Sudden Cardiac Death in Athletes in Italy during 2019: Internet-Based Epidemiological Research


Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
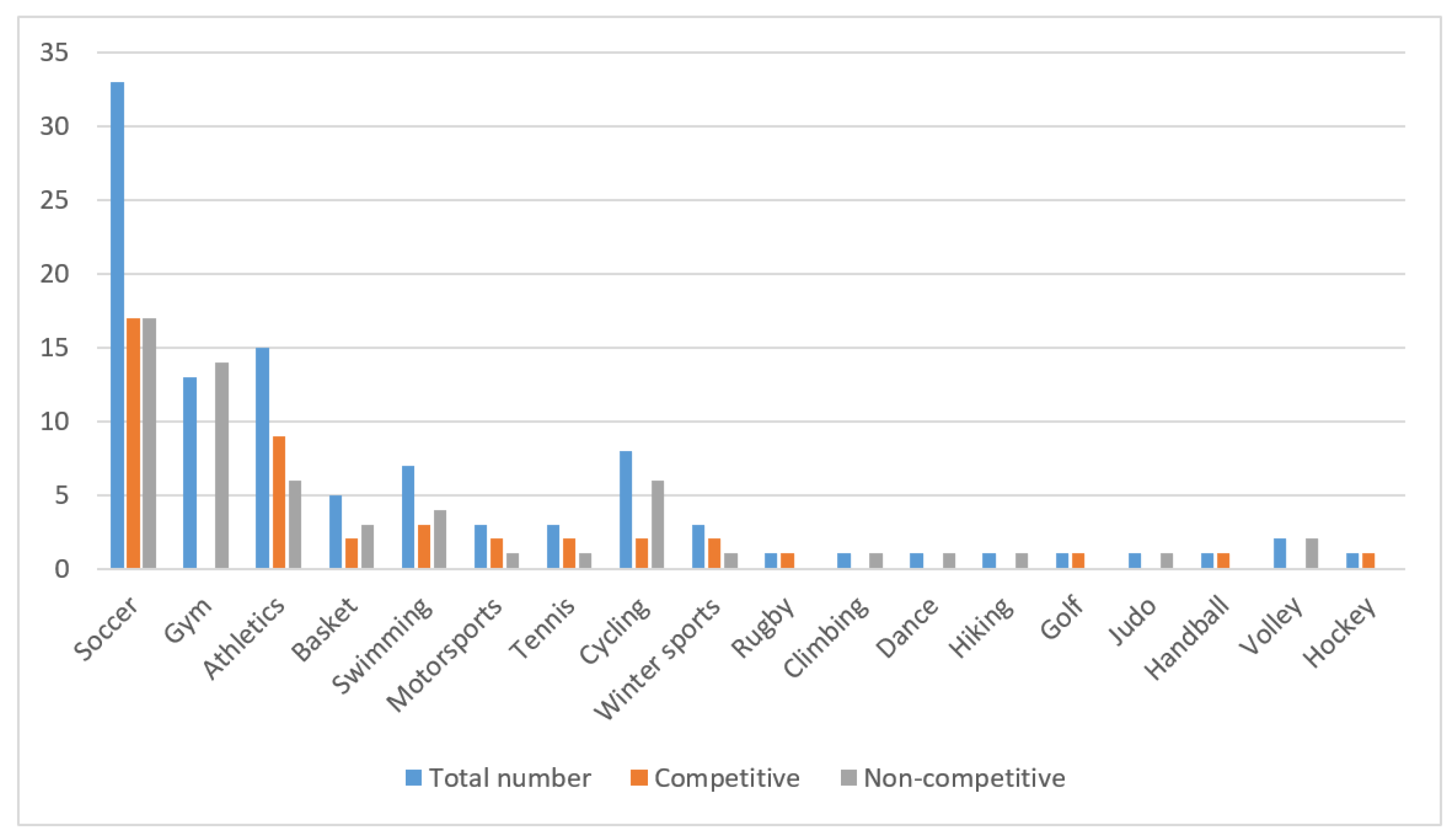
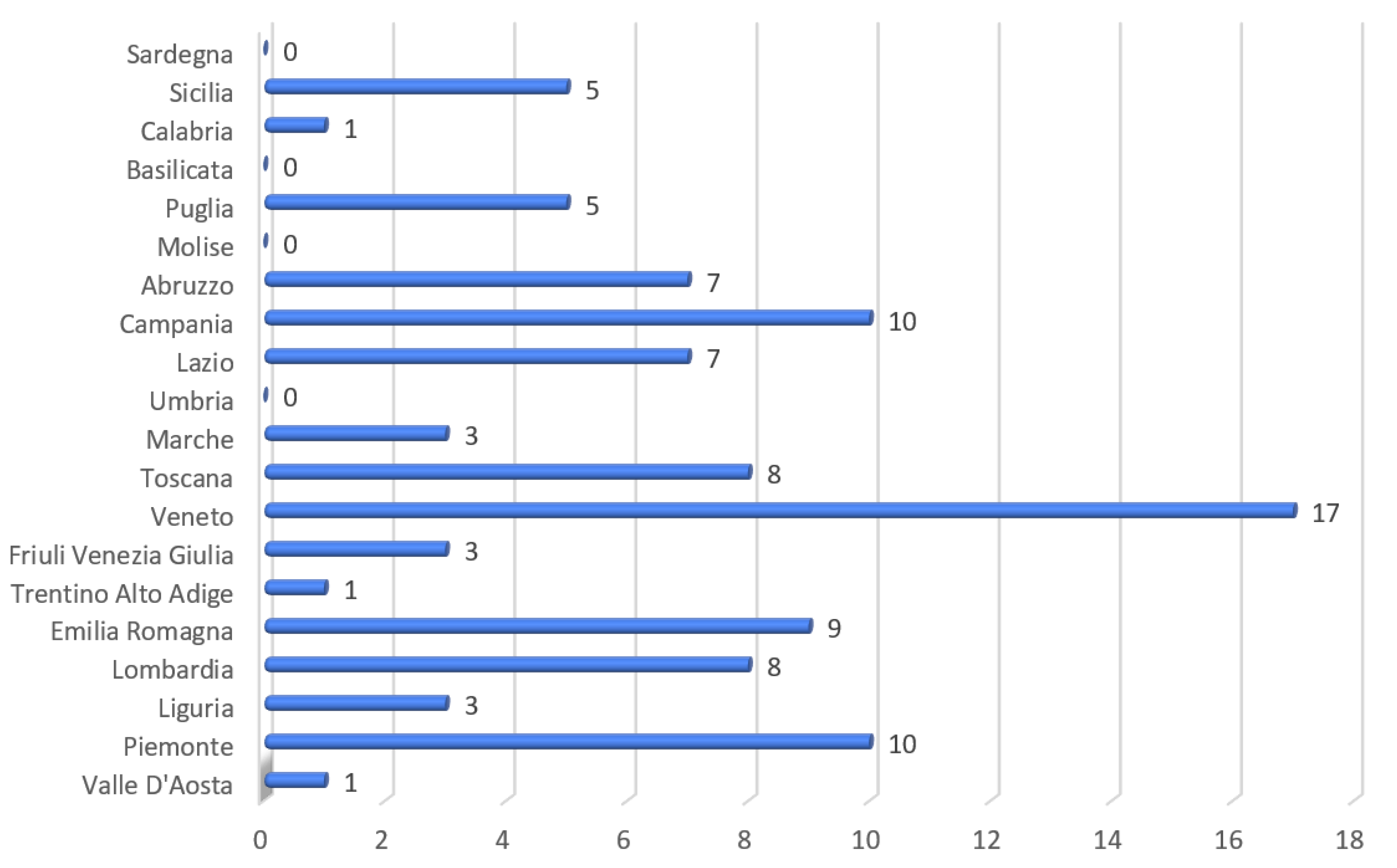
3. Results
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marijon, E.; Uy-Evanado, A.; Reinier, K.; Teodorescu, C.; Narayanan, K.; Jouven, X.; Gunson, K.; Jui, J.; Chugh, S.S. Sudden cardiac arrest during sports activity in middle age. Circulation 2015, 131, 1384–1391. [Google Scholar] [PubMed] [Green Version]
- Marijon, E.; Tafflet, M.; Celermajer, D.S.; Dumas, F.; Perier, M.C.; Mustafic, H.; Toussaint, J.F.; Desnos, M.; Rieu, M.; Benameur, N.; et al. Sports-related sudden death in the general population. Circulation 2011, 124, 672–681. [Google Scholar] [PubMed] [Green Version]
- Narayanan, K.; Bougouin, W.; Sharifzadehgan, A.; Waldmann, V.; Karam, N.; Marijon, E. Sudden Cardiac Death during Sports Activities in the General Population. Card. Electrophysiol. Clin. 2017, 9, 559–567. [Google Scholar] [PubMed]
