Daily Heart Rate Variability Indices in Subjects with and Without Metabolic Syndrome Before and After the Elimination of the Influence of Day-time Physical Activity


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
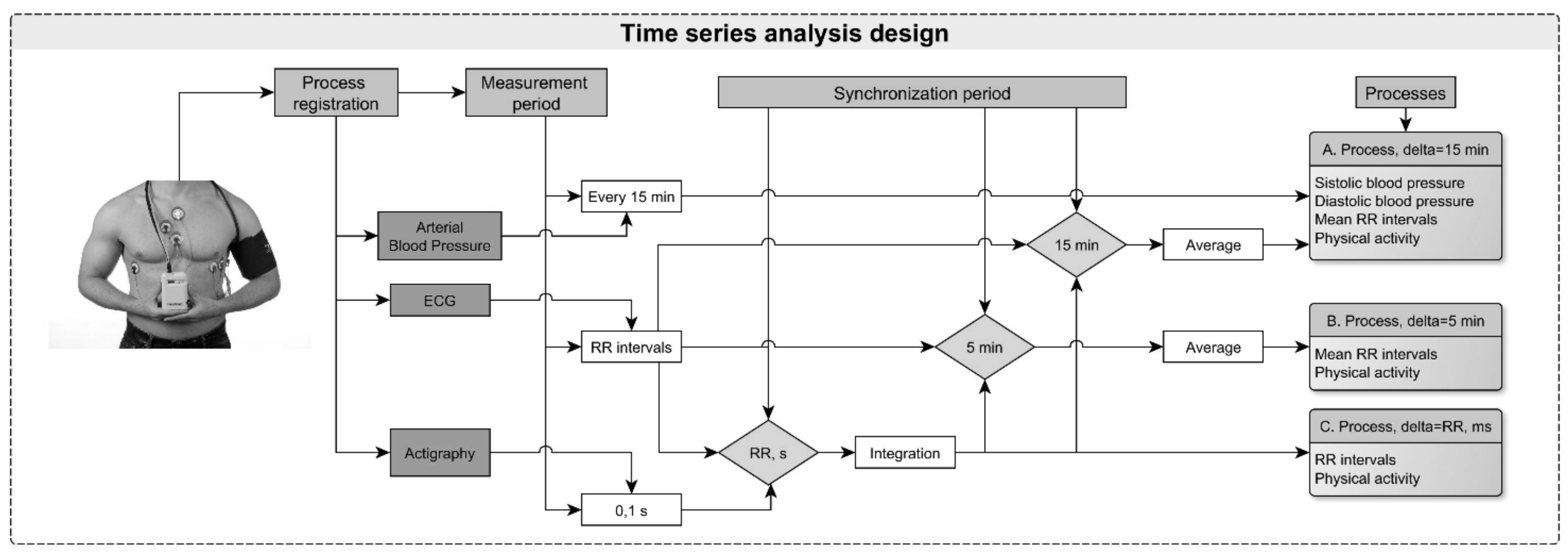
2.2. Study Protocol and Measurements Used
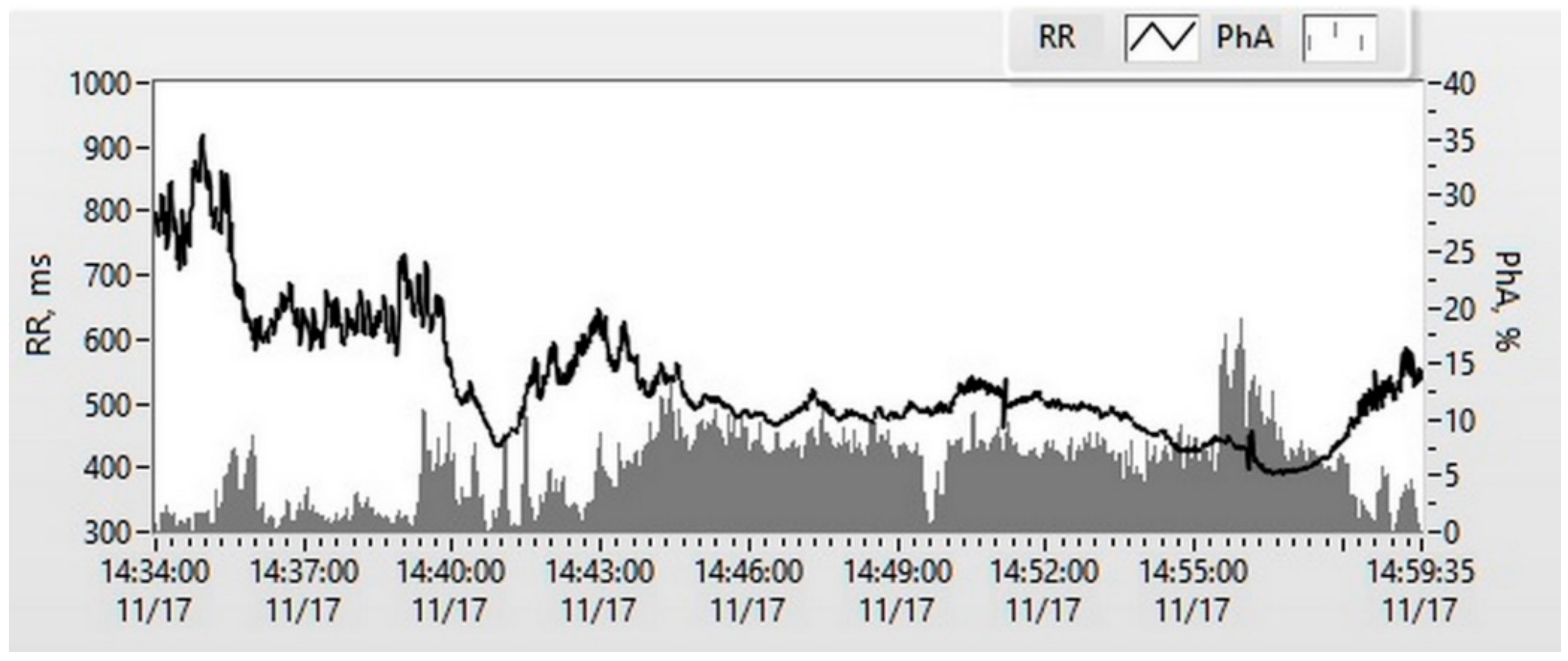
2.3. Data Analysis
2.4. Sequence Transformations
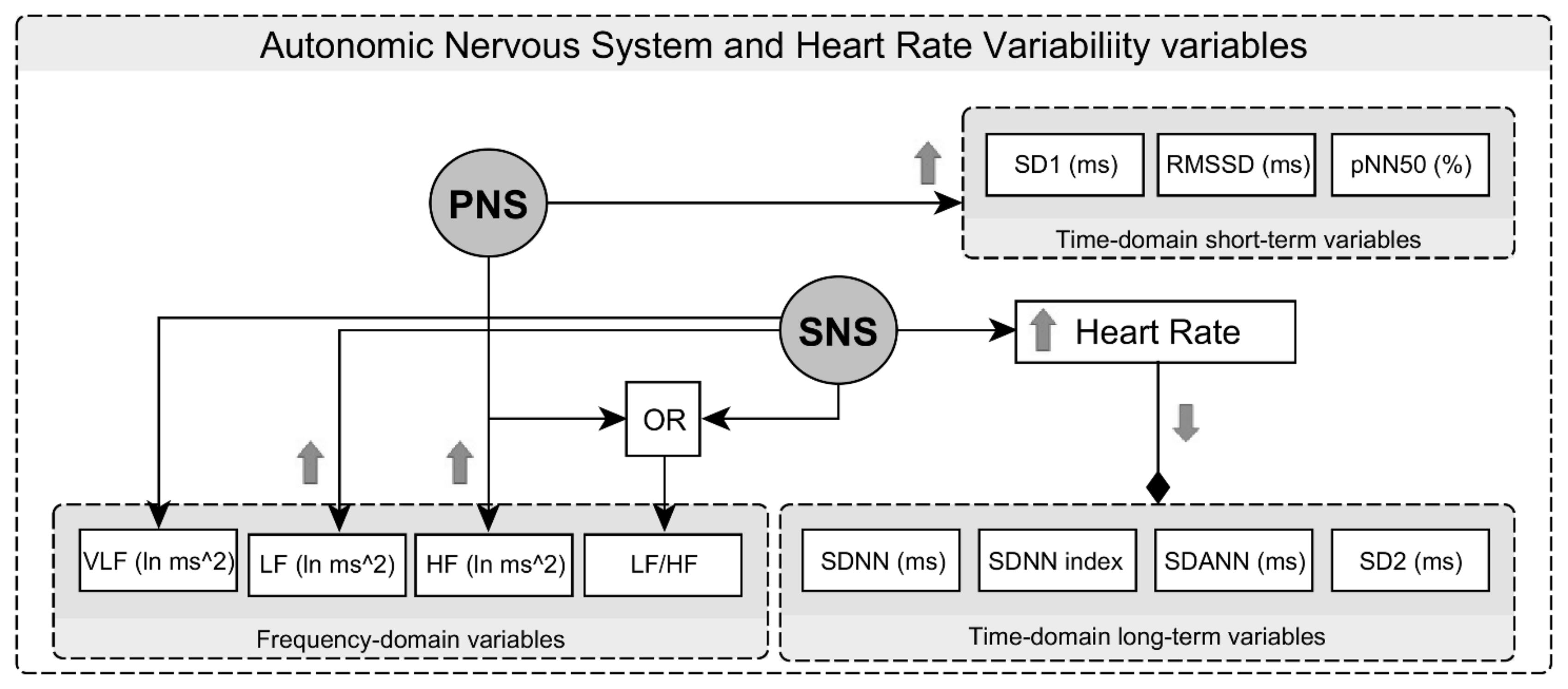
2.5. Time-Domain and Frequency-Domain Analysis of RRI
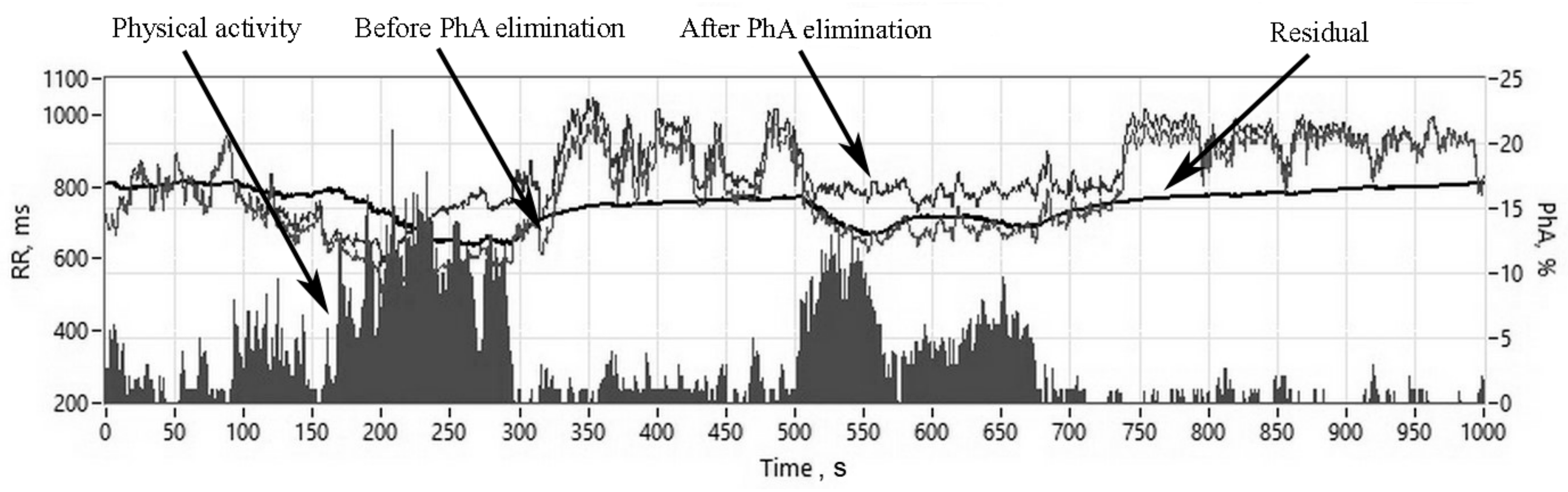
2.6. Assessment of Physical Activity-Related HRV Changes
2.7. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics
3.2. Heart Rate Variability Characteristics Before the Elimination of Physical Activity Influence
3.3. Heart Rate Variability Characteristics after Elimination of Physical Activity Influence
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Laucevičius, A.; Rinkūnienė, E.; Skorniakov, V.; Petrulionienė, Ž.; Kasiulevičius, V.; Jatužis, D.; Ryliškytė, L.; Badarienė, J.; Klumbienė, J.; Šlapikas, R. High-risk profile in a region with extremely elevated cardiovascular mortality. Hell. J. Cardiol. 2013, 54, 441–447. [Google Scholar]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corra, U.; Cosyns, B.; Deaton, C. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [PubMed]
- Petrie, J.R.; Guzik, T.J.; Touyz, R.M. Diabetes, hypertension, and cardiovascular disease: Clinical insights and vascular mechanisms. Can. J. Cardiol. 2018, 34, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Laucevičius, A.; Rinkūnienė, E.; Petrulionienė, Ž.; Puronaitė, R.; Kasiulevičius, V.; Jatužis, D.; Ryliškytė, L.; Badarienė, J.; Čypienė, A.; Navickas, R. Prevalence of high-risk profile in middle-aged subjects with arterial hypertension: A nationwide survey. Blood Press. 