Accuracy of Contrast Extravasation on Computed Tomography for Diagnosing Severe Pelvic Hemorrhage in Pelvic Trauma Patients: A Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
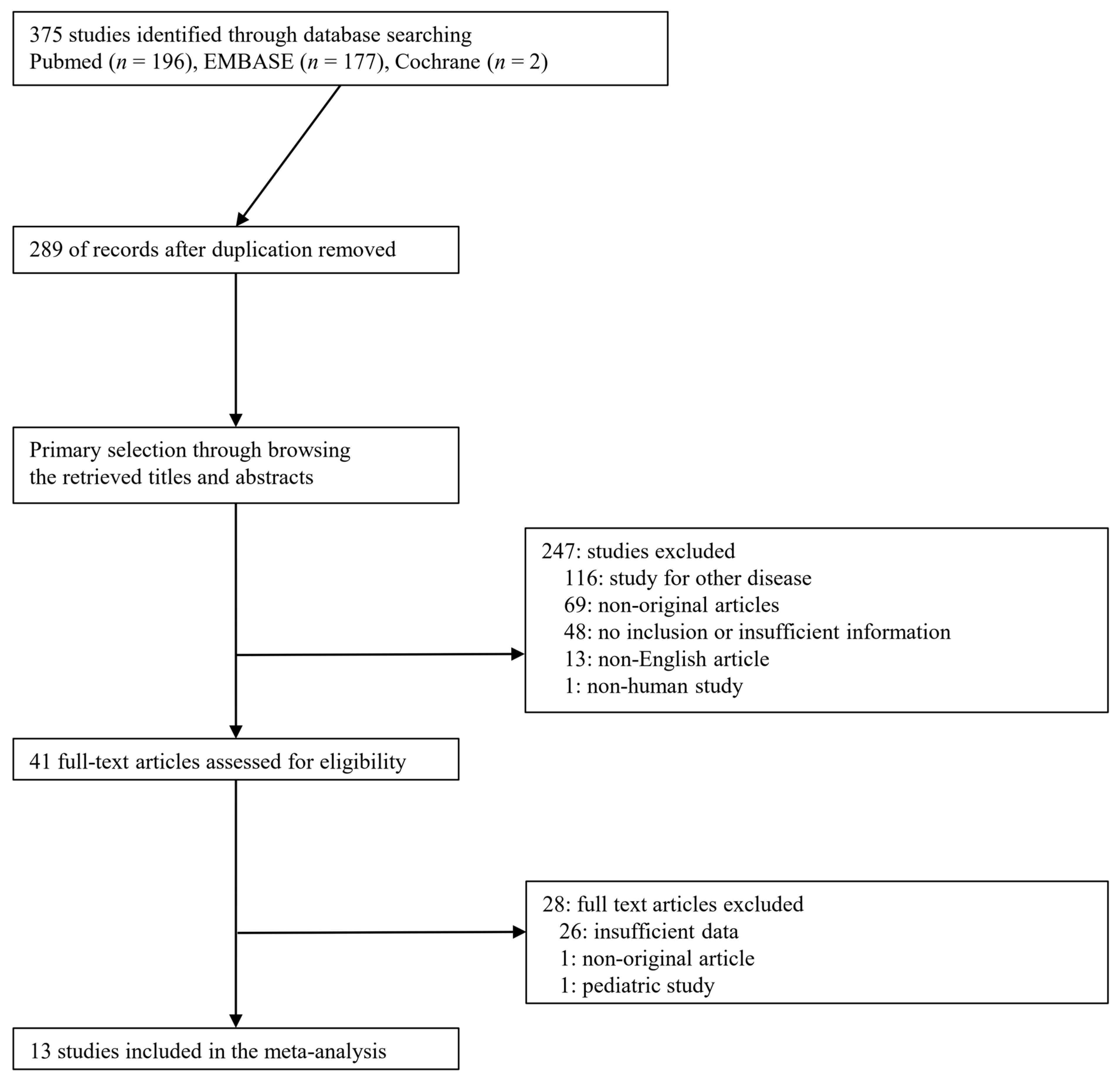
2.1. Published Study Search and Selection Criteria
2.2. Data Extraction
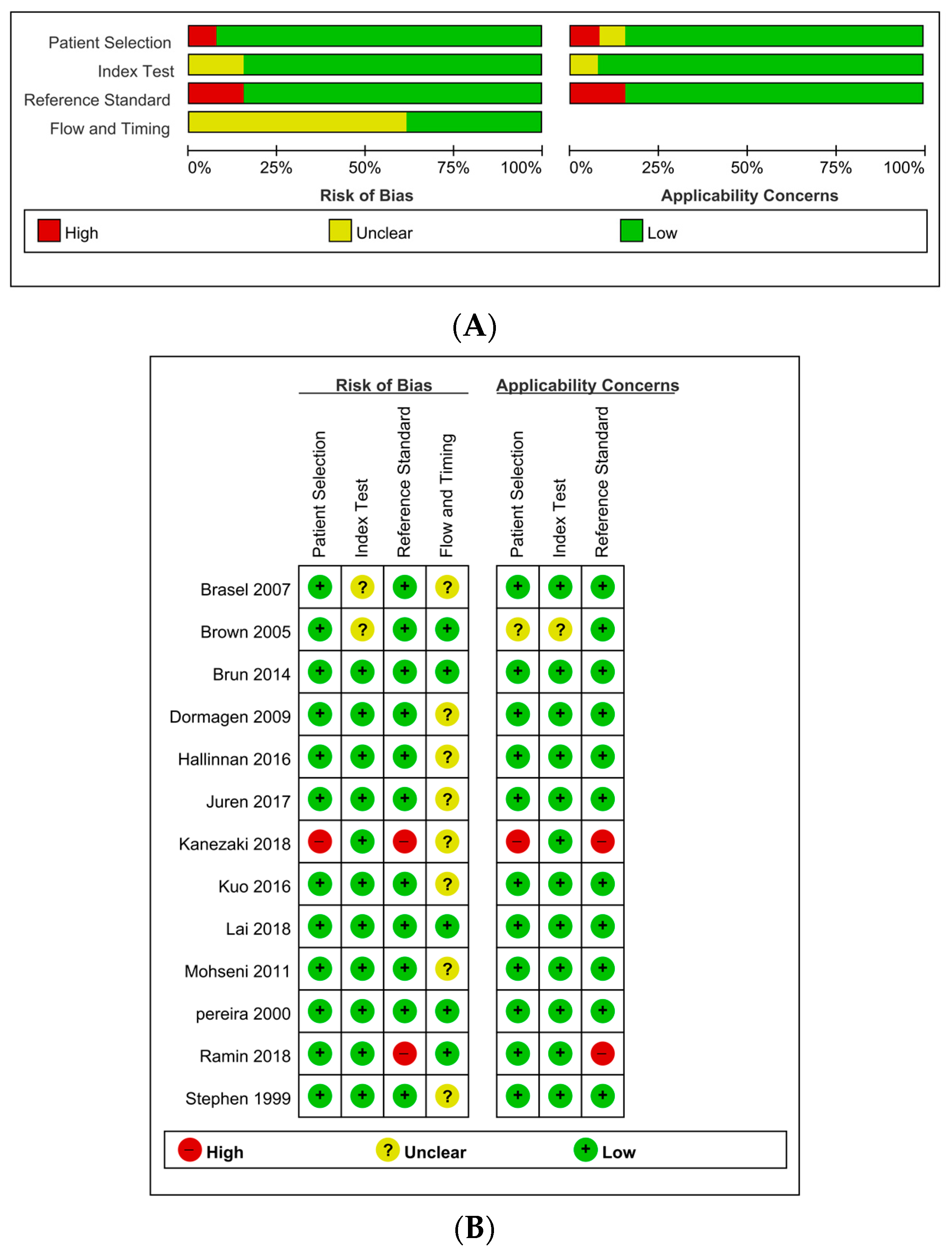
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Selection and Characteristics
3.2. Clinical Characteristics of Patients and Contrast Extravasation on CT
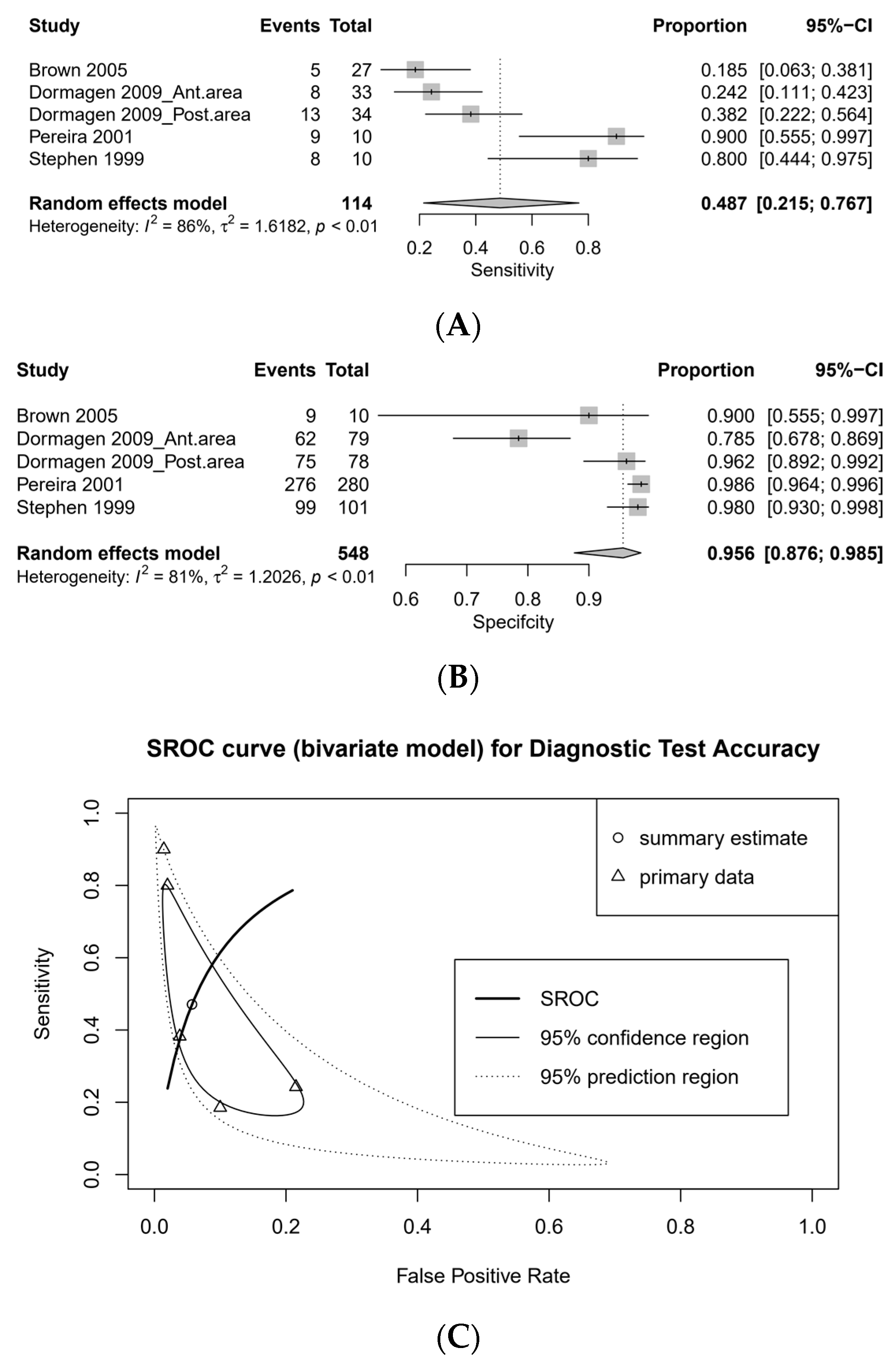
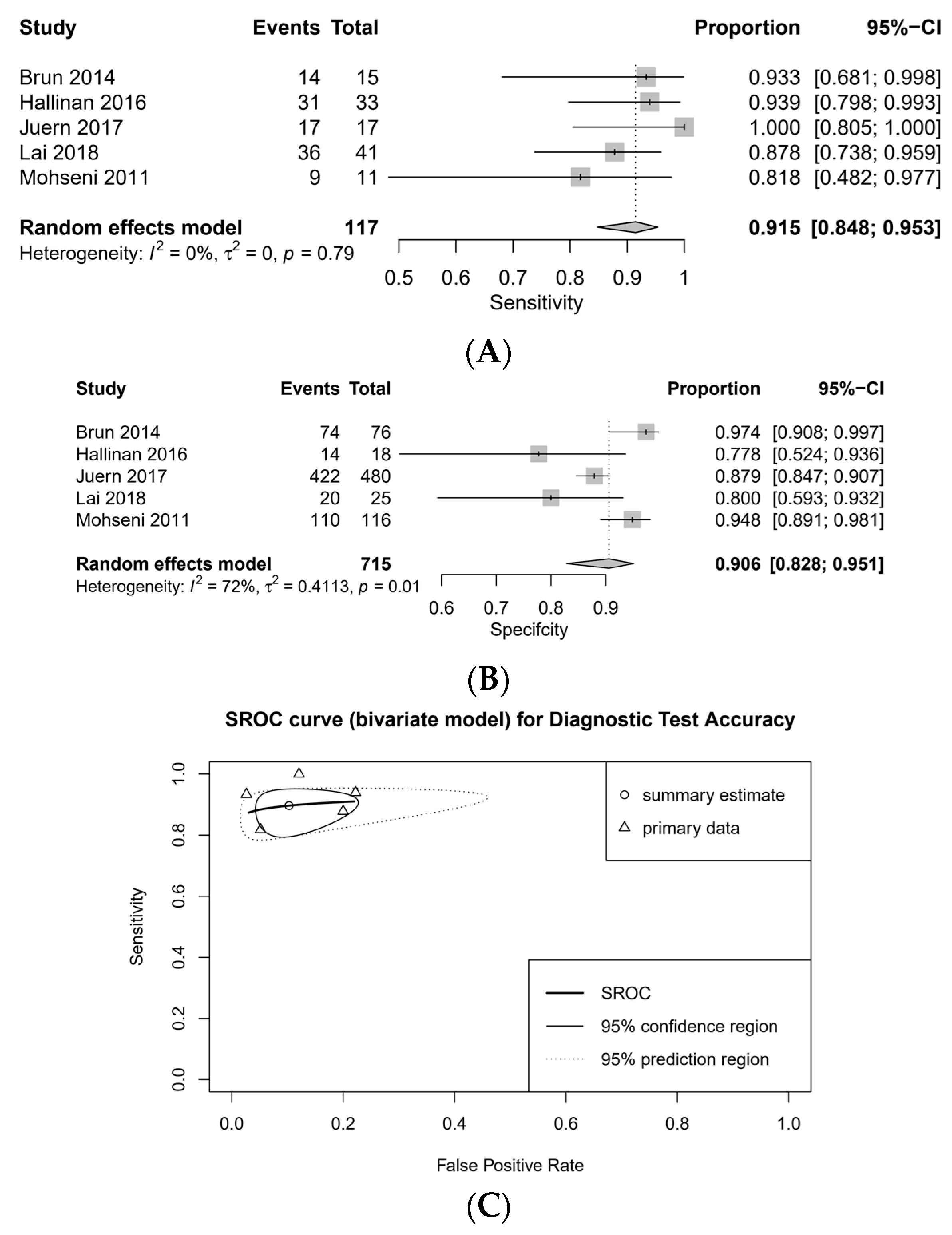
3.3. DTA Review
3.4. Sensitivity Analysis and Subgroup Analysis
3.5. Quality Assessment
3.6. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jang, J.Y.; Shim, H.; Jung, P.Y.; Kim, S.; Bae, K.S. Preperitoneal pelvic packing in patients with hemodynamic instability due to severe pelvic fracture: Early experience in a Korean trauma center. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Burlew, C.C.; Moore, E.E.; Stahel, P.F.; Geddes, A.E.; Wagenaar, A.E.; Pieracci, F.M.; Fox, C.J.; Campion, E.M.; Johnson, J.L.; Mauffrey, C. Preperitoneal pelvic packing reduces mortality in patients with life-threatening hemorrhage due to unstable pelvic fractures. J. Trauma Acute Care Surg. 2017, 82, 233. [Google Scholar] [CrossRef] [PubMed]
- Costantini, T.W.; Coimbra, R.; Holcomb, J.B.; Podbielski, J.M.; Catalano, R.; Blackburn, A.; Scalea, T.M.; Stein, D.M.; Williams, L.; Conflitti, J. Current management of hemorrhage from severe pelvic fractures: Results of an American Association for the Surgery of Trauma multi-institutional trial. J. Trauma Acute Care Surg. 2016, 80, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Pommerening, M.J.; Goodman, M.D.; Holcomb, J.B.; Wade, C.E.; Fox, E.E.; del Junco, D.J.; Brasel, K.J.; Bulger, E.M.; Cohen, M.J.; Alarcon, L.H. Clinical gestalt and the prediction of massive transfusion after trauma. Injury 2015, 46, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Tran, A.; Matar, M.; Lampron, J.; Steyerberg, E.; Taljaard, M.; Vaillancourt, C. Early identification of patients requiring massive transfusion, embolization or hemostatic surgery for traumatic hemorrhage: A systematic review and meta-analysis. J. Trauma Acute Care Surg. 2018, 84, 505–516. