
The Role of Exercise to Reduce the Impact of Diabetes in the Seminal Quality: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Risk of Bias
2.3. Data Extraction
3. Results
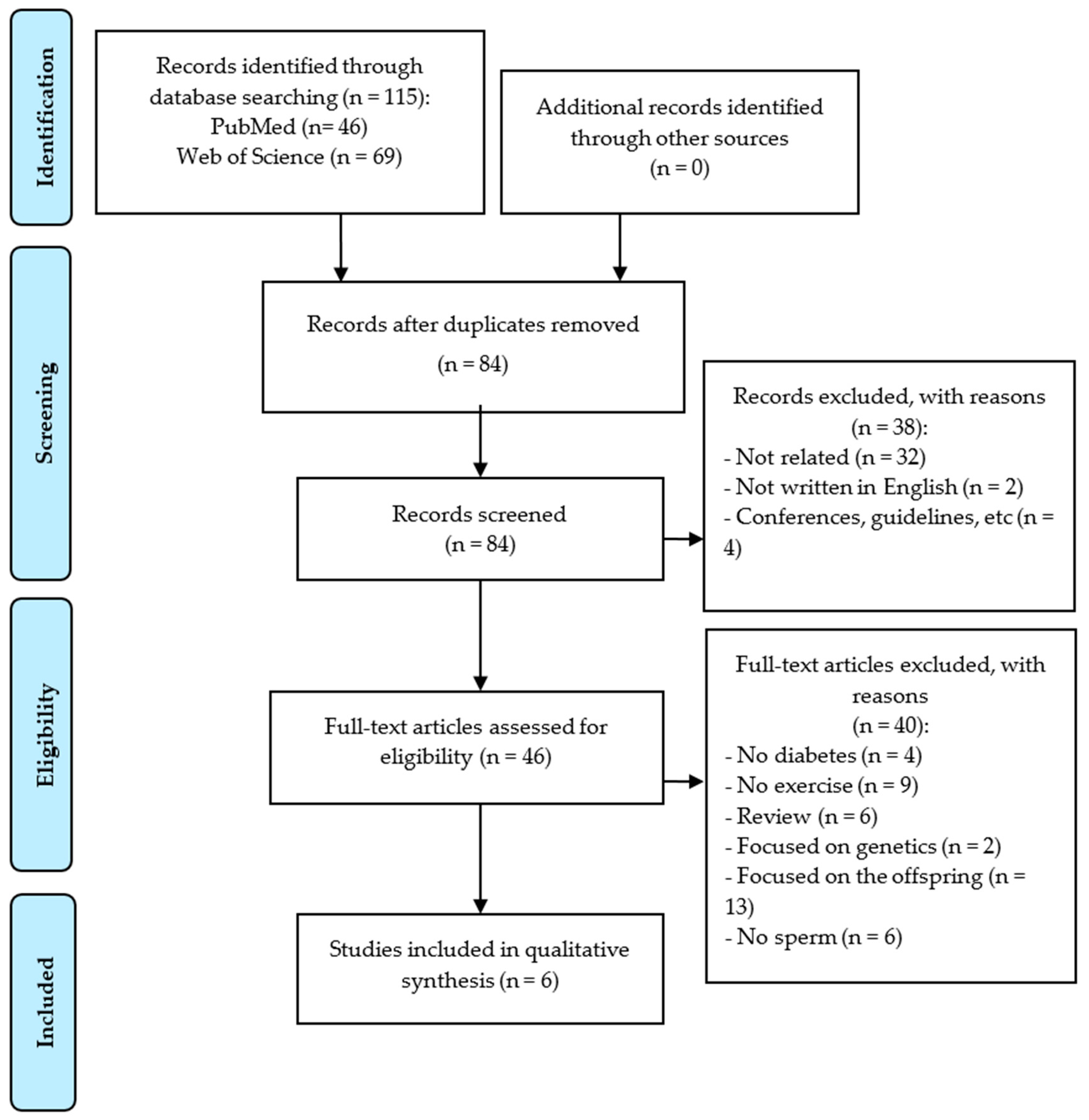
3.1. Study Selection
3.2. Risk of Bias

{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Participant Representativeness | Equivalence of Comparison Groups | Total Score | |||||
|---|---|---|---|---|---|---|---|---|---|
| Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | ||
| Humans | |||||||||
| Rosety Rodríguez 2014 [19] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | 7/8 |
| Murray 1988 [18] | Yes | No | Yes | No | No | Yes | No | No | 3/8 |
| Rats | |||||||||
| Samadian 2019a [16] | No | Yes | No | No | Yes | Yes | N/A | N/A | 3/6 |
| Samadian 2019b [17] | No | Yes | No | No | Yes | Yes | N/A | N/A | 3/6 |
| Parastesh 2019a [20] | Yes | Yes | No | No | Yes | Yes | Yes | N/A | 5/7 |
| Parastesh 2019b [21] | Yes | Yes | No | No | Yes | Yes | Yes | N/A | 5/7 |
3.3. Study Characteristics
3.4. Interventions and Comparison Groups
3.5. Outcome Measures
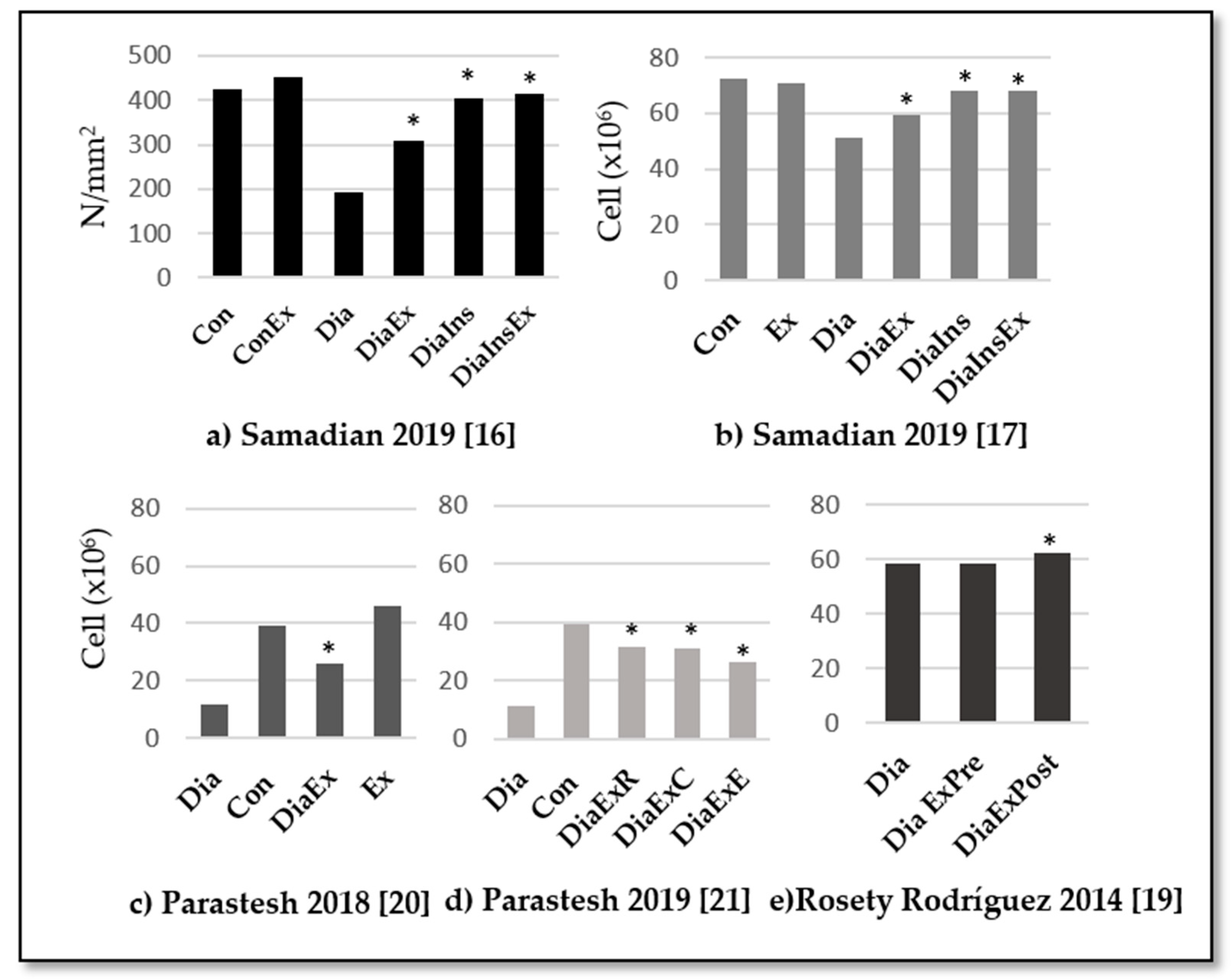
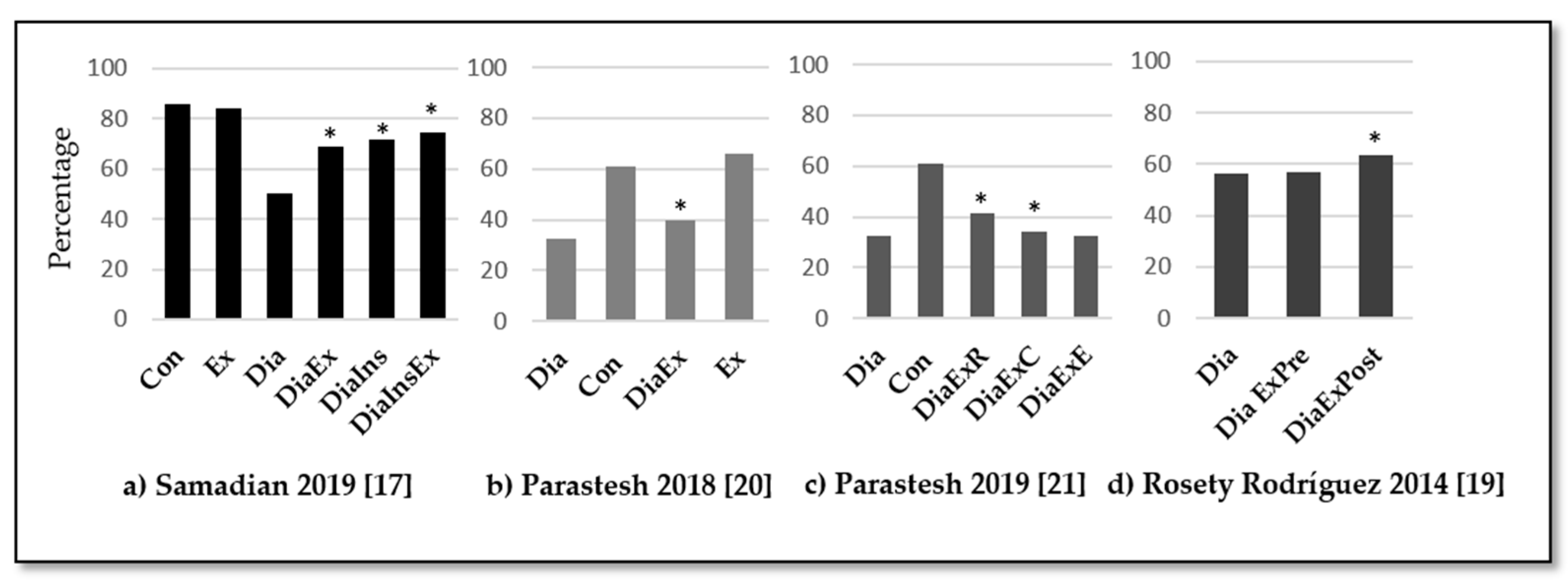
3.5.1. Sperm Count and Motility
3.5.2. Sperm Morphology
3.5.3. Other Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Study | Variable | Measurement Procedure | Results |
|---|---|---|---|
| Samadian 2019 [16] | Total cell number in 1 mm2 of testicular tissue and relative ratios | Immunohistochemical staining (IHC) and light microscope (Olympus-CH-2, Japan) | Con, Ex, diaIn, diaEx and diaInEx > Dia |
| Caspase-3 + cell percentage to total cell number in one mm2 of testicular tissue | Immunohistochemical staining (IHC) and light microscope (olympus-ch-2, Japan) | Con and Ex < diaIn and diaExIn < diaEx< Dia | |
| Bax + cell percentage to Bcl-2 + cells in one mm2 of testicular tissue | Immunohistochemical staining (IHC) and light microscope (Olympus-CH-2, Japan) | Con and Ex < diaInEx < diaIn and diaEx < Dia | |
| Negative Tubular Differentiation (TDI) and Spermiogenesis Indices (SPI) | Tissue fixation and staining with hematoxylin and eosin. Tubules containing less than three layers of germinal cells and those with impaired spermiogenesis are negative TDI and SPI, respectively. | TDI: Con, Ex, diaIn and diaInEx < diaEx < Dia SPI: Con, Ex, diaIn and diaInEx < diaEx < Dia | |
| Relative intensity of Bcl-2/GAPDH | RT-PCR. Mrna isolation, account determined by nanodrop spectrophotometer. Cdna sintetized by Protocol of Fermentas, gmbh, Germany. Rt-PCR by protocol Primers manufactured by Cinna-Gen Co. Final products analysis using PCR Gel software. | Con, Ex, diaIn and diaInEx > diaEx and Dia | |
| Mean percentages of Bcl-2 + cells | Immunohistochemical staining protocol. Bcl-2 antibody Abcam, catno:ab59348 1:300 was used. Positive IHC reactions were marked as brown stains under a light microscope. The percentage of reacted cells in five microscopic fields was evaluated. | Con, Ex, diaIn and diaInEx > diaEx > Dia | |
| Relative intensity of Bcl-2 protein/β-Actin | Western blot analyses. Protein evaluation by Lowry method. Bcl-2 antibody Abcam, catno:ab59348 1:300. Blots were visualized using an Enhanced Chemiluminescence Kit (ECL, Thermo scientific) and protein were analyzed using Arash Teb Pishro (ATP) enhanced laser densitometer. | Con, Ex, diaIn and diaInEx > diaEx and Dia | |
