R.M.; Borojevic, R.; Rossi, M.A.; Duarte, M.E.; Farina, M. Characterization of a bovine collagen–hydroxyapatite composite scaffold for bone tissue engineering. Biomaterials 2003, 24, 4987–4997. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Ramirez-Fernandez, M.P.; Mate-Sanchez de Val, J.E.; Negri, B.; Velasquez, P.; de Aza, P.N. Enhanced bone regeneration with a novel synthetic bone substitute in combination with a new natural cross-linked collagen membrane: Radiographic and histomorphometric study. Clin. Oral Implants Res. 2015, 26, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Conz, M.B.; Granjeiro, J.M.; de Almeida Soares, G. Physicochemical characterization of six commercial hydroxyapatites for medical dental applications as bone graft. J. Appl. Oral Sci. 2005, 13, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Barakat, N.A.M.; Khalil, K.A.; Faheem, A.S.; Omran, A.M.; Gaihre, B.; Khil, S.M.; Kim, H.Y. Physiochemical characterizations of hydroxyapatite extracted from bovine bones by three different methods: Extraction of biologically desirable Hap. Mater. Sci. Eng. Part C 2008, 28, 1381–1387. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Mate-Sanchez de Val, J.E.; Delgado Ruiz, R.A.; Romanos, G.; De Aza, P.N.; Vélasquez, P. Bone neo-formation and mineral degradation of 4Bone® ParII: Histological and histomophometric analysis in critical size defects in rabbits. Clin. Oral Implants Res. 2015, 26, 1402–1406. [Google Scholar] [CrossRef] [PubMed]
- Manfro, R.; Fonseca, F.S.; Bortoluzzi, M.C.; Sendyk, W.R. Comparative, Histological and Histomorphometric Analysis of Three Anorganic Bovine Xenogenous Bone Substitutes: Bio-Oss, Bone-Fill and Gen-Ox Anorganic. J. Oral Maxillofac. Surg. 2014, 13, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Hutmacher, D.W.; Schantz, J.T.; Lam, C.X.; Tan, K.C.; Lim, T.C. State of the art and future directions of scaffold-based bone engineering from a biomaterials perspective. J. Tissue Eng. Regen. Med. 2007, 1, 245–260. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.L.; Faria, P.E.; Grisi, M.F.; Souza, S.L.; Taba, M.J.; Palioto, D.B.; Novaes, A.B.; Fraga, A.F.; Ozyegin, L.S.; Oktar, F.N.; et al. Effects of granule size on the osteoconductivity of bovine and synthetic hydroxyapatite: A histologic and histometric study in dogs. J. Oral Implantol. 2007, 33, 267–276. [Google Scholar] [CrossRef]
- Lee, J.S.; Shin, H.K.; Yun, J.H.; Cho, KS. Randomized clinical trial of maxillary sinus grafting using deproteinized porcine and bovine bone mineral. Clin. Implant Dent. Relat. Res. 2016. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, Z.; Weesner, T.; van Dijk, S.; Cochran, D.L.; Mellonig, J.T.; Lohmann, C.H.; Carnes, D.L.; Goldstein, M.; Dean, D.D.; Boyan, B.D. Ability of deproteinized cancellous bovine bone to induce new bone formation. J. Periodontol. 2000, 71, 1258–1269. [Google Scholar] [CrossRef] [PubMed]
- Azran, Y.M.; Idris, B.; Rusnah, M.; Rohaida, C.H. Hap physical investigation the effect of sintering temperature. Med. J. Malays. 2004, 59, 79–80. [Google Scholar] [PubMed]
- Kalkura, S.N.; Anee, T.K.; Ashok, M.; Betzel, C. Investigations on the synthesis and crystallization of hydroxyapatite at low temperature. Bio.-Med. Mater. Eng. 2004, 1, 581–592. [Google Scholar] [PubMed]
- Herliansyah, M.K.; Hamdia, M.; de-Ektessabic, A.I.; Wildanb, M.W.; Toque, J.A. The influence of sintering temperature on the properties of compacted bovine. Mater. Sci. Eng. C 2009, 29, 1674–1680. [Google Scholar] [CrossRef]
- Poinern, G.J.; Brundavanam, R.; Le, X.T.; Djordjevic, S.; Prokic, M.; Fawcett, D. Thermal and ultrasonic influence in the formation of nanometer scale hydroxyapatite bio-ceramic. Int. J. Nanomed. 2011, 6, 2083–2095. [Google Scholar] [CrossRef] [PubMed]
