Nonenzymatic Serum Antioxidant Capacity in IBD and Its Association with the Severity of Bowel Inflammation and Corticosteroids Treatment

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Analytical Methods
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. Patients
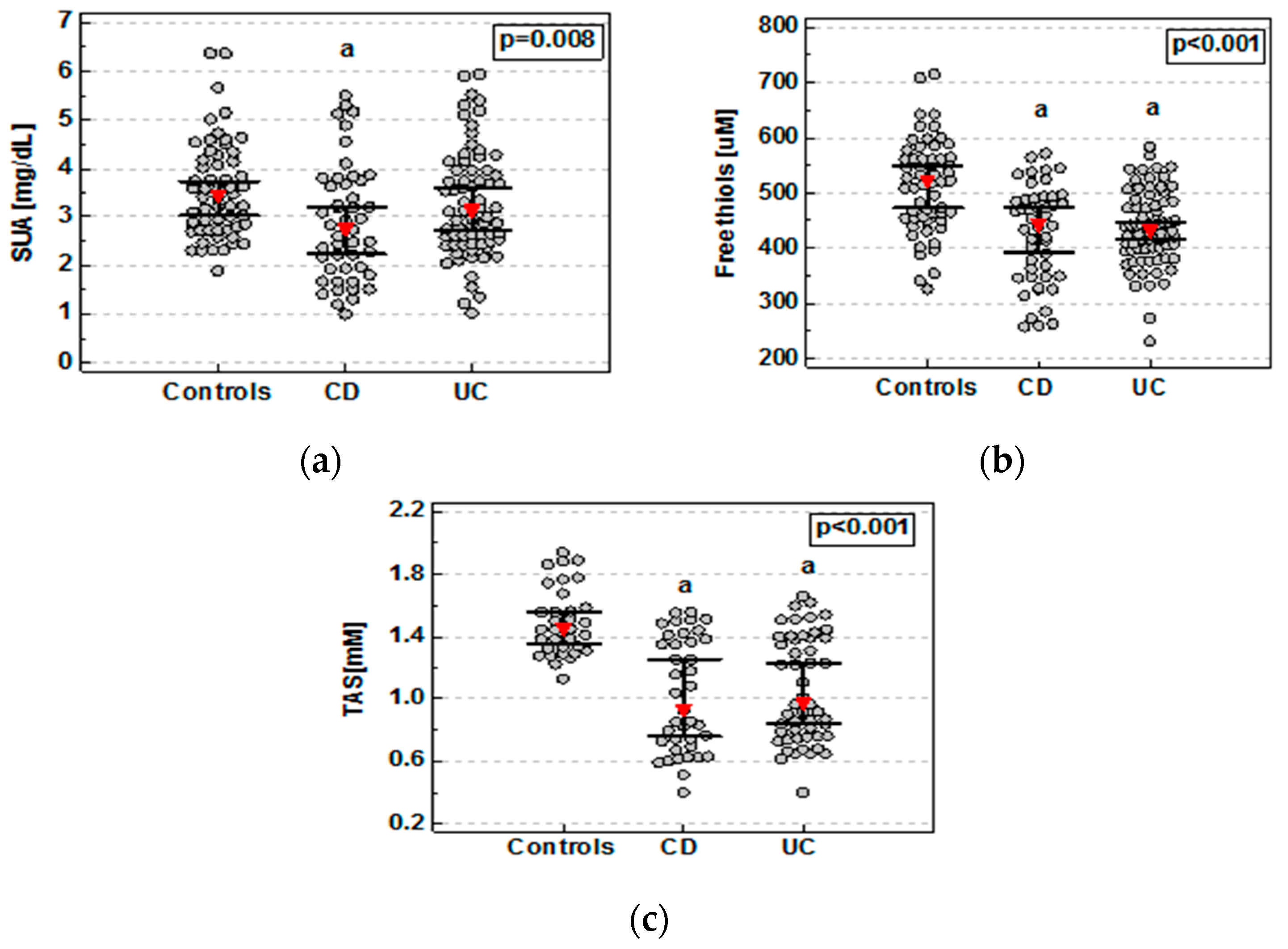
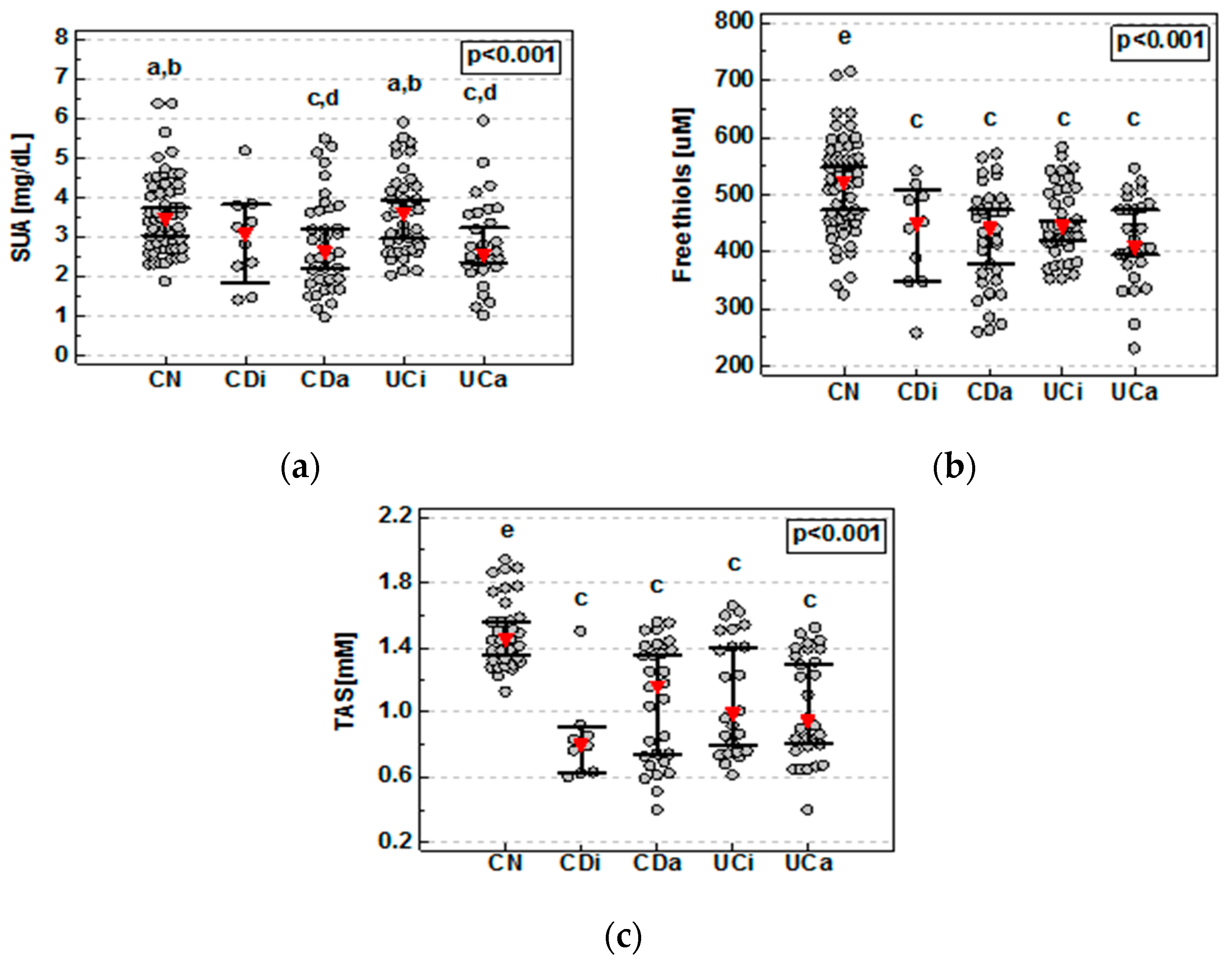
3.2. Nonenzymatic Serum Antioxidants in IBD
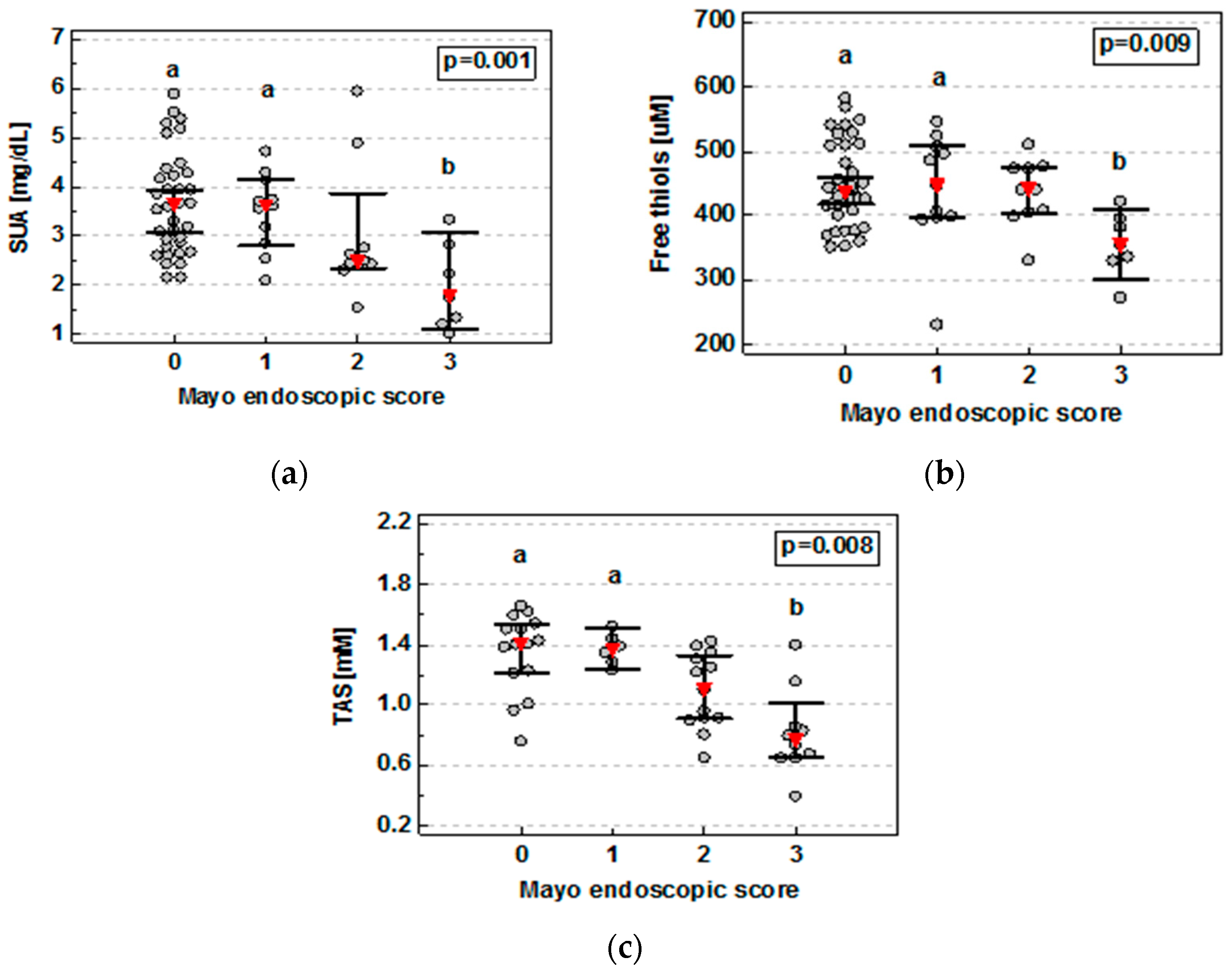
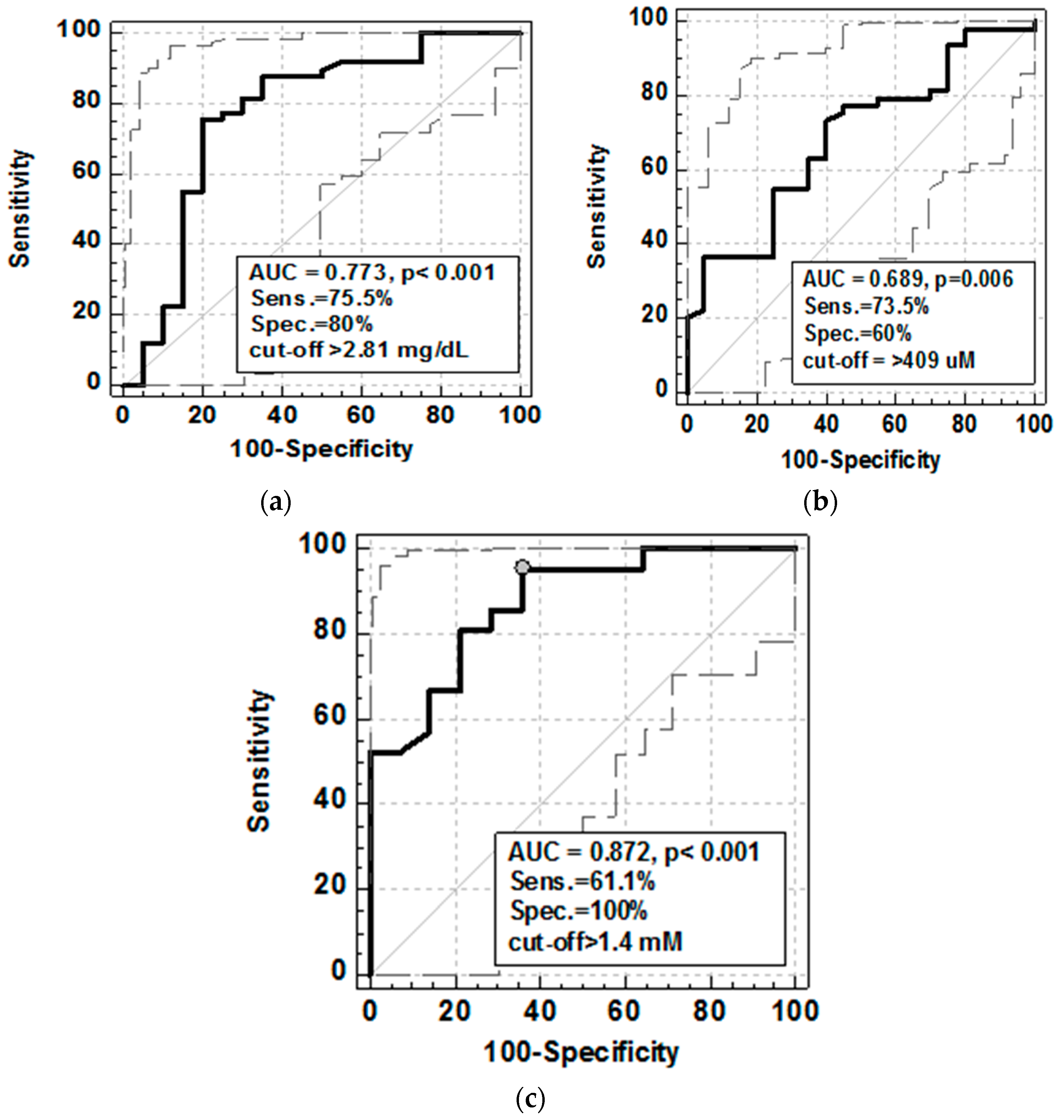
3.3. Nonenzymatic Serum Antioxidants and Mucosal Healing (MH)
3.4. Nonenzymatic Serum Antioxidants and Inflammatory and Oxidative Stress Markers
3.5. Nonenzymatic Serum Antioxidants and Anemia
3.6. Nonenzymatic Serum Antioxidants and Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Colombel, J.F.; Mahadevan, U. Inflammatory bowel disease 2017: Innovations and changing paradigms. Gastroenterology 2017, 152, 309–312. [Google Scholar] [CrossRef]
- De Souza, H.; Fiocchi, C. Network medicine: A mandatory next step for inflammatory bowel disease. Inflamm. Bowel Dis. 2018, 4, 671–679. [Google Scholar] [CrossRef]
- Daperno, M.; Castiglione, F.; de Ridder, L.; Dotan, I.; Färkkilä, M.; Florholmen, J.; Fraser, G.; Fries, W.; Hebuterne, X.; Lakatos, P.L.; et al. Results of the 2nd part ScientificWorkshop of the ECCO (II): Measures and markers of prediction to achieve, detect, and monitor intestinal healing in Inflammatory Bowel Disease. J. Crohn’s Colitis 2011, 5, 484–498. [Google Scholar] [CrossRef]
- Atreya, R.; Neurath, M.F. Current and future targets for mucosal healing in inflammatory bowel disease. Visc. Med. 2017, 33, 82–88. [Google Scholar] [CrossRef]
- Pereira, C.C.; Duraes, C.; Coelho, R.; Gracio, D.; Silva, M.; Peixoto, A.; Lago, P.; Pereira, M.; Catarino, T.; Pinho, S.; Teixeira, J.P.; et al. Association between polymorphisms in antioxidant genes and inflammatory bowel disease. PLoS ONE 2017. [Google Scholar] [CrossRef]
- Balmus, I.M.; Ciobica, A.; Trifan, A.; Stanciu, C. The Implications of Oxidative Stress and Antioxidant Therapies in Inflammatory Bowel Disease: Clinical Aspects and Animal Models. Saudi J. Gastroenterol. 2016, 22, 3–17. [Google Scholar] [CrossRef]