| Relative intensity of Bax/GAPDH | RT-PCR. Mrna isolation, account determined by nanodrop spectrophotometer. Cdna sintetized by Protocol of Fermentas, gmbh, Germany. Rt-PCR Primers designed and manufactured by Cinna-Gen Co. Final products analysis using PCR Gel analyzing software (ATP, Tehran, Iran). | Con and Ex < diaIn, diaEx and diaInEx < Dia | |
| Mean percentages of Bax + cells | Immunohistochemical staining protocol antibody Bax (Abcam, Cat NO: ab53154,1:500) was used. Positive IHC reactions were marked as brown stains under a light microscope. The percentage of reacted cells in five microscopic fields was evaluated. | Con, Ex and diaInEx < diaIn < diaEx < Dia | |
| Relative intensity of Bax protein/β-Actin | Western blot analyses. Protein evaluation by Lowry method. Antibody Bax (Abcam, Cat NO: ab53154,1:500). Blots were visualized using an Enhanced Chemiluminescence Kit (ECL, Thermo scientific) and protein were analyzed using Arash Teb Pishro (ATP) enhanced laser densitometer. | Con, Ex, diaIn, diaEx and diaInEx < Dia | |
| Relative intensity of Caspase-3/GAPDH | RT-PCR. Mrna isolation, account determined by nanodrop spectrophotometer. Cdna sintetized by Protocol of Fermentas, gmbh, Germany. Rt-PCR Primers designed and manufactured by Cinna-Gen Co. Final products analysis using PCR Gel analyzing software (ATP, Tehran, Iran). | Con, Ex < diaIn and diaInEx < diaEx and Dia | |
| Mean percentages of Caspase-3 + cells | Immunohistochemical staining protocol. Antibody Caspase-3 (Abcam, Cat NO: ab4051, 1:300) was used. Positive IHC reactions were marked as brown stains under a light microscope. The percentage of reacted cells in five microscopic fields was evaluated. | Con and Ex < diaIn and diaInEx < diaEx and Dia | |
| Relative intensity of Caspase-3 protein/β-Actin | Western blot analyses. Protein evaluation by Lowry method. Antibody Caspase-3 (Abcam, Cat NO: ab4051, 1:300). Blots were visualized using an Enhanced Chemiluminescence Kit (ECL, Thermo scientific) and proteins were analyzed using Arash Teb Pishro (ATP) enhanced laser densitometer. | Con and Ex <diaIn and diaInEx < diaEx and Dia | |
| Samadian 2019 [17] | Testicular weight relative to total body weight | Measure testicular weight relative to total body weight | Con, Ex, diaIn, diaInEx > diaEx, Dia |
| Serum level of insulin (ng/mL) 3 | Evaluated using special commercial ELISA kits. Insulin (Ray Biotechnology, Cat No: ELR-Insulin) | Con, Ex, diaIn, diaInEx > diaEx > Dia | |
| Negative Tubular Differentiation (TDI) and Spermiogenesis Indices (SPI) | Tissue fixation and staining with hematoxylin and eosin. Analized using a light microscope Olympus-CH-2, Japan. Tubules containing less than three layers of germinal cells and those with impaired spermiogenesis are negative TDI and SPI, respectively. | TDI: Con, Ex, diaIn, diaInEx < diaEx < Dia SPI: Con Ex, diaIn, diaInEx < diaEx < Dia | |
| Leydig Cell distribution | Evaluated by TUNEL (terminal deoxynucleotidyl transferase enzyme-mediated dutp nick end labeling) staining kit (In situ cell death detection kit, POD, Roche; Cat, Germany). | Con, Ex, diaIn, diaInEx, diaEx > Dia | |
| Leydig cell apoptosis | Evaluated by tunel (terminal deoxynucleotidyl transferase enzyme-mediated dutp nick end labeling) staining kit (in situ cell death detection kit, POD, roche; cat, Germany). | Con, Ex < diaIn, diaInEx < diaEx | |
