
Superior Capsular Reconstruction of the Shoulder Using the Long Head of the Biceps Tendon: A Systematic Review of Surgical Techniques and Clinical Outcomes

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Study Selection and Data Collection
2.4. Quality Assessment
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
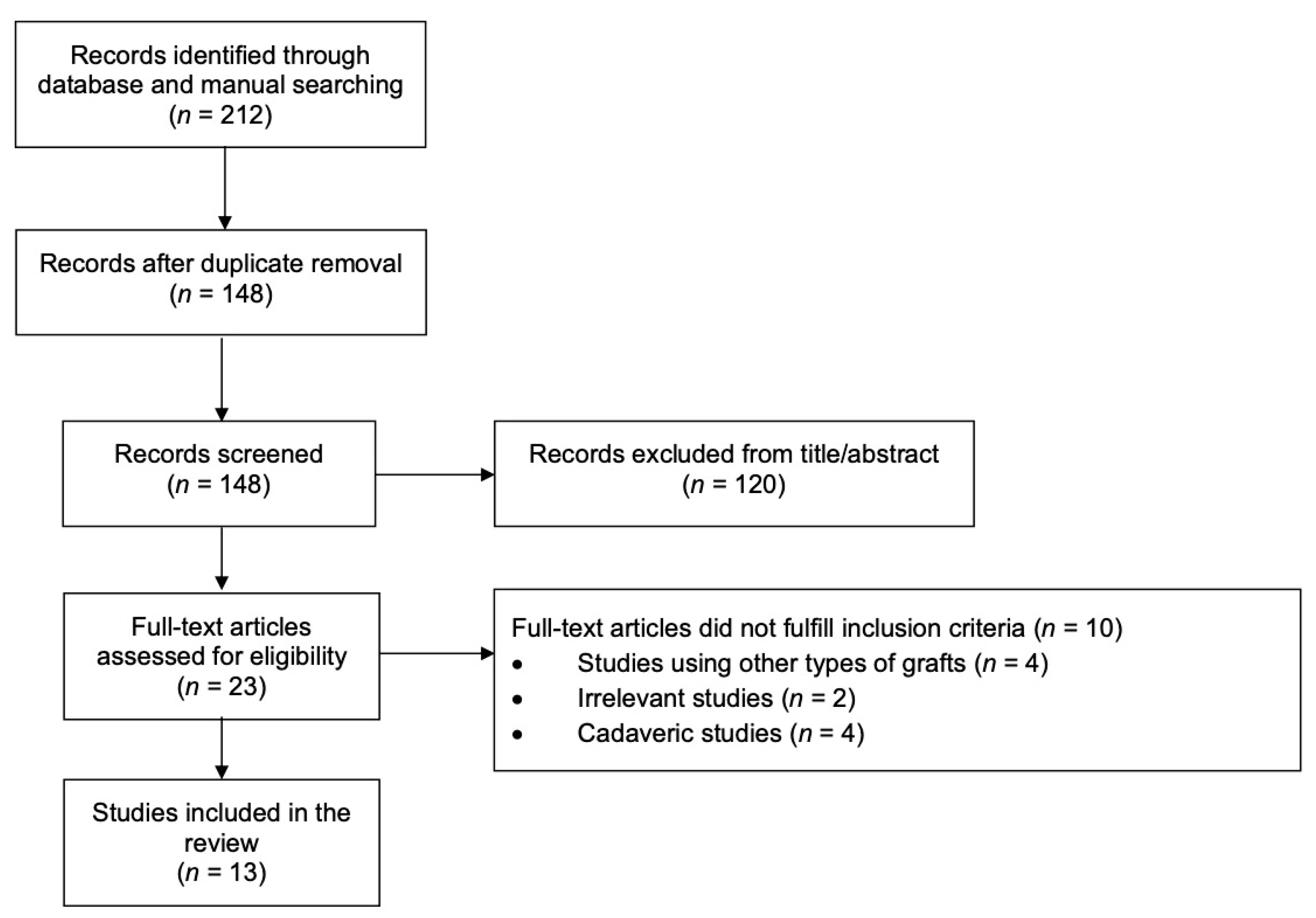
3.1. Identification of Studies
3.2. Surgical Techniques Studies’ Characteristics
3.3. Clinical Studies’ Characteristics
3.4. Quality Assessment
3.5. Clinical Outcomes
4. Discussion
4.1. Summary of Results
4.2. Interpretation of the Results in the Context of the Literature
4.3. LHBT Management
4.4. Implications for Future Research
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Burnier, M.; Elhassan, B.T.; Sanchez-Sotelo, J. Surgical Management of Irreparable Rotator Cuff Tears. J. Bone Jt. Surgery-American Vol. 2019, 101, 1603–1612. [Google Scholar] [CrossRef] [PubMed]
- Barth, J.; Olmos, M.I.; Swan, J.; Barthelemy, R.; Delsol, P.; Boutsiadis, A. Superior Capsular Reconstruction with the Long Head of the Biceps Autograft Prevents Infraspinatus Retear in Massive Posterosuperior Retracted Rotator Cuff Tears. Am. J. Sports Med. 2020, 48, 1430–1438. [Google Scholar] [CrossRef]
- Kitridis, D.; Tsikopoulos, K.; Bisbinas, I.; Papaioannidou, P.; Givissis, P. Efficacy of Pharmacological Therapies for Adhesive Capsulitis of the Shoulder: A Systematic Review and Network Meta-analysis. Am. J. Sports Med. 2019, 47, 3552–3560. [Google Scholar] [CrossRef]
- Catapano, M.; de Sa, D.; Ekhtiari, S.; Lin, A.; Bedi, A.; Lesniak, B.P. Arthroscopic Superior Capsular Reconstruction for Massive, Irreparable Rotator Cuff Tears: A Systematic Review of Modern Literature. Arthroscopy 2019, 35, 1243–1253. [Google Scholar] [CrossRef]
- Mihata, T.; Lee, T.Q.; Watanabe, C.; Fukunishi, K.; Ohue, M.; Tsujimura, T.; Kinoshita, M. Clinical results of arthroscopic superior capsule reconstruction for irreparable rotator cuff tears. Arthroscopy 2013, 29, 459–470. [Google Scholar] [CrossRef] [PubMed]
- Elrahman, A.A.A.; Sobhy, M.H.; Abdelazim, H.; Haroun, H.K.O. Superior Capsular Reconstruction: Fascia Lata Versus Acellular Dermal Allograft: A Systematic Review. Arthrosc. Sports Med. Rehabil. 2020, 2, e389–e397. [Google Scholar] [CrossRef] [PubMed]
- Boutsiadis, A.; Chen, S.; Jiang, C.; Lenoir, H.; Delsol, P.; Barth, J. Long Head of the Biceps as a Suitable Available Local Tissue Autograft for Superior Capsular Reconstruction: “The Chinese Way. ” Arthrosc. Tech. 2017, 6, e1559–e1566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veen, E.J.; Stevens, M.; Diercks, R.L. Biceps Autograft Augmentation for Rotator Cuff Repair: A Systematic Review. Arthroscopy 2018, 34, 1297–1305. [Google Scholar] [CrossRef] [PubMed]