- Solberg, E.E.; Borjesson, M.; Sharma, S.; Papadakis, M.; Wilhelm, M.; Drezner, J.A.; Harmon, K.G.; Alonso, J.M.; Heidbuchel, H.; Dugmore, D.; et al. Sudden cardiac arrest in sports-need for uniform registration: A Position Paper from the Sport Cardiology Section of the European Association for Cardiovascular Prevention and Rehabilitation. Eur. J. Prev. Cardiol. 2016, 23, 657–667. [Google Scholar]
- Lippi, G.; Favaloro, E.J.; Sanchis-Gomar, F. Sudden Cardiac and Noncardiac Death in Sports: Epidemiology, Causes, Pathogenesis, and Prevention. Semin. Thromb. Hemost. 2018, 8, 780–786. [Google Scholar]
- Bohm, P.; Scharhag, J.; Meyer, T. Data from a nationwide registry on sports-related sudden cardiac deaths in Germany. Eur. J. Prev. Cardiol. 2016, 23, 649–656. [Google Scholar]
- Malhotra, A.; Dhutia, H.; Finocchiaro, G.; Gati, S.; Beasley, I.; Clift, P.; Cowie, C.; Kenny, A.; Mayet, J.; Oxborough, D.; et al. Outcomes of Cardiac Screening in Adolescent Soccer Players. N. Engl. J. Med. 2018, 379, 524–534. [Google Scholar]
- Risgaard, B.; Winkel, B.G.; Jabbari, R.; Glinge, C.; Ingemann-Hansen, O.; Thomsen, J.L.; Ottesen, G.L.; Haunsø, S.; Holst, A.G.; Tfelt-Hansen, J. Sports-related sudden cardiac death in a competitive and a noncompetitive athlete population aged 12 to 49 years: Data from an unselected nationwide study in Denmark. Heart Rhythm. 2014, 11, 1673–1681. [Google Scholar]
- Maron, B.J.; Thompson, P.D.; Ackerman, M.J.; Balady, G.; Berger, S.; Cohen, D.; Dimeff, R.; Douglas, P.S.; Glover, D.W.; Hutter, A.M., Jr.; et al. Recommendations and considerations related to preparticipation screening for cardiovascular abnormalities in competitive athletes: 2007 update: A scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism: Endorsed by the American College of Cardiology Foundation. Circulation 2007, 115, 1643–1655. [Google Scholar]
- Decreto Ministeriale 4 Aprile 2001. Gazzetta Ufficiale della Repubblica Italiana—Serie Generale, Rome, 17 April 2001; No. 89.