| Testosterone level | Evaluated using special commercial ELISA kits special kit for rat testosterone (cat no: csb-e05100r). | Con, Ex, diaIn, diaInEx >diaEx >dia | |
| Testicular Antioxidants level: TAC (total antioxidant activity), SOD, and GPX | Commercial kits: superoxide dismutase (SOD, Zellbio, gmbh, Cat No: ZB-SOD-96A) Glutathione peroxidase (GPX, Zellbio, gmbh, Cat No: ZB-GPX-A96) from Elim-Teb Co. The commercial kit for assessment of tissue total antioxidant capacity (TAC, Cat No: ATAK-105112) was from AYANDEH lab. Co. | TAC: Con, Ex >diaIn, diaInEx > diaEx > Dia SOD: Con, Ex, diaIn, diaInEx > diaEx > Dia GPX: Com, Ex, diaIn, diaInEx > diaEx > Dia | |
| Intracellular storage of carbohydrates in germinal cell | Periodic acid Schiff (PAS) staining was conducted. The PAS+ cell numbers/mm 2 of tissue were counted and compared between groups. | Con, Ex, diaIn, diaInEx > diaEx > Dia | |
| Parastesh 2019 [20] | Hormonal levels LH | Blood samples were collected by cardiac puncture (5 cc) and centrifuged at 3500 rpm for 10 min and the serum samples were stored at −70 °C (all hormonal analysis). Commercial Kit LH detection (Rat ELISA Kit, Eastbiopharm Cat. No Ck-E90904, China, sensitivity: 0.11 miu/L, Assay range: 0.2–60 miu/L) | Dia (3.9 ± 0.7) < Con (5.6 ± 2.8) Ex (9.8 ± 1.6) > Con, Dia and diaEx (4.7 ± 1) |
| Hormonal levels FSH | Commercial Kit FSH (Rat ELISA Kit, Eastbiopharm Cat. No Ck-E30597, China, sensitivity: 0.12 miu/L, Assay range: 0.2–60 miu/L) | Con: 4.4 ± 1 Dia: 3.5 ± 1.1 DiaEx: 5.9 ± 5 Ex: 4.3 ± 1 | |
| Hormonal levels Testosterone | Commercial Kit Testosterone detection (Rat ELISA Kit, Eastbiopharm Cat. No Ck- E90243, China, sensitivity: 0.25 nmol/L, Assay range: 0.5–100 nmol/L) | Dia (4.6 ± 1.6) < Con (6.6 ± 1.8) Ex (7.9 ± 1.7) > Dia and diaEx (5.7 ± 2.3) | |
| Hormonal levels Adiponectina | Commercial Kit Adiponectin detection (Rat ELISA Kit, Eastbiopharm Cat. No Ck-E30584, China, sensitivity: 0.16 mg/L, Assay range: 0.2–60 mg/L) | Dia (1.6 ± 0.6) and diaEx (3.8 ± 1.1) < Con (5.6 ± 2.2) DiaEx > diaEx (5.3 ± 0.7) > Dia and diaEx | |
| Parastesh 2019 [21] | Hormonal levels LH | Blood samples were collected by cardiac puncture (5 cc) and centrifuged at 3500 rpm for 10 min and the serum samples were stored at −70 °C (all hormonal analysis). Commercial Kit LH detection (Rat ELISA Kit, Eastbiopharm Cat. No Ck-E90904, China, sensitivity: 0.11 miu/L, Assay range: 0.2–60 miu/L) | Dia (3.3 ± 0.4)< Con (5.6 ± 1.6), diaExE (6.7 ± 1.9), diaExR (6.3 ± 1.6) and diaExC (6.3 ± 1.8) > Dia |
| Hormonal levels FSH | Commercial Kit FSH (Rat ELISA Kit, Eastbiopharm Cat. No Ck- E30597, China, sensitivity: 0.12 miu/L, Assay range: 0.2–60 miu/L) | Con: 4.1 ± 1.5 DiaExE: 5.8 ± 4.01 DiaExR: 4.4 ± 0.75 DiaExC: 5 ± 4.27 DiaExE (5.8 ± 4.01) > Dia (2.7 ± 0.33) | |
| Hormonal levels Testosterone | Commercial Kit Testosterone detection (Rat ELISA Kit, Eastbiopharm Cat. No Ck- E90243, China, sensitivity: 0.25 nmol/L, Assay range: 0.5–100 nmol/L | Dia (3.3 ± 0.2) < Con (4.5 ± 0.9), diaExE (4.8 ± 0.9), diaExR (5.2 ± 1.5) and diaExC (5 ± 1.8) > Dia | |
| Rosety-Rodríguez 2014 [19] | TAC (Total Antioxidant capacity) | Seminal plasma was obtained after centrifugation at 3500 rpm for 15 min and it was loaded in the eppendorf tubes (3 mL) and stored at −80 °C until analysis. Colorimetric method using randox commercial kits on the Hitachi 902 autoanalyzer. | DiaEx (pre) (1.41 ± 0.53) < diaEx (post) (1.89 ± 0.46) (p < 0.05) > dia (post) (1.36 ± 0.60) (p < 0.05) Dia (pre): 1.32 ± 0.58 Within and between group increase in the diabetic exercise group. |