- Sano, H.; Mineta, M.; Kita, A.; Itoi, E. Tendon patch grafting using the long head of the biceps for irreparable massive rotator cuff tears. J. Orthop. Sci. 2010, 15, 310–316. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. for the PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Coleman, B.D.; Khan, K.M.; Maffulli, N.; Cook, J.L.; Wark, J.D. Studies of surgical outcome after patellar tendinopathy: Clinical significance of methodological deficiencies and guidelines for future studies. Scand. J. Med. Sci. Sports 2000, 10, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Moga, C.; Guo, B.; Schopflocher, D.; Harstall, C. Development of a quality appraisal tool for case series studies using a modified Delphi technique. Edmont. Inst. Heal. Econ. 2012, 1–52. [Google Scholar]
- Bond, M.; Pilowsky, I. Subjective assessment of pain and its relationship to the administration of analgesics in patients with advanced cancer. J. Psychosom. Res. 1966, 10, 203–208. [Google Scholar] [CrossRef]
- Lee, J.S. Clinically important change in the visual analog scale after adequate pain control. Acad. Emerg. Med. 2003, 10, 1128–1130. [Google Scholar] [CrossRef]
- Higgins, J.; Deeks, J. Chapter 9: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J., Green, S., Eds.; John Willey & Sons: Chichester, UK, 2008; pp. 243–296. [Google Scholar]
- Kim, Y.-S.; Lee, H.-J.; Park, I.; Sung, G.Y.; Kim, D.-J.; Kim, J.-H. Arthroscopic In Situ Superior Capsular Reconstruction Using the Long Head of the Biceps Tendon. Arthrosc. Tech. 2018, 7, e97–e103. [Google Scholar] [CrossRef] [Green Version]
- Fandridis, E.; Zampeli, F. Superior Capsular Reconstruction with Double Bundle of Long Head Biceps Tendon Autograft: The “Box” Technique. Arthrosc. Tech. 2020, 9, e1747–e1757. [Google Scholar] [CrossRef] [PubMed]
- Adrian, S.C.; Field, L.D. Biceps Transposition for Biological Superior Capsular Reconstruction. Arthrosc. Tech. 2020, 9, e841–e846. [Google Scholar] [CrossRef]
- Kim, D.; Jang, Y.; Park, J.; On, M. Arthroscopic Superior Capsular Reconstruction with Biceps Autograft: Snake Technique. Arthrosc. Tech. 2019, 8, e1085–e1092. [Google Scholar] [CrossRef]
- Milano, G.; Marchi, G.; Bertoni, G.; Vaisitti, N.; Galli, S.; Scaini, A.; Saccomanno, M.F. Augmented Repair of Large to Massive Delaminated Rotator Cuff Tears with Autologous Long Head of the Biceps Tendon Graft: The Arthroscopic “Cuff-Plus” Technique. Arthrosc. Tech. 2020, 9, e1683–e1688. [Google Scholar] [CrossRef]
- Chiang, C.H.; Shaw, L.; Chih, W.H.; Yeh, M.L.; Su, W.R. Arthroscopic Rotator Cuff Repair Combined with Modified Superior Capsule Reconstruction as Reinforcement by the Long Head of the Biceps. Arthrosc. Tech. 2019, 8, e1223–e1231. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.-S.; Yeom, J.; Park, J.; Cha, J. L-Shape Superior Capsular Augmentation Technique Using Biceps Tendon: The Biceps L-Shape Shifting Technique. Arthrosc. Tech. 2020, 9, e703–e709. [Google Scholar] [CrossRef]