- Krzystek-Korpacka, M.; Neubauer, K.; Berdowska, I.; Boehm, D.; Zieliński, B.; Petryszyn, P.; Terlecki, G.; Paradowski, L.; Gamian, A. Enhanced formation of advanced oxidation protein products in IBD. Inflamm. Bowel Dis. 2008, 146, 794–802. [Google Scholar] [CrossRef]
- Boehm, D.; Krzystek-Korpacka, M.; Neubauer, K.; Matusiewicz, M.; Paradowski, L.; Gamian, A. Lipid peroxidation markers in Crohn’ s disease: The associations and diagnostic value. Clin. Chem. Lab. Med. 2012, 50, 1359–1366. [Google Scholar] [CrossRef]
- Boehm, D.; Krzystek-Korpacka, M.; Neubauer, K.; Matusiewicz, M.; Berdowska, I.; Zielinski, B.; Paradowski, L.; Gamian, A. Paraoxonase-1 status in Crohn’s disease and ulcerative colitis. Inflamm. Bowel Dis. 2009, 15, 93–99. [Google Scholar] [CrossRef]
- Krzystek-Korpacka, M.; Neubauer, K.; Berdowska, I.; Zielinski, B.; Paradowski, L.; Gamian, A. Impaired erythrocyte antioxidant defense in active inflammatory bowel disease: Impact of anemia and treatment. Inflamm. Bowel Dis. 2010, 16, 1467–1475. [Google Scholar] [CrossRef]
- Shearn, C.T.; Orlicky, D.J.; Petersen, D.R. Dysregulation of antioxidant responses in patients diagnosed with concomitant primary sclerosing cholangitis/inflammatory bowel disease. Exp. Mol. Pathol. 2018, 104, 1–8. [Google Scholar] [CrossRef]
- Rentsch, M.; Beham, A.; Schlitt, H.J.; Jauch, K.W. Crohn’s Disease Activity Index and Vienna Classification—Is it worthwhile to calculate before surgery? Dig. Surg. 2006, 23, 241–249. [Google Scholar] [CrossRef]
- Rutgeerts, P.; Sandborn, W.J.; Feagan, B.G.; Reinisch, W.; Olson, A.; Johanns, J.; Travers, S.; Rachmilewitz, D.; Hanauer, S.B.; Lichtenstein, G.R.; et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med. 2005, 353, 2462–2476. [Google Scholar] [CrossRef] [PubMed]
- Bartosz, G. Druga Twarz Tlenu. Wolne Rodniki w Przyrodzie. (The Other Face of Oxygen. Free Radicals in the Environment), 2nd ed.; Wydawnictwo Naukowe PWN: Warszawa, Poland, 2004. [Google Scholar]
- Witko-Sarsat, V.; Friedlander, M.; Capeillère-Blandin, C.; Nguyen-Khoa, T.; Nguyen, A.T.; Zingraff, J.; Jungers, P.; Descamps-Latscha, B. Advanced oxidation protein products as a novel marker of oxidative stress in uremia. Kidney Int. 1996, 49, 1304–1313. [Google Scholar] [CrossRef] [Green Version]