- Corrado, D.; Basso, C.; Pavei, A.; Michieli, P.; Schiavon, M.; Thiene, G. Trends in sudden cardiovascular death in young competitive athletes after implementation of a preparticipation screening program. JAMA 2006, 296, 1593–1601. [Google Scholar]
- Holst, A.G.; Winkel, B.G.; Theilade, J.; Kristensen, I.B.; Thomsen, J.L.; Ottesen, G.L.; Svendsen, J.H.; Haunsø, S.; Prescott, E.; Tfelt-Hansen, J. Incidence and etiology of sports-related sudden cardiac death in Denmark: Implications for preparticipation screening. Heart Rhythm. 2010, 7, 1365–1371. [Google Scholar]
- Berge, H.M.; Andersen, T.E.; Bahr, R. Cardiovascular incidents in male professional football players with negative preparticipation cardiac screening results: An 8-year follow-up. Br. J. Sports Med. 2018, 53, 1279–1284. [Google Scholar]
- Oliva, A.; Grassi, V.M.; Campuzano, O.; Brion, M.; Arena, V.; Partemi, S.; Coll, M.; Pascali, V.L.; Brugada, J.; Carracedo, A.; et al. Medico-legal perspectives on sudden cardiac death in young athletes. Int. J. Leg. Med. 2017, 131, 393–409. [Google Scholar]
- Maron, B.J.; Levine, B.D.; Washington, R.L.; Baggish, A.L.; Kovacs, R.J.; Maron, M.S.; American Heart Association Electrocardiography and Arrhythmias Committee of Council on Clinical Cardiology; Council on Cardiovascular Disease in Young; Council on Cardiovascular and Stroke Nursing; Council on Functional Genomics and Translational Biology; et al. Eligibility and Disqualification Recommendations for Competitive Athletes with Cardiovascular Abnormalities: Task Force 2: Preparticipation Screening for Cardiovascular Disease in Competitive Athletes: A Scientific Statement From the American Heart Association and American College of Cardiology. Circulation 2015, 132, e267–e272. [Google Scholar]
- Schoenbaum, M.; Denchev, P.; Vitiello, B.; Kaltman, J.R. Economic evaluation of strategies to reduce sudden cardiac death in young athletes. Pediatrics 2012, 130, e380–e389. [Google Scholar]
- Vessella, T.; Zorzi, A.; Merlo, L.; Pegoraro, C.; Giorgiano, F.; Trevisanato, M.; Viel, M.; Formentini, P.; Corrado, D.; Sarto, P. The Italian preparticipation evaluation programme: Diagnostic yield, rate of disqualification and cost analysis. Br. J. Sports Med. 2020, 54, 231–237. [Google Scholar] [PubMed] [Green Version]
- Mitchell, J.H.; Maron, B.J.; Epstein, S.E. 16th Bethesda Conference: Cardiovascular abnormalities in the athlete: Recommendations regarding eligibility for competition. J. Am. Coll. Cardiol. 1985, 6, 1186–1232. [Google Scholar] [PubMed]
- Italian National Institute of Statistics (ISTAT). Annual Report 2020—The State of the Nation. Available online: https://www.istat.it/en/archivio/247100 (accessed on 11 January 2021).
- CONI Servizi. I Numeri dello Sport 2017. Available online: https://www.coni.it/images/numeri_dello_sport/Rapporto_FSN_DSA_2017.pdf (accessed on 11 January 2021).
- Drezner, J.A.; Rao, A.L.; Heistand, J.; Bloomingdale, M.K.; Harmon, K.G. Effectiveness of emergency response planning for sudden cardiac arrest in United States high schools with automated external defibrillators. Circulation 2009, 120, 518–525. [Google Scholar]
- Corrado, D.; Basso, C.; Rizzoli, G.; Schiavon, M.; Thiene, G. Does sports activity enhance the risk of sudden death in adolescents and young adults? J. Am. Coll. Cardiol. 2003, 42, 1959–1963. [Google Scholar] [PubMed]
- Margey, R.; Roy, A.; Tobin, S.; O’Keane, C.J.; McGorrian, C.; Morris, V.; Jennings, S.; Galvin, J. Sudden cardiac death in 14- to 35-year olds in Ireland from 2005 to 2007: A retrospective registry. Europace 2011, 13, 1411–1418. [Google Scholar] [PubMed]
- Maron, B.J.; Haas, T.S.; Ahluwalia, A.; Rutten-Ramos, S.C. Incidence of cardiovascular sudden deaths in Minnesota high school athletes. Heart Rhythm. 2013, 10, 374–377. [Google Scholar] [CrossRef] [PubMed]
