Digital Customized Titanium Mesh for Bone Regeneration of Vertical, Horizontal and Combined Defects: A Case Series

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
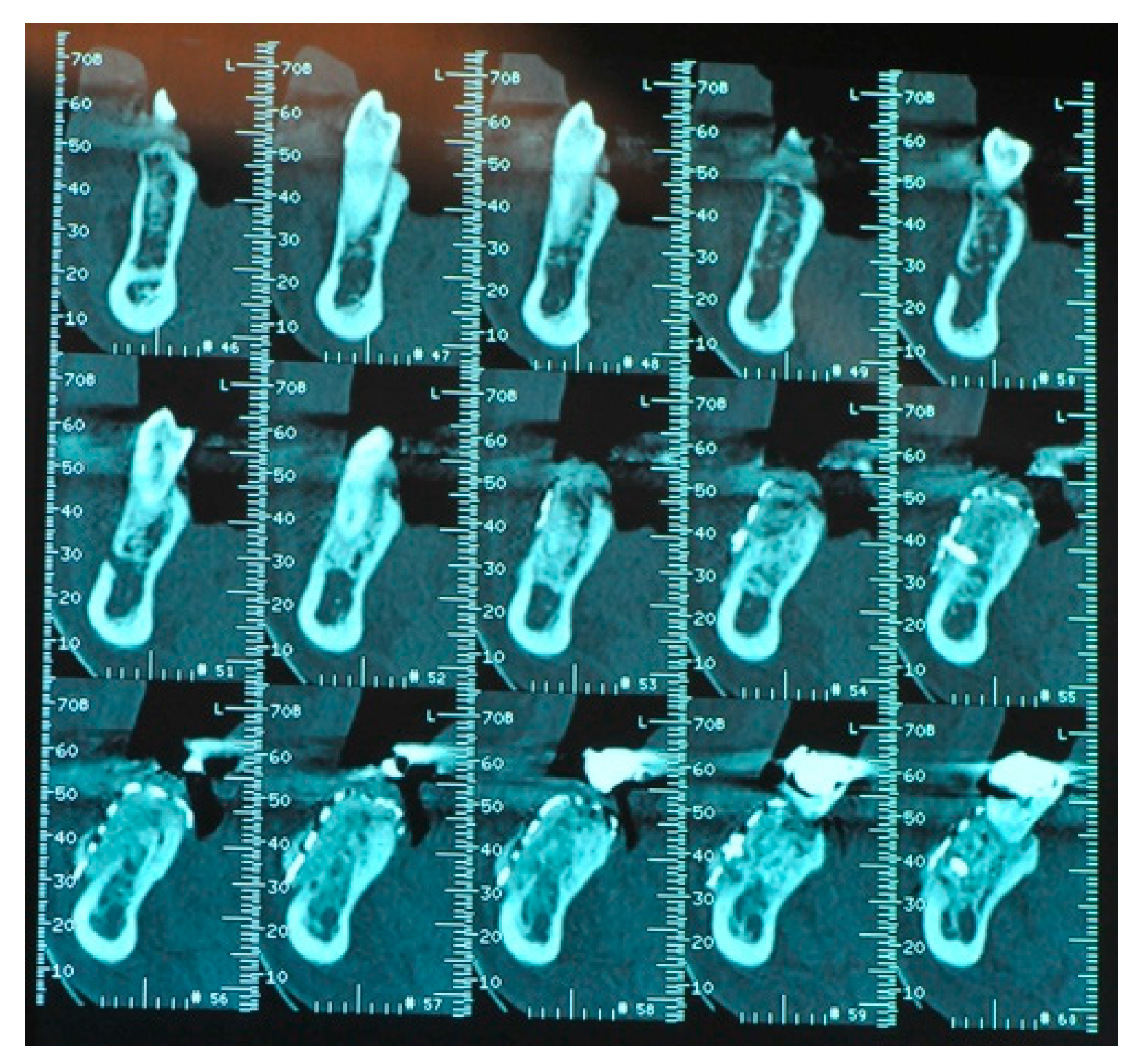
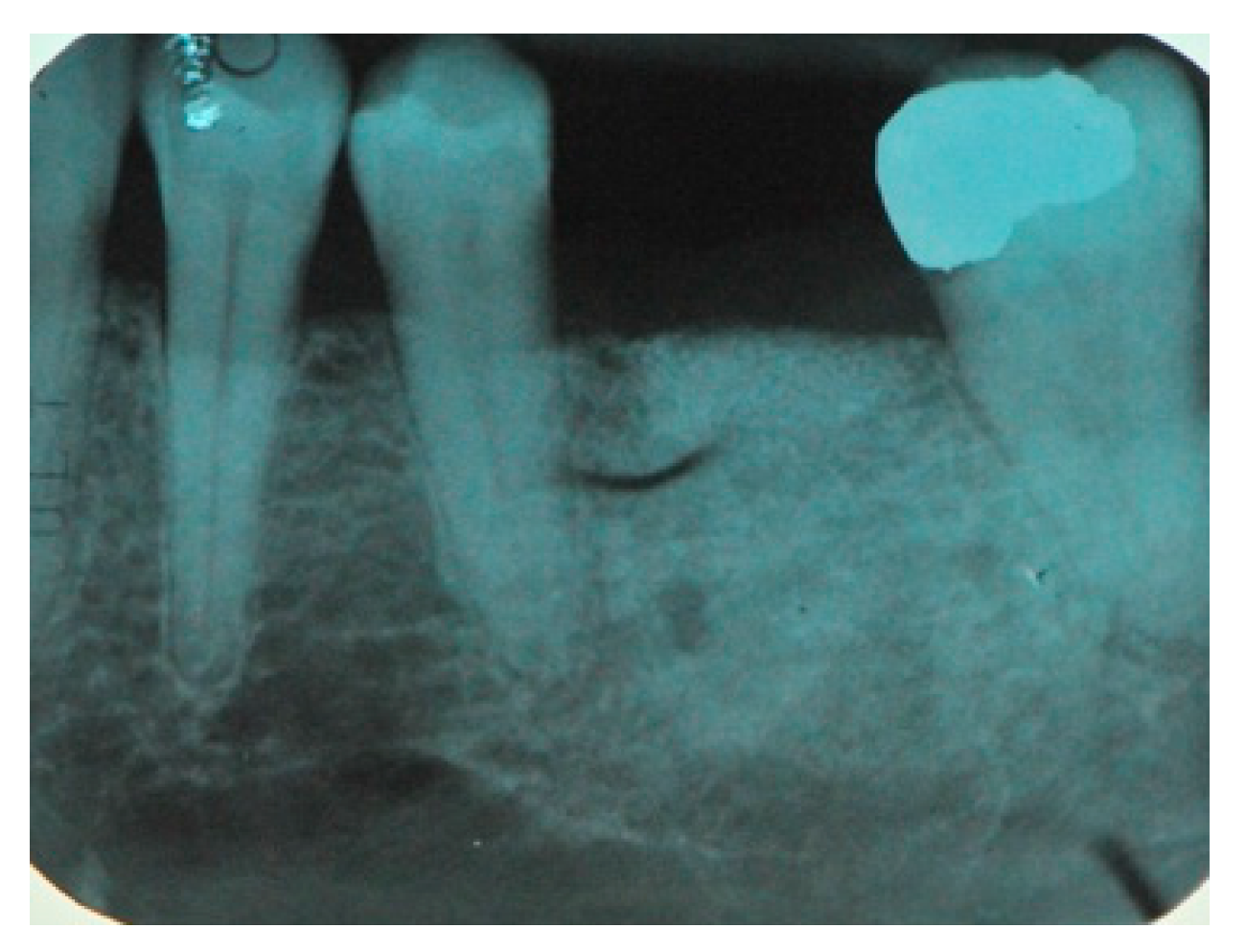
- The presence, clinically and radiographically (intraoral radiographs, panoramic, CT scans) assessed, of horizontal, vertical or mixed bone defects of the maxillary bones in particular the presence of residual bone <8 mm in height and <5 mm in width.
