Effect of Different Irrigation Solutions on the Diffusion of MTA Cement into the Root Canal Dentin

 , , , , , , ,
, , , , , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Root Canal Preparation
2.3. Final Irrigation Protocol
2.4. Root Canal Filling
2.5. Sectioning and Image Analysis
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rossi-Fedele, G.; Doğramacı, E.J.; Guastalli, A.R.; Steier, L.; de Figueiredo, J.A.P. Antagonistic Interactions between Sodium Hypochlorite, Chlorhexidine, EDTA, and Citric Acid. J. Endod. 2012, 38, 426–431. [Google Scholar] [CrossRef] [PubMed]
- De Assis, D.F.; Prado, M.; do Simão, R.A. Evaluation of the Interaction between Endodontic Sealers and Dentin Treated with Different Irrigant Solutions. J. Endod. 2011, 37, 1550–1552. [Google Scholar] [CrossRef] [PubMed]
- Razmi, H.; Bolhari, B.; Dashti, N.K.; Fazlyab, M. The Effect of Canal Dryness on Bond Strength of Bioceramic and Epoxy-resin Sealers after Irrigation with Sodium Hypochlorite or Chlorhexidine. Iran. Endod. J. 2016, 11, 129–133. [Google Scholar] [PubMed]
- Basrani, B.R.; Manek, S.; Sodhi, R.N.S.; Fillery, E.; Manzur, A. Interaction between Sodium Hypochlorite and Chlorhexidine Gluconate. J. Endod. 2007, 33, 966–969. [Google Scholar] [CrossRef]
- Bui, T.B.; Baumgartner, J.C.; Mitchell, J.C. Evaluation of the Interaction between Sodium Hypochlorite and Chlorhexidine Gluconate and its Effect on Root Dentin. J. Endod. 2008, 34, 181–185. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Psimma, Z.; van der Sluis, L.W.M. Factors affecting irrigant extrusion during root canal irrigation: A systematic review. Int. Endod. J. 2013, 46, 599–618. [Google Scholar] [CrossRef] [Green Version]
- Kuçi, A.; Alaçam, T.; Yavaş, Ö.; Ergul-Ulger, Z.; Kayaoglu, G. Sealer Penetration into Dentinal Tubules in the Presence or Absence of Smear Layer: A Confocal Laser Scanning Microscopic Study. J. Endod. 2014, 40, 1627–1631. [Google Scholar] [CrossRef]
- Violich, D.R.; Chandler, N.P. The smear layer in endodontics-a review. Int. Endod. J. 2010, 43, 2–15. [Google Scholar] [CrossRef]
