1. Introduction
Fetal growth restriction (FGR) is a common complication of pregnancy that is associated with various adverse perinatal outcomes [
1]. However, there is currently no proven fetal therapy to reverse or ameliorate overt FGR. To prevent FGR, nutritional and dietary supplementation, bed rest, and aspirin therapy have been investigated, but the efficacy of these treatments is not supported by sufficient evidence [
2].
Therefore, development of a novel therapy for FGR has been a focus in many countries. Tadalafil, a phosphodiesterase 5 (PDE5) inhibitor, was reported to be one of these novel therapies for FGR [
3,
4,
5,
6,
7]. Although several other PDE5 inhibitors are available, such as sildenafil, tadalafil has a longer half-life than sildenafil (14–15 h vs. 2–4 h) and is consequently presumed to be more stable and effective [
8]. Another benefit of the longer half-life of tadalafil is that one dose per day is sufficient, whereas sildenafil must be administered at least twice per day. Although PDE5 enzymes are widely distributed in blood vessels, tadalafil is particularly selective for PDE5 enzymes found in the reproductive organs [
9]. In fact, the TADAFER II study revealed that tadalafil administration prolonged gestation, in contrast to the STRIDER study [
10]. Sildenafil, as a PDE5 inhibitor, did not prolong gestation in FGR in the STRIDER study [
11,
12]. The differences between the STRIDER study and the TADAFER study are shown in
Table 1.
For the effective use of tadalafil for FGR, the aim of this study was to identify the relationship between the serum concentration of tadalafil and uterine artery blood flow in pregnant women and determine the ideal dosage to promote uterine artery blood flow.
2. Materials and Methods
2.1. Subjects
We recruited all pregnant women who were receiving tadalafil treatment for FGR from April 2016 to November 2018. All women who gotten informed consent were registered in this study. It was conducted at a single institution in Japan. The dose of tadalafil was 20 mg per day in all cases (oral administration). The dose of tadalafil was determined by our phase I study for FGR [
5]. FGR was defined as 1.5 standard deviations below the mean estimated fetal body weight according to gestation as calculated from ultrasonography. We received informed consent from all study subjects according to the Declaration of Helsinki. This trial was approved by the Mie University Faculty of Medicine Ethics Committee (approval number 3121, approval date 10 April 2017).
2.2. Maternal Background, Adverse Events Due to Tadalafil, and Serum Tadalafil Concentration
The clinical parameters of each patient, including age, height, weight, systolic blood pressure before tadalafil administration, systolic blood pressure after tadalafil administration, past history, gestational age at tadalafil administration and adverse events due to tadalafil, were considered in the analysis.
The blood concentration of tadalafil in each patient was measured 1, 2, 4, 6, 8, and 24 h after tadalafil administration. Uterine artery blood flow was measured before tadalafil administration and 2–4 h and 20–24 h after tadalafil administration. We then analyzed the correlation between the blood concentration of tadalafil and uterine artery blood flow.
2.3. Determination of Serum Tadalafil Concentration
The concentration of serum tadalafil was determined by high-performance liquid chromatography (HPLC) according to a previously described method with slight modifications [
13]. Briefly, a 100-L serum sample was alkalized with 400 L of 0.1 M glycine buffer (saturated with NaCl, pH 10.6) and eluted with 1 mL 1-chlorobutane and dichloromethane (4:1, v/v) for 1 h. The organic phase (800 L) was evaporated to dryness, and the residue was dissolved in 50% acetonitrile and subjected to HPLC. The unbound fractions of tadalafil in serum were determined by ultrafiltration using Amicon
® Ultra-0.5 mL centrifugal filters (Millipore, Billerica, MA, USA) at 14,000×
g for 10 min.