- The absence of any local or systemic contraindication to surgical treatment such as infections, a smoking habit of >10 cigarettes a day, uncontrolled diabetes (HBA1c ≥ 7.5%), previous radiotherapy in the head and neck anatomical areas, chemotherapy, liver, blood and kidney diseases, immunosuppression, state of pregnancy, inflammatory and autoimmune diseases of the oral cavity, poor oral hygiene and poor motivation.
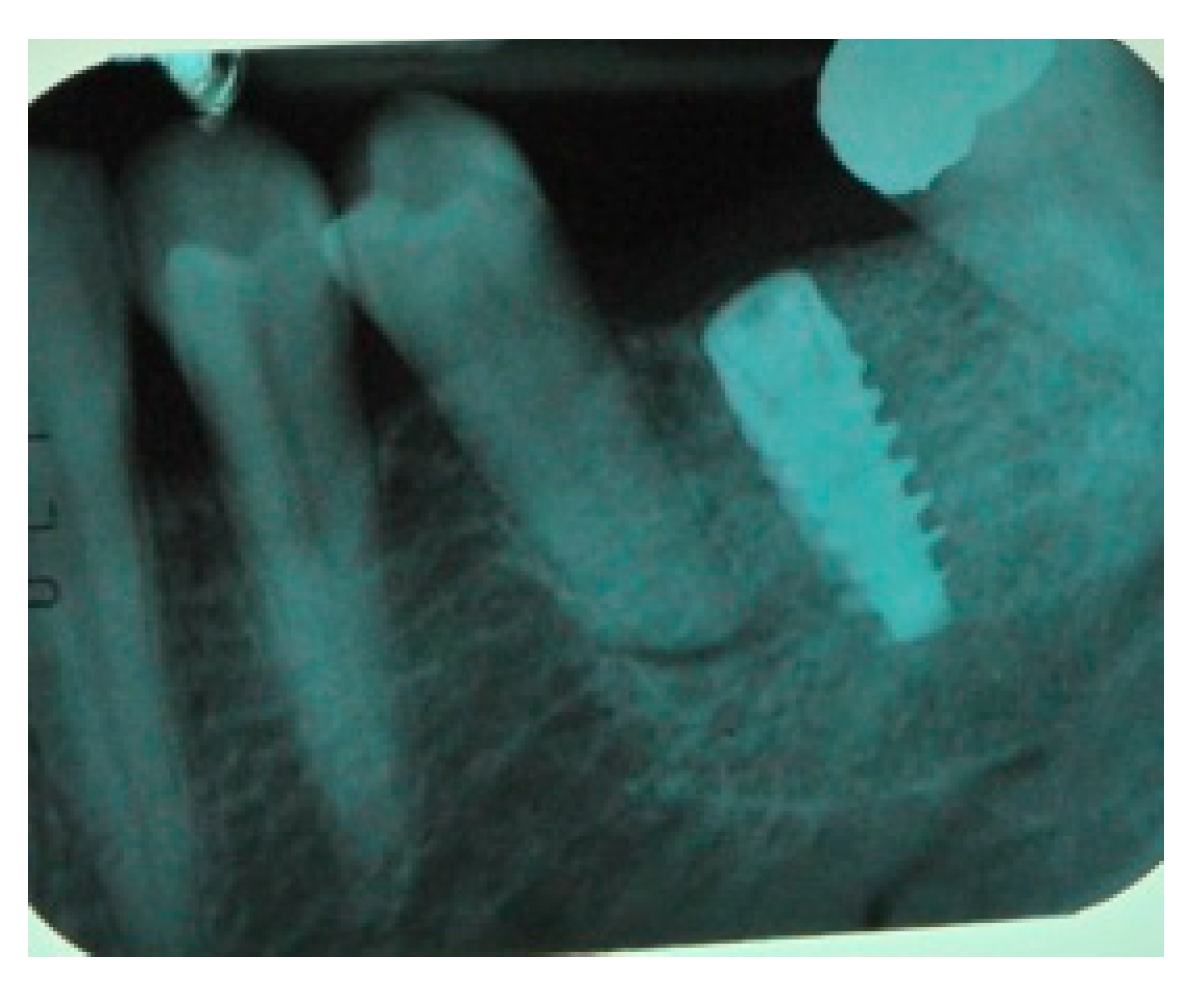
- The need for a staged treatment with the placement of dental implants eight months after bone regeneration.
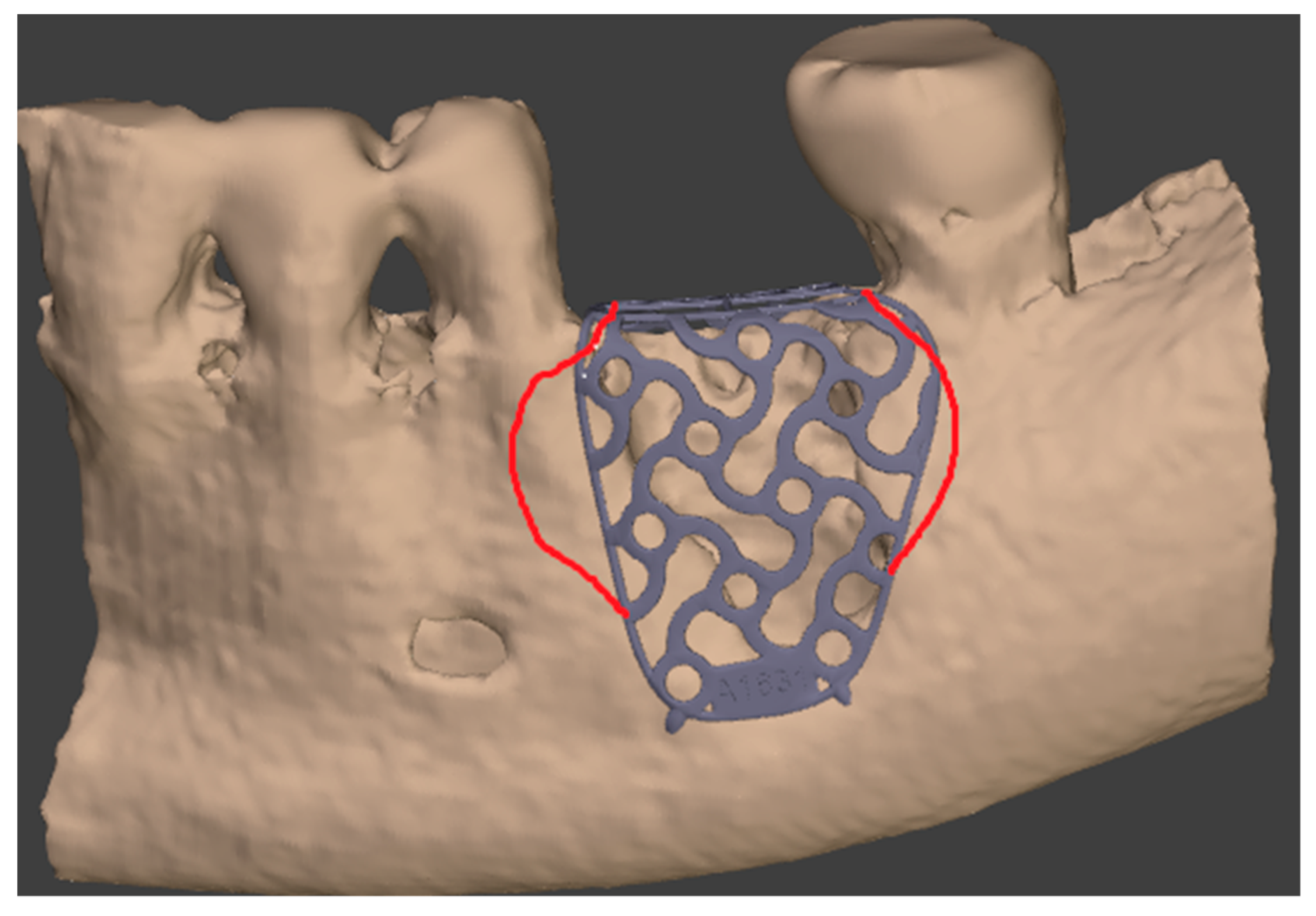
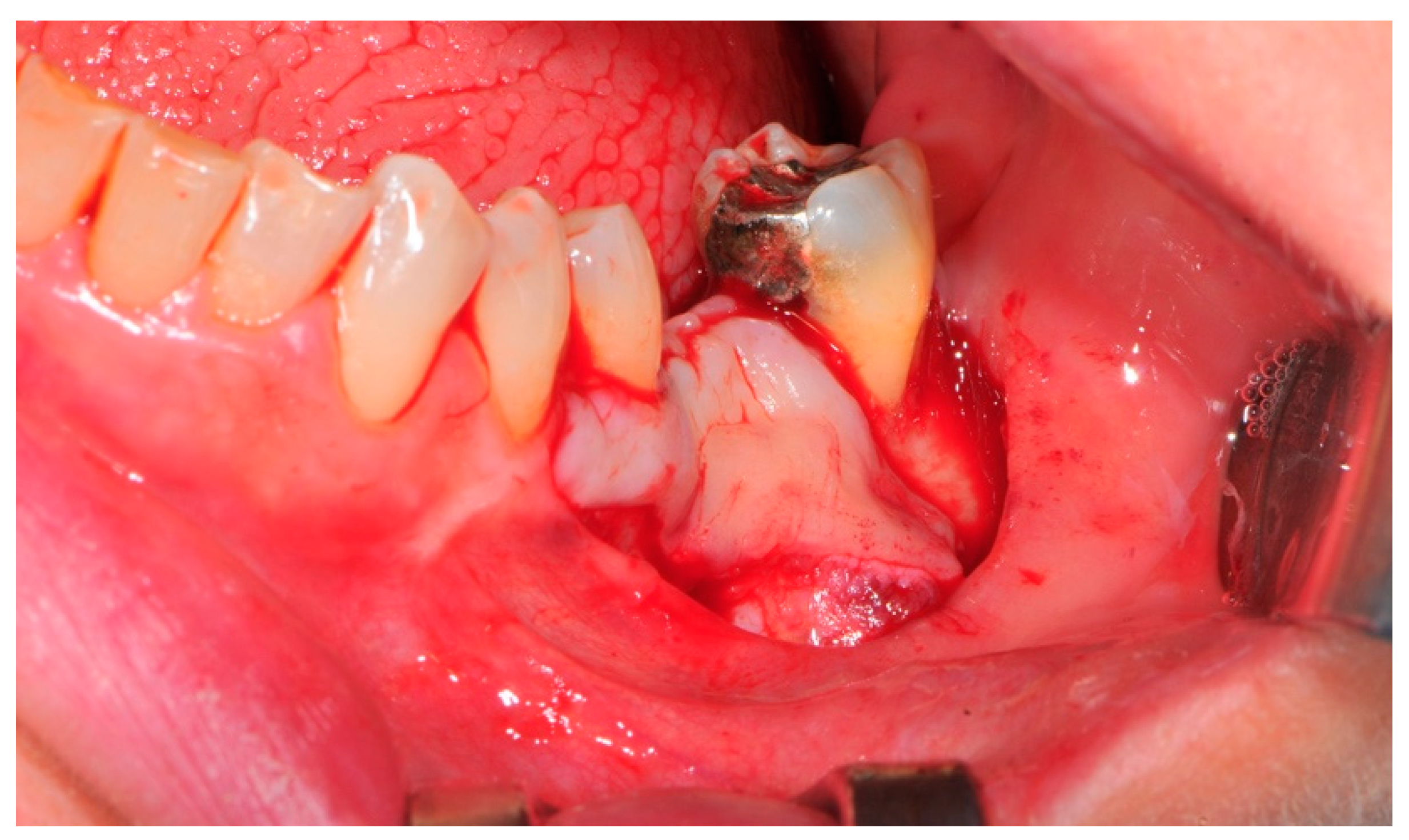
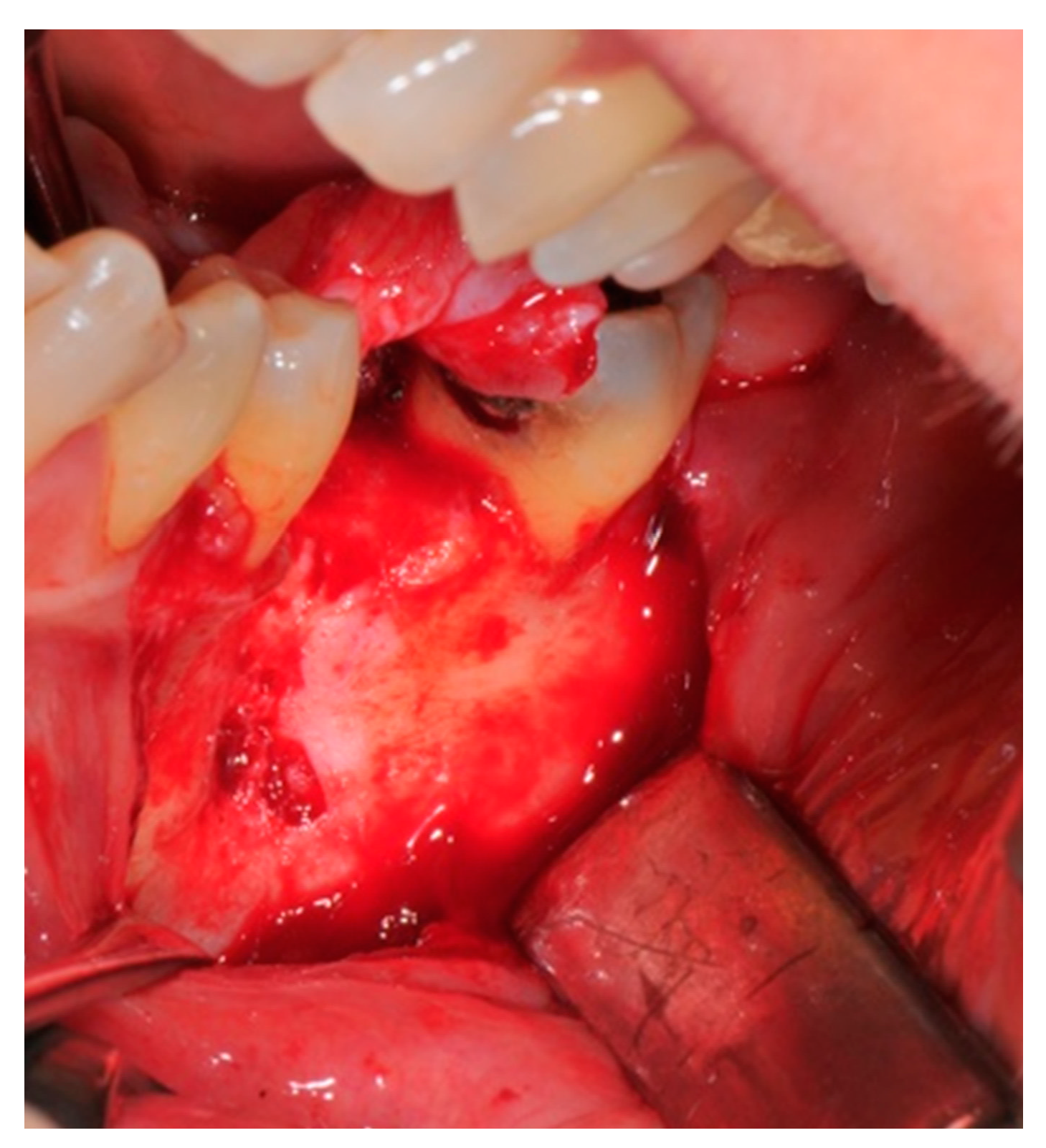
- Flap design: Soft tissue management should be as accurate as possible. The design of the flap should ensure a tension-free primary closure of the wound even after voluminous grafting of the defect. One option (preferred especially in wide vertical defects) is the execution of the so-called “poncho” flap. This technique includes a high vestibular incision of the mucosa, muscle and periosteum in order to undermine the preparation of the flap and to achieve its mobilization, followed by a deep incision in the buccal area with two additional vertical incisions that are performed at an appropriate distance from the occlusal area and the site of augmentation. After the incision, the preparation of a muco-periosteal flap and the remotion of scar tissue, a full thickness flap is raised until the bone defect is uncovered [17,18,19,20]. Finally, the positioning of the customized titanium mesh is passively tested to evaluate its fit intra-operatively (Figure 2, Figure 3, Figure 4 and Figure 5).