- Akisue, E.; Tomita, V.S.; Gavini, G.; de Figueiredo, J.A.P. Effect of the Combination of Sodium Hypochlorite and Chlorhexidine on Dentinal Permeability and Scanning Electron Microscopy Precipitate Observation. J. Endod. 2010, 36, 847–850. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; Sudhakaran, S. Evaluation and Prevention of the Precipitate Formed on Interaction between Sodium Hypochlorite and Chlorhexidine. J. Endod. 2010, 36, 1154–1157. [Google Scholar] [CrossRef]
- Ballal, V.; Kundabala, M.; Acharya, S.; Ballal, M. Antimicrobial action of calcium hydroxide, chlorhexidine and their combination on endodontic pathogens. Aust. Dent. J. 2007, 52, 118–121. [Google Scholar] [CrossRef]
- Sena, N.T.; Gomes, B.P.F.A.; Vianna, M.E.; Berber, V.B.; Zaia, A.A.; Ferraz, C.C.R.; Souza-Filho, F.J. In vitro antimicrobial activity of sodium hypochlorite and chlorhexidine against selected single-species biofilms. Int. Endod. J. 2006, 39, 878–885. [Google Scholar] [CrossRef] [PubMed]
- White, R.R.; Hays, G.L.; Janer, L.R. Residual antimicrobial activity after canal irrigation with chlorhexidine. J. Endod. 1997, 23, 229–231. [Google Scholar] [CrossRef]
- Ma, R.; Liu, Z.; Zhu, C. Lian A comparative study of root smear layer removal using different pH EDTA salts. Shanghai Kou Qiang Yi Xue 2003, 12, 197–199. [Google Scholar] [PubMed]
- Borges, Á.H.; Dorileo, M.C.G.O.; Villa, R.D.; Borba, A.M.; Semenoff, T.A.D.V.; Guedes, O.A.; Estrela, C.R.A.; Bandeca, M.C. Physicochemical Properties and Surfaces Morphologies Evaluation of MTA FillApex and AH Plus. Sci. World J. 2014, 2014, 1–6. [Google Scholar] [CrossRef] [PubMed]
- AL-Haddad, A.; Ab Aziz, Z.A.C. Bioceramic-Based Root Canal Sealers: A Review. Int. J. Biomater. 2016, 2016, 9753210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, K.C.; Soares, C.J.; Steier, L.; Versiani, M.A.; Abi Rached-Júnior, F.J.; Pécora, J.D.; Silva-Sousa, Y.T.C.; de Sousa-Neto, M.D. Influence of Drying Protocol with Isopropyl Alcohol on the Bond Strength of Resin-based Sealers to the Root Dentin. J. Endod. 2014, 40, 1454–1458. [Google Scholar] [CrossRef]