| GPX | Seminal plasma was obtained after centrifugation at 3500 rpm for 15 min and it was loaded in the eppendorf tubes (3 mL) and stored at −80 °C until analysis. Subsequent oxidation of NADPH at 240 nm with t-butyl-hydro-peroxide as a substrate. GPX units (u/g protein) were defined as mol NADPH oxidized/g protein. | DiaEx (pre) (4.77 ± 1.66) < diaEx (post) (6.23 ± 1.50) (p < 0.05) > dia (post) (4.61 ± 1.55) (p < 0.05) Dia (pre): 4.58 ± 1.49 Within and between group increase in the diabetic exercise group. | |
| Murray 1988 [18] | Serum LH | Determined on unextracted urine at pH 7.0 Radioimmunoassays during exercise were performed using the WHO 2nd IRP-HMG reference preparation obtained from Diagnostic Products Corp. (Los Angeles, CA) as Standard. | Dia< Con at rest. It remains lower in Dia during exercise but not in recovery. |
| Serum FSH | Radioimmunoassays during exercise were performed using the WHO 2nd IRP-HMG reference preparation obtained from Diagnostic Products Corp. (Los Angeles, CA) as Standard. | Dia < Con at rest, exercise, and recovery. No changes observed during exercise. | |
| Total testosterone | Established radioimmunoassays. | Dia: Significant increment during exercise and reduction to basal levels in the recovery. |
References
- Cho, N.; Shaw, J.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.; Ohlrogge, A.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forouhi, N.G.; Wareham, N.J. Epidemiology of diabetes. Medicine 2010, 38, 602–606. [Google Scholar] [CrossRef]
- Bener, A.; Al-Ansari, A.A.; Zirie, M.; Al-Hamaq, A.O. Is male fertility associated with type 2 diabetes mellitus? Int. Urol. Nephrol. 2009, 41, 777–784. [Google Scholar] [CrossRef]
- De Jonge, C.; Barratt, C.L.R. The present crisis in male reproductive health: An urgent need for a political, social, and research roadmap. Andrology 2019, 7, 762–768. [Google Scholar] [CrossRef]
- Singh, S.; Malini, T.; Rengarajan, S.; Balasubramanian, K. Impact of experimental diabetes and insulin replacement on epididymal secretory products and sperm maturation in albino rats. J. Cell. Biochem. 2009, 108, 1094–1101. [Google Scholar] [CrossRef]
- Shi, G.J.; Zheng, J.; Wu, J.; Qiao, H.Q.; Chang, Q.; Niu, Y.; Sun, T.; Li, Y.X.; Yu, J.Q. Beneficial effects of Lycium barbarum polysaccharide on spermatogenesis by improving antioxidant activity and inhibiting apoptosis in streptozotocin-induced diabetic male mice. Food Funct. 2017, 8, 1215–1226. [Google Scholar] [CrossRef]
- Condorelli, R.A.; La Vignera, S.; Mongioì, L.M.; Alamo, A.; Calogero, A.E. Diabetes Mellitus and Infertility: Different Pathophysiological Effects in Type 1 and Type 2 on Sperm Function. Front. Endocrinol. 2018, 9, 268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aune, D.; Norat, T.; Leitzmann, M.; Tonstad, S.; Vatten, L.J. Physical activity and the risk of type 2 diabetes: A systematic review and dose-response meta-analysis. Eur. J. Epidemiol. 2015, 30, 529–542. [Google Scholar] [CrossRef]
- Rosety, M.; Díaz, A.J.; Rosety, J.M.; Pery, M.T.; Brenes-Martín, F.; Bernardi, M.; García, N.; Rosety-Rodríguez, M.; Ordoñez, F.J.; Rosety, I. Exercise improved semen quality and reproductive hormone levels in sedentary obese adults. Nutr. Hosp. 2017, 34, 603–607. [Google Scholar] [CrossRef]
