
Tissue Level Changes after Maxillary Sinus Floor Elevation with Three Types of Calcium Phosphate Ceramics: A Radiological Study with a 5-Year Follow-Up

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Maxillary Sinus Floor Elevation Procedure
2.3. Dental Implant Placement
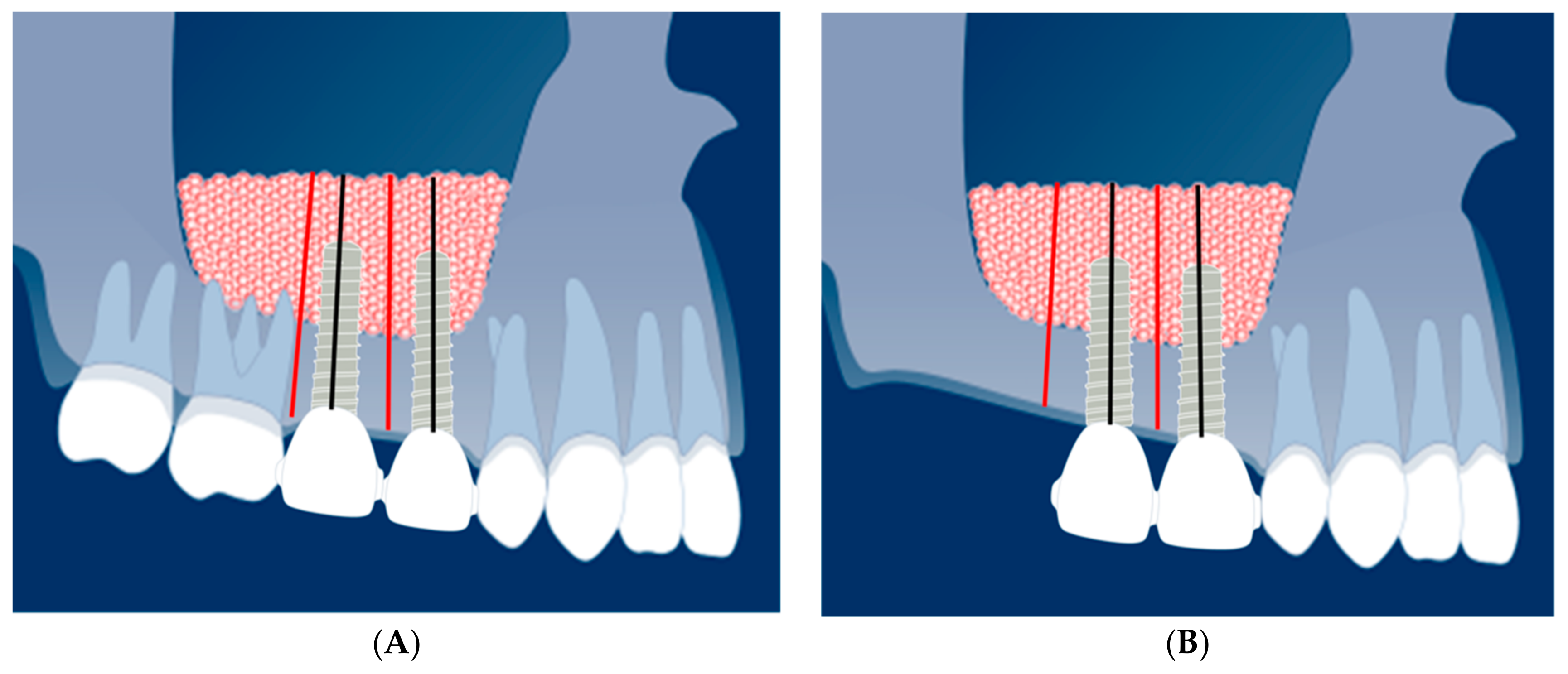
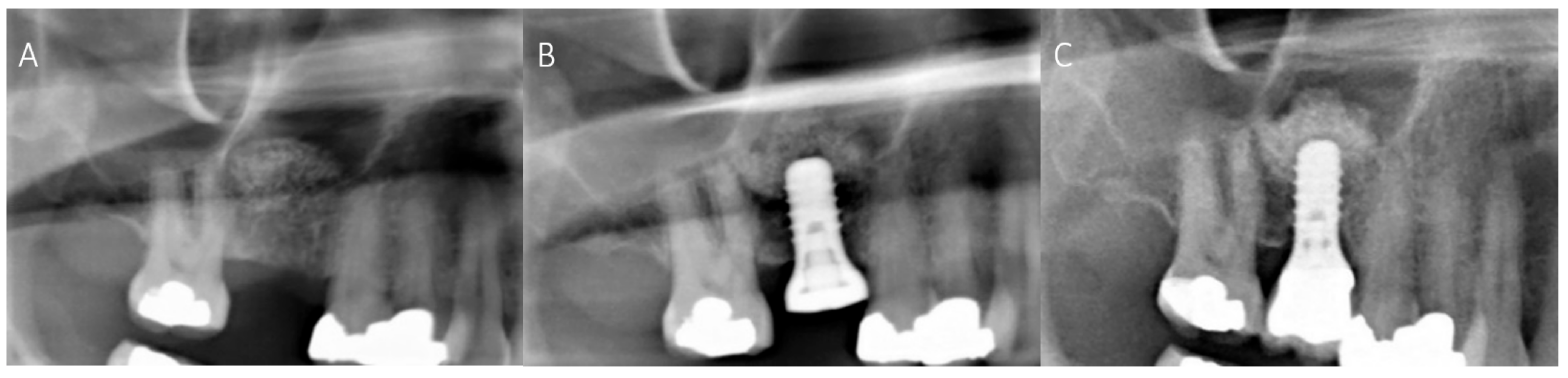
2.4. Radiological Evaluation
2.5. Statistical Analysis
3. Results
3.1. Patient Data
3.2. Maxillary Sinus Floor Elevation with Calcium Phosphate Ceramics
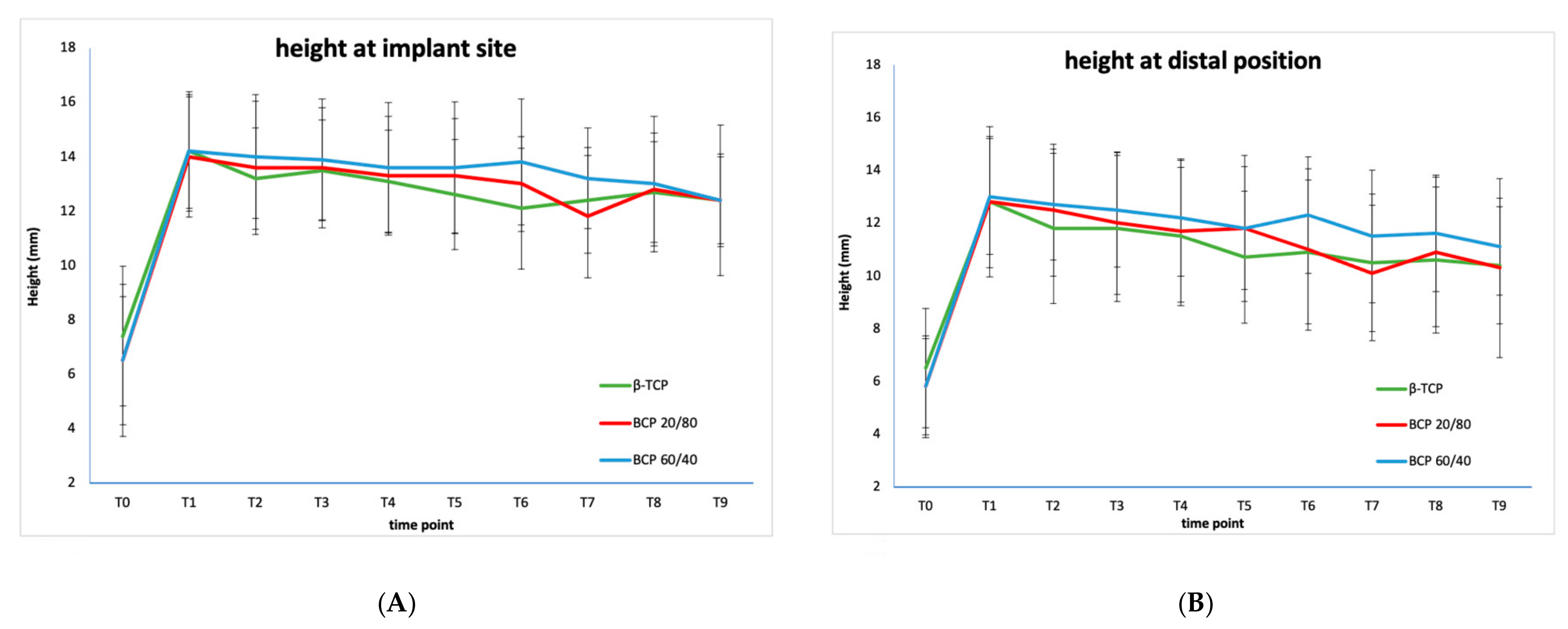
3.3. Comparison of Three Individual Types of Calcium Phosphate Ceramics
3.4. Comparison of the Combined Calcium Phosphate Ceramics at Implant Position and Inter-Implant (Distal) Position
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BCP | biphasic calcium phosphate |
| β-TCP | β-tricalcium phosphate |
| g | gram |
| HA | hydroxyapatite |
| ns | not significant |
| mg | milligram |
| mL | milliliter |
| mm | millimeters |
| MSFE | maxillary sinus floor elevation |
| p-value | null hypothesis significance testing |
| SBC | Straumann® Bone Ceramic |
| SD | Standard Deviation ± |
| SLA | sand-blasted, large-grit, acid-etched |
| w/w | weight-based |
References
- Boyne, P.J.; James, R.A. Grafting of the maxillary sinus floor with autogenous marrow and bone. J. Oral Surg. 1980, 38, 613–616. [Google Scholar] [PubMed]
- Tatum, H., Jr. Maxillary and sinus implant reconstructions. Dent Clin. N. Am. 1986, 30, 207–229. [Google Scholar] [PubMed]
- Wallace, S.S.; Froum, S.J. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann. Periodontol. 2003, 8, 328–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zijderveld, S.A.; Zerbo, I.R.; Van den Bergh, J.P.A.; Schulten, E.A.J.M.; ten Bruggenkate, C.M. Maxillary Sinus Floor Augmentation Using a β–Tricalcium Phosphate (Cerasorb) Alone Compared to Autogenous Bone Grafts. Int. J. Oral Maxillofac. Implant. 2005, 20, 432–440. [Google Scholar]
- Bouwman, W.F.; Bravenboer, N.; Frenken, J.W.F.H.; ten Bruggenkate, C.M.; Schulten, E.A.J.M. The use of a biphasic calcium phosphate in a maxillary sinus floor elevation procedure: A clinical radiological histological and histomorphometric evaluation with 9- and 12-month healing times. Int. J. Implant Dent. 2017, 3, 34. [Google Scholar] [CrossRef] [Green Version]
- Klijn, R.J.; Meijer, G.J.; Bronkhorst, E.M.; Jansen, J.A. A meta-analysis of histomorphometric results and graft healing time of various biomaterials compared to autologous bone used as sinus floor augmentation material in humans. Tissue Eng. Part B Rev. 2010, 16, 493–507. [Google Scholar] [CrossRef] [Green Version]
- Van den Bergh, J.P.; ten Bruggenkate, C.M.; Krekeler, G.; Tuinzing, D.B. Sinus floor elevation and grafting with autogenous iliac crest bone. Clin. Oral Implant. Res. 1998, 9, 429–435. [Google Scholar] [CrossRef]