- Pandey, P.; Aggarwal, H.; Tikku, A.P.; Singh, A.; Bains, R.; Mishra, S. Comparative evaluation of sealing ability of gutta percha and resilon as root canal filling materials—A systematic review. J. Oral Biol. Craniofacial Res. 2020, 10, 220–226. [Google Scholar] [CrossRef]
- Pinto, J.; Torres, F.; Pivoto-João, M.; Cirelli, J.; Guerreiro-Tanomaru, J.; Tanomaru-Filho, M. Filling ability and flow of root canal sealers: A micro-computed tomographic study. Braz. Dent. J. 2020, 31, 499–504. [Google Scholar] [CrossRef]
- Donnermeyer, D.; Burklein, S.; Dammaschke, T.; Schafer, E. Endodontic sealers based on calcium silicates: A systematic review. Odontology 2019, 107, 421–436. [Google Scholar] [CrossRef]
- Li, G.; Niu, L.; Selem, L.; Eid, A.; Bergeron, B.; Chen, J.; Pashely, D.; Tay, F. Quality of obturation achieved by an endodontic core-carrier system with crosslinked gutta-percha carrier in single-rooted canals. J. Dent. 2014, 42, 1124–1134. [Google Scholar] [CrossRef] [Green Version]
- Silva, E.J.N.L.; Rosa, T.P.; Herrera, D.R.; Jacinto, R.C.; Gomes, B.P.F.A.; Zaia, A.A. Evaluation of Cytotoxicity and Physicochemical Properties of Calcium Silicate-based Endodontic Sealer MTA Fillapex. J. Endod. 2013, 39, 274–277. [Google Scholar] [CrossRef]
- Nagas, E.; Uyanik, M.O.; Eymirli, A.; Cehreli, Z.C.; Vallittu, P.K.; Lassila, L.V.J.; Durmaz, V. Dentin Moisture Conditions Affect the Adhesion of Root Canal Sealers. J. Endod. 2012, 38, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Asawaworarit, W.; Yachor, P.; Kijsamanmith, K.; Vongsavan, N. Comparison of the Apical Sealing Ability of Calcium Silicate-Based Sealer and Resin-Based Sealer Using the Fluid-Filtration Technique. Med. Princ. Pract. 2016, 25, 561–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, S.W.; Lee, S.Y.; Kang, S.K.; Kum, K.Y.; Kim, E.C. In vitro biocompatibility, inflammatory response, and osteogenic potential of 4 root canal sealers: Sealapex, sankin apatite root sealer, MTA Fillapex, and iroot SP root canal sealer. J. Endod. 2014, 40, 1642–1648. [Google Scholar] [CrossRef] [PubMed]