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, T.; Yamakawa, K.; Matsuda, H.; Yoshikawa, Y.; Wada, D.; Hamasaki, T.; Ono, K.; Nakamori, Y.; Fujimi, S. The survival benefit of a novel trauma workflow that includes immediate whole-body computed tomography, surgery, and interventional radiology, all in one trauma resuscitation room: A retrospective historical control study. Ann. Surg. 2019, 269, 370. [Google Scholar] [CrossRef] [PubMed]
- Wada, D.; Nakamori, Y.; Yamakawa, K.; Fujimi, S. First clinical experience with IVR-CT system in the emergency room: Positive impact on trauma workflow. Scand. J. Trauma Resusc. Emerg. Med. 2012, 20, 52. [Google Scholar] [CrossRef]
- Dreizin, D.; Liang, Y.; Dent, J.; Akhter, N.; Mascarenhas, D.; Scalea, T.M. Diagnostic value of CT contrast extravasation for major arterial injury after pelvic fracture: A meta-analysis. Am. J. Emerg. Med. 2019, 38, 2335–2342. [Google Scholar] [CrossRef]
- McInnes, M.D.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: The PRISMA-DTA statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Brasel, K.J.; Pham, K.; Yang, H.; Christensen, R.; Weigelt, J.A. Significance of contrast extravasation in patients with pelvic fracture. J. Trauma Acute Care Surg. 2007, 62, 1149–1152. [Google Scholar] [CrossRef]
- Brown, C.V.; Kasotakis, G.; Wilcox, A.; Rhee, P.; Salim, A.; Demetriades, D. Does pelvic hematoma on admission computed tomography predict active bleeding at angiography for pelvic fracture? Am. Surg. 2005, 71, 759–762. [Google Scholar] [CrossRef] [PubMed]
- Brun, J.; Guillot, S.; Bouzat, P.; Broux, C.; Thony, F.; Genty, C.; Heylbroeck, C.; Albaladejo, P.; Arvieux, C.; Tonetti, J.; et al. Detecting active pelvic arterial haemorrhage on admission following serious pelvic fracture in multiple trauma patients. Injury 2014, 45, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Dormagen, J.B.; Tötterman, A.; Røise, O.; Sandvik, L.; Kløw, N.E. Efficacy of plain radiography and computer tomography in localizing the site of pelvic arterial bleeding in trauma patients. Acta Radiol. 