- Hermanowicz, K.; Góralczyk, A.; Malinowski, K.; Jancewicz, P.; Domżalski, M.E. Long Head Biceps Tendon—Natural Patch for Massive Irreparable Rotator Cuff Tears. Arthrosc. Tech. 2018, 7, e473–e478. [Google Scholar] [CrossRef] [Green Version]
- Chillemi, C.; Mantovani, M.; Gigante, A. Superior capsular reconstruction of the shoulder: The ABC (Arthroscopic Biceps Chillemi) technique. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Lee, H.-J.; Park, T.-Y.; Lee, J.-U.; Kim, Y.-S. Preliminary Outcomes of Arthroscopic Biceps Rerouting for the Treatment of Large to Massive Rotator Cuff Tears. J. Shoulder Elb. Surg. 2020. [Google Scholar] [CrossRef]
- Kocaoglu, B.; Firatli, G.; Ulku, T.K. Partial Rotator Cuff Repair with Superior Capsular Reconstruction Using the Biceps Tendon Is as Effective as Superior Capsular Reconstruction Using a Tensor Fasciae Latae Autograft in the Treatment of Irreparable Massive Rotator Cuff Tears. Orthop. J. Sports Med. 2020, 8. [Google Scholar] [CrossRef]
- Moore, D.R.; Cain, E.L.; Schwartz, M.L.; Clancy, W.G. Allograft reconstruction for massive, irreparable rotator cuff tears. Am. J. Sports Med. 2006, 34, 392–396. [Google Scholar] [CrossRef]
- Sclamberg, S.G.; Tibone, J.E.; Itamura, J.M.; Kasraeian, S. Six-month magnetic resonance imaging follow-up of large and massive rotator cuff repairs reinforced with porcine small intestinal submucosa. J. Shoulder Elb. Surg. 2004, 13, 538–541. [Google Scholar] [CrossRef] [PubMed]
- Neumann, J.A.; Zgonis, M.H.; Rickert, K.D.; Bradley, K.E.; Kremen, T.J.; Boggess, B.R.; Toth, A.P. Interposition Dermal Matrix Xenografts: A Successful Alternative to Traditional Treatment of Massive Rotator Cuff Tears. Am. J. Sports Med. 2017, 45, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- Pogorzelski, J.; Horan, M.P.; Fritz, E.M.; Katthagen, J.C.; Godin, J.A.; Millett, P.J. Arthroscopic Superior Capsule Reconstruction (ASCR) vs Latissimus Dorsi Transfer (LDT): A Comparison of Early Clinical Outcomes. Orthop. J. Sports Med. 2017, 5. [Google Scholar] [CrossRef] [Green Version]
- Mihata, T. Editorial Commentary: Superior Capsule Reconstruction: Graft Healing for Success. Arthrosc. J. Arthrosc. Relat. Surg. 2018, 34, 100–101. [Google Scholar] [CrossRef] [Green Version]
- Mihata, T.; McGarry, M.H.; Kahn, T.; Goldberg, I.; Neo, M.; Lee, T.Q. Biomechanical Effect of Thickness and Tension of Fascia Lata Graft on Glenohumeral Stability for Superior Capsule Reconstruction in Irreparable Supraspinatus Tears. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 32, 418–426. [Google Scholar] [CrossRef] [PubMed]