HPLC analyses were performed using an HPLC system (LC-20AD, Shimadzu, Kyoto, Japan) connected to a TSKgel® ODS-80Tm 5-m column (150 × 4.6 mm i.d.; Tosho, Tokyo, Japan) and a fluorescence detector (RF-20Axs, Shimadzu). The column temperature was set at 40 °C. The elution of tadalafil was conducted using 0.1% trifluoroacetic acid and acetonitrile (60:40, v/v) at 1 mL/min. The fluorescence detector was operated at excitation and emission wavelengths of 275 nm and 335 nm, respectively. The mean intra- and inter-day precision and accuracy of this assay were estimated by analyzing five replicates at serum tadalafil concentrations of 25, 50, 500, and 750 ng/mL and were determined to be 5.5% and −3.1%, respectively. The limit of detection of tadalafil was 3 ng/mL.
2.4. Measurement of Uterine Artery Blood Flow
Before measurements were performed, the pregnant women rested for more than 20 min in the semi-recumbent position. It was confirmed that there were no abnormalities in the measured uterine artery waveform. The appropriate waveform was defined by the absence of the following: an increased systolic/diastolic (A/B) ratio (>2.6) with or without a notch on the uterine artery blood flow velocity waveform or a normal A/B ratio (<2.6) with either a unilateral notch or a bilateral notch on the uterine artery blood flow velocity waveform. The method of visualization of the uterine artery conformed to that of Bower [
14]: by placing the transducer in the lower lateral quadrant of the uterus and angling it medially, we identified crossover of the external iliac artery and placed the range gate over the entire diameter of the uterine artery 1 cm distal to that site. The Doppler waveform was measured during three to six heartbeat cycles, and the median of three measurements was used as the measured value. Using a computer, the left and right uterine arterial blood flow rates were measured based on the blood flow velocity, mean time-averaged flow velocity (TAV), and inner diameter of the uterine artery. Standard changes in uterine arterial blood flow that occurred with each gestational week, as reported by Konje et al. [
15], were used to evaluate the uterine artery.
The uterine artery Doppler mode of the GE Voluson E8 Expert machine (Chicago, IL, USA) was selected for measurement of the uterine arteries, ensuring maximum standardization of settings. Pulse repetition frequency was adjusted for each examination to ensure the best fit of the waveforms. The following preset variables were used: harmonic setting: mid, power: 100%, gain: −3, C7 M5 P3 E3, SRI II: 2, frequency: low, quality: normal, pulse Doppler wall motion filter: 60 Hz, and sample size: 2 mm. The angle correction was measured within 60 degrees.
2.5. Statistical Analysis
Statistical analyses were performed using univariate chi-squared and Mann–Whitney U-tests. p values of <0.05 were considered statistically significant. All analyses were performed using the statistical software package, SAS (version 9.4).
3. Results
We recruited a total of five pregnant women. The age, height, weight, and systolic blood pressure are shown in
Table 2. All women had normal renal function (the range of serum creatinine was 0.32–0.45) and none had preeclampsia at registration.
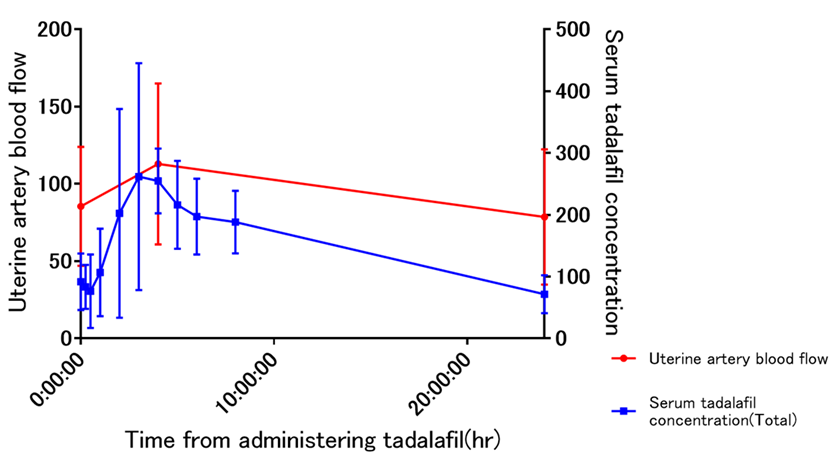
The blood concentration of tadalafil correlated with uterine artery blood flow, and the blood concentration of tadalafil and uterine artery blood flow decreased from 5 h after administration of tadalafil (
Figure 1).