2010, 51, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Hallinan, J.T.P.D.; Tan, C.H.; Pua, U. The role of multidetector computed tomography versus digital subtraction angiography in triaging care and management in abdominopelvic trauma. Singap. Med. J. 2016, 57, 497. [Google Scholar] [CrossRef] [PubMed]
- Juern, J.S.; Milia, D.; Codner, P.; Beckman, M.; Somberg, L.; Webb, T.; Weigelt, J.A. Clinical significance of computed tomography contrast extravasation in blunt trauma patients with a pelvic fracture. J. Trauma Acute Care Surg. 2017, 82, 138–140. [Google Scholar] [CrossRef] [PubMed]
- Kanezaki, S.; Miyazaki, M.; Notani, N.; Tsumura, H. Clinical presentation of geriatric polytrauma patients with severe pelvic fractures: Comparison with younger adult patients. Eur. J. Orthop. Surg. Traumatol. 2016, 26, 885–890. [Google Scholar] [CrossRef] [PubMed]
- Kuo, L.-W.; Yang, S.-J.; Fu, C.-Y.; Liao, C.-H.; Wang, S.-Y.; Wu, S.-C. Relative hypotension increases the probability of the need for angioembolisation in pelvic fracture patients without contrast extravasation on computed tomography scan. Injury 2016, 47, 37–42. [Google Scholar]
- Lai, Y.-C.; Wu, C.-H.; Chen, H.-W.; Wang, L.-J.; Wong, Y.-C. Predictors of active arterial hemorrhage on angiography in pelvic fracture patients. Jpn. J. Radiol. 2018, 36, 223–230. [Google Scholar] [CrossRef]
- Mohseni, S.; Talving, P.; Kobayashi, L.; Lam, L.; Inaba, K.; Branco, B.C.; Oliver, M.; Demetriades, D. The diagnostic accuracy of 64-slice computed tomography in detecting clinically significant arterial bleeding after pelvic fractures. Am. Surg. 2011, 77, 1176–1182. [Google Scholar] [CrossRef]
- Pereira, S.J.; O’Brien, D.P.; Luchette, F.A.; Choe, K.A.; Lim, E.; Davis, K., Jr.; Hurst, J.M.; Johannigman, J.A.; Frame, S.B. Dynamic helical computed tomography scan accurately detects hemorrhage in patients with pelvic fracture. Surgery 2000, 128, 678–685. [Google Scholar]