2014, 23, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Laucevičius, A.; Kasiulevičius, V.; Jatužis, D.; Petrulionienė, Ž.; Ryliškytė, L.; Rinkūnienė, E.; Badarienė, J.; Gustienė, O.; Šlapikas, R. Lithuanian High Cardiovascular Risk (LitHiR) primary prevention programme-rationale and design. Semin. Cardiovasc. Med. 2012, 18, 1–6. [Google Scholar] [CrossRef]
- Grassi, G.; Biffi, A.; Seravalle, G.; Trevano, F.Q.; Dell’Oro, R.; Corrao, G.; Mancia, G. Sympathetic Neural Overdrive in the Obese and Overweight State: Meta-Analysis of Published Studies. Hypertension 2019, 74, 349–358. [Google Scholar] [CrossRef]
- Esler, M.; Straznicky, N.; Eikelis, N.; Masuo, K.; Lambert, G.; Lambert, E. Mechanisms of Sympathetic Activation in Obesity-Related Hypertension. Hypertension 2006, 48, 787–796. [Google Scholar] [CrossRef] [Green Version]
- Tentolouris, N.; Liatis, S.; Katsilambros, N. Sympathetic system activity in obesity and metabolic syndrome. Ann. N. Y. Acad. Sci. 2006, 1083, 129–152. [Google Scholar] [CrossRef]
- Lemche, E.; Chaban, O.S.; Lemche, A.V. Neuroendorine and Epigentic Mechanisms Subserving Autonomic Imbalance and HPA Dysfunction in the Metabolic Syndrome. Front. Neurosci. 2016, 10, 142. [Google Scholar] [CrossRef]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef]
- Sessa, F.; Anna, V.; Messina, G.; Cibelli, G.; Monda, V.; Marsala, G.; Ruberto, M.; Biondi, A.; Cascio, O.; Bertozzi, G. Heart rate variability as predictive factor for sudden cardiac death. Aging (Albany NY) 2018, 10, 166. [Google Scholar] [CrossRef] [PubMed]
- Hayano, J.; Yuda, E.; Furukawa, Y.; Yoshida, Y. Association of 24-hour heart rate variability and daytime physical activity: ALLSTAR big data analysis. Int. J. Biosci. Biochem. Bioinform. 2018, 8, 61–67. [Google Scholar] [CrossRef]