- Matusiewicz, M.; Neubauer, K.; Lewandowska, P.; Gamian, A.; Krzystek-Korpacka, M. Reduced transferin levels in active inflammatory bowel disease. BioMed Res. Int. 2017, 2017, 9541370. [Google Scholar] [CrossRef] [PubMed]
- Pereira, C.; Gracio, D.; Teixeira, J.P.; Magro, F. Oxidative stress and DNA damage: Implications in inflammatory bowel disease. Inflamm. Bowel Dis. 2015, 21, 2403–2417. [Google Scholar] [CrossRef] [PubMed]
- Tian, T.; Wang, Z.; Zhang, J. Pathomechanisms of oxidative stress in inflammatory bowel disease and potential antioxidant therapies. Oxid. Med. Cell. Longev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Robles, H.V.; Madrid, A.F.C.; Ponce, A.G.; Silva Olivares, A.; Shibayama, M.; Betanzos, A.; Del Valle Mondragón, L.; Nava, P.; Schnoor, M. Experimental colitis is attenuated by cardioprotective diet supplementation that reduces oxidative stress, inflammation, and mucosal damage. Oxid. Med. Cell. Longev. 2016, 2016, 8473242. [Google Scholar] [CrossRef]
- Pearson, D.C.; Jourd’Heuil, D.; Meddings, J.B. The anti-oxidant properties of 5-aminosalicylic acid. Free Radic. Biol. Med. 1996, 21, 367–373. [Google Scholar] [CrossRef]
- Lopez, A.; Pouillon, L.; Beaugerie, L.; Danese, S.; Peyrin-Biroulet, L. Colorectal cancer prevention in patients with ulcerative colitis. Best Pract. Res. Clin. Gastroenterol. 2018, 32–33, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Piechota-Polanczyk, A.; Fichna, J. Review article: The role of oxidative stress in pathogenesis and treatment of inflammatory bowel diseases. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2014, 387, 605–620. [Google Scholar] [CrossRef] [PubMed]
- Leníček, M.; Ďuricová, D.; Hradsky, O.; Dušátková, P.; Jirásková, A.; Lukáš, M.; Nachtigal, P.; Vítek, L. The Relationship between serum bilirubin and Crohn’s disease. Inflamm. Bowel Dis. 2014, 3, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Schieffer, K.M.; Bruffy, S.M.; Rauscher, R.; Koltun, W.A.; Yochum, G.S.; Gallagher, C.J. Reduced total serum bilirubin levels are associated with ulcerative colitis. PLoS ONE 2017, 12, e0179267. [Google Scholar] [CrossRef] [PubMed]
- Frick, A.; Khare, V.; Paul, G.; Lang, M.; Ferk, F.; Knasmüller, S.; Beer, A.; Oberhuber, G.; Gasche, C. Overt increase of oxidative stress and DNA damage in murine and human colitis and colitis-associated neoplasia. Mol. Cancer Res. 2018, 16, 634–642. [Google Scholar] [CrossRef]