- McGough, R.L.; Debski, R.E.; Taskiran, E.; Fu, F.H.; Woo, S.L.-Y. Mechanical properties of the long head of the biceps tendon. Knee Surgery, Sports Traumatol. Arthrosc. 1996, 3, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Park, M.C.; Itami, Y.; Lin, C.C.; Kantor, A.; McGarry, M.H.; Park, C.J.; Lee, T.Q. Anterior Cable Reconstruction Using the Proximal Biceps Tendon for Large Rotator Cuff Defects Limits Superior Migration and Subacromial Contact Without Inhibiting Range of Motion: A Biomechanical Analysis. Arthroscopy 2018, 34, 2590–2600. [Google Scholar] [CrossRef]
- Han, S.-Y.; Lee, T.Q.; Wright, D.J.; Park, I.-J.; Mauro, M.; McGarry, M.H.; Lee, H.-J.; Kim, Y.-S. Effect of biceps rerouting technique to restore glenohumeral joint stability for large irreparable rotator cuff tears: A cadaveric biomechanical study. J. Shoulder Elb. Surg. 2020, 29, 1425–1434. [Google Scholar] [CrossRef] [PubMed]
- El-Shaar, R.; Soin, S.; Nicandri, G.; Maloney, M.; Voloshin, I. Superior Capsular Reconstruction with a Long Head of the Biceps Tendon Autograft: A Cadaveric Study. Orthop. J. Sports Med. 2018, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, F.; Kong, C.H.; Hasan, M.Y.; Ramruttun, A.K.; Kumar, V.P. Superior capsular reconstruction for irreparable supraspinatus tendon tears using the long head of biceps: A biomechanical study on cadavers. Orthop. Traumatol. Surg. Res. 2019, 105, 257–263. [Google Scholar] [CrossRef]
- Dierickx, C.; Ceccarelli, E.; Conti, M.; Vanlommel, J.; Castagna, A. Variations of the intra-articular portion of the long head of the biceps tendon: A classification of embryologically explained variations. J. Shoulder Elb. Surg. 2009, 18, 556–565. [Google Scholar] [CrossRef]
- Shang, X.; Chen, J.; Chen, S. A meta-analysis comparing tenotomy and tenodesis for treating rotator cuff tears combined with long head of the biceps tendon lesions. PLoS ONE 2017, 12, e0185788. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-J.; Jeong, J.-Y.; Kim, C.-K.; Kim, Y.-S. Surgical treatment of lesions of the long head of the biceps brachii tendon with rotator cuff tear: A prospective randomized clinical trial comparing the clinical results of tenotomy and tenodesis. J. Shoulder Elb. Surg. 2016, 25, 1107–1114. [Google Scholar] [CrossRef]
- Aflatooni, J.O.; Meeks, B.D.; Froehle, A.W.; Bonner, K.F. Biceps tenotomy versus tenodesis: Patient-reported outcomes and satisfaction. J. Orthop. Surg. Res. 2020, 15, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Zabrzyński, J.; Huri, G.; Gryckiewicz, S.; Çetik, R.M.; Szwedowski, D.; Łukasz, Ł.; Gagat, M.; Paczesny, Ł. Biceps Tenodesis versus Tenotomy with Fast Rehabilitation Protocol—A Functional Perspective in Chronic Tendinopathy. J. Clin. Med. 2020, 9, 3938. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Jiang, C. The Elongation of Biceps Muscle Tendon Unit After Rerouting of the Long Head of Biceps Tendon as Superior Capsular Augmentation: A Quantitative Measurement. Arthrosc. Sports Med. Rehabil. 2020, 2, e531–e537. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study (Year) | Anesthesia | Position | Surgical Steps | |||||