- Tegegne, B.S.; Man, T.; van Roon, A.M.; Riese, H.; Snieder, H. Determinants of Heart Rate Variability in the General Population: The Lifelines Cohort Study Determinants of Heart Rate Variability. Heart Rhythm 2018, 15, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Guzzetti, S.; Piccaluga, E.; Casati, R.; Cerutti, S.; Lombardi, F.; Pagani, M.; Malliani, A. Sympathetic predominance in essential hypertension: A study employing spectral analysis of heart rate variability. J. Hypertens. 1988, 6, 711–717. [Google Scholar] [CrossRef]
- Dalal, J.; Dasbiswas, A.; Sathyamurthy, I.; Maddury, S.R.; Kerkar, P.; Bansal, S.; Thomas, J.; Mandal, S.C.; Mookerjee, S.; Natarajan, S. Heart Rate in Hypertension: Review and Expert Opinion. Int. J. Hypertens. 2019, 2019. [Google Scholar] [CrossRef]
- Giles, D.A.; Draper, N. Heart Rate Variability During Exercise: A Comparison of Artefact Correction Methods. J. Strength Cond. Res. 2018, 32, 726–735. [Google Scholar] [CrossRef]
- Assoumou, H.G.N.; Pichot, V.; Barthelemy, J.C.; Dauphinot, V.; Celle, S.; Gosse, P.; Kossovsky, M.; Gaspoz, J.M.; Roche, F. Metabolic Syndrome and Short-Term and Long-Term Heart Rate Variability in Elderly Free of Clinical Cardiovascular Disease: The PROOF Study. Rejuvenation Res. 2010, 13, 653–663. [Google Scholar] [CrossRef]
- Stuckey, M.I.; Tulppo, M.P.; Kiviniemi, A.M.; Petrella, R.J. Heart rate variability and the metabolic syndrome: A systematic review of the literature. Diabetes Metab. Res. Rev. 2014, 30, 784–793. [Google Scholar] [CrossRef]
- Aoyagi, N.; Ohashi, K.; Tomono, S.; Yamamoto, Y. Temporal contribution of body movement to very long-term heart rate variability in humans. Am. J. Physiol.-Heart Circ. Physiol. 2000, 278, H1035–H1041. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef]