- Ramin, S.; Hermida, M.; Millet, I.; Murez, T.; Monnin, V.; Hamoui, M.; Capdevila, X.; Charbit, J. Limits of intravascular contrast extravasation on computed tomography scan to define the need for pelvic angioembolization in pelvic blunt trauma: A specific assessment on the risk of false positives. J. Trauma Acute Care Surg. 2018, 85, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Stephen, D.J.; Kreder, H.J.; Day, A.C.; McKee, M.D.; Schemitsch, E.H.; ElMaraghy, A.; Hamilton, P.; McLellan, B. Early detection of arterial bleeding in acute pelvic trauma. J. Trauma Acute Care Surg. 1999, 47, 638. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.; Rutjes, A.W.; Reitsma, J.B.; Bossuyt, P.M.; Kleijnen, J. The development of QUADAS: A tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med. Res. Methodol. 2003, 3, 25. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2009. [Google Scholar]
- Macaskill, P.; Gatsonis, C.; Deeks, J.; Harbord, R.; Takwoingi, Y. Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy; Version 0.9.0; The Cochrane Collaboration: London, UK, 2010. [Google Scholar]
- Verbeek, D.O.; Zijlstra, I.A.; van der Leij, C.; Ponsen, K.J.; van Delden, O.M.; Goslings, J.C. Management of pelvic ring fracture patients with a pelvic “blush” on early computed tomography. J. Trauma Acute Care Surg. 2014, 76, 374–379. [Google Scholar] [CrossRef]
- Tran, T.L.N.; Brasel, K.J.; Karmy-Jones, R.; Rowell, S.; Schreiber, M.A.; Shatz, D.V.; Albrecht, R.M.; Cohen, M.J.; DeMoya, M.A.; Biffl, W.L. Western Trauma Association Critical Decisions in Trauma: Management of pelvic fracture with hemodynamic instability—2016 updates. J. Trauma Acute Care Surg. 2016, 81, 1171–1174. [Google Scholar] [CrossRef]
- Coccolini, F.; Stahel, P.F.; Montori, G.; Biffl, W.; Horer, T.M.; Catena, F.; Kluger, Y.; Moore, E.E.; Peitzman, A.B.; Ivatury, R. Pelvic trauma: WSES classification and guidelines. World J. Emerg. Surg. 2017, 12, 1–18. [Google Scholar] [CrossRef]
- van Trigt, J.; Schep, N.W.; Peters, R.W.; Goslings, J.C.; Schepers, T.; Halm, J.A. Routine pelvic X-rays in asymptomatic hemodynamically stable blunt trauma patients: A meta-analysis. Injury 2018, 49, 2024–2031. [Google Scholar] [CrossRef]