- Maté Sánchez de Val, J.E.; Calvo-Guirado, J.L.; Gomez Moreno, G.; Gherke, S.; Mazón, P.; De Aza, P.N. Influence of hydroxyapatite granule size, porosity and crystallinity on tissue reaction in vivo. Part B: A comparative study with biphasic synthetic biomaterials. Clin. Oral Implants Res. 2017. [Google Scholar] [CrossRef]
- Muralithran, G.; Ramesh, S. The effects of sintering temperature on the properties of hydroxyapatite. Ceram. Int. 2000, 26, 221–230. [Google Scholar] [CrossRef]
- Ashok, M.; Sundaram, N.M.; Kalkura, S.N. Crystallization of hydoxyapatite at physiological temperature. Mater. Lett. 2003, 57, 2066–2070. [Google Scholar] [CrossRef]
- Hong, J.Y.; Kim, Y.J.; Lee, H.W.; Lee, W.K.; Ko, J.S.; Kim, H.M. Osteoblastic cell response to thin film of poorly crystalline calcium phosphate apatite formed at low temperatures. Biomaterials 2003, 24, 2977–2984. [Google Scholar] [CrossRef]
- Accorsi-Mendonça, T.; Conz, M.B.; Barros, T.C.; de Sena, L.A.; de Almeida Soares, G.; Granjeiro, J.M. Physicochemical characterization of two deproteinized bovine xenografts. Braz. Oral Res. 2008, 22, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Rabadan-Ros, R.; Velasquez, P.; Meseguer-Olmo, L.; de Aza, P.N. Morphological and structural study of a novel porous Nurse´s A ceramic with osteoconductive properties for tissue engineering. Materials 2016, 9, 474. [Google Scholar] [CrossRef]
- Rosa, A.L.; Beloti, M.M.; Oliveira, P.T.; Van Noort, R. Osseointegration and osseoconductivity of hydroxyapatite of different microporosities. J. Mater. Sci. Mater. Med. 2002, 13, 1071–1075. [Google Scholar] [CrossRef] [PubMed]
- Ros-Tarraga, P.; Mazón, P.; Rodriguez, M.A.; Meseguer-Olmo, L.; de Aza, P.N. Novel resorbable and osteoconductive calcium silicophosphate scaffold induced bone formation. Materials 2016, 9, 785. [Google Scholar] [CrossRef]
- De Aza, P.N.; Peña, J.I.; Luklinska, Z.B.; Meseguer-Olmo, L. Bioeutectic® Ceramics for biomedical applications obtained by laser floating method. In vivo evaluation. Materials 2014, 7, 2395–2410. [Google Scholar] [CrossRef]
- Mate-Sanchez de Val, J.E.; Mazon, P.; Calvo-Guirado, J.L.; Delgado-Ruiz, R.A.; Ramirez-Fernandez, M.P.; Negri, B.; Abboud, M.; de Aza, P.N. Comparison of three novel β-tricalcium phosphate/collagen ceramic scaffolds: An in vivo study. J. Biomed. Mater. Res. A 2014, 102, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Antonakos, A.; Liarokapis, E.; Leventouri, T. Micro-Raman and FTIR studies of synthetic and natural apatites. Biomaterials 2007, 28, 3043–3054. [Google Scholar] [CrossRef] [PubMed]
- Ren, F.; Ding, Y.; Leng, Y. Infrared spectroscopic characterization of carbonated apatite: A combined experimental and computational study. J. Biomed. Mater. Res. Part A 2014, 102, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Ślósarczyk, A.; Paluszkiewicz, C.; Gawlicki, M.; Paszkiewicz, Z. The FTIR spectroscopy and QXRD studies of calcium phosphate based materials produced from the powder precursors with different CaP ratios. Ceram. Int. 1997, 23, 297–304. [Google Scholar] [CrossRef]
- Lindgren, C.; Hallman, M.; Sennerby, L.; Sammons, R. Back-scattered electron imaging and elemental analysis of retrieved bone tissue following sinus augmentation with deproteinized bovine bone or biphasic calcium phosphate. Clin. Oral Implants Res. 2010, 21, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.O.; Kämmerer, P.W.; Götz, H.; Duschner, H.; Wagner, W. Long-term bony integration and resorption kinetics of a xenogeneic bone substitute after sinus floor augmentation: Histomorphometric analyses of human biopsy specimens. Int. J. Periodontics Restorative Dent. 2013, 33, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Munar, M.L.; Udoh, K.; Ishikawa, K.; Matsuya, S.; Nakagawa, M. Effects of