- Harmon, K.G.; Asif, I.M.; Klossner, D.; Drezner, J.A. Incidence of sudden cardiac death in National Collegiate Athletic Association Athletes. Circulation 2011, 123, 1594–1600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckart, R.E.; Shry, E.A.; Burke, A.P.; McNear, J.A.; Appel, D.A.; Castillo-Rojas, L.M.; Avedissian, L.; Pearse, L.A.; Potter, R.N.; Tremaine, L.; et al. Sudden death in young adults: An autopsy-based series of a population undergoing active surveillance. J. Am. Coll. Cardiol. 2011, 58, 1254–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maron, B.J.; Doerer, J.J.; Haas, T.S.; Tierney, D.M.; Mueller, F.O. Sudden deaths in young competitive athletes analysis of 1866 deaths in the United States 1980–2006. Circulation 2009, 119, 1085–1092. [Google Scholar] [CrossRef]
- Agut-Busquet, A.; Galtés, I. Sudden cardiac death and sport. Review and key trends. Rev. Esp. Med. Leg. 2018, 44, 158–168. [Google Scholar]
- Harmon, K.G.; Drezner, J.A.; Wilson, M.G.; Sharma, S. Incidence of sudden cardiac death in athletes: A state-of-the-art review. Heart 2014, 100, 1227–1234. [Google Scholar] [CrossRef]
- Zorzi, A.; Susana, A.; Spadotto, V.; Cacciavillani, L.; Corrado, D. L’arresto cardiaco negli impianti sportivi nel 2015: Possibili implicazioni epidemiologiche dell’applicazione della “Legge Balduzzi” [Sudden cardiac arrest in Italian sports facilities in 2015: Epidemiological implications of the so-called “Balduzzi decree”]. G. Ital. Cardiol. 2016, 17, 903–907. [Google Scholar]
- Finegold, J.A.; Asaria, P.; Francis, D.P. Mortality from ischaemic heart disease by country, region, and age: Statistics from World Health Organisation and United Nations. Int. J. Cardiol. 2013, 168, 934–945. [Google Scholar] [CrossRef] [Green Version]
- Gervasi, S.F.; Palumbo, L.; Cammarano, M.; Orvieto, S.; Di Rocco, A.; Vestri, A.; Marano, R.; Savino, G.; Bianco, M.; Zeppilli, P.; et al. Coronary atherosclerosis in apparently healthy master athletes discovered during pre-PARTECIPATION screening. Role of coronary CT angiography (CCTA). Int. J. Cardiol. 2019, 282, 99–107. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sport | Competitive Athletes | SCD-A in Competitive Athletes | Incidence of SCD-A Per Sport (Per 100,000 Athletes/Year) |
|---|---|---|---|
| Soccer | 1,056,824 | 17 | 1.6 |
| Tennis | 372,964 | 2 | 0.5 |
| Basketball | 317,321 | 2 | 0.6 |
| Athletics | 270,602 | 9 | 3.3 |
| Swimming | 163,307 | 3 | 1.8 |
| Golf | 90,167 | 1 | 1.1 |
| Rugby | 82,432 | 1 | 1.2 |
| Cycling | 75,543 | 2 | 2.6 |
| Winter sports | 73,541 | 2 | 2.7 |
| Handball | 33,021 | 1 | 3.3 |
| Motorsports | 20,958 | 2 | 9.5 |
| Hockey | 5509 | 1 | 18.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sollazzo, F.; Palmieri, V.; Gervasi, S.F.; Cuccaro, F.; Modica, G.; Narducci, M.L.; Pelargonio, G.; Zeppilli, P.; Bianco, M. Sudden Cardiac Death in Athletes in Italy during 2019: Internet-Based Epidemiological Research. Medicina 2021, 57, 61. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010061
Sollazzo F, Palmieri V, Gervasi SF, Cuccaro F, Modica G, Narducci ML, Pelargonio G, Zeppilli P, Bianco M. Sudden Cardiac Death in Athletes in Italy during 2019: Internet-Based Epidemiological Research. Medicina. 2021; 57(1):61. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010061
Chicago/Turabian StyleSollazzo, Fabrizio, Vincenzo Palmieri, Salvatore Francesco Gervasi, Francesco Cuccaro, Gloria Modica, Maria Lucia Narducci, Gemma Pelargonio, Paolo Zeppilli, and Massimiliano Bianco. 2021. "Sudden Cardiac Death in Athletes in Italy during 2019: Internet-Based Epidemiological Research" Medicina 57, no. 1: 61. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010061