- Stewart, B.G.; Rhea, J.T.; Sheridan, R.L.; Novelline, R.A. Is the screening portable pelvis film clinically useful in multiple trauma patients who will be examined by abdominopelvic CT? Experience with 397 patients. Emerg. Radiol. 2002, 9, 266–271. [Google Scholar] [CrossRef]
- Richards, J.R.; McGahan, J.P. Focused assessment with sonography in trauma (FAST) in 2017: What radiologists can learn. Radiology 2017, 283, 30–48. [Google Scholar] [CrossRef]
- Friese, R.S.; Malekzadeh, S.; Shafi, S.; Gentilello, L.M.; Starr, A. Abdominal ultrasound is an unreliable modality for the detection of hemoperitoneum in patients with pelvic fracture. J. Trauma Acute Care Surg. 2007, 63, 97–102. [Google Scholar] [CrossRef]
- Grünherz, L.; Jensen, K.O.; Neuhaus, V.; Mica, L.; Werner, C.M.; Ciritsis, B.; Michelitsch, C.; Osterhoff, G.; Simmen, H.-P.; Sprengel, K. Early computed tomography or focused assessment with sonography in abdominal trauma: What are the leading opinions? Eur. J. Trauma Emerg. Surg. 2018, 44, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Sierink, J.C.; Treskes, K.; Edwards, M.J.; Beuker, B.J.; den Hartog, D.; Hohmann, J.; Dijkgraaf, M.G.; Luitse, J.S.; Beenen, L.F.; Hollmann, M.W. Immediate total-body CT scanning versus conventional imaging and selective CT scanning in patients with severe trauma (REACT-2): A randomised controlled trial. Lancet 2016, 388, 673–683. [Google Scholar] [CrossRef]
- Chidambaram, S.; Goh, E.L.; Khan, M.A. A meta-analysis of the efficacy of whole-body computed tomography imaging in the management of trauma and injury. Injury 2017, 48, 1784–1793. [Google Scholar] [CrossRef] [PubMed]
- The ATLS Subcommittee; American College of Surgeons’ Committee on Trauma; The International ATLS Working Group. Advanced trauma life support (ATLS®): The ninth edition. J. Trauma Acute Care Surg. 2013, 74, 1363–1366. [Google Scholar]