- Annese, V.; Beaugerie, L.; Egan, L.; Biancone, L.; Bolling, C.; Brandts, C.; Dierickx, D.; Dummer, R.; Fiorino, G.; Gornet, J.M. European evidence-based consensus: Inflammatory bowel disease and malignancies. J. Crohn’s Colitis 2015, 9, 945–965. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.S.; Burakoff, R. Extraintestinal Manifestations of Inflammatory Bowel Disease. Gastroenterol. Hepatol. 2011, 7, 235–241. [Google Scholar]
- Harbord, M.; Annese, V.; Vavricka, S.R.; Allez, M.; Barreiro-de Acosta, M.; Boberg, K.M.; Burisch, J.; De Vos, M.; De Vries, A.M.; Dick, A.D. The first European evidence-based consensus on extra-intestinal manifestations in inflammatory bowel disease. J. Crohn’s Colitis 2016, 10, 239–254. [Google Scholar] [CrossRef]
- Solmaz, D.; Kozacı, D.; Sarı, İ.; Taylan, A.; Önen, F.; Akkoç, N.; Akar, S. Oxidative stress and related factors in patients with ankylosing spondylitis. Eur. J. Rheumatol. 2016, 3, 20–24. [Google Scholar] [CrossRef]
- Lin, X.; Huang, T. Oxidative stress in psoriasis and potential therapeutic use of antioxidants. Free Radic. Res. 2016, 50, 585–595. [Google Scholar] [CrossRef]
- Cichoż-Lach, H.; Michalak, A. Oxidative stress as a crucial factor in liver diseases. World J. Gastroenterol. 2014, 20, 8082–8091. [Google Scholar] [CrossRef]
- Bissinger, R.; Bhuyan, A.A.M.; Qadri, S.M.; Lang, F. Oxidative stress, eryptosis and anemia: A pivotal mechanistic nexus in systemic diseases. FEBS J. 2018. [Google Scholar] [CrossRef] [PubMed]
- Dignas, A.U.; Gasche, C.; Bettenworth, D.; Birgegård, G.; Danese, S.; Gisbert, J.P.; Gomollon, F.; Iqbal, T.; Katsanos, K.; Koutroubakis, I. European consensus on the diagnosis and management of iron deficiency and anaemia in inflammatory bowel disease. J. Crohn’s Colitis 2015, 9, 211–222. [Google Scholar] [CrossRef]
- Kim, M.; Basharat, A.; Santosh, R.; Mehdi, S.F.; Razyi, Z.; Yoo, S.K.; Lowell, B.; Kumar, A.; Brima, W.; Danoff, A.; et al. Reuniting overnutrition and undernutrition, macronutrients and micronutrients. Diabet. Metab. Res. Rev. 2018, e3072. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Lario, B.; Macarron-Vicente, J. Is there anything good in uric acid? Q. J. Med. 2011, 104, 1015–1024. [Google Scholar] [CrossRef] [Green Version]