- Misch, C.M. Autogenous Bone: Is It Still the Gold Standard? Implant Dent. 2010, 19, 361. [Google Scholar] [CrossRef]
- Stumbras, A.; Krukis, M.M.; Januzis, G.; Juodzbalys, G. Regenerative bone potential after sinus floor elevation using various bone graft materials: A systematic review. Quintessence Int. 2019, 50, 548–558. [Google Scholar]
- Beirne, J.C.; Barry, H.J.; Brady, F.A.; Morris, V.B. Donor site morbidity of the anterior iliac crest following cancellous bone harvest. Int. J. Oral Maxillofac. Implant. 1996, 25, 268–271. [Google Scholar] [CrossRef]
- Kalk, W.W.; Raghoebar, G.M.; Jansma, J.; Boering, G. Morbidity from iliac crest bone harvesting. Int. J. Oral Maxillofac. Implant. 1996, 54, 1424–1429. [Google Scholar] [CrossRef]
- Nkenke, E.; Stelzle, F. Clinical outcomes of sinus floor augmentation for implant placement using autogenous bone or bone substitutes: A systematic review. Clin. Oral Implant. Res. 2009, 20 (Suppl. 4), 124–133. [Google Scholar] [CrossRef]
- Raghoebar, G.M.; Louwerse, C.; Kalk, W.W.; Vissink, A. Morbidity of chin bone harvesting. Clin. Oral Implant. Res. 2001, 12, 503–507. [Google Scholar] [CrossRef]
- Zijderveld, S.A.; ten Bruggenkate, C.M.; Van Den Bergh, J.P.; Schulten, E.A.J.M. Fractures of the iliac crest after split-thickness bone grafting for preprosthetic surgery: Report of 3 cases and review of the literature. J. Oral Maxillofac. Surg. 2004, 7, 781–786. [Google Scholar] [CrossRef]
- Wheeler, S.L. Sinus augmentation for dental implants: The use of alloplastic materials. J. Oral Maxillofac. Surg. 1997, 55, 1287–1293. [Google Scholar] [CrossRef]
- Corbella, S.; Taschieri, S.; Weinstein, R.; Del Fabbro, M. Histomorphometric outcomes after lateral sinus floor elevation procedure: A systematic review of the literature and meta-analysis. Clin. Oral Implant. Res. 2016, 27, 1106–1122. [Google Scholar] [CrossRef]
- Haugen, H.J.; Lyngstadaas, S.P.; Rossi, F.; Perale, G. Bone grafts: Which is the ideal biomaterial? J. Clin. Periodontol. 2019, 46 (Suppl. 21), 92–102. [Google Scholar] [CrossRef]
- Joosten, U.; Joist, A.; Frebel, T.; Walter, M.; Langer, M. The use of an in situ curing hydroxyapatite cement as an alternative to bone graft following removal of enchondroma of the hand. J. Hand Surg. Br. Eur. Vol. 2000, 25, 288–291. [Google Scholar] [CrossRef]
- Nery, E.B.; Lee, K.K.; Czajkowski, S.; Dooner, J.J.; Duggan, M.; Ellinger, R.F.; Henkin, J.M.; Hines, R.; Miller, M.; Olson, J.W.; et al. A Veterans Administration Cooperative Study of biphasic calcium phosphate ceramic in periodontal osseous defects. J. Periodontol. 1990, 61, 737–744. [Google Scholar] [CrossRef]
- Zerbo, I.R.; Zijderveld, S.A.; De Boer, A.; Bronckers, A.L.J.J.; De Lange, G.; ten Bruggenkate, C.M.; Burger, E.H. Histomorphometry of human sinus floor augmentation using a porous beta-tricalcium phosphate: A prospective study. Clin. Oral Implant. Res. 2004, 15, 724–732. [Google Scholar] [CrossRef]