- Lau, J.; Ioannidis, J.P.; Terrin, N.; Schmid, C.H.; Olkin, I. The case of the misleading funnel plot. BMJ 2006, 333, 597–600. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Location | Study Design | Study Period | Trauma Type | CT Modality (Detector Row) | Contrast Agent Infusion Amount, Rate | Scan Time after Contrast Agent Infusion | Reference Standard | Hemostatic Modality | Time from Admission to Hemostasis | Subgroup | Number of Patients | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | CE (+) | CE (−) | ||||||||||||
| Brasel 2007 | USA, single level 1 center | Re | 1998–2005 | ND | 4, 8, 16 | 150 mL, 5 mL/s | 60 s | Angiography | AE | ND | 604 | 42 | 562 | |
| Brown 2005 | USA, single level 1 center | Re | 2001–2003 | ND | 1 | 350 mL, 2 mL/s | ND | Angiography | AE | 7 ± 4 h | 37 | 6 | 31 | |
| Brun 2014 | France, single level 1 center | Re | 2004–2008 | ND | 40, 64 | ND | ND | Angiography | AE | 120 (77–191) min, median(IQR) | Stabilized patients | 95 | 16 | 75 |
| Unstabilized patients | ||||||||||||||
| Dormagen 2009 | Norway, single center | Re | 1995–2007 | ND | 1,2,4 | 100–150 mL, 2–5 mL/s | 70 s | Angiography | AE | ND | Anterior area | 112 | 25 | 87 |
| Arterial blush | ||||||||||||||
| Posterior area | 112 | 34 | 78 | |||||||||||
| Arterial blush | ||||||||||||||
| Hallinan 2016 | Singapore, single center | Re | 2004–2012 | Blunt | 16 or 64 | 100 mL, 3 mL/s | 70 s | Angiography | AE | within 24 h | 51 | 35 | 16 | |
| Juern 2017 | USA, single level 1 center | Re | 2009–2014 | Blunt | 64 | 125 mL, 2.5 mL/s | 70 s | Angiography | AE | ND | 497 | 75 | 422 | |
| Kanezaki 2016 | Japan, single center | Re | 2012–2015 | ND | ND | ND | ND | Angiography | AE | ND | Geriatric group | 15 | 10 | 5 |
| Surgery | IABO | |||||||||||||
| Pelvic fixation | ||||||||||||||
| Surgical hemostasis | ||||||||||||||
| Younger group | 13 | 6 | 7 | |||||||||||
| Kuo 2016 | Taiwan, single center | Re | 2005–2012 | ND | ND | ND | ND | Angiography | AE | ND | 201 | 47 | 154 | |
| Lai 2018 | Taiwan, single center | Re | 2012–2014 | ND | 64 | 100 mL, 3 mL/s | 70 s | Angiography | AE | 3.2 h, mean | 66 | 41 | 25 | |
| Mohseni 2011 | USA, single level 1 center | Re | 2008–2010 | Blunt | 64 | 100 mL, 3 mL/s | ND | Angiography | AE | ND | 127 | 15 | 112 | |
| Surgery | BILA | |||||||||||||