- Hajizadeh Maleki, B.; Tartibian, B.; Chehrazi, M. Effects of Aerobic, Resistance, and Combined Exercise on Markers of Male Reproduction in Healthy Human Subjects: A Randomized Controlled Trial. J. strength Cond. Res. 2019, 33, 1130–1145. [Google Scholar] [CrossRef] [PubMed]
- Matos, B.; Howl, J.; Ferreira, R.; Fardilha, M. Exploring the effect of exercise training on testicular function. Eur. J. Appl. Physiol. 2019, 119, 1–8. [Google Scholar] [CrossRef]
- Santos, M.; Rodríguez-González, G.L.; Ibáñez, C.; Vega, C.C.; Nathanielsz, P.W.; Zambrano, E. Adult exercise effects on oxidative stress and reproductive programming in male offspring of obese rats. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 308, R219–R225. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, C.E.; Fonner, V.A.; Armstrong, K.A.; Denison, J.A.; Yeh, P.T.; O’Reilly, K.R.; Sweat, M.D. The Evidence Project risk of bias tool: Assessing study rigor for both randomized and non-randomized intervention studies. Syst. Rev. 2019, 8, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Samadian, Z.; Azar, J.T.; Moshari, S.; Razi, M.; Tofighi, A. Moderate-intensity exercise training in sole and simultaneous forms with insulin ameliorates the experimental type 1 diabetes-induced intrinsic apoptosis in testicular tissue. Int. J. Sports Med. 2019, 40, 909–920. [Google Scholar] [CrossRef]
- Samadian, Z.; Tofighi, A.; Razi, M.; Tolouei Azar, J.; Ghaderi Pakdel, F. Moderate-intensity exercise training ameliorates the diabetes-suppressed spermatogenesis and improves sperm parameters: Insole and simultaneous with insulin. Andrologia 2019, 51, e13457. [Google Scholar] [CrossRef] [PubMed]
- Murray, F.T.; Cameron, D.F.; Vogel, R.B.; Thomas, R.G.; Wyss, H.U.; Zauner, C.W. The pituitary-testicular axis at rest and during moderate exercise in males with diabetes mellitus and normal sexual function. J. Androl. 1988, 9, 197–206. [Google Scholar] [CrossRef]
- Rosety-Rodriguez, M.; Rosety, J.; Fornieles, G.; Rosety, M.; Diaz, A.; Rosety, I.; Rodríguez-Pareja, A.; Rosety, M.; Ordonez, F.; Elosegui, S. Home-based treadmill training improved seminal quality in adults with type 2 diabetes. Actas Urológicas Españolas (Engl. Ed.) 2014, 38, 589–593. [Google Scholar] [CrossRef]
- Parastesh, M.; Saremi, A.; Ahmadi, A.; Kaviani, M. The effect of aerobic training on serum levels of adiponectin, hypothalamic-pituitary-gonadal axis and sperm quality in diabetic rats. Urol. J. 2019, 16, 592–597. [Google Scholar]
- Parastesh, M.; Heidarianpour, A.; Sadegh, M. Investigating the effects of endurance, resistance and combined training on reproductive hormones and sperm parameters of streptozotocin–nicotinamide diabetic male rats. J. Diabetes Metab. Disord. 2019, 18, 273–279. [Google Scholar] [CrossRef]
- Minas, A.; Najafi, G.; Jalali, A.S.; Razi, M. Fennel induces cytotoxic effects against testicular germ cells in mice; evidences for suppressed pre-implantation embryo development. Environ. Toxicol. 2018, 33, 841–850. [Google Scholar] [CrossRef]
- Examination and Processing of Human Semen. Available online: https://www.who.int/docs/default-source/reproductive-health/infertility/examination-and-processing-of-human-semen-5ed-eng.pdf?sfvrsn=5227886e_2 (accessed on 27 September 2020).