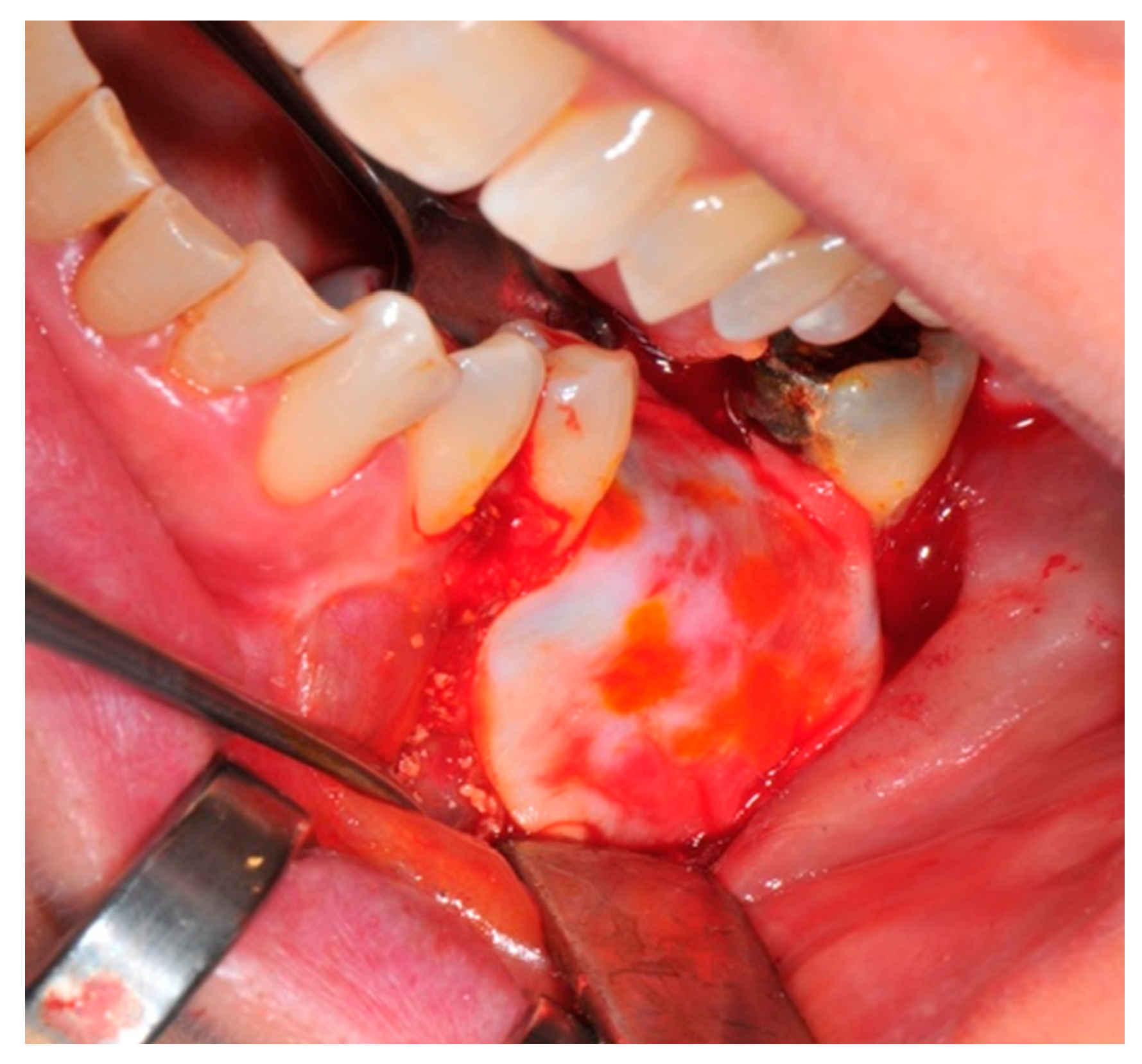
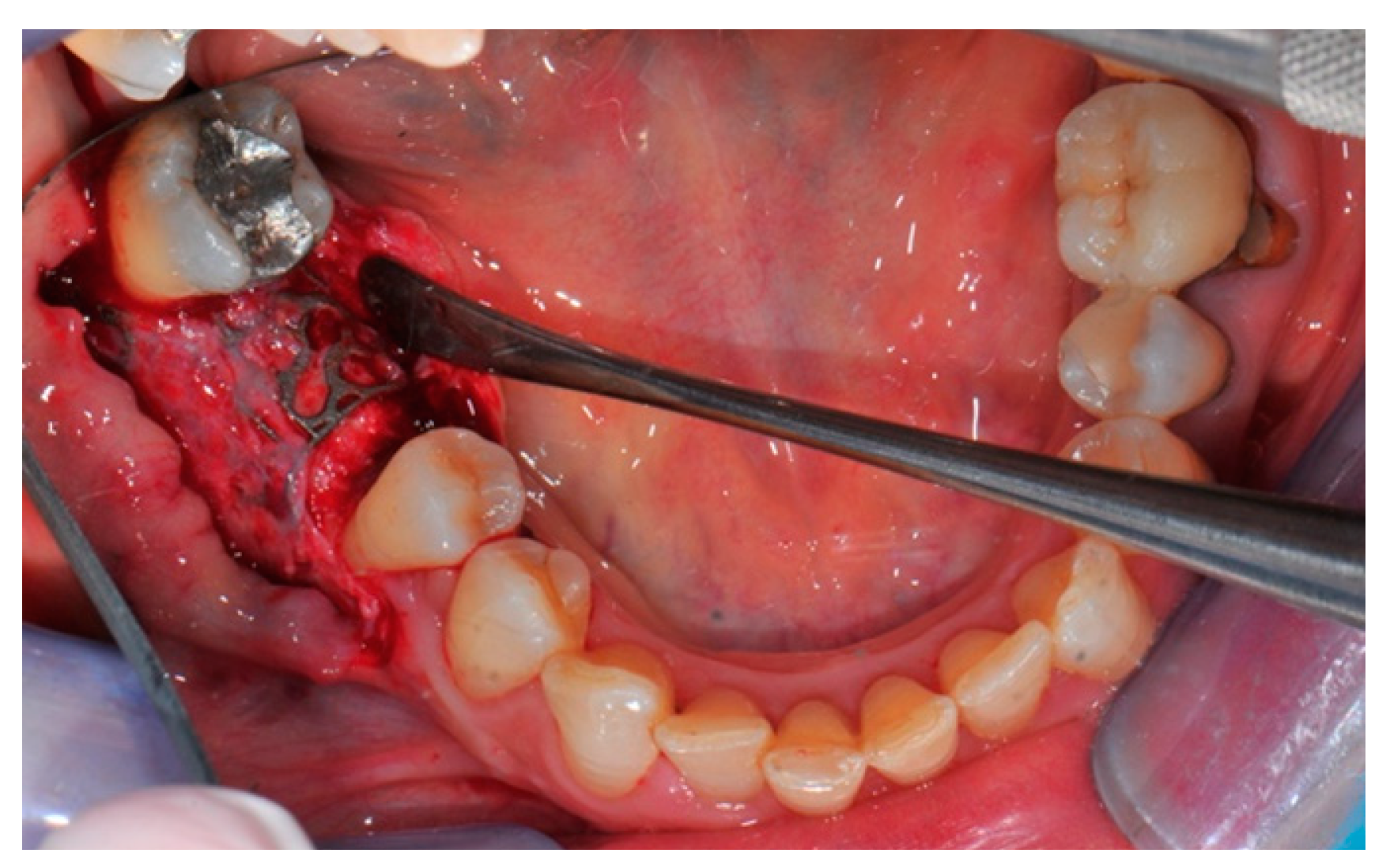
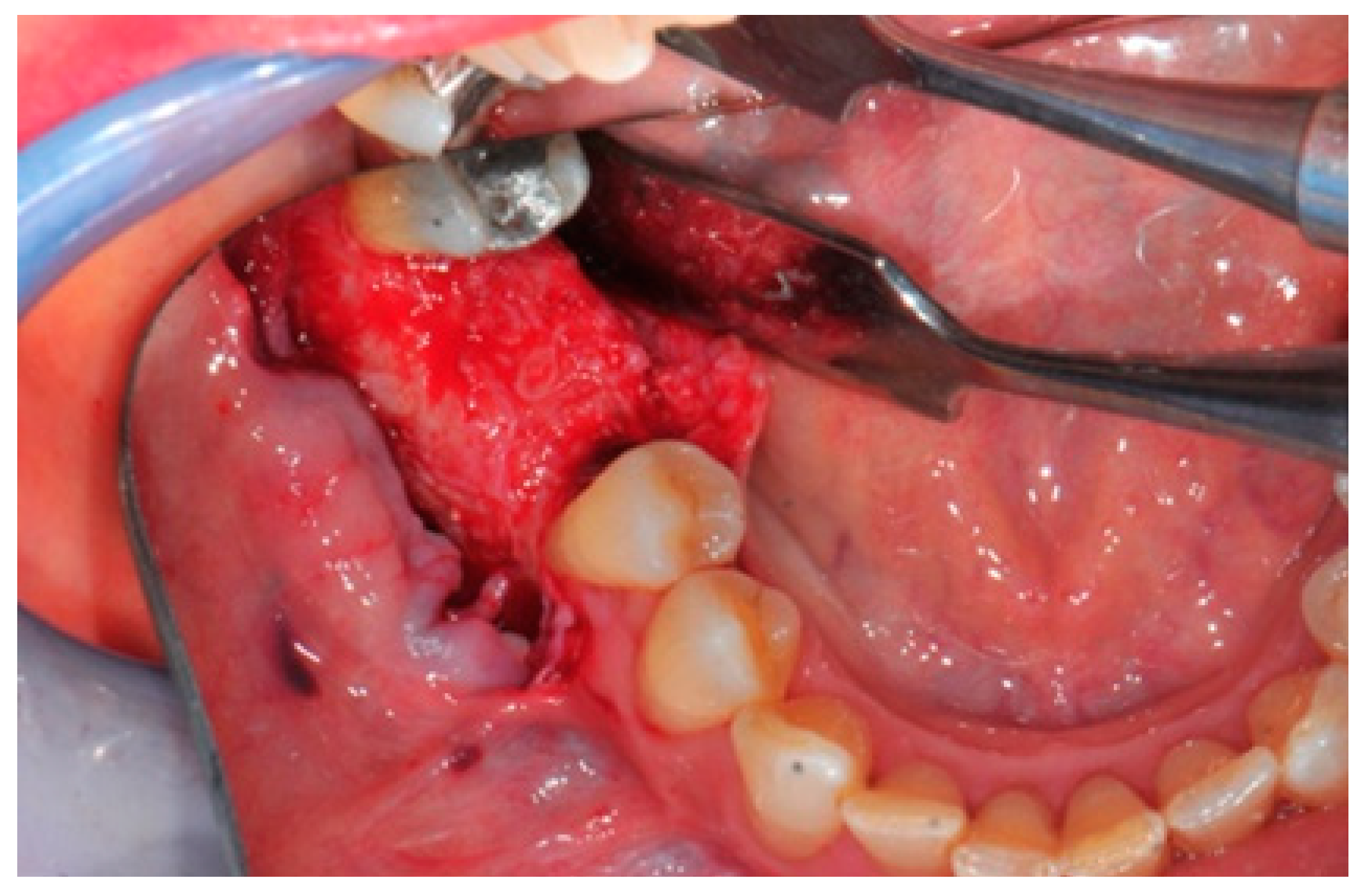
- Preparation of the receiving site: The exposed bone is cleaned from all of the remaining soft tissue and it is then prepared with multiple perforations using a small ball bur; this procedure is known as “bone refreshing” and it is performed to expose the cancellous portion of the residual bone, which shows a great osteo-genetic potential (Figure 6).
- Particulate bone: At this stage, a 50:50 autologous/heterologous bone mix is grafted both in the atrophic site and within the titanium mesh (Figure 7).
- Positioning of the customized titanium mesh: Being patient-customized or responding to the specific requirements of the patient in terms of planned bone augmentation, this mesh does not require any modification and it should perfectly fit the patient’s residual bone (Figure 8).