sintering temperature over 1,300 degrees C on the physical and compositional properties of porous hydroxyapatite foam. Dent. Mater. J. 2006, 25, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Wierzchos, J.; Falcioni, T.; Kiciak, A.; Woliński, J.; Koczorowski, R.; Chomicki, P.; Porembska, M.; Ascaso, C. Advances in the ultrastructural study of the implant-bone interface by backscattered electron imaging. Micron 2008, 39, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Slater, N.; Dasmah, A.; Sennerby, L.; Hallman, M.; Piattelli, A.; Sammons, R. Back-scattered electron imaging and elemental microanalysis of retrieved bone tissue following maxillary sinus floor augmentation with calcium sulphate. Clin. Oral Implants Res. 2008, 19, 814–822. [Google Scholar] [CrossRef] [PubMed]
- Blokhuis, T.J.; Termaat, M.F.; den Boer, F.C.; Patka, P.; Bakker, F.C.; Haarman, H.J. Properties of calcium phosphate ceramics in relation to their in vivo behavior. J. Trauma Acute Care Surg. 2000, 48, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Hamada, H.; Ohshima, H.; Ito, A.; Higuchi, W.I.; Otsuka, M. Effect of geometrical structure on the biodegradation of a three-dimensionally perforated porous apatite/collagen composite bone cell scaffold. Biol. Pharm. Bull. 2010, 33, 1228–1232. [Google Scholar] [CrossRef] [PubMed]
- Raynaud, S.; Champion, E.; Bernache-Assollant, D. Calcium phosphate apatites with variable Ca/P atomic ratio II. Calcination and sintering. Biomaterials. 2002, 23, 1073–1080. [Google Scholar] [CrossRef]
- Danoux, C.; Pereira, D.; Döbelin, N.; Stähli, C.; Barralet, J.; van Blitterswijk, C.; Habibovic, P. The effects of crystal phase and particle morphology of calcium phosphates on proliferation and differentiation of human mesenchymal stromal cells. Adv. Healthc. Mater. 2016, 5, 1775–1785. [Google Scholar] [CrossRef] [PubMed]
- Rammelt, S.; Schulze, E.; Witt, M.; Petsch, E.; Biewener, A.; Pompe, W.; Zwipp, H. Collagen type I increases bone remodelling around hydroxyapatite implants in the rat tibia. Cells Tissues Org. 2004, 178, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Nannmark, U.; Sennerby, L. The bone tissue responses to prehydrated and collagenated cortico-cancellous porcine bone grafts: A study in rabbit maxillary defects. Clin. Implant Dent. Relat. Res. 2008, 10, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Orsini, G.; Scarano, A.; Piattelli, M.; Piccirilli, M.; Caputi, S.; Piattelli, A. Histologic and ultrastructural analysis of regenerated bone in maxillary sinus augmentation using a porcine bone-derived biomaterial. J. Periodontol. 2006, 77, 1984–1990. [Google Scholar] [CrossRef] [PubMed]
- Arcuri, C.; Cecchetti, F.; Germano, F.; Motta, A.; Santacroce, C. Clinical and histological study of a xenogenic bone substitute used as a filler in postextractive alveolus. Miner. Stomatol. 2005, 54, 351–362. [Google Scholar] [PubMed]
- Annaz, B.; Hing, K.A.; Kayser, M.; Buckland, T.; Di Silvio, L. Porosity variation in hydroxyapatite and osteoblast morphology: A scanning electron microscopy study. J. Microsc. 2004, 215, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Cyster, L.A.; Grant, D.M.; Howdle, S.M.; Rose, F.R.; Irvine, D.J.; Freeman, D.; Scotchford, C.A.; Shakesheff, K.M. The influence of dispersant concentration on the pore morphology of hydroxyapatite ceramics for bone tissue engineering. Biomaterials 2005, 26, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Traini, T.; Valentini, P.; Lezzi, G.; Piatelli, A. A histologic and histomorphometric evaluation of anorganic bovine bone retrieved 9 years after a sinus augmentation procedure. J. Periodontol. 2007, 78, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Mordenfeld, A.; Hallman, M.; Albrektsson, T. Histological & histomorpho-metrical analyses of biopsies harvested 11 years after maxillary sinus augmentation with 80% Bio-Oss and 20% autogenous bone. Clin. Oral Implants Res. 2010, 21, 961–970. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Moreno, P.; Hernández-Cortés, P.; Mesa, F.; Carranza, N.; Juodzbalys, G.; Aguilar, M.; O’Valle, F. Slow resorption of anorganic bovine bone by osteoclasts in maxillary sinus augmentation. Clin. Implant Dent. Relat. Res. 2013, 15, 858–866. [Google Scholar] [CrossRef] [PubMed]