- Pergialiotis, V.; Prodromidou, A.; Frountzas, M.; Korou, L.M.; Vlachos, G.D.; Perrea, D. Diabetes mellitus and functional sperm characteristics: A meta-analysis of observational studies. J. Diabetes Its Complicat. 2016, 30, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Leisegang, K.; Sengupta, P.; Agarwal, A.; Henkel, R. Obesity and male infertility: Mechanisms and management. Andrologia 2020, e13617. [Google Scholar] [CrossRef]
- Bieniek, J.M.; Kashanian, J.A.; Deibert, C.M.; Grober, E.D.; Lo, K.C.; Brannigan, R.E.; Sandlow, J.I.; Jarvi, K.A. Influence of increasing body mass index on semen and reproductive hormonal parameters in a multi-institutional cohort of subfertile men. Fertil. Steril. 2016, 106, 1070–1075. [Google Scholar] [CrossRef] [Green Version]
- Ibañez-Perez, J.; Santos-Zorrozua, B.; Lopez-Lopez, E.; Matorras, R.; Garcia-Orad, A. An update on the implication of physical activity on semen quality: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2019, 299, 901–921. [Google Scholar] [CrossRef] [PubMed]
- Jóźków, P.; Rossato, M. The Impact of Intense Exercise on Semen Quality. Am. J. Men’s Health 2017, 11, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Maleki, B.H.; Tartibian, B. High-Intensity Exercise Training for Improving Reproductive Function in Infertile Patients: A Randomized Controlled Trial. J. Obstet. Gynaecol. Can. 2017, 39, 545–558. [Google Scholar] [CrossRef]
- Zhao, H.; Xu, S.; Wang, Z.; Li, Y.; Guo, W.; Lin, C.; Gong, S.; Li, C.; Wang, G.; Cai, L. Repetitive exposures to low-dose X-rays attenuate testicular apoptotic cell death in streptozotocin-induced diabetes rats. Toxicol. Lett. 2010, 192, 356–364. [Google Scholar] [CrossRef]



| Study | Study Design | Group: Sample Size | Age | Weight/Body Composition |
|---|---|---|---|---|
| Samadian 2019a [16] | Controlled trial | Sedentary Con: n = 6 Sedentary Dia: n = 6 Sedentary DiaIn: n = 6 Ex: n = 6 DiaEx: n = 6 DiaInEx: n = 6 | Two-month-old male Wistar rats | 180–220 g |
| Samadian 2019b [17] | Controlled trial | Sedentary Con: n = 6 Dia: n = 6 DiaIn: n = 6 Ex: n = 6 DiaEx: n = 6 DiaInEx: n = 6 | Two-month-old male Wistar rats | 180–220 g |
| Parastesh 2019a [20] | Controlled trial | Con: n = 12 Dia: n = 12 DiaIn: n = 12 Ex: n = 12 DiaEx: n = 12 DiaInEx: n = 12 | 8-wk old Sprague Dawley rats | 200–250 g |
| Parastesh 2019b [21] | Controlled trial | Con: n = 12 Dia: n = 12 DiaExE: n = 12 DiaExR: n = 12 DiaExC: n = 12 | 8-wk old Sprague Dawley rats | 200–250 g |
| Rosety Rodríguez 2014 [19] | Randomized controlled trial | Dia. n = 30 DiaEx: n = 30 | Dia: 35.7 ± 4.0 years DiaEx: 36.2 ± 3.5 years | Dia: 29.7 ± 2.6% Fat mass DiaEx: 30.3 ± 2.8% Fat mass |
| Murray 1988 [18] | Controlled trial | Ex: n = 10 DiaInEx: n = 8 | Ex: 26 ± 1.7 years DiaInEx: 23 ± 0.8 years | Ex: 22.4 ± 1.24 body mass index DiaInEx: 23.2 ± 1.50 body mass index |
| Study | Group | Intervention Duration | Frequency | Session Duration | Description | Progression | Additional Information |
|---|---|---|---|---|---|---|---|
| Samadian 2019 [16] | Con | 6 weeks | None | None | None | None | |
| Dia | None | None | None | None | |||
| DiaIn | None | None | None | None | Insulin: 0.9 IU.100/g once a day for 6 weeks | ||
| Ex | 5 days/wk | 25 min (mean) | 5 min warm-up and cool-down Running at 18 m/min at 5% of inclination and 65% VO2max from 9 to 18 min | Speed: from 9 m/min to 18 m/min Duration: from 15 min to 30 min | |||
| DiaEx | |||||||
| DiaInEx | Insulin: 0.9 IU.100 g−1 once a day for 6 weeks | ||||||
| Samadian 2019 [17] | Con | 6 weeks | None | None | None | None | |
| Dia | None | None | None | None | |||