- Fixation and coverage: Fixation is a crucial aspect of the procedure as the stability of the graft must be maintained in order to ensure bone regeneration. The grid is fixed on the residual bone with titanium screws. Subsequently, the titanium mesh is covered with a resorbable membrane (Figure 9 and Figure 10).
- Passivation of the flap: Delicate periosteal incisions are performed to achieve mobility of the flap and allowing first intention closure, creating a passive/tension-free flap in order to avoid detrimental tension or graft exposure (Figure 11).
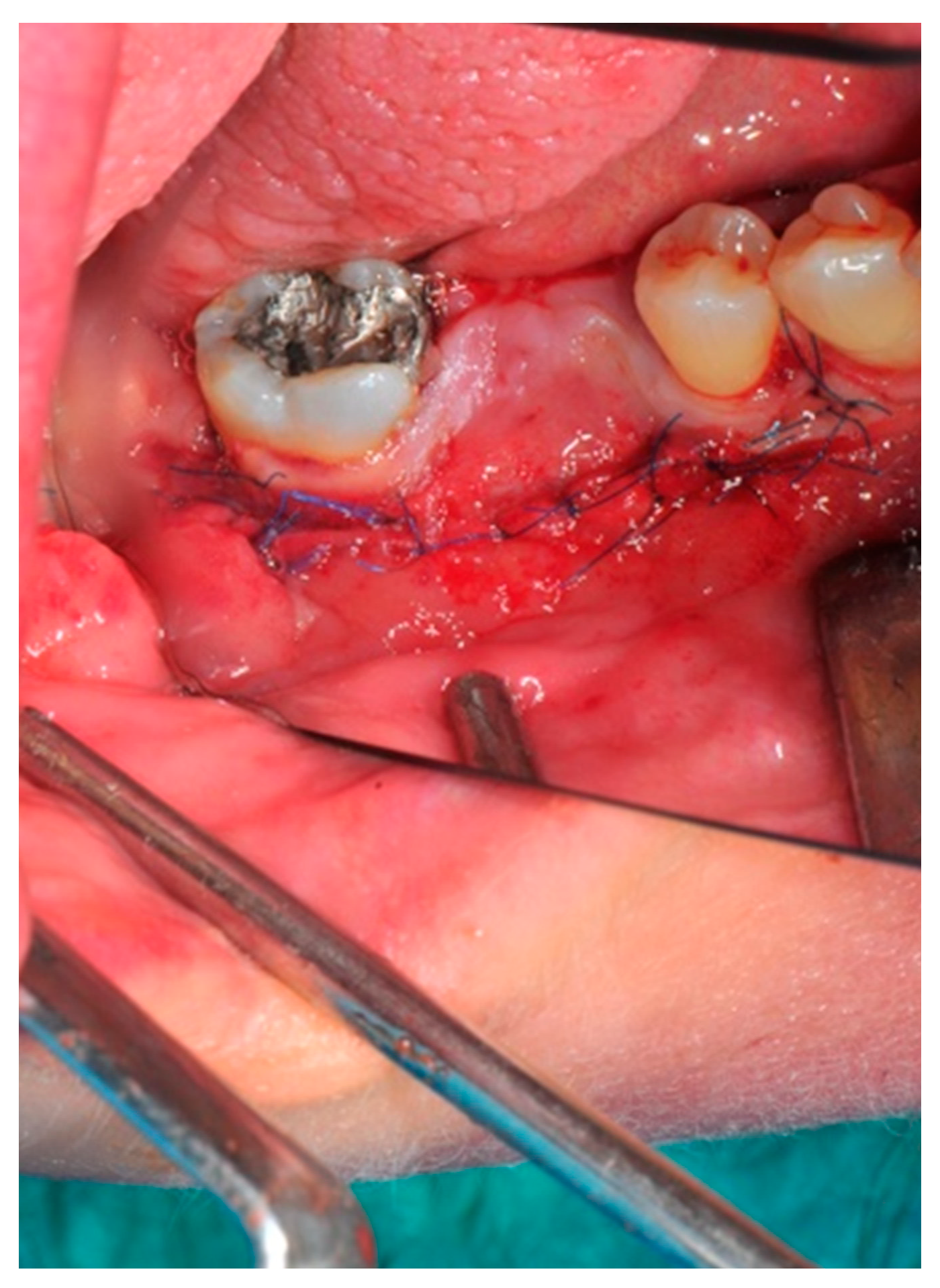
- Suture: Perfect closure is achieved with a first line of horizontal mattress sutures positioned 5 mm from the incision line and, subsequently, with single interrupted stitches connecting the edges of the flap. With this technique, the edges of the flap are reversed, putting the inner layers of the connective tissue in close contact with each other. The intimate connection between the layers of connective tissue forms a barrier that largely prevents the exposure of the membrane (Figure 12 and Figure 13).
Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Nocini, P.F.; Chiarini, L.; De Santis, D. Pre-Prosthetic Surgery and Tissue Engineering Treatment; Martina: Minneapolis, MN, USA, 2005; p. 1. [Google Scholar]
- Chiapasco, M.; Casentini, P.; Zaniboni, M. Bone augmentation procedures in implant dentistry. Int. J. Oral Maxillofac. Implant. 2009, 24, 237–259. [Google Scholar]
- Rakhmatia, Y.D.; Ayukawa, Y.; Furuhashi, A.; Koyano, K. Current barrier membranes: Titanium mesh and other membranes for guided bone regeneration in dental applications. J. Prosthodont. Res. 2013, 57, 3–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buser, D.; Dula, K.; Hess, D.; Hirt, H.P.; Belser, U.C. Localized ridge augmentation with autografts and barrier membranes. Periodontol. 2000 1999, 19, 151–163. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.L.; Boyapati, L. PASS: Principles for predictable bone regeneration. Implant Dent. 2006, 15, 8–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Her, S.; Kang, T.; Fien, M.J. Titanium mesh as an alternative to a membrane for ridge augmentation. J. Oral Maxillofac. Surg. 2012, 70, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Cordaro, L.; Sarzi Amadè, D.; Cordaro, M. Clinical results of alveolar ridge augmentation with mandibular block bone grafts in partially edentulous patients prior to implant placement. Clin. Oral Implant. Res. 2002, 13, 103–111. [Google Scholar] [CrossRef]
- Kolerman, R.; Nissan, J.; Mijiritski, E.; Hamoudi, N.; Mangano, C.; Tai, H. Esthetic assessment of immediately implants combined with GBR and free connective tissue graft. Clin. Oral Implant. Res. 2016, 27, 1414–1422. [Google Scholar] [CrossRef]
- Cucchi, A.; Giavatto, M.A.; Giannatiempo, J.; Lizio, G.; Corinaldesi, G. Custom Made Titanium Mesh for Maxillary Bone Augmentation with Immediate Implants and Delayed Loading. J. Oral Implantol. 2019, 45, 59–64. [Google Scholar] [CrossRef]
- De Santis, D.; Graziani, P.; Castellani, R.; Zanotti, G.; Gelpi, F.; Marconcini, S.; Bertossi, D.; Nocini, P.F. A New Radiologic Protocol and a New Occlusal Radiographic Index for Computer-Guided Implant Surgery. J. Craniofac. Surg. 2016, 27, e506–e510. [Google Scholar] [CrossRef]
- D’Ahaese, J.; Ackhurst, J.; Wismejer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computed guided implant surgery. Periodontol. 2000 2017, 73, 121–133. [Google Scholar] [CrossRef]
- Kim, J.E.; Lee, J.; Jang, M.; Kwak, M.H.; Go, J.; Kho, E.K.; Song, S.H.; Sung, J.E.; Lee, J. Hwang DY.Accelerated healing of cutaneous wounds using photochemically stabilized gold nanoparticles deposited hydrocolloid membranes. Biomater. Sci. 2015, 3, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Ciocca, L.; Lizio, G.; Baldissara, P.; Sambuco, A.; Scotti, R.; Corinaldesi, G. Prosthetically CAD-CAM guided bone augmentation of atrophic jaws using customized titanium mesh: Preliminary results 147 of an open prospective study. J. Oral Implantol. 2019, 45, 59–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyamoto, I.; Funaki, K.; Yamauchi, K.; Kodama, T.; Takahashi, T. Alveolar ridge reconstruction with titanium mesh and autogenous particulate bone graft. Clin. Implant Dent. Relat. Res. 2012, 14, 304–313. [Google Scholar] [CrossRef] [PubMed]
- De Santis, D.; Trevisiol, L.; D’Agostino, A.; Cucchi, A.; De Gemmis, A.; Nocini, P.F. Guided bone regeneration with autogenous block grafts applied to Le Fort I osteotomy for treatment of severely resorbed maxillae: A 4- to 6-year prospective study. Clin. Oral Implant. Res. 2012, 23, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.S.; Terheyden, H. Bone augmentation procedures in localized defects in the alveolar ridge: Clinical results with different bone grafts and bone-substitute materials. Int. J. Oral Maxillofac. Implants 2009, 24, 218–236. [Google Scholar]