- Frenken, J.W.; Bouwman, W.F.; Bravenboer, N.; Zijderveld, S.A.; Schulten, E.A.J.M. The use of Straumann® Bone Ceramic in a maxillary sinus floor elevation procedure: A clinical radiological histological and histomorphometric evaluation with a 6-month healing period. Clin. Oral Implant. Res. 2010, 21, 201–208. [Google Scholar] [CrossRef]
- Costantino, P.D.; Friedman, C.D.; Jones, K.; Chow, L.C.; Pelzer, H.J.; Sisson, G.A. Hydroxyapatite cement: I. Basic chemistry and histologic properties. Arch. Otolaryngol. Head Neck Surg. 1991, 117, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Costantino, P.D.; Friedman, C.D. Synthetic bone graft substitutes. Otolaryngol. Clin. N. Am. 1994, 27, 1037–1074. [Google Scholar] [CrossRef]
- Fujita, R.; Yokoyama, A.; Kawasaki, T.; Kohgo, T. Bone augmentation osteogenesis using hydroxyapatite and ß-tricalcium phosphate blocks. J. Oral Maxillofac. Surg. 2003, 9, 1045–1053. [Google Scholar] [CrossRef]
- Jensen, S.S.; Aaboe, M.; Pinholt, E.M.; Hjorting-Hansen, E.; Melsen, F.; Ruyter, I.E. Tissue reaction and material characteristics of four bone substitutes. Int. J. Oral Maxillofac. Implant. 1996, 11, 55–66. [Google Scholar]
- Burchardt, H. The biology of bone graft repair. Clin. Orthop. Relat. Res. 1983, 174, 28–42. [Google Scholar] [CrossRef]
- Jensen, O.T.; Shulman, L.B.; Block, M.S.; Iacono, V.J. Report of the Sinus Consensus Conference of 1996. Int. J. Oral Maxillofac. Implant. 1998, 13, 11–45. [Google Scholar]
- Tong, D.C.; Rioux, K.; Drangsholt, M.; Beirne, O.R. A review of survival rates for implants placed in grafted maxillary sinuses using meta-analysis. Int. J. Oral Maxillofac. Implant. 1998, 13, 175–182. [Google Scholar]
- Lindgren, C.; Mordenfeld, A.; Hallman, M. A prospective 1-year clinical and radiographic study of implants placed after maxillary sinus floor augmentation with synthetic biphasic calcium phosphate or deproteinized bovine bone. Clin. Implant Dent. 2012, 14, 41–50. [Google Scholar] [CrossRef]
- Mertens, C.; Wiens, D.; Steveling, H.G.; Sander, A.; Freier, K. Maxillary sinus-floor elevation with nanoporous biphasic bone graft material for early implant placement. Clin. Implant Dent. 2014, 16, 365–373. [Google Scholar] [CrossRef]
- Oba, Y.; Tachikawa, N.; Munakata, M.; Okada, T.; Kasugai, S. Evaluation of maxillary sinus floor augmentation with the crestal approach and beta-tricalcium phosphate: A cone-beam computed tomography 3- to 9-year follow-up. Int. J. Implant Dent. 2020, 6, 27. [Google Scholar] [CrossRef] [PubMed]