| DiaIn | None | None | None | None | Insulin: 0.9 IU.100 g−1 once a day for 6 weeks | ||
| Ex | 5 days/wk | 25 min (mean) | 5 min warm-up and cool-down Running at 18 m/min at 5% of inclination and 65% VO2max from 9 to 18 min | Speed: from 9 m/min to 18 m/min Duration: from 15 min to 30 min | |||
| DiaEx | |||||||
| DiaInEx | Insulin: 0.9 IU.100 g−1 once a day for 6 weeks | ||||||
| Parastesh 2019 [20] | Con | 10 weeks | None | None | None | None | |
| Dia | None | None | None | None | |||
| Ex | 6 days/wk | 52.1 min (mean) | 5 min warm-up and cool-down (16 m/min) Running at 27 m/min and 0º inclination | Adaptation wk: walking 8 m/min Duration from 1st wk to 4th wk (2 min/session) until 60 min and maintain | |||
| DiaEx | |||||||
| Parastesh 2019 [21] | Con | 10 weeks | None | None | None | None | |
| Dia | None | None | None | None | |||
| DiaExE | 5 days/wk | 52.1 min (mean) | 5 min warm-up and cool-down (16 m/min) Running at 27 m/min and 0º inclination | Adaptation wk: walking 8 m/min Duration from 1st wk to 4th wk (2 min/session) until 60 min and maintain | |||
| DiaExR | 5 days/wk | Not reported | 1 m climbing a long ladder at 90º with a weight in animals’ tails 3 sets (2 min rest between) of 4 repetitions (10 s rest between) | Adaptation 1st wk Weight: 30% animal weight in 2nd wk and increase until 200% in 10th wk | |||
| DiaExC | 5 days/wk | Alternatively: DiaExE protocol and DiaExR | |||||
| Rosety Rodríguez 2014 [19] | Dia | 14 weeks | None | None | None | None | |
| DiaEx | 3 days/wk | ~60 min | 10–15 min warm-up 40 min treadmill at an intensity 55–70% HRpeak 5–10 min cool-down | Intensity: 2.5% HRpeak/2 wks | |||
| Murray 1988 [18] | Ex | Acute session | 45 min | Cycling at 50% VO2max | Workload: automatically readjust during the test. | ||
| DiaInEx | Diabetic: 5 units of NPH intermediate-acting insulin subcutaneously in the left hip 30 min before exercise | ||||||
| Study | Variable | Measurement Procedure | Results |
|---|---|---|---|
| Samadian 2019 [16] | Cell count | Analyses by light microscopic | Figure 2 |
| Apoptosis index | Evaluated by TUNEL (Terminal deoxynucleotidyl transferase enzyme-mediated dUTP nick end labeling) staining kit (In situ cell death detection kit, POD, Roche; Cat, Germany). | (Con = Ex = DiaIn = DiaInEx) < DiaEx < Dia | |
| Samadian 2019 [17] | Quality Sperm: Count | Incubation of tissues in heat transfer fluid (HTF) medium, 45 min at 37 °C in 5% CO2. Dilution of 1:50 and observation with light microscope stereo zoom microscope. Count based on standard Neobar slide method. | Figure 2 |
| Quality Sperm: Motility | Incubation of tissues in HTF medium, 45 min at 37 °C in 5% CO2. Dilution of 1:50 50 and observation with light microscope stereo zoom microscope. | Figure 3 | |
| Quality Sperm: Impaired chromatin condensation | Aniline blue staining. The spermatozoa with unstained nuclei were considered as mature (representing protamine content), while the spermatozoa with stained nuclei (representing histone content) were marked as immature [22]. | (Con = Ex) < (DiaIn = DiaInEx = DiaEx) < Dia | |
| Quality Sperm: DNA Fragmentation | Acridine orange Staining and evaluation by fluorescence microscope (Zeiss Company). Spermatozoa with green DNA content were marked as spermatozoa with double-stranded DNA, while the spermatozoa with yellowish and/or reddish fluorescent DNA content were considered as spermatozoa with DNA fragmentation. | (Con = Ex) < (DiaIn = DiaInEx = DiaEx) < Dia | |