- Burden, R.; Faires, J.; Burden, A. Numerical Analysis; Cengage Learning: Boston, MA, USA, 2014. [Google Scholar]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Ljung, L. System Identification Theory for the User; Prentice Hall: Sao Paulo, Brazil, 1999. [Google Scholar]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef] [PubMed]
- Eyre, E.L.J.; Duncan, M.J.; Birch, S.L.; Fisher, J.P. The influence of age and weight status on cardiac autonomic control in healthy children: A review. Auton. Neurosci. 2014, 186, 8–21. [Google Scholar] [CrossRef] [PubMed]
- Koskinen, T.; Kähönen, M.; Jula, A.; Mattsson, N.; Laitinen, T.; Keltikangas-Järvinen, L.; Viikari, J.; Välimäki, I.; Rönnemaa, T.; Raitakari, O.T. Metabolic syndrome and short-term heart rate variability in young adults. Diabet. Med. 2009, 26, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Moneghetti, K.J.; Christle, J.W.; Hadley, D.; Froelicher, V.; Plews, D. Heart Rate Variability: An Old Metric with New Meaning in the Era of Using mHealth technologies for Health and Exercise Training Guidance. Part Two: Prognosis and Training. Arrhythmia Electrophysiol. Rev. 2018, 7, 247. [Google Scholar] [CrossRef] [PubMed]
- Valentini, M.; Parati, G. Variables Influencing Heart Rate. Prog. Cardiovasc. Dis. 2009, 52, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Sarmiento, S.; García-Manso, J.M.; Martín-González, J.M.; Vaamonde, D.; Calderón, J.; Da Silva-Grigoletto, M.E. Heart rate variability during high-intensity exercise. J. Syst. Sci. Complex. 2013, 26, 104–116. [Google Scholar] [CrossRef]
- Monfredi, O.; Lyashkov, A.E.; Johnsen, A.-B.; Inada, S.; Schneider, H.; Wang, R.; Nirmalan, M.; Wisloff, U.; Maltsev, V.A.; Lakatta, E.G. Biophysical characterization of the underappreciated and important relationship between heart rate variability and heart rate. Hypertension 2014, 64, 1334–1343. [Google Scholar] [CrossRef]