The cumulative frequency of adverse events from tadalafil administration was four women with headache (Grade 1; three women, Grade 2; one woman), and face flush in one woman (Grade 1). There were no severe fetal and neonatal adverse events that seemed to be related to tadalafil. Adverse events were expressed by grade based on the Common Terminology Criteria for Adverse Events v4.0, as with the TADAFER II study [
11].
4. Discussion
This study investigated the blood concentration and efficacy (uterine artery blood flow) of tadalafil on a single day, with the aim of evaluating the suitability of the current once-daily doses. Once-daily administration poses challenges in maintaining blood drug levels, and efficacy (evaluated in terms of uterine artery blood flow) was not sufficiently maintained. These results suggest that methods for administering tadalafil need to be investigated further.
Previous studies indicated that tadalafil may be effective for treating FGR. Nonetheless, better and more effective administration methods must be considered. Animal experiments that involved continuous administration of tadalafil mixed with water resulted in stable blood drug concentration and efficacy. Regarding human administration, the package insert stipulates a once-daily dosage given the half-life of tadalafil. However, the question of whether this method actually yields a stable tadalafil blood concentration and efficacy remains to be confirmed. We selected uterine artery blood flow as an indicator of efficacy after finding that the blood concentration of tadalafil had decreased 5 hr after administration, while uterine artery blood flow had diminished within the same time frame. These findings suggest that the method for administering tadalafil in humans must be investigated further. We believe that twice-daily administration is superior for yielding a stable blood drug concentration, and we intend to investigate this in the future. As in the present study, we will also investigate efficacy parameters on the basis of uterine artery blood flow.
This study was limited by the small number of participants. In addition, we were unable to measure uterine artery blood flow 6 to 24 h after tadalafil administration. Future studies are advised to measure uterine artery blood flow in more detail.
In summary, in the current once-daily administration of tadalafil, adequate blood concentrations could not be maintained and stable efficacy was not obtained. Therefore, twice-daily or other administration frequencies must be investigated.
5. Conclusions
The blood concentration and uterine artery blood flow fluctuate in parallel, the latter was decreased by reduced blood concentration. Thus, a study of tadalafil administered twice a day in pregnant women will be needed to stabilize uterine artery blood flow.
Author Contributions
Conceptualization: H.T. and T.I.; methodology: S.M. (Shintaro Maki), S.M. (Shoichi Magawa), M.N., validation: H.T., and K.T. (Kuniaki Toriyabe); formal analysis: H.T., S.M. (Shintaro Maki) and K.T. (Kayo Tanaka); investigation: H.T. and K.I.; data curation: H.T., S.M. (Shintaro Maki) and K.I.; writing: H.T.; supervision: K.T. (Kayo Tanaka) and T.I.
Funding
This work was supported by the Japan Society for the Promotion of Science KAKENHI (Grant Number 19K18638).
Conflicts of Interest
The authors declare no conflict of interest.