| Parastesh 2019 [20] | Sperm count (106) | Dissected epididymis was transferred into a 5 cc (DMEM) medium. Sperm swim out into the medium. One mL of the solution was diluted with 9 mL formaldehyde fixative. Neubauer chamber and manually counted under a microscope. | Figure 2 |
| Sperm viability | Eosin-nigrosine staining was used to evaluate sperm viability according to WHO protocol [23]. | Ex (87.8 ± 2.9%) > Con (77.5 ± 4.6%) > DiaEx (41.7 ± 7.2%) > Dia (29.7 ± 16.2%) | |
| Sperm morphology | Papanicolaou stain according to WHO protocol [23]. | Día (85.2 ± 7.5) < Con (95.4 ± 1.3); Ex (90.4 ± 9.1) > (Dia (85.2 ± 7.5) = DiaEx (88 ± 8.8)) | |
| Sperm motility | WHO protocol [23]. Ten µl of the sperm suspension was located on a microscope slide. | Figure 3 | |
| Parastesh 2019 [21] | Sperm count (106) | Dissected epididymis was transferred into a 5 cc (DMEM) medium. Sperm swim out into the medium. 1 mL of the solution was diluted with 9 mL formaldehyde fixative. Neubauer chamber and manually counted under a microscope. | Figure 2 |
| Sperm viability | Eosin-nigrosine staining was used to evaluate sperm viability according to WHO protocol [23]. | (Dia (29.7 ± 16.2) = DiaExE (41.7 ± 7.2)) < Con (77.5 ± 4.6); DiaExR (60.6 ± 8) and DiaExC (60.6 ± 8) > Dia (29.7 ± 16.2) | |
| Sperm morphology | Papanicolaou stain according to WHO protocol [23]. | Dia (85.2 ± 7.5) < Con (95.4 ± 1.3); DiaExE (88 ± 8.8) = DiaExR (89.1 ± 6.9) = DiaExC (93.4 ± 2.7) | |
| Sperm motility | WHO protocol [23]. Ten µl of the sperm suspension was located on a microscope slide and covered. | Figure 3 | |
| Rosety Rodríguez 2014 [19] | Volume | Semen was collected after 3 days of sexual abstinence (intercourse or masturbation) by manual masturbation into a sterile container on-site and examined within 30 min of ejaculation [23]. | Dia (pre, 2.90 ± 0.86) = Dia (post, 2.92 ± 0.90); DiaEx (pre, 2.92 ± 0.90 = DiaEx (post, 3.08 ± 0.86) |
| Concentration | Hemacytometer (HauserScientific Inc., Horsham, PA, USA) | Figure 2 | |
| Motility | Computer-aided semen analysis (CASA system, Microptic S.L., Spain) | Figure 3 | |
| Morphology | Hemacytometer (Hauser Scientific Inc., Horsham, PA, USA) and Computer-aided semen analysis (CASA system, MicropticS.L., Spain) | DiaEx (pre, 46.1 ± 4.6) < DiaEx (post, 51.2 ± 5.0) DiaEx (post, 51.2 ± 5.0) > Dia (post, 45.9 ± 4.8) | |
| Murray 1988 [18] | Evaluation of sperm quality before exercise | One single measure comparing diabetic and healthy young males:
| |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lavín-Pérez, A.M.; Collado-Mateo, D.; Villafaina, S.; Calle-Guisado, V. The Role of Exercise to Reduce the Impact of Diabetes in the Seminal Quality: A Systematic Review. Medicina 2021, 57, 159. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57020159
Lavín-Pérez AM, Collado-Mateo D, Villafaina S, Calle-Guisado V. The Role of Exercise to Reduce the Impact of Diabetes in the Seminal Quality: A Systematic Review. Medicina. 2021; 57(2):159. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57020159
Chicago/Turabian StyleLavín-Pérez, Ana Myriam, Daniel Collado-Mateo, Santos Villafaina, and Violeta Calle-Guisado. 2021. "The Role of Exercise to Reduce the Impact of Diabetes in the Seminal Quality: A Systematic Review" Medicina 57, no. 2: 159. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57020159