- Nevins, M.; Mendoza-Azpur, G.; De Angelis, N.; Kim, D.M. The Biocompatibility of Cyanoacrylate Tissue Adhesive in Conjunction with a Collagen Membrane for Providing Soft and Hard Tissue Regeneration in Extraction Socket Preservation Procedures. Int. J. Periodont. Restor. Dent. 2018, 38, s37–s42. [Google Scholar] [CrossRef] [PubMed]
- Czarnomysy, R.; Bielawska, A.; Bielawski, K. Effect of 2nd and 3rd generation PAMAM dendrimers on proliferation, differentiation, and pro-inflammatory cytokines in human keratinocytes and fibroblasts. Int. J. Nanomed. 2019, 14, 7123. [Google Scholar] [CrossRef] [Green Version]
- Sagheb, K.; Schiegnitz, E.; Moergel, M.; Walter, C.; Al-Nawas, B.; Wagner, W. Clinical outcome of alveolar ridge augmentation with individualized CAD-CAM-produced titanium mesh. Int. J. Implant Dent. 2017, 3, 36. [Google Scholar] [CrossRef] [Green Version]
- Buser, D.; Dula, K.; Hirt, H.P.; Schenk, R.K. Lateral ridge augmentation using autografts and barrier membrane: A clinical study with 40 partially edentulous patients. J. Oral Maxillofac. Surg. 1996, 54, 420–432. [Google Scholar] [CrossRef]
- Springer, I.N.; Nocini, P.F.; Schlegel, K.A.; De Santis, D.; Park, J.; Warnke, P.H.; Terheyden, H.; Zimmermann, R.; Chiarini, L.; Gardner, K.; et al. Two techniques for the preparation of cell-scaffold constructs suitable for sinus augmentation: Steps into clinical application. Tissue Eng. 2006, 12, 2649–2656. [Google Scholar] [CrossRef]
- Hoexter, D.L.; Epstein, S.B. The Poncho Flap: Repositioned perforated attached gingival flap. Oral Implantol. 1975, 5, 547–552. [Google Scholar] [PubMed]
- Puisys, A.; Vindasiute, E.; Linkevciene, L.; Linkevicius, T. The use of acellular dermal matrix membrane for vertical soft tissue augmentation during submerged implant placement: A case series. Clin. Oral Implant. Res. 2015, 26, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Papi, P.; Pompa, G. The Use of a Novel Porcine Derived Acellular Dermal Matrix (Mucoderm) in Peri-Implant Soft Tissue Augmentation: Preliminary Results of a Prospective Pilot Cohort Study. Biomed. Res. Int. 2018, 9, 6406051. [Google Scholar] [CrossRef] [PubMed]
- De Santis, D.; Cucchi, A.; De Gemmis, A.; Nocini, P.F. New collagen matrix to avoid the reduction of keratinized tissue during guided bone regeneration in postextraction sites. J. Craniofac. Surg. 2012, 23, e186–e189. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, C.; Felice, P.; Lizio, G.; Rossi, F. Le Fort I osteotomy with interpositional graft and immediate loading of delayed modified SLActive surface dental implants for rehabilitation of extremely atrophied maxilla: A case report. J. Oral Maxillofac. Surg. 2009, 67, 1486–1494. [Google Scholar] [CrossRef]
- Polini, F.; Robiony, M.; Sembronio, S.; Costa, F.; Politi, M. Bifunctional sculpturing of the bone graft for 3-dimensional augmentation of the atrophic posterior mandible. J. Oral Maxillofacial. Surg. 2009, 67, 174–177. [Google Scholar] [CrossRef]
- Troeltzsch, M.; Troeltzsch, M.; Kauffmann, P.; Gruber, R.; Brockmeyer, P.; Moser, N.; Rau, A.; Schliephake, H. Clinical efficacy of grafting materials in alveolar ridge augmentation: A systematic review. Int. J. Oral Maxillofac. Implant. 1997, 12, 232–236. [Google Scholar] [CrossRef]
- Marconcini, S.; Covani, U.; Giammarinaro, E.; Velasco-Ortega, E.; De Santis, D.; Alfonsi, F.; Barone, A. Clinical Success of Dental Implants Placed in Posterior Mandible Augmented with Interpositional Block Graft: 3-Year Results from a Prospective Cohort Clinical Study. J. Oral Maxillofac. Surg. 2019, 77, 289–298. [Google Scholar] [CrossRef]
- Pabst, A.; Kämmerer, P.W. Collagen matrices: Opportunities and perspectives in oral hard and soft tissue regeneration. Quintessence Int. 2020, 51, 318–327. [Google Scholar]
- Esposito, M.; Grusovin, M.G.; Felice, P.; Karatzopoulos, G.; Worthington, H.V.; Coulthard, P. The Efficacy of horizontal and vertical bone augmentation procedure for dental implants–A Cochrane systematic review. Eur. J. Oral. Implantol. 2009, 2, 167–184. [Google Scholar]