- Al-Haddad, A.Y.; Kutty, M.G.; Abu Kasim, N.H.; Ab Aziz, Z.A.C. The effect of moisture conditions on the constitution of two bioceramic-based root canal sealers. J. Dent. Sci. 2017, 12, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Gharib, S.R.; Tordik, P.A.; Imamura, G.M.; Baginski, T.A.; Goodell, G.G. A confocal laser scanning microscope investigation of the epiphany obturation system. J. Endod. 2007, 33, 957–961. [Google Scholar] [CrossRef]
- Coronas, V.; Villa, N.; Nascimento, A.; Duarte, P.; Rosa, R.; Só, M. Dentinal tubule penetration of a calcium silicate-based root canal sealer using a specific calcium fluorophore. Braz. Dent. J. 2020, 31, 109–115. [Google Scholar] [CrossRef]
- Tedesco, M.; Chain, M.; Felippe, W.; Alves, A.; Garcia, L.; Bortoluzzi, E.; Cordeiro, M.; Teixeira, C. Correlation between bond strength to dentin and sealers penetration by push-out test and CLSM analysis. Braz. Dent. J. 2019, 30, 555–562. [Google Scholar] [CrossRef] [PubMed]
- El Hachem, R.; Le Brun, G.; Le Jeune, B.; Pellen, F.; Khalil, I.; Abboud, M. Influence of the EndoActivator irrigation system on dentinal tubule penetration of a novel tricalcium silicate-based sealer. Dent. J. 2018, 6, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bem, I.; Oliveira, R.; Weissheimer, T.; Bier, C.; Só, M.; Rosa, R. Effect of ultrasonic activation of endodontic sealers on intratubular penetration and bond strength to root dentin. J. Endod. 2020, 46, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Oksan, T.; Aktener, B.O.; Şen, B.H.; Tezel, H. The penetration of root canal sealers into dentinai tubules. A scanning electron microscopic study. Int. Endod. J. 1993, 26, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Ordinola-Zapata, R.; Bramante, C.M.; Bernardineli, N.; Graeff, M.S.Z.; Garcia, R.B.; de Moraes, I.G.; Debelian, G. A preliminary study of the percentage of sealer penetration in roots obturated with the Thermafil and RealSeal-1 obturation techniques in mesial root canals of mandibular molars. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 961–968. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.W.; DeGraft-Johnson, A.; Dorn, S.O.; Di Fiore, P.M. Dentinal Tubule Penetration of a Calcium Silicate–based Root Canal Sealer with Different Obturation Methods. J. Endod. 2017, 43, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Qian, W.; Shen, Y.; Haapasalo, M. Quantitative Analysis of the Effect of Irrigant Solution Sequences on Dentin Erosion. J. Endod. 2011, 37, 1437–1441. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section | Irrigant Solution | Mean | Median | Sd | Min | Max |
|---|---|---|---|---|---|---|
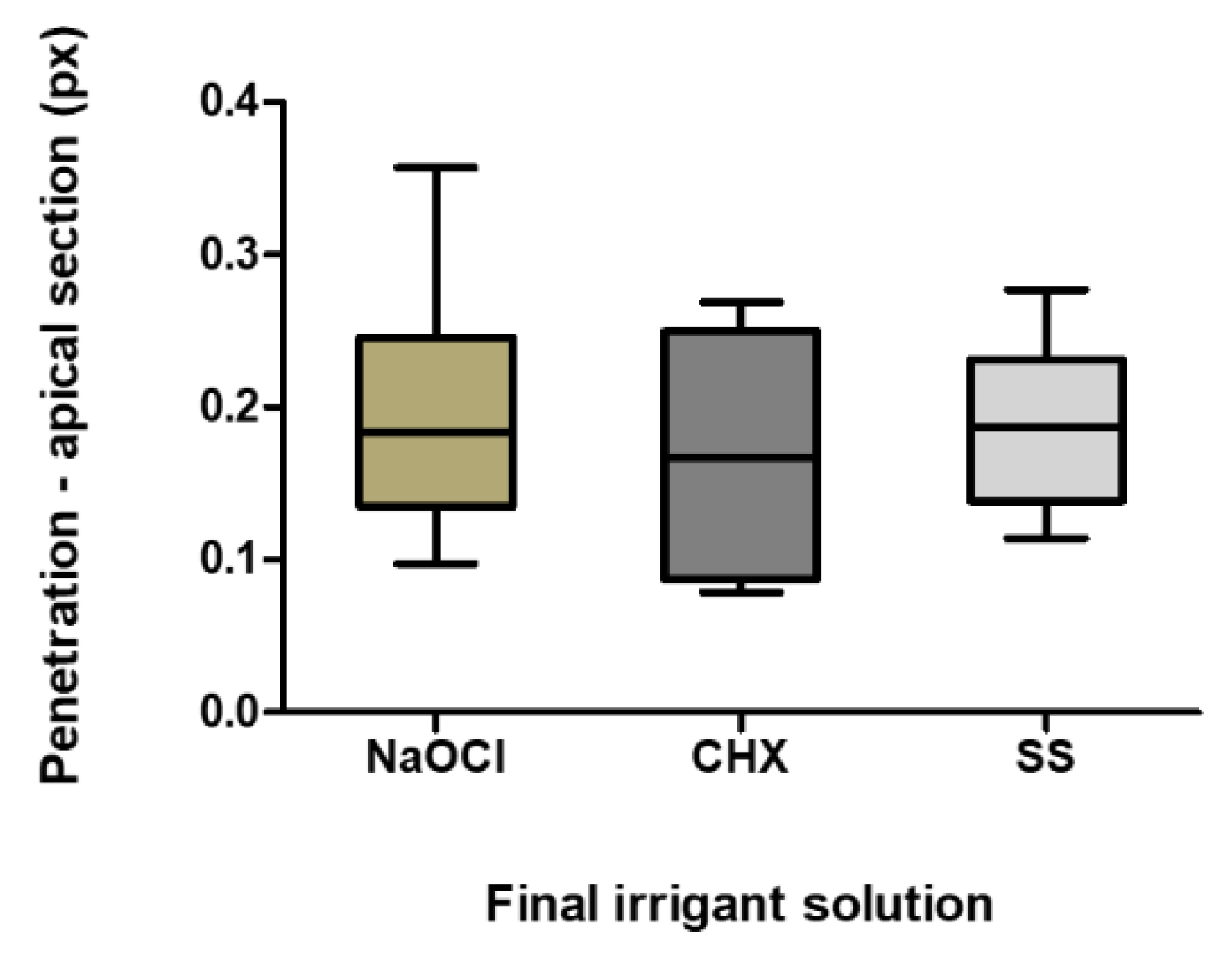
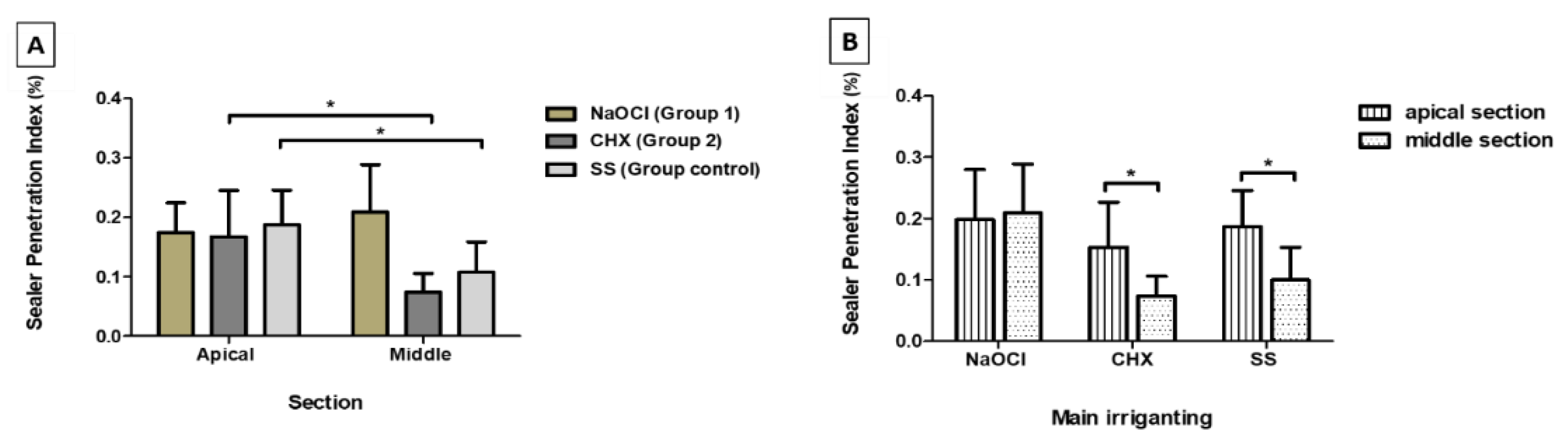
| Apical | Group 1 (NaOCl) | 0.174 | 0.164 | 0.051 | 0.098 | 0.255 |
| Group 2 (CHX) | 0.167 | 0.167 | 0.078 | 0.079 | 0.269 | |
| Control Group (SS) | 0.187 | 0.187 | 0.058 | 0.114 | 0.277 | |
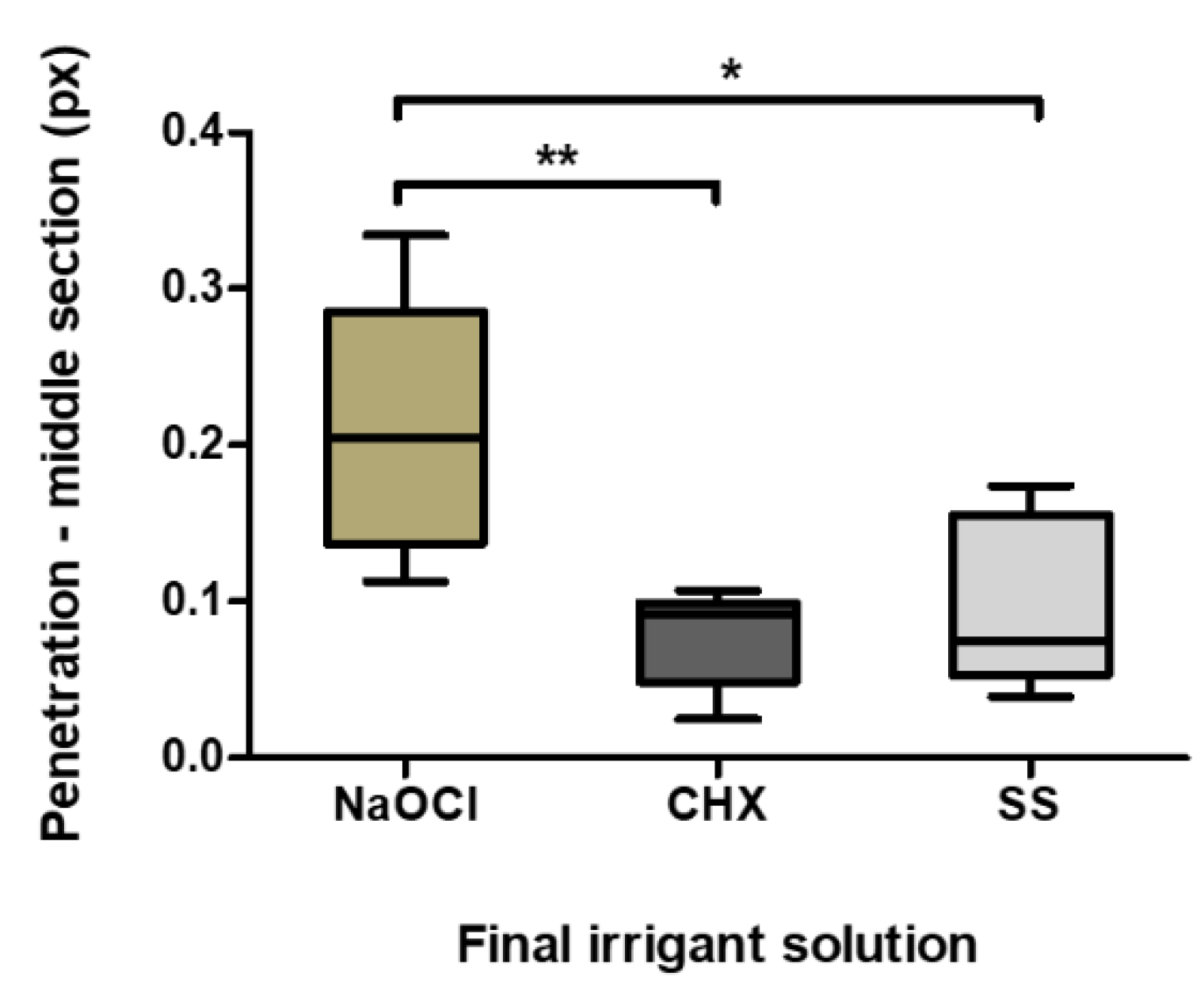
| Middle | Group 1 (NaOCl) | 0.209 | 0.205 | 0.080 | 0.113 | 0.334 |
| Group 2 (CHX) | 0.074 | 0.092 | 0.032 | 0.025 | 0.107 | |
| Control Group (SS) | 0.108 | 0.102 | 0.051 | 0.046 | 0.174 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinho, J.P.; França, S.; Paulo, S.; Paula, A.B.; Coelho, A.S.; Abrantes, A.M.; Caramelo, F.; Carrilho, E.; Marto, C.M.; Botelho, M.F.; et al. Effect of Different Irrigation Solutions on the Diffusion of MTA Cement into the Root Canal Dentin. Materials 2020, 13, 5472. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13235472
Martinho JP, França S, Paulo S, Paula AB, Coelho AS, Abrantes AM, Caramelo F, Carrilho E, Marto CM, Botelho MF, et al. Effect of Different Irrigation Solutions on the Diffusion of MTA Cement into the Root Canal Dentin. Materials. 2020; 13(23):5472. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13235472
Chicago/Turabian StyleMartinho, José Pedro, Sara França, Siri Paulo, Anabela Baptista Paula, Ana Sofia Coelho, Ana Margarida Abrantes, Francisco Caramelo, Eunice Carrilho, Carlos Miguel Marto, Maria Filomena Botelho, and et al. 2020. "Effect of Different Irrigation Solutions on the Diffusion of MTA Cement into the Root Canal Dentin" Materials 13, no. 23: 5472. https://0-doi-org.brum.beds.ac.uk/10.3390/ma13235472