- Okada, T.; Kanai, T.; Tachikawa, N.; Munakata, M.; Kasugai, S. Long-term radiographic assessment of maxillary sinus floor augmentation using beta-tricalcium phosphate: Analysis by cone-beam computed tomography. Int. J. Implant Dent. 2016, 2, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, R.S.; Gorla, L.F.; Boos, F.B.J.D.; Okamoto, R.; Garcia Junior, I.R.; Hochuli-Vieira, E. Use of autogenous bone and beta-tricalcium phosphate in maxillary sinus lifting: Histomorphometric study and immunohistochemical assessment of RUNX2 and VEGF. Int. J. Oral Maxillofac. Surg. 2017, 46, 503–510. [Google Scholar] [CrossRef] [Green Version]
- Nkenke, E.; Neukam, F.W. Autogenous bone harvesting and grafting in advanced jaw resorption: Morbidity, resorption and implant survival. Eur. J. Oral. Implantol. 2014, 7, 203–217. [Google Scholar]
- Sbordone, L.; Levin, L.; Guidetti, F.; Sbordone, C.; Glikman, A.; Schwartz-Arad, D. Apical and marginal bone alterations around implants in maxillary sinus augmentation graftedwith autogenous bone or bovine bone material and simultaneous or delayed dental implant positioning. Clin. Oral Implant. Res. 2011, 22, 485–491. [Google Scholar] [CrossRef]
- Atwood, D.A. Bone Loss of Edentulous Alveolar Ridges. J. Periodontol. 1979, 50, 11–21. [Google Scholar] [CrossRef]
- Tallgren, A. The continuing reduction of the residual alveolar ridges in complete denture wearers: A mixed-longitudinal study covering 25 years. J. Prosthet. Dent. 1972, 27, 120–132. [Google Scholar] [CrossRef]
- von Wowern, N.; Gotfredsen, K. Implant-supported overdentures, a prevention of bone loss in edentulous mandibles? A 5-year follow-up study. Clin. Oral Implant. Res. 2001, 12, 19–25. [Google Scholar] [CrossRef]
- Schulten, E.A.J.M.; Prins, H.J.; Overman, J.R.; Helder, M.N.; ten Bruggenkate, C.M.; Klein-Nuland, J. A novel approach revealing the effect of collagenous membrane on osteoconduction in maxillary sinus floor elevation with β-tricalcium phosphate. Eur. Cell. Mater. 2013, 25, 215–228. [Google Scholar] [CrossRef]
- Summers, R.B. The osteotome technique: Part 3—Less invasive methods of elevating the sinus floor. Compendium 1994, 15, 698. [Google Scholar]
- Zijderveld, S.A.; Schulten, E.J.A.M.; Aartman, I.H.A.; ten Bruggenkate, C.M. Long-term changes in graft height after maxillary sinus floor elevation with different grafting materials: Radiographic evaluation with a minimum follow-up of 4.5 years. Clin. Oral Implant. Res. 2009, 20, 691–700. [Google Scholar] [CrossRef]
- Mordenfeld, A.; Lindgren, C.; Hallman, M. Sinus Floor Augmentation Using Straumann® BoneCeramic™ and Bio-Oss® in a Split Mouth Design and Later Placement of Implants: A 5-Year Report from a Longitudinal Study. Clin. Implant Dent. Relat. Res. 2016, 18, 926–936. [Google Scholar] [CrossRef] [PubMed]