- De Geus, E.J.C.; Gianaros, P.J.; Brindle, R.C.; Jennings, J.R.; Berntson, G.G. Should heart rate variability be “corrected” for heart rate? Biological, quantitative, and interpretive considerations. Psychophysiology 2019, 56, e13287. [Google Scholar] [CrossRef]
- Sacha, J. Interaction between heart rate and heart rate variability. Ann. Noninvasive Electrocardiol. 2014, 19, 207–216. [Google Scholar] [CrossRef]
- Sacha, J.; Sobon, J.; Sacha, K.; Barabach, S. Heart rate impact on the reproducibility of heart rate variability analysis. Int. J. Cardiol. 2013, 168, 4257–4259. [Google Scholar] [CrossRef] [PubMed]
- Fortrat, J.-O.; Formet, C.; Frutoso, J.; Gharib, C. Even slight movements disturb analysis of cardiovascular dynamics. Am. J. Physiol. -Heart Circ. Physiol. 1999, 277, H261–H267. [Google Scholar] [CrossRef] [PubMed]
- Zulfiqar, U.; Jurivich, D.A.; Gao, W.; Singer, D.H. Relation of high heart rate variability to healthy longevity. Am. J. Cardiol. 2010, 105, 1181–1185. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Control Group (37) | MetS Group (69) | ||
|---|---|---|---|---|
| Male | 16 (43.2%) | 38 (55.1%) | ||
| Female | 21 (56.8%) | 31 (44.9%) | ||
| Age (years) | 51.7 ± 1.38 | 52.9 ± 1.14 ** | ||
| Weight (kg) | 74.9 ± 11.3 | 89.5 ± 13.9 ** | ||
| WC (cm) | 86.1 ± 8.87 | 102.5 ± 10.08 ** | ||
| Abdominal obesity (%) | 5.4 | 87.0 ** | ||
| Overweight (%) | 10.8 | 97.1 ** | ||
| BMI (kg/m2) (%): | ||||
| Normal (18.5–24.9) | 55.6 | 2.9 ** | ||
| Overweight (25.0–29.9) | 41.7 | 43.5 * | ||
| Obesity (30.0–40.0) | 2.8 | 53.6 ** | ||
| SBP (24 h) | 118.5 ± 8.8 | 127.9 ± 10.7 ** | ||
| DBP (24 h) | 73.7 ± 6.7 | 78.9 ± 8.1 ** | ||
| SBP (diurnal/nocturnal) | 124.1 ± 8.9 | 106.5 ± 10.1 | 134.1 ± 11.2 ** | 114.8 ± 11.6 ** |
| DBP (diurnal/nocturnal) | 77.9 ± 8.2 | 63.8 ± 7.2 | 83.8 ± 8.9 ** | 69.1 ± 8.7 ** |
| Glucose concentration (mmol/L) (increase, %) | 4.82 ± 0.57 (0.0%) | 5.72 ± 0.80 (55.1%) ** | ||