- Covani, U.; Marconcini, S.; Galassini, G.; Cornelini, R.; Santini, S.; Barone, A. Connective tissue graft used as a biologic barrier to cover an immediate implant. J. Periodontol. 2007, 78, 1644–1649. [Google Scholar] [CrossRef] [PubMed]
- Mounir, M.; Shalash, M.; Mounir, S.; Nassar, Y.; El Khatib, O. Assessment of three dimensional bone augmentation of severely atrophied maxillary alveolar ridges using prebent titanium mesh vs customized poly-ether-ether-ketone (PEEK) mesh: A randomized clinical trial. Clin. Implant Dent. Relat. Res. 2019, 21, 960–967. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, A.; Hildebrandt, H.; Schmohl, J.U.; Kämmerer, P.W. Evaluation of Risk Parameters in Bone Regeneration Using a Customized Titanium Mesh: Results of a Clinical Study. Implant Dent. 2019, 28, 543–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louis, P.J.; Gutta, R.; Said-Al-Naief, N.; Bartolucci, A.A. Reconstruction of the maxilla and mandible with particulate bone graft and titanium mesh for implant placement. J. Oral Maxillofac. Surg. 2008, 66, 235–245. [Google Scholar] [CrossRef]
- Corinaldesi, G.; Pieri, F.; Sapigni, L.; Marchetti, C. Evaluation of survival and success rates of dental implants placed at the time of or after alveolar ridge augmentation with an autogenous mandibular bone graft and titanium mesh: A 3- to 8-year retrospective study. Int. J. Oral Maxillofac. Implant. 2009, 24, 1119–1128. [Google Scholar]
- Von Arx, T.; Kurt, B. Implant placement and simultaneous ridge augmentation using autogenous bone and a micro titaniummesh: A prospective clinical study with 20 implants. Clin. Oral Implant. Res. 1999, 10, 24–33. [Google Scholar] [CrossRef]
- Von Arx, T.; Kurt, B. Implant placement and simultaneous peri-implant bone grafting using a micro titanium mesh for graft stabilization. Int. J. Periodont. Restor. Dent. 1998, 18, 117–127. [Google Scholar]
- Von Arx, T.; Kurt, B. Localized ridge augmentation using a micro titanium mesh: A report on 27 implants followed from 1 to 3 years after functional loading. Clin. Oral Implant. Res. 1998, 9, 123–130. [Google Scholar] [CrossRef]
- Malchiodi, L.; Scarano, A.; Quaranta, M.; Piatelli, A. Rigid Fixation by means of Titanium Mesh in Edentulous ridge Expansion for Horizontal Ridge Augmentation in the maxilla. Int. J. Oral Maxillofac. Implant. 1998, 13, 701–705. [Google Scholar]























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
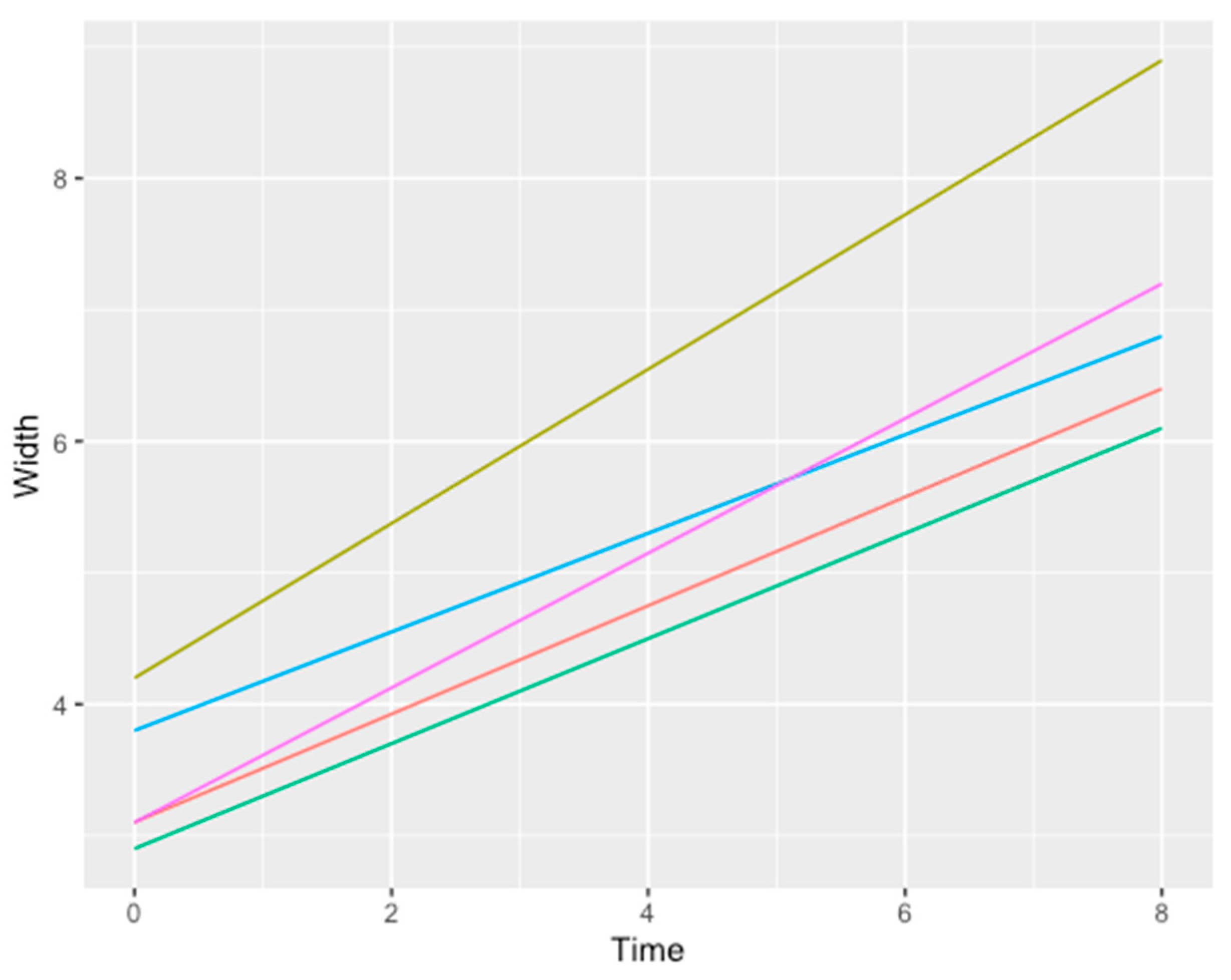
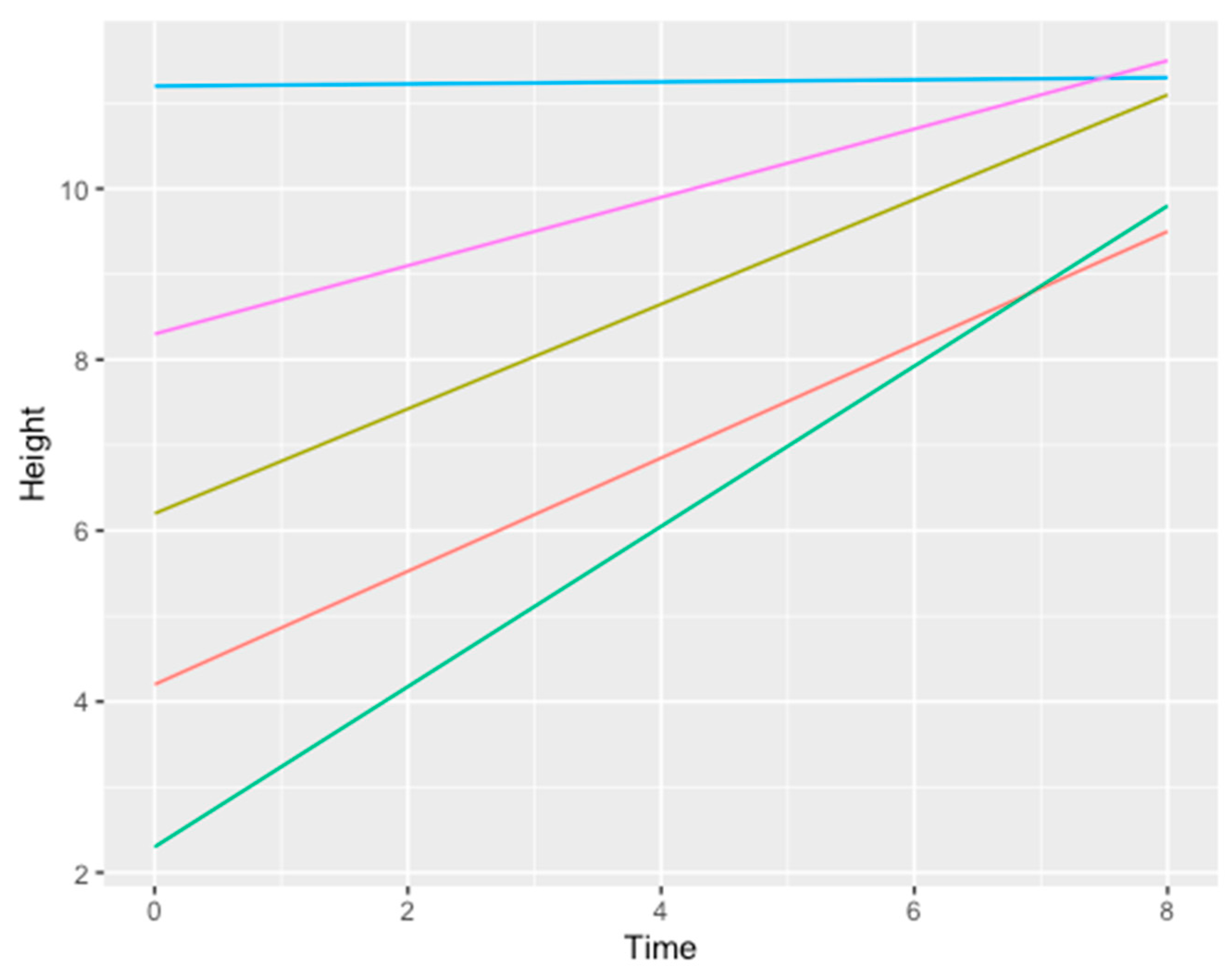
| Patient | Atrophic Site | Initial Width | Initial Height | Final Width | Final Height | Fixture |
|---|---|---|---|---|---|---|
| 1 | 36 | 4.2 ± 0.8 | 6.2 ± 0.8 | 8.9 ± 1.2 | 11.1 ± 2.2 | 1 |
| 2 | 24–25–26 | 2.9 ± 0.9 | 2.3 ± 1.3 | 6.1 ± 0.5 | 9.8 ± 0.3 | 3 |
| 3 | 12–11–21–22 | 3.8 ± 0.5 | 11.2 ± 0.5 | 6.8 ± 0.3 | 11.3 ± 0.5 | 4 |
| 4 | 36 | 3.1 ± 0.2 | 8.3 ± 0.8 | 7.2 ± 0.9 | 11.5 ± 0.3 | 1 |
| 5 | 14–15–16 | 3.1 ± 0.5 | 4.2 ± 0.2 | 6.4 ± 0.5 | 9.5 ± 0.5 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Santis, D.; Gelpi, F.; Verlato, G.; Luciano, U.; Torroni, L.; Antonucci, N.; Bernardello, F.; Zarantonello, M.; Nocini, P.F. Digital Customized Titanium Mesh for Bone Regeneration of Vertical, Horizontal and Combined Defects: A Case Series. Medicina 2021, 57, 60. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010060
De Santis D, Gelpi F, Verlato G, Luciano U, Torroni L, Antonucci N, Bernardello F, Zarantonello M, Nocini PF. Digital Customized Titanium Mesh for Bone Regeneration of Vertical, Horizontal and Combined Defects: A Case Series. Medicina. 2021; 57(1):60. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010060
Chicago/Turabian StyleDe Santis, Daniele, Federico Gelpi, Giuseppe Verlato, Umberto Luciano, Lorena Torroni, Nadia Antonucci, Fabio Bernardello, Morris Zarantonello, and Pier Francesco Nocini. 2021. "Digital Customized Titanium Mesh for Bone Regeneration of Vertical, Horizontal and Combined Defects: A Case Series" Medicina 57, no. 1: 60. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010060