
Post-Progression Survival Is Strongly Associated with Overall Survival in Patients Exhibiting Postoperative Relapse of Non-Small-Cell Lung Cancer Harboring Sensitizing EGFR Mutations

 , and
, and
Abstract
:1. Introduction
2. Patients and Methods
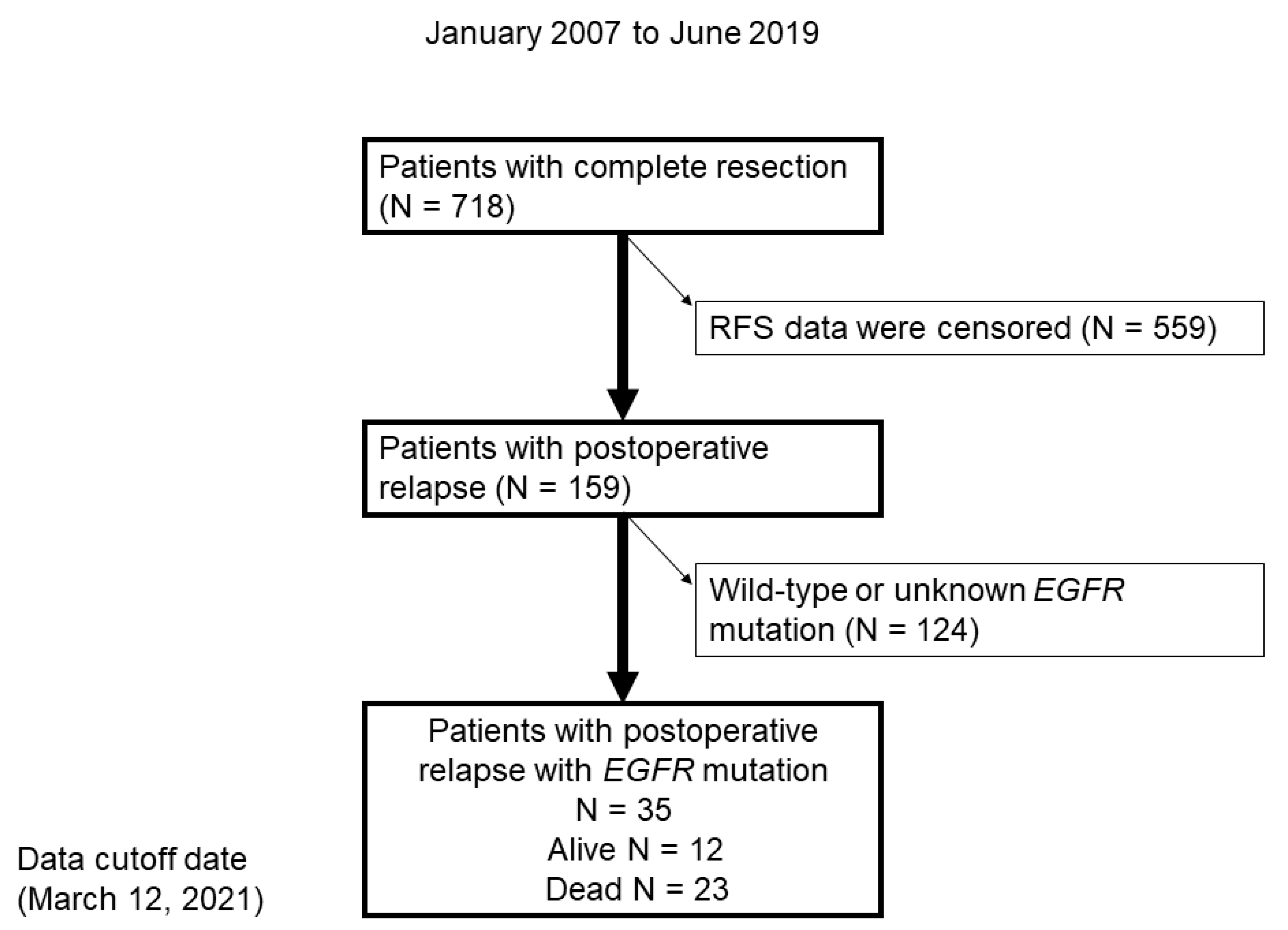
2.1. Patients
2.2. Treatment Response Assessment