| Dyslipidemia: | ||||
| TC (mmol/L) | 5.61 ± 1.2 | 6.39 ± 1.3 * | ||
| LDL-C (mmol/L) | 3.62 ± 0.99 | 4.2 ± 1.2 * | ||
| TG (mmol/L) | 1.0 ± 0.39 | 2.17 ± 1.1 ** | ||
| HDL-C (mmol/L) | 1.69 ± 0.46 | 1.4 ± 0.5 * | ||
| Dyslipidemia (%) | 64.9 | 98.6 ** | ||
| Diabetes (%) | 0.0 | 14.5 | ||
| Metabolic Syndrome (%) | 0.0 | 100 | ||
| HRV Variables | Diurnal | Nocturnal | ||
|---|---|---|---|---|
| Control | MetS | Control | MetS | |
| RRI (ms) | 734.0 ± 82.7 | 762.3 ± 99.6 | 951.1 ± 100.0 ### | 953.0 ± 112.4 ### |
| Time-domain variables | ||||
| SDNN (ms) | 107.7 ± 26.6 | 105.5 ± 27.7 | 93.0 ± 31.1 # | 90.0 ± 26.4 # |
| SDNN index (ms) | 53.8 ± 14.1 | 47.8 ± 13.0 * | 56.7 ± 16.0 | 54.3 ± 16.7 # |
| SDANN (ms) | 91.3 ± 26.9 | 92.5 ± 26.8 | 63.2 ± 20.0 ### | 64.4 ± 20.9 ### |
| SD1 (ms) | 14.2 ± 5.4 | 12.9 ± 4.9 | 19.9 ± 8.4 ### | 19.7 ± 8.3 ### |
| SD2 (ms) | 151.6 ± 37.5 | 147.9 ± 37.0 | 128.8 ± 40.7 # | 125.1 ± 35.9 ## |
| RMSSD (ms) | 20.0 ± 7.5 | 18.3 ± 6.9 | 27.9 ± 10.7 ### | 27.8 ± 11.8 ### |
| pNN50 (%) | 3.8 ± 3.5 | 3.2 ± 3.8 | 8.9 ± 8.6 ### | 9.4 ± 9.5 ### |
| Frequency-domain variables | ||||
| VLF (ln ms2) | 7.47 ± 0.55 | 7.27 ± 0.53 | 7.69 ± 0.59 | 7.52 ± 0.58 # |
| LF (ln ms2) | 5.86 ± 0.61 | 5.51 ± 0.59 ** | 5.89 ± 0.58 | 5.63 ± 0.63 * |
| HF (ln ms2) | 4.66 ± 0.77 | 4.50 ± 0.81 | 5.24 ± 0.87 ## | 5.13 ± 0.92 ## |
| LF/HF | 3.62 ± 1.35 | 3.04 ± 1.37 * | 2.15 ± 1.03 ### | 1.95 ± 1.16 ### |
| Variables | Control (37) | MetS (69) | Control (37) | Mets (69) |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Delta Mean | Delta Mean | |
| RRI (ms) | 785.96 ± 93.03 | 819.61 ± 104.42 | −62.3 ### | −75.6 ### |
| Time-domain variables | ||||
| SDNN (ms) | 91.30 ± 27.67 | 96.38 ± 33.85 | 6.2 | 7.2 |
| SDNN index (ms) | 59.86 ± 14.89 | 50.31 ± 16.21 * | −8.39 # | −9.24 # |