- Jamnik, J.; Rehman, S.; Blanco, M.S.; de Souza, R.J.; Khan, T.A.; Leiter, L.A.; Wolever, T.M.; Kendall, C.W.; Jenkins, D.J.; Sievenpiper, J.L. Fructose intake and risk of gout and hyperuricemia: A systematic review and meta-analysis of prospective cohort studies. BMJ Open 2016, 6, e01319. [Google Scholar] [CrossRef]
- Forbes, A.; Escher, J.; Hebuterne, X.; Kłęk, S.; Krznaric, Z.; Schneider, S.; Shamir, R.; Sterdelova, K.; Wierdsma, N.; Wiskin, A.E.; et al. ESPEN guideline: Clinical nutrition in inflammatory bowel disease. Clin. Nutr. 2017, 36, 321–347. [Google Scholar] [CrossRef] [Green Version]
- Zhu, F.; Feng, D.; Zhang, T. Uric acid metabolism was altered in isolated colonic Crohn’s disease but not ulcerative colitis. J. Gastroenterol. Hepatol. 2018. [Google Scholar] [CrossRef]
- Sendid, B.; Jawhara, S.; Sarter, H.; Maboudou, P.; Thierny, C.; Gower-Rousseau, C.; Colombel, J.F.; Poulain, D. Uric acid levels are independent of anti-Saccharomycescerevisiae antibodies (ASCA) in Crohn’s disease: A reappraisal of the role of S.cerevisiae in this setting. Virulence 2018. [Google Scholar] [CrossRef]
- Koutroubakis, I.E.; Malliaraki, N.; Dimoulios, P.D.; Karmiris, K.; Castanas, E.; Kouroumalis, E.A. Decreased total and corrected antioxidant capacity in patients with inflammatory bowel disease. Dig. Dis. Sci. 2014, 49, 1433–1437. [Google Scholar] [CrossRef]
- Belikov, A.V.; Schraven, B.; Simeoni, L. T cells and reactive oxygen species. J. Biomed. Sci. 2015, 22, 85. [Google Scholar] [CrossRef] [PubMed]
- Coulson, G.B.; Johnson, B.K.; Zheng, H.; Colvin, C.J.; Fillinger, R.J.; Haiderer, E.R.; Hammer, N.D.; Abramovitch, R.B. Targeting Mycobacterium tuberculosis sensitivity to thiol stress at acidic pH kills the bacterium and potentiates antibiotics. Cell. Chem. Biol. 2017, 24, 993–1004. [Google Scholar] [CrossRef]