References
- American College of Obstetricians and Gynecologists. ACOG Practice bulletin no. 134 fetal growth restriction. In Obstet. Gynecol.; 2013; Volume 121, pp. 1122–1133. [Google Scholar]
- Hui, L.; Challis, D. Diagnosis and management of fetal growth restriction: The role of fetal therapy. Best Pract. Res. Clin. Obstet. Gynaecol. 2008, 22, 139–158. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Tanaka, H.; Maki, S.; Kubo, M.; Nii, M.; Magawa, S.; Hatano, F.; Tsuji, M.; Osato, K.; Kamimoto, Y.; et al. Cardiac function and tadalafil used for treating fetal growth restriction in pregnant women without cardiovascular disease. J. Matern.-Fetal Neonatal Med. 2018, 20, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, K.; Umekawa, T.; Maki, S.; Kubo, M.; Nii, M.; Tanaka, K.; Tanaka, H.; Osato, K.; Kamimoto, Y.; Kondo, E.; et al. Tadalafil improves L-NG-nitroarginine methyl Ester-Induced preeclampsia with fetal growth Restriction-Like symptoms in pregnant mice. Am. J. Hypertens. 2017, 31, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Kubo, M.; Tanaka, H.; Maki, S.; Nii, M.; Murabayashi, N.; Osato, K.; Kamimoto, Y.; Umekawa, T.; Kondo, E.; Ikeda, T.; et al. Safety and dose-finding trial of tadalafil administered for fetal growth restriction: A Phase-1 clinical study. J. Obstet. Gynaecol. Res. 2017, 43, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Kubo, M.; Nii, M.; Maki, S.; Umekawa, T.; Ikeda, T. Treatment using tadalafil for severe pre-eclampsia with fetal growth restriction. J. Obstet. Gynaecol. Res. 2017, 43, 1205–1208. [Google Scholar] [CrossRef] [PubMed]
- Kubo, M.; Umekawa, T.; Maekawa, Y.; Tanaka, H.; Nii, M.; Murabayashi, N.; Osato, K.; Kamimoto, Y.; Ikeda, T. Retrospective study of tadalafil for fetal growth restriction: Impact on maternal and perinatal outcomes. J. Obstet. Gynaecol. Res. 2017, 43, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Park, S.I.; Heo, S.H.; Kim, G.; Chang, S.; Song, K.H.; Kim, M.G.; Jin, E.H.; Kim, J.; Lee, S.; Hong, J.H. Comparison of tadalafil pharmacokinetics after administration of a new orodispersible film versus a film-coated tablet. Drug Des. Dev. Ther. 2018, 12, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Wright, P.J. Comparison of phosphodiesterase type 5 (PDE5) inhibitors. Int. J. Clin. Pract. 2006, 60, 967–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umekawa, T.; Maki, S.; Kubo, M.; Tanaka, H.; Nii, M.; Tanaka, K.; Osato, K.; Kamimoto, Y.; Tamaru, S.; Ogura, T.; et al. TADAFER study group. TADAFER II: Tadalafil treatment for fetal growth restriction—A study protocol for a multicenter randomised controlled phase II trial. BMJ Open 2018, 8, e020948. [Google Scholar] [CrossRef] [PubMed]
- Maki, S.; Tanaka, H.; Tsuji, M.; Furuhashi, F.; Magawa, S.; Kaneda, M.K.; Nii, M.; Tanaka, K.; Kondo, E.; Tamaru, S.; et al. Safety Evaluation of Tadalafil Treatment for Fetuses with Early-Onset Growth Restriction (TADAFER): Results from the Phase II Trial. J. Clin. Med. 2019, 15, 856. [Google Scholar] [CrossRef] [PubMed]
- Sharp, A.; Cornforth, C.; Jackson, R.; Harrold, J.; Turner, M.A.; Kenny, L.C.; Baker, P.N.; Johnstone, E.D.; Khalil, A.; von Dadelszen, P.; et al. Maternal sildenafil for severe fetal growth restriction (STRIDER): A multicentre, randomised, placebo-controlled, Double-Blind trial. Lancet Child Adolesc. Health 2018, 2, 93–102. [Google Scholar] [CrossRef]
- Kim, Y.K.; Quadro, L. Reverse-phase High-Performance liquid chromatography (HPLC) analysis of retinol and retinyl esters in mouse serum and tissues. Methods Mol. Biol. 2010, 652, 263–275. [Google Scholar] [PubMed]
- Bower, S.; Bewley, S.; Campbell, S. Improved prediction of Pre-Eclampsia by Two-Stage screening of uterine arteries using the early diastolic notch and color Doppler imaging. Obstet. Gynecol. 1993, 82, 78–83. [Google Scholar] [PubMed]
- Konje, J.C.; Kaufmann, P.; Bell, S.C.; Taylor, D.J. A longitudinal study of quantitative uterine blood flow with the use of color power angiography in appropriate for gestational age pregnancies. Am. J. Obstet. Gynecol. 2001, 185, 608–613. [Google Scholar] [CrossRef] [PubMed]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).

 ,
, 

{kind=link}