- Orsini, G.; Traini, T.; Scarano, A.; Degidi, M.; Perrotti, V.; Piccirilli, M.; Piattelli, A. Maxillary sinus augmentation with Bio-Oss particles: A light, scanning, and transmission electron microscopy study in man. J. Biomed. Mater. Res. Part B Appl. Biomater. 2005, 74, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Cordaro, L.; Bosshardt, D.D.; Palatella, P.; Rao, W.; Serino, G.; Chiapasco, M. Maxillary sinus grafting with Bio-Oss® or Straumann® Bone Ceramic: Histomorphometric result from a randomized controlled multicenter clinical trial. Clin. Oral Implants Res. 2008, 19, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Traini, T.; Degidi, M.; Sammons, R.; Stanley, P.; Piattelli, A. Histologic and elemental microanalytical study of anorganic bovine bone substitution following sinus floor augmentation in humans. J. Periodontol. 2008, 79, 1232–1240. [Google Scholar] [CrossRef] [PubMed]
- Briem, D.; Linhart, W.; Lehmann, W.; Meenen, N.M.; Rueger, J.M. Long-term outcomes after using porous hydroxyapatite ceramics (Endobon®) for surgical management of fractures of the head of the tibia. Unfallchirurg 2002, 105, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.C.; Cuff, S.E.; Leger, J.P.; Morra, A.; Anderson, G.I. In vitro osteoclast resorption of bone substitute biomaterials used for implant site augmentation: A pilot study. Int. J. Oral Maxillofac. Implant. 2002, 17, 321–330. [Google Scholar] [PubMed]
- Moon, J.W.; Sohn, D.S.; Heo, J.U. Histomorphometric analysis of maxillary sinus augmentation with calcium phosphate nanocrystal-coated xenograft. Implant. Dent. 2015, 24, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Fienitz, T.; Moses, O.; Klemm, C.; Happe, A.; Ferrari, D.; Kreppel, M.; Ormianer, Z.; Gal, M.; Rothamel, D. Histological and radiological evaluation of sintered and non-sintered deproteinized bovine bone substitute materials in sinus augmentation procedures. A prospective, randomized-controlled, clinical multicenter study. Clin. Oral Investig. 2017, 21, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Bertazzo, S.; Zambuzzi, W.F.; Campos, D.D.; Ogeda, T.L.; Ferreira, C.V.; Bertran, C.A. Hydroxyapatite surface solubility and effect on cell adhesion. Colloids Surf. B Biointerf. 2010, 78, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Chou, Y.F.; Huang, W.; Dunn, L.C.; Miller, T.A.; Wu, B.M. The effect of biomimetic apatite structure on osteoblast viability, proliferation and gene expression. Biomaterials 2005, 26, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Berger, C.E.; Rathod, H.; Gillespie, J.I.; Horrocks, B.R.; Datta, H.K. Scanning electrochemical microscopy at the surface of bone-resorbing osteoclasts: Evidence for steady-state disposal and intracellular functional compartmentalization of calcium. J. Bone Miner. Res. 2001, 16, 2092–2102. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Shimizu, Y.; Asai, S.; Ooya, K. Grafting of deproteinized bone particles inhibits bone resorption after maxillary sinus floor elevation. Clin. Oral Implants Res. 2004, 15, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Detsch, R.; Boccaccini, A.R. The role of osteoclasts in bone tissue engineering. J. Tissue Eng. Regen. Med. 2015, 9, 1133–1149. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, S.L.; Jeffrey, C.K.L.; Tan, C.Y.; Wong, Y.H.; Ganesan, P.; Ramesh, S.; Kutty, M.G.; Chandran, H.; Devaraj, P. Sintering behaviour and properties of magnesium orthosilicate-hydroxyapatite ceramic. Ceram. Int. 2016, 42, 15756–15761. [Google Scholar] [CrossRef]