- Fienitz, T.; Moses, O.; Klemm, C.; Happe, A.; Ferrari, D.; Kreppel, M.; Ormianer, Z.; Gal, M.; Rothamel, D. Histological and radiological evaluation of sintered and non-sintered deproteinized bovine bone substitute materials in sinus augmentation procedures. A prospective, randomized-controlled, clinical multicenter study. Clin. Oral Investig. 2017, 21, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Fouad, W.; Osman, A.; Atef, M.; Hakam, M. Guided maxillary sinus floor elevation using deproteinized bovine bone versus graftless Schneiderian membrane elevation with simultaneous implant placement: Randomized clinical trial. Clin. Implant Dent. Relat. Res. 2018, 20, 424–433. [Google Scholar] [CrossRef]
- Kasabah, S.; Simůnek, A.; Krug, J.; Lecaro, M.C. Maxillary sinus augmentation with deproteinized bovine bone (Bio-Oss) and Impladent dental implant system. Part II. Evaluation of deprotienized bovine bone (Bio-Oss) and implant surface. Acta Medica 2002, 45, 167–171. [Google Scholar] [CrossRef]
- Lee, D.Z.; Chen, S.T.; Darby, I.B. Maxillary sinus floor elevation and grafting with deproteinized bovine bone mineral: A clinical and histomorphometric study. Clin. Oral Implant. Res. 2012, 23, 918–924. [Google Scholar] [CrossRef]
- Younes, F.; Cosyn, J.; De Bruyckere, T.; Cleymaet, R.; Eghbali, A. A 2-year prospective case series on volumetric changes, PROMs, and clinical outcomes following sinus floor elevation using deproteinized bovine bone mineral as filling material. Clin. Implant Dent. Relat. Res. 2019, 21, 301–309. [Google Scholar] [CrossRef]
- Erdem, N.F.; Çiftçi, A.; Acar, A.H. Three-Year Clinical and Radiographic Implant Follow-up in Sinus-Lifted Maxilla with Lateral Window Technique. Implant Dent. 2016, 25, 214–221. [Google Scholar] [CrossRef]
- Özkan, Y.; Akoğlu, B.; Kulak-Özkan, Y. Maxillary Sinus Floor Augmentation Using Bovine Bone Grafts with Simultaneous Implant Placement: A 5-Year Prospective Follow-Up Study. Implant Dent. 2011, 20, 455–459. [Google Scholar] [CrossRef]
- Shin, S.Y.; Hwang, Y.J.; Kim, J.H.; Seol, Y.J. Long-term results of new deproteinized bovine bone material in a maxillary sinus graft procedure. J. Periodontal Implant Sci. 2014, 44, 259–264. [Google Scholar] [CrossRef] [Green Version]
- Trombelli, L.; Franceschetti, G.; Stacchi, C.; Minenna, L.; Riccardi, O.; Di Raimondo, R.; Rizzi, A.; Farina, R. Minimally invasive transcrestal sinus floor elevation with deproteinized bovine bone or β-tricalcium phosphate: A multicenter, double-blind, randomized, controlled clinical trial. J. Clin. Periodontol. 2014, 41, 311–319. [Google Scholar] [CrossRef]
- Younes, F.; Eghbali, A.; De Troyer, S.; De Bruyckere, T.; Cleymaet, R.; Cosyn, J. Marginal and apical bone stability after staged sinus floor augmentation using bone condensing implants with variable-thread design: A two-dimensional analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 1135–1141. [Google Scholar] [CrossRef]