| PP | ||||||||||||||
| Pereira 2001 | USA, single level 1 center | Re | 1994–1999 | ND | 1 | 150 mL, 2 mL/s | 60 s | Angiography | AE | 3.3 ± 0.4 h | 290 | 13 | 277 | |
| Ramin 2018 | France, single level 1 center | Re | 2010–2015 | ND | 64 | 140 mL, 4 mL/s | 70–80 s | Angiography | AE | 120 (90–560) min, median (IQR) | 311 | 94 | 217 | |
| Surgery | PP | |||||||||||||
| Pelvic fixation | ||||||||||||||
| Stephen 1999 | Canada, two level 1 centers | Re | 1995–1996 | ND | 1 | 100 mL, 2 mL/s | 65 s | Angiography | AE | 11 (3–49) hours, median (range) | 111 | 10 | 101 | |
| Number of Subsets | Fixed Effect (95% CI) | Heterogeneity Test (p-Value) | Random Effect (95% CI) | Egger’s Test (p-Value) | |
|---|---|---|---|---|---|
| Age, mean | |||||
| CE (+) | 5 | 49.431 (47.195, 51.667) | 0.326 | 49.251 (46.761, 51.742) | 0.361 |
| CE (−) | 5 | 39.032 (38.904, 39.161) | <0.001 | 40.185 (38.241, 42.129) | 0.332 |
| Sex, male rate | |||||
| CE (+) | 5 | 0.623 (0.559, 0.683) | 0.074 | 0.615 (0.511, 0.710) | 0.660 |
| CE (−) | 5 | 0.601 (0.577, 0.625) | 0.279 | 0.603 (0.575, 0.631) | 0.110 |
| ISS, mean | |||||
| CE (+) | 4 | 30.762 (28.834, 32.690) | <0.001 | 29.536 (24.215, 34.857) | 0.537 |
| CE (−) | 4 | 18.210 (18.117, 18.304) | <0.001 | 19.184 (17.707, 20.660) | 0.413 |
| Mortality, rate | |||||
| CE (+) | 7 | 0.163 (0.125, 0.208) | 0.682 | 0.163 (0.125, 0.208) | 0.078 |
| CE (−) | 5 | 0.057 (0.045, 0.072) | 0.015 | 0.048 (0.029, 0.078) | 0.046 |
| Number | Fixed Effect | Heterogeneity Test | Random Effect | Egger’s | Trim and Fill Test | ||
|---|---|---|---|---|---|---|---|
| of | [95% CI] | [p-Value] | [95% CI] | Test | * Meta-Regression Test [p-Value] | ||
| Subsets | [p-Value] | ||||||
| Overall patients | 24 | 0.730 (0.694, 0.762] | <0.001 | 0.861 (0.766, 0.922] | 0.01 | 0.884 (0.779, 0.943] | |
| America | 12 | 0.602 (0.532, 0.669] | <0.001 | 0.896 (0.693, 0.970] | <0.001 | 0.862 (0.629, 0.958] | |
| Asia | 6 | 0.845 (0.799, 0.882] | 0.335 | 0.852 (0.798, 0.893] | 0.102 | - | 0.948 |
| Europe | 6 | 0.728 (0.667, 0.782] | <0.001 | 0.777 (0.597, 0.891] | 0.526 | - | 0.448 |