|---|---|---|---|---|---|---|---|---|
| Subacromial Decompression | Subscapularis Repair | LHBT Graft Harvesting Through Separate Incision | LHBT Fixation | Management of LHBT Distal to Fixation | RC Tear | |||
| Adrian (2020) [18] | N/R | Beach chair or lateral decubitus | Bursectomy, optional acromioplasty | N/R | No | 1 Anchor to GT | Intact, rerouted | Partial repair |
| Boutsiadis (2017) [7] | General and interscalene block | Beach chair | Bursectomy, acromioplasty | Yes | No | 1 Anchor to GT | Tenotomy | Partial repair, side-to-side to LHBT |
| Chiang (2019) [21] | General | Beach chair | Bursectomy, optional acromioplasty | N/R | No | 1 Anchor to GT | Tenotomy or tenodesis | Repair including LHBT |
| Fandridis (2020) [17] | N/R | Lateral decubitus | Bursectomy, optional acromioplasty | Yes | 8–12 cm sufficient for double-bundle | 2 anchors to superior glenoid, 2 anchors to GT | Tenodesis | Partial repair, side-to-side to LHBT |
| Hermanowicz (2018) [23] | General | Beach chair | Bursectomy, optional acromioplasty | Yes | No | 1 Anchor to GT | Intact | Partial repair, side-to-side to LHBT |
| Kim Y. (2018) [16] | General | Lateral decubitus | Bursectomy, optional acromioplasty | N/R | No | 1 Anchor to GT, 1 anchor for medial LHBT to anterior footprint | Intact, rerouted | Partial repair |
| Kim D. (2019) [19] | General and suprascapular block | Beach chair | Bursectomy, acromioplasty | N/R | 14 cm sufficient for double- or triple-bundle | 2 anchors to superior glenoid, 4 anchors to GT | Tenodesis | Partial repair, side-to-side to LHBT |
| Kim D. (2020) [22] | General | Beach chair | Bursectomy, acromioplasty | N/R | No | 1 Anchor to GT | Intact | Partial repair including LHBT |
| Milano (2020) [20] | General and/or interscalene block | Beach chair or lateral decubitus | Bursectomy | Yes | No | 1 Anchor to GT | Tenotomy | Repair including LHBT |
| Study (Year) | Intervention | Number of Patients | Males/Females | Mean Age, Years (SD) | Mean Follow-up, Months (SD) |
|---|---|---|---|---|---|
| Barth (2020) [2] |
| A. 28 B. 30 C. 24 | A. 15/13 B. 19/11 C. 16/8 | A. 63 (9) B. 59 (7.6) C. 60 (7) | A. 15 (2) B. 27 (5) C. 25 (2) |
| Chillemi (2018) [24] | SCR with LHBT | 9 | 4/5 | 66.4 (3) | 6 |
| Kim J. (2020) [25] | SCR with LHBT | 61 | 25/36 | 64.5 (8.2) | 21.2 (range 18–27) |
| Kocaoglu (2020) [26] |
| A. 14 B. 12 | N/R | A. 64.6 (8.4) B. 62.5 (6.5) | A. 28 B. 32 |
| Study (Year) | Anesthesia | Position | Surgical Steps | ||||