- Cordaro, L.; Bosshardt, D.D.; Palattella, P.; Rao, W.; Serino, G.; Chiapasco, M. Maxillary sinus grafting with Bio-Oss or Straumann Bone Ceramic: Histomorphometric results from a randomized controlled multicenter clinical trial. Clin. Oral Implant. Res. 2008, 19, 796–803. [Google Scholar] [CrossRef]
- Lindgren, C.; Hallman, M.; Sennerby, L.; Sammons, R. Back-scattered electron imaging and elemental analysis of retrieved bone tissue following sinus augmentation with deproteinized bovine bone or biphasic calcium phosphate. Clin. Oral Implant. Res. 2010, 9, 924–930. [Google Scholar] [CrossRef]
- Oh, J.S.; Seo, Y.S.; Lee, G.J.; You, J.S.; Kim, S.G. A Comparative Study with Biphasic Calcium Phosphate to Deproteinized Bovine Bone in Maxillary Sinus Augmentation: A Prospective Randomized and Controlled Clinical Trial. Int. J. Oral Maxillofac. Implant. 2019, 34, 233–242. [Google Scholar] [CrossRef]
- Ohe, J.Y.; Kim, G.T.; Lee, J.W.; Al Nawas, B.; Jung, J.; Kwon, Y.D. Volume stability of hydroxyapatite and β-tricalcium phosphate biphasic bone graft material in maxillary sinus floor elevation: A radiographic study using 3D cone beam computed tomography. Clin. Oral Implant. Res. 2016, 27, 348–353. [Google Scholar] [CrossRef]
- Portelli, M.; Cicciù, M.; Lauritano, F.; Cervino, G.; Manuelli, M.; Gherlone, E.F.; Lucchese, A. Histomorphometric Evaluation of Two Different Bone Substitutes in Sinus Floor Augmentation Procedures. J. Craniofac. Surg. 2017. [Google Scholar] [CrossRef]
- Wu, J.; Li, B.; Lin, X. Histological outcomes of sinus augmentation for dental implants with calcium phosphate or deproteinized bovine bone: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 1471–1477. [Google Scholar] [CrossRef]
- Cha, J.K.; Park, J.C.; Jung, U.W.; Kim, C.S.; Cho, K.S.; Choi, S.H. Case series of maxillary sinus augmentation with biphasic calcium phosphate: A clinical and radiographic study. J. Periodontal Implant Sci. 2011, 41, 98–104. [Google Scholar] [CrossRef]
- Hieu, P.D.; Chung, J.H.; Yim, S.B.; Hong, K.S. A radiographical study on the changes in height of grafting materials after sinus lift: A comparison between two types of xenogenic materials. J. Periodontal Implant Sci. 2010, 40, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Kessler, P.A.; Merten, H.A.; Neukam, F.W.; Wiltfang, J. The effects of magnitude and frequency of distraction forces on tissue regeneration in distraction osteogenesis of the mandible. Plast. Reconstr. Surg. 2002, 109, 171–180. [Google Scholar] [CrossRef]
- Kessler, P.A.; Neukam, F.W.; Wiltfang, J. Effects of distraction forces and frequency of distraction on bony regeneration. Br. J. Oral Maxillofac. Surg. 2005, 43, 392–398. [Google Scholar] [CrossRef]