- Guney, T.; Kanat, I.F.; Alkan, A.; Alisik, M.; Akinci, S.; Silay, K.; Neselioglu, S.; Dilek, I.; Erel, O. Assessment of serum thiol/disulfidehomeostasis in multiple myeloma patients by a new method. Redox Rep. 2017, 22, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Frenay, A.S.; de Borst, M.H.; Bachtler, M.; Tschopp, N.; Keyzer, C.A.; van den Berg, E.; Bakker, S.J.L.; Feelisch, M.; Pasch, A.; van Goor, H. Serum free sulfhydryl status is associated with patient and graft survival in renal transplant recipients. Free Radic. Biol. Med. 2016, 99, 345–351. [Google Scholar] [CrossRef] [Green Version]
- Koning, A.M.; Meijers, W.C.; Pasch, A.; Leuvenink, H.G.D.; Frenay, A.S.; Dekker, M.M.; Feelisch, M.; de Boer, R.A.; van Goor, H. Serum free thiols in chronic heart failure. Pharmacol. Res. 2016, 111, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Elmas, B.; Erel, Ö.; Ersavaş, D.; Yürümez, Y. Thiol/disulfide homeostasis as a novel indicator of oxidative stress in children with simple febrile seizures. Neurol. Sci. 2017, 38, 1969–1975. [Google Scholar] [CrossRef]
- Nakashima, F.; Shibata, T.; Kamiya, K.; Yoshitake, J.; Kikuchi, R.; Matsushita, T.; Ishii, I.; Giménez-Bastida, J.A.; Schneider, C.; Uchida, K. Structural and functional insights into S-thiolation of human serum albumins. Sci. Rep. 2018, 8, 932. [Google Scholar] [CrossRef] [Green Version]
- Gionchetti, P.; Rizzello, F.; Annese, V.; Armuzzi, A.; Biancone, L.; Castiglione, F.; Comberlato, M.; Cottone, M.; Danese, S.; Daperno, M.; et al. Italian Group for the Study of Inflammatory Bowel Disease (IG-IBD).Use of corticosteroids and immunosuppressive drugs in inflammatory bowel disease: Clinical practice guidelines of the Italian Group for the Study of Inflammatory Bowel Disease. Dig. Liver Dis. 2017, 49, 604–617. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, X.; Hu, C.A. Therapeutic potential of amino acids in inflammatory bowel disease. Nutrients 2017, 9, 920. [Google Scholar] [CrossRef]
- Mazzuoli, S.; Guglielmi, F.W.; Antonelli, E.; Salemme, M.; Bassotti, G.; Vllanacci, V. Definition and evaluation of mucosal healing in clinical practice. Dig. Liver Dis. 2013, 45, 969–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waljee, A.K.; Wiitala, W.L.; Govani, S.; Stidham, R.; Saini, S.; Hou, J.; Feagins, L.A.; Khan, N.; Good, C.B.; Vijan, S.; Higgins, P.D.R. Corticosteroid use and complications in a US inflammatory bowel disease cohort. PLoS ONE 2016, 11, e0158017. [Google Scholar] [CrossRef]