| SDANN (ms) | 65.44 ± 29.53 | 77.67 ± 36.93 | 13.20 | 13.30 |
| SD1 (ms) | 18.47 ± 5.32 | 15.34 ± 5.24 ** | −4.32 ### | −3.02 ### |
| SD2 (ms) | 127.65 ± 39.25 | 135.37 ± 47.78 | 9.46 | 10.54 |
| RMSSD (ms) | 26.11 ± 7.52 | 21.70 ± 7.41 ** | −6.11 ### | −4.26 ### |
| pNN50 (%) | 7.81 ± 5.93 | 4.72 ± 4.92 ** | −3.87 ### | −1.82 ### |
| Frequency-domain variables | ||||
| VLF (ln ms2) | 7.43 ± 0.59 | 7.12 ± 1.25 | −0.104 | −0.102 |
| LF (ln ms2) | 5.65 ± 0.63 | 5.07 ± 1.46 ** | 0.180 | 0.245 |
| HF (ln ms2) | 3.18 ± 0.81 | 2.83 ± 1.61 | 1.483 | 1.494 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Slušnienė, A.; Laucevičius, A.; Navickas, P.; Ryliškytė, L.; Stankus, V.; Stankus, A.; Navickas, R.; Laucevičienė, I.; Kasiulevičius, V. Daily Heart Rate Variability Indices in Subjects with and Without Metabolic Syndrome Before and After the Elimination of the Influence of Day-time Physical Activity. Medicina 2019, 55, 700. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100700
Slušnienė A, Laucevičius A, Navickas P, Ryliškytė L, Stankus V, Stankus A, Navickas R, Laucevičienė I, Kasiulevičius V. Daily Heart Rate Variability Indices in Subjects with and Without Metabolic Syndrome Before and After the Elimination of the Influence of Day-time Physical Activity. Medicina. 2019; 55(10):700. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100700
Chicago/Turabian StyleSlušnienė, Anžela, Aleksandras Laucevičius, Petras Navickas, Ligita Ryliškytė, Vytautas Stankus, Albinas Stankus, Rokas Navickas, Ieva Laucevičienė, and Vytautas Kasiulevičius. 2019. "Daily Heart Rate Variability Indices in Subjects with and Without Metabolic Syndrome Before and After the Elimination of the Influence of Day-time Physical Activity" Medicina 55, no. 10: 700. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina55100700