- Lie, N.; Merten, H.A.; Yamauchi, K.; Wiltfang, J.; Kessler, P. Pre-implantological bone formation in the floor of the maxillary sinus in a self-supporting space. J. Craniomaxillofac. Surg. 2019, 47, 454–460. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Tan, W.C.; Zwahlen, M.; Lang, N.P. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. Part, I.; Lateral approach. J. Clin. Periodontol. 2008, 35, 216–240. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Testori, T.; Francetti, L.; Weinstein, R. Systematic review of survival rates for implants placed in the grafted maxillary sinus. Int. J. Periodontics Restor. Dent. 2004, 6, 565–577. [Google Scholar] [CrossRef]
- Helder, M.N.; van Esterik, F.A.S.; Kwehandjaja, M.D.; ten Bruggenkate, C.M.; Klein-Nulend, J.; Schulten, E.A.J.M. Evaluation of a new biphasic calcium phosphate for maxillary sinus floor elevation: Micro-CT and histomorphometrical analyses. Clin. Oral Implant. Res. 2018, 29, 488–498. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| β-TCP | BCP 20/80 | BCP 60/40 | |
|---|---|---|---|
| Porosity | 60% | 90% | 90% |
| Interconnecting macropores | 100–500 μm | 100–500 μm | 100–500 μm |
| Particle size | 700-1400 μm | 500–1000 μm | 500–1000 μm |
| Microporosity (vol%) | 1–2% | 2% | 2% |
| Crystal size | Not specified. | 1.0–6.0 μm | 0.6–6.0μm |
| Specific surface area | Not specified. | 9.5 × 10−3m2/g | 6.9 × 10−3m2/g |
| β-TCP | BCP 20/80 | BCP 60/40 | |
|---|---|---|---|
| Number of patients included | 40 | 76 | 47 |
| Number of implant sites included | 69 | 120 | 67 |
| M/F | 21 M, 19 F | 32 M, 44 F | 22 M, 25 F |
| Mean age in years | 57 | 59 | 55 |
| Age range in years | 27–78 | 18–79 | 18–77 |
| MSFE performed between | 2/2009–6/2012 | 3/2010–9/2012 | 1/2009–11/2013 |
| Months of Observation | β-TCP | BCP 20/80 | BCP 60/40 | Total | |
|---|---|---|---|---|---|
| T0 | −8 | 40 | 76 | 47 | 163 |
| T1 | −6 | 40 | 76 | 47 | 163 |
| T2 | −1 | 40 | 76 | 47 | 163 |
| T3 | 0 | 40 | 76 | 47 | 163 |
| T4 | 3 | 40 | 38 | 47 | 125 |
| T5 | 12 | 35 | 21 | 26 | 82 |
| T6 | 24 | 17 | 34 | 27 | 78 |
| T7 | 36 | 23 | 28 | 15 | 66 |
| T8 | 48 | 29 | 30 | 22 | 81 |
| T9 | 60 | 25 | 8 | 10 | 43 |
| Time Points | Months of Observation | β-TCP | BCP 20/80 | BCP 60/40 | Combined Calcium Phosphates | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Implant Site Height mm (mean ±SD) | Distal Position Height mm (mean ±SD) | Mean Tissue Height mm | Implant Site Height mm (mean ±SD) | Distal Position Height mm (mean ±SD) | Mean Tissue Height mm | Implant Site Height mm (mean ±SD) | Distal Position Height mm (mean ±SD) | Mean Tissue Height mm | Mean tissue Height Implant Site mm | Mean Tissue Height Distal Site mm | Mean Tissue Height mm | ||
| T0 | −8 | 7.4 | 6.5 | 7.0 | 6.5 | 5.8 | 6.2 | 6.5 | 5.8 | 6.2 | 6.7 | 6.2 | 6.5 |
| ± 2.8 | ± 2.3 | ± 2.6 | ± 2.4 | ± 1.8 | ± 2.1 | ± 2.6 | ± 1.9 | ± 2.3 | ± 2.6 | ± 2.0 | ± 2.3 | ||
| T1 | −6 | 14.2 | 12.8 | 13.5 | 14.0 | 12.8 | 13.4 | 14.2 | 13.0 | 13.6 | 14.1 | 12.8 | 13.5 |