| 1–4 detector row | 10 | 0.707 (0.650, 0.758] | <0.001 | 0.793 (0.616, 0.901] | 0.345 | - | |
| America | 6 | 0.715 (0.600, 0.807] | <0.001 | 0.881 (0.514, 0.981] | 0.052 | - | |
| Europe | 4 | 0.704 (0.638, 0.763] | <0.001 | 0.672 (0.475, 0.823] | 0.648 | - | 0.227 |
| 16–64 detector row | 10 | 0.693 (0.620, 0.759] | <0.001 | 0.897 (0.702, 0.970] | <0.001 | 0.933 (0.682, 0.989] | |
| America | 4 | 0..455 (0.348, 0.567] | <0.001 | 0.904 (0.360, 0.994] | 0.047 | 0.904 (0.360, 0.994] | |
| Asia | 4 | 0.860 (0.784, 0.913] | 0.785 | 0.860 (0.784, 0.913] | 0.799 | - | 0.886 |
| Europe | 2 | 0.942 (0.834, 0.982] | 0.061 | 0.954 (0.674, 0.995] | - | - | 0.563 |
| CE positive patients | 12 | 0.566 (0.499, 0.632] | <0.001 | 0.723 (0.533, 0.856] | 0.003 | 0.655 (0.470. 0.802] | |
| 1–4 detector row | 5 | 0.600 (0.465, 0.720] | 0.01 | 0.683 (0.427, 0.861] | 0.079 | - | |
| 16-64 detector row | 5 | 0.544 (0.559, 0.636] | <0.001 | 0.729 (0.355, 0.929] | 0.057 | - | |
| CE negative patients | 12 | 0.814 (0.714, 0.845] | <0.001 | 0.937 (0.859, 0.974] | 0.016 | 0.867 (0.726, 0.941] | |
| 1–4 detector row | 5 | 0.736 (0.674, 0.789] | <0.001 | 0.867 (0.634, 0.961] | 0.343 | - | |
| 16–64 detector row | 5 | 0.934 (0.882, 0.964] | <0.001 | 0.968 (0.855, 0.994] | 0.052 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moon, S.N.; Pyo, J.-S.; Kang, W.S. Accuracy of Contrast Extravasation on Computed Tomography for Diagnosing Severe Pelvic Hemorrhage in Pelvic Trauma Patients: A Meta-Analysis. Medicina 2021, 57, 63. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010063
Moon SN, Pyo J-S, Kang WS. Accuracy of Contrast Extravasation on Computed Tomography for Diagnosing Severe Pelvic Hemorrhage in Pelvic Trauma Patients: A Meta-Analysis. Medicina. 2021; 57(1):63. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010063
Chicago/Turabian StyleMoon, Sung Nam, Jung-Soo Pyo, and Wu Seong Kang. 2021. "Accuracy of Contrast Extravasation on Computed Tomography for Diagnosing Severe Pelvic Hemorrhage in Pelvic Trauma Patients: A Meta-Analysis" Medicina 57, no. 1: 63. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57010063