|---|---|---|---|---|---|---|---|
| Subacromial Decompression | Subscapularis Repair | LHBT Fixation | Management of LHBT Distal to Fixation | RC Tear | |||
| Barth (2020) [2] | General and interscalene block | Beach chair | Bursectomy, acromioplasty | Yes | 1 Anchor to GT | Tenotomy | Partial repair, side-to-side to LHBT |
| Chillemi (2018) [24] | General and/or interscalene block | Beach chair or lateral decubitus | Bursectomy | Yes | 2 Anchors or 2 transosseous tunnels to GT | Tenotomy or tenodesis | Side-to-side convergence to LHBT |
| Kim J. (2020) [25] | General | Lateral decubitus | Bursectomy, acromioplasty | Yes | 1 Anchor to GT, 1 anchor for medial LHBT to anterior footprint | Intact, rerouted | Partial repair including LHBT |
| Kocaoglu (2020) [26] | General | Beach chair | Bursectomy, optional acromioplasty | Yes | 2 anchors to superior glenoid, 2 anchors to GT | Intact | Partial repair, side-to-side to LHBT |
| Mean Preoperative (SD) | Mean Postoperative (SD) | p | |
|---|---|---|---|
| Barth (2020) [2] | |||
| Pain VAS | 5.2 (2) | 1.4 (1.4) | <0.001 |
| Constant Score | 50 (13) | 77 (10) | <0.001 |
| ASES | 45 (19) | 80 (15) | <0.001 |
| SST | 4 (3) | 8 (3) | <0.001 |
| SSV | 41 (22) | 75 (18) | <0.001 |
| Strength, kg | 2.3 (1) | 6.4 (1.6) | |
| Chillemi (2018) [24] | |||
| Pain VAS | 7.2 | 2.3 | <0.01 |
| Kim J. (2020) [25] | |||
| Pain VAS | 3.7 (2) | 1.6 (1.7) | 0.019 |
| ASES | 60 (19.7) | 85. 2 (11.4) | <0.001 |
| KSS | 64.3 (15.5) | 85.3 (11.4) | 0.001 |
| AHD, mm | 7.1 (2.1) | 9 (2.9) | <0.001 |
| Kocaoglu (2020) [26] | |||
| Pain VAS | 8.5 (3.5) | 1.4 (0.8) | 0.001 |
| ASES | 46.2 (16.2) | 85.2 (12.4) | 0.005 |
| Quick DASH | 52.5 (12.8) | 12.6 (18) | 0.012 |
| AHD, mm | 7 (1.5) | 10.2 (2.5) | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitridis, D.; Yiannakopoulos, C.; Sinopidis, C.; Givissis, P.; Galanis, N. Superior Capsular Reconstruction of the Shoulder Using the Long Head of the Biceps Tendon: A Systematic Review of Surgical Techniques and Clinical Outcomes. Medicina 2021, 57, 229. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030229
Kitridis D, Yiannakopoulos C, Sinopidis C, Givissis P, Galanis N. Superior Capsular Reconstruction of the Shoulder Using the Long Head of the Biceps Tendon: A Systematic Review of Surgical Techniques and Clinical Outcomes. Medicina. 2021; 57(3):229. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030229
Chicago/Turabian StyleKitridis, Dimitrios, Christos Yiannakopoulos, Chris Sinopidis, Panagiotis Givissis, and Nikiforos Galanis. 2021. "Superior Capsular Reconstruction of the Shoulder Using the Long Head of the Biceps Tendon: A Systematic Review of Surgical Techniques and Clinical Outcomes" Medicina 57, no. 3: 229. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57030229