2.3. Statistical Analysis
3. Results
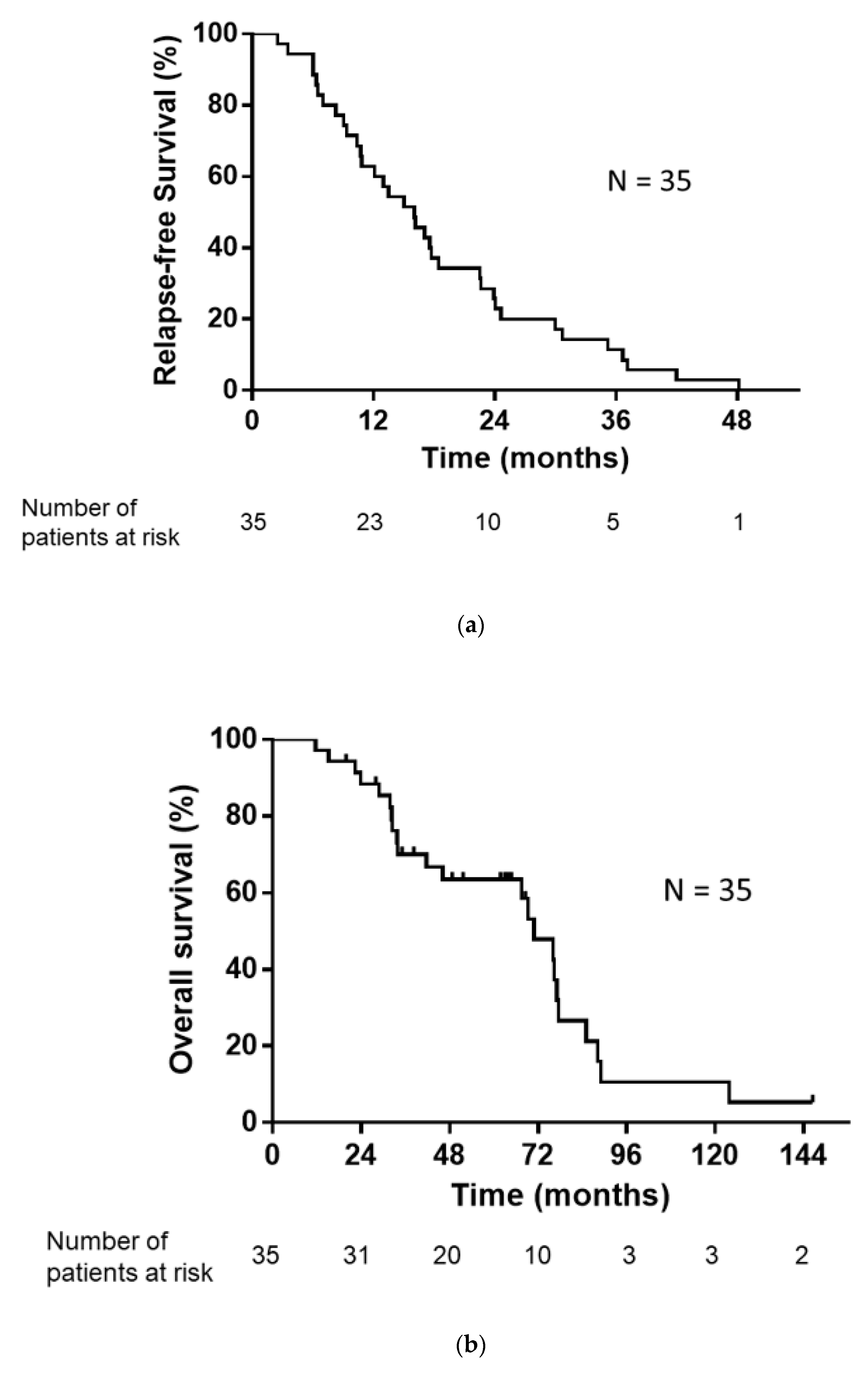
3.1. Patient Baseline Characteristics and Therapeutic Efficacy
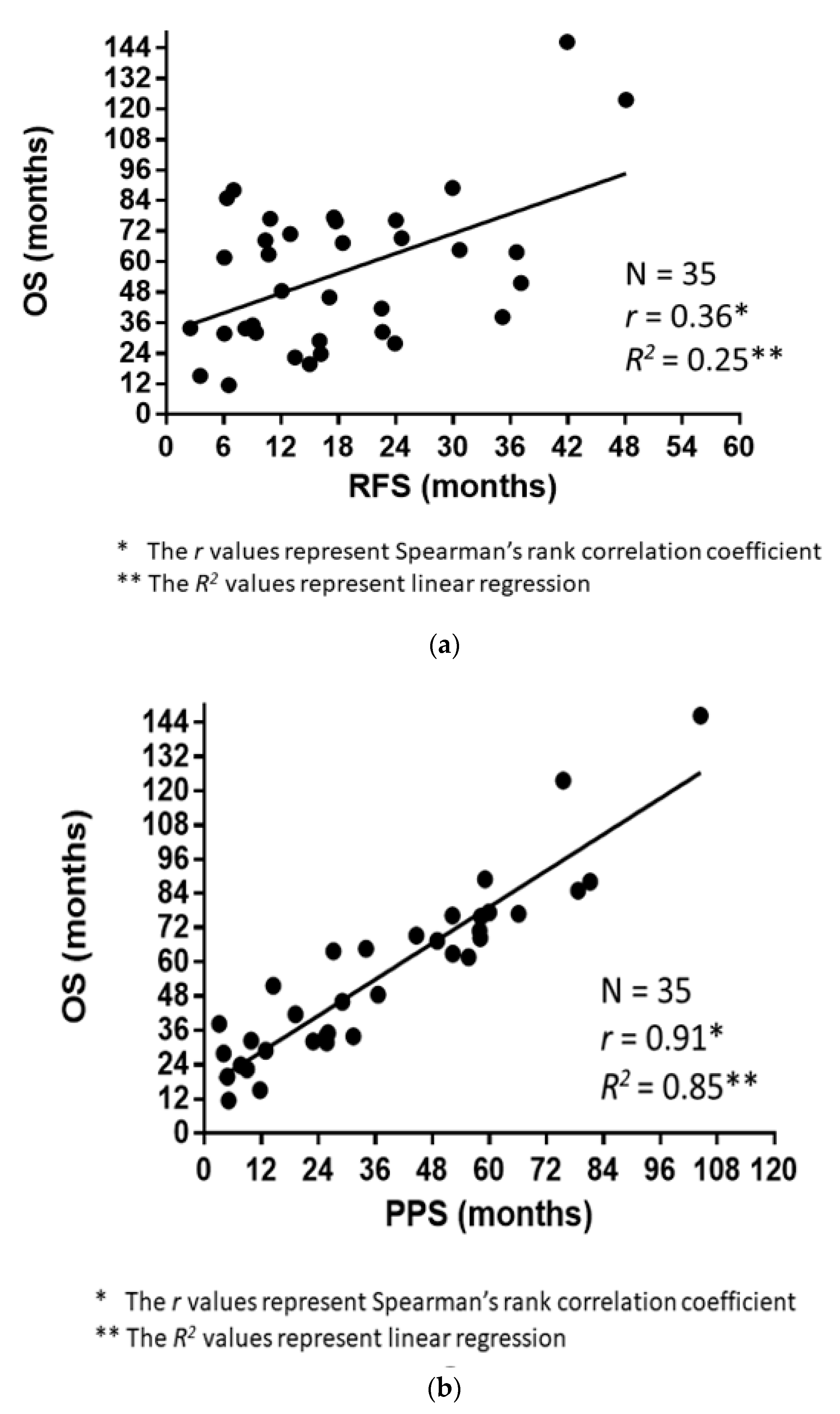