- Schilling, A.F.; Linhart, W.; Filke, S.; Gebauer, M.; Schinke, T.; Rueger, J.M.; Amling, M. Resorbability of bone substitute biomaterials by human osteoclasts. Biomaterials 2004, 25, 3963–3972. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, S.; Detsch, R.; Uhl, F.; Deisinger, U.; Ziegler, G. How degradation of calcium phosphate bone substitute materials is influenced by phase composition and porosity. Adv. Eng. Mater. 2011, 13, 342–350. [Google Scholar] [CrossRef]
- Monteiro, M.M.; Campos da Rocha, N.C.; Rossi, A.M.; de Almeida Soares, G. Dissolution properties of calcium phosphate granules with different compositions in simulated body fluid. J. Biomed. Mater. Res. A 2003, 65, 299–305. [Google Scholar] [CrossRef] [PubMed]
- von Doernberg, M.C.; von Rechenberg, B.; Bohner, M.; Grünenfelder, S.; van Lenthe, G.H.; Müller, R.; Gasser, B.; Mathys, R.; Baroud, G.; Auer, J. In vivo behavior of calcium phosphate scaffolds with four different pore sizes. Biomaterials. 2006, 27, 5186–5198. [Google Scholar] [CrossRef] [PubMed]
- Costa-Rodrigues, J.; Fernandes, A.; Lopes, M.A.; Fernandes, M.H. Hydroxyapatite surface roughness: Complex modulation of the osteoclastogenesis of human precursor cells. Acta Biomater. 2012, 8, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Rezwan, K.; Chen, Q.Z.; Blaker, J.J.; Boccaccini, A.R. Biodegradable and bioactive porous polymer/inorganic composite scaffolds for bone tissue engineering. Biomaterials 2006, 27, 3413–3431. [Google Scholar] [CrossRef] [PubMed]
- Tatum, H., Jr. Maxillary and sinus implant reconstructions. Dent. Clin. N. Am. 1986, 30, 207–229. [Google Scholar] [PubMed]
- Shull, C.G. The determination of X-ray diffraction line widths. Phys. Rev. 1946, 70, 679–684. [Google Scholar] [CrossRef]
- Wejrzanowski, T.; Pielaszek, R.; Opalińska, A.; Matysiak, H.; Łojkowski, W.; Kurzydłowski, K.J. Quantitative methods for nanopowders characterization. Appl. Surf. Sci. 2016, 253, 204–208. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ca/P Ratios (wt %) | DPHa | DBHa |
|---|---|---|
| Mean | 2.22 | 2.31 |
| SD | 0.08 | 0.09 |
| Median | 2.22 | 2.28 |
| Materials Characterized | Real Density (g/cc) | Apparent Density (g/cc) | Surface Area (m2/g) | Total Porosity (%) a | Phase/s | Particle Size (μm) | Crystal Size (nm) |
|---|---|---|---|---|---|---|---|
| DPHa | 2.85 | 1.14 | 9.78 | 59.90 | HA + Coll | 600–1000 | 325 |
| DBHa | 2.98 | 1.51 | 2.77 | 49.13 | HA | 500–1000 | 732 |
| HA Synthetic | 3.16 | 1.62 | 3.10 | 46.4 | HA | 600–1000 | 731 |
| Osseous Matri | 1.46 | 1.24 | – | 69.3 | HA + Coll | 400–700 | 68.4 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramírez Fernández, M.P.; Gehrke, S.A.; Pérez Albacete Martinez, C.; Calvo Guirado, J.L.; De Aza, P.N. SEM-EDX Study of the Degradation Process of Two Xenograft Materials Used in Sinus Lift Procedures. Materials 2017, 10, 542. https://0-doi-org.brum.beds.ac.uk/10.3390/ma10050542
Ramírez Fernández MP, Gehrke SA, Pérez Albacete Martinez C, Calvo Guirado JL, De Aza PN. SEM-EDX Study of the Degradation Process of Two Xenograft Materials Used in Sinus Lift Procedures. Materials. 2017; 10(5):542. https://0-doi-org.brum.beds.ac.uk/10.3390/ma10050542
Chicago/Turabian StyleRamírez Fernández, María Piedad, Sergio A. Gehrke, Carlos Pérez Albacete Martinez, Jose L. Calvo Guirado, and Piedad N. De Aza. 2017. "SEM-EDX Study of the Degradation Process of Two Xenograft Materials Used in Sinus Lift Procedures" Materials 10, no. 5: 542. https://0-doi-org.brum.beds.ac.uk/10.3390/ma10050542