| ± 2.2 | ± 2.8 | ± 2.6 | ± 2.2 | ± 2.5 | ± 2.4 | ± 2.1 | ± 2.2 | ± 2.2 | ± 2.2 | ± 2.5 | ± 2.4 | ||
| T2 | −1 | 13.2 | 11.8 | 12.5 | 13.6 | 12.5 | 13.1 | 14.0 | 12.7 | 13.4 | 13.5 | 12.4 | 13.0 |
| ± 2.4 | ± 2.8 | ± 2.7 | ± 2.3 | ± 2.5 | ± 2.4 | ± 1.9 | ± 2.1 | ± 2.1 | ± 2.2 | ± 2.5 | ± 2.4 | ||
| T3 | 0 | 13.5 | 11.8 | 12.7 | 13.6 | 12.0 | 12.8 | 13.9 | 12.5 | 13.2 | 13.6 | 12.1 | 12.9 |
| ± 2.2 | ± 2.8 | ± 2.6 | ± 2.2 | ± 2.7 | ± 2.6 | ± 1.8 | ± 2.2 | ± 2.1 | ± 2.1 | ± 2.6 | ± 2.5 | ||
| T4 | 3 | 13.1 | 11.5 | 12.3 | 13.3 | 11.7 | 12.5 | 13.6 | 12.2 | 12.9 | 13.3 | 11.8 | 12.6 |
| ± 2.2 | ± 2.6 | ± 2.5 | ± 2.4 | ± 2.7 | ± 2.7 | ± 1.9 | ± 2.2 | ± 2.2 | ± 2.2 | ± 2.6 | ± 2.5 | ||
| T5 | 12 | 12.6 | 10.7 | 11.7 | 13.3 | 11.8 | 12.6 | 13.6 | 11.8 | 12.7 | 13.2 | 11.4 | 12.3 |
| ± 2.1 | ± 2.5 | ± 2.5 | ± 2.4 | ± 2.8 | ± 2.7 | ± 2.0 | ± 2.3 | ± 2.3 | ± 2.2 | ± 2.7 | ± 2.6 | ||
| T6 | 24 | 12.1 | 10.9 | 11.5 | 13.0 | 11.0 | 12.0 | 13.8 | 12.3 | 13.1 | 13.0 | 11.4 | 12.2 |
| ± 1.7 | ± 2.7 | ± 2.3 | ± 2.3 | ± 3.1 | ± 2.9 | ± 2.2 | ± 2.2 | ± 2.3 | ± 2.2 | ± 2.7 | ± 2.6 | ||
| T7 | 36 | 12.4 | 10.5 | 11.5 | 11.8 | 10.1 | 11.0 | 13.2 | 11.5 | 12.4 | 12.6 | 10.8 | 11.8 |
| ± 2.3 | ± 2.6 | ± 2.6 | ± 1.9 | ± 2.6 | ± 2.4 | ± 2.0 | ± 2.5 | ± 2.3 | ± 2.0 | ± 2.6 | ± 2.5 | ||
| T8 | 48 | 12.7 | 10.6 | 11.7 | 12.8 | 10.9 | 11.9 | 13.0 | 11.6 | 12.3 | 12.8 | 11.0 | 11.9 |
| ± 2.1 | ± 2.8 | ± 2.6 | ± 2.5 | ± 2.8 | ± 2.8 | ± 1.8 | ± 2.2 | ± 2.1 | ± 2.1 | ± 2.6 | ± 2.6 | ||
| T9 | 60 | 12.4 | 10.4 | 11.4 | 12.4 | 10.3 | 11.4 | 12.4 | 11.1 | 11.8 | 12.4 | 10.5 | 11.5 |
| ± 1.6 | ± 2.2 | ± 2.2 | ± 2.8 | ± 3.4 | ± 3.1 | ± 1.7 | ± 1.8 | ± 1.8 | ± 1.8 | ± 2.3 | ± 2.3 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bouwman, W.F.; Bravenboer, N.; ten Bruggenkate, C.M.; Eijsackers, F.A.; Stringa, N.; Schulten, E.A.J.M. Tissue Level Changes after Maxillary Sinus Floor Elevation with Three Types of Calcium Phosphate Ceramics: A Radiological Study with a 5-Year Follow-Up. Materials 2021, 14, 1471. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14061471
Bouwman WF, Bravenboer N, ten Bruggenkate CM, Eijsackers FA, Stringa N, Schulten EAJM. Tissue Level Changes after Maxillary Sinus Floor Elevation with Three Types of Calcium Phosphate Ceramics: A Radiological Study with a 5-Year Follow-Up. Materials. 2021; 14(6):1471. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14061471
Chicago/Turabian StyleBouwman, Wilhelmus F., Nathalie Bravenboer, Christiaan M. ten Bruggenkate, Francis A. Eijsackers, Najada Stringa, and Engelbert A. J. M. Schulten. 2021. "Tissue Level Changes after Maxillary Sinus Floor Elevation with Three Types of Calcium Phosphate Ceramics: A Radiological Study with a 5-Year Follow-Up" Materials 14, no. 6: 1471. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14061471