- Katz, J.A. Treatment of inflammatory bowel disease with corticosteroids. Gastroenterol. Clin. N. Am. 2004, 33, 171–189. [Google Scholar] [CrossRef] [PubMed]
- Krzystek-Korpacka, M.; Neubauer, K.; Matusiewicz, M. Platelet-derived growth factor-BB reflects clinical, inflammatory and angiogenic disease activity and oxidative stress in inflammatory bowel disease. Clin. Biochem. 2009, 42, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- Neubauer, K.; Matusiewicz, M.; Bednarz-Misa, I.; Gorska, S.; Gamian, A.; Krzystek-Korpacka, M. Diagnostic potential of systemic eosinophil-associated cytokines and growth factors in IBD. Gastroenterol. Res. Pract. 2018, 2018, 7265812. [Google Scholar] [CrossRef]
- You, J.M.; Yun, S.J.; Nam, K.N.; Kang, C.; Won, R.; Lee, E.H. Mechanism of glucocorticoid-induced oxidative stress in rat hippocampal slice cultures. Can. J. Physiol. Pharmacol. 2009, 87, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Sasaki, E.; Higuchi, S.; Takai, S.; Tsuneyama, K.; Fukami, T.; Nakajima, M.; Yokoi, T. Involvement of oxidative stress and immune- and inflammation-related factors in azathioprine-induced liver injury. Toxicol. Lett. 2014, 224, 215–224. [Google Scholar] [CrossRef]
- Misdaq, M.; Ziegler, S.; von Ahsen, N.; Oellerich, M.; Asif, A.R. Thiopurines induce oxidative stress in T-lymphocytes: A proteomic approach. Mediat. Inflamm. 2015, 2015, 434825. [Google Scholar] [CrossRef] [PubMed]
- Haberman, F.; Tang, S.C.; Arumugam, T.V.; Hyun, D.H.; Yu, Q.S.; Cutler, R.G.; Guo, Z.; Holloway, H.W.; Greig, N.H.; Mattson, M.P. Soluble neuroprotective antioxidant uric acid analogs ameliorate ischemic brain injury in mice. Neuromol. Med. 2007, 9, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Rezaie, A.; Parker, R.D.; Abdollahi, M. Oxidative stress and pathogenesis of inflammatory bowel disease: An epiphenomenon or the cause? Dig. Dis. Sci. 2007, 52, 2015–2021. [Google Scholar] [CrossRef]
- Yadav, V.; Varum, F.; Bravo, R.; Furrer, E.; Bojic, D.; Basit, A.W. Inflammatory bowel disease: Exploring gut pathophysiology for novel therapeutic targets. Transl. Res. 2016, 176, 38–68. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Controls | CD Patients | UC Patients | p-Value |
|---|---|---|---|---|
| Number of cases | 57 | 47 | 71 | |
| Sex (F/M) | 27/30 | 23/24 | 31/40 | 0.837 Χ2 |
| Age [years] | 42 (35–50.4) | 40 (30.6–42.7) | 46 (36.1–50.2) | 0.260 K |
| Active disease, n (%) | - | 37 (78.7) | 30 (42.3%) | <0.001 F |
| CS, n (%) | - | 20 (42.6) | 23 (32.4) | 0.329 F |
| AZA, n (%) | - | 19 (40.4) | 15 (21.1) | 0.037 F |
| BMI [kg/m2] | 25 (21.7–28.2) | 23.1 (21.4–24.7) | 23.5 (22.4–24.6) | 0.445 A |
| ALB [g/dL] | 4.77 (4.7–4.9) a,b | 4.23 (4.1–4.4) b,c | (4.48 (4.4–4.6) a,c | <0.001 A |
| hsCRP [mg/L] | 1.84 (0.84–4.95) a,b | 52.9 (17.4–99.3) c | 25 (13.8–43.5) c | <0.0001 K |
| HGB [g/dL] | 13.2 (12.3–15) | 12.1 (11.4–12.6) | 12.8 (12.2–13.5) | 0.084 K |
| Iron [μM] | 18.6 (15.7–21.4) a,b | 10.8 (8–12.5) b,c | 15.5 (13.4–17.6) a,c | <0.0001 K |
| ESR [mm/hr] | 9 (7.2–15) a | 20 (16.8–26.5) b | 14.5 (11.7–22) | 0.018 K |
| PLT [×103/mm3] | 250 (216–320) a | 367 (330–411) b,c | 292 (276–316) a | 0.011 K |
| WBC [×103/mm3] | 6 (5.47–6.61) | 6.35 (5.6–8.16) | 6.4 (5.8–7.53) | 0.474 K |
| IL-1 [pg/mL] | 0.79 (0.31–1.71) | 0.93 (0.59–1.37) | 0.94 (0.7–1.41) | 0.550 K |
| IL-6 [pg/mL] | 0.77 (0.68–1.14) a,b | 2.57 (1.83–3.84) c | 1.99 (1.23–2.82) c | <0.0001 K |
| TNF [pg/mL] | 0.83 (0.4–1.44) | 0.77 (0.37–1.04) | 0.53 (0.35–0.94) | 0.914 K |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neubauer, K.; Kempinski, R.; Matusiewicz, M.; Bednarz-Misa, I.; Krzystek-Korpacka, M. Nonenzymatic Serum Antioxidant Capacity in IBD and Its Association with the Severity of Bowel Inflammation and Corticosteroids Treatment. Medicina 2019, 55, 88. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55040088
Neubauer K, Kempinski R, Matusiewicz M, Bednarz-Misa I, Krzystek-Korpacka M. Nonenzymatic Serum Antioxidant Capacity in IBD and Its Association with the Severity of Bowel Inflammation and Corticosteroids Treatment. Medicina. 2019; 55(4):88. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55040088
Chicago/Turabian StyleNeubauer, Katarzyna, Radoslaw Kempinski, Malgorzata Matusiewicz, Iwona Bednarz-Misa, and Malgorzata Krzystek-Korpacka. 2019. "Nonenzymatic Serum Antioxidant Capacity in IBD and Its Association with the Severity of Bowel Inflammation and Corticosteroids Treatment" Medicina 55, no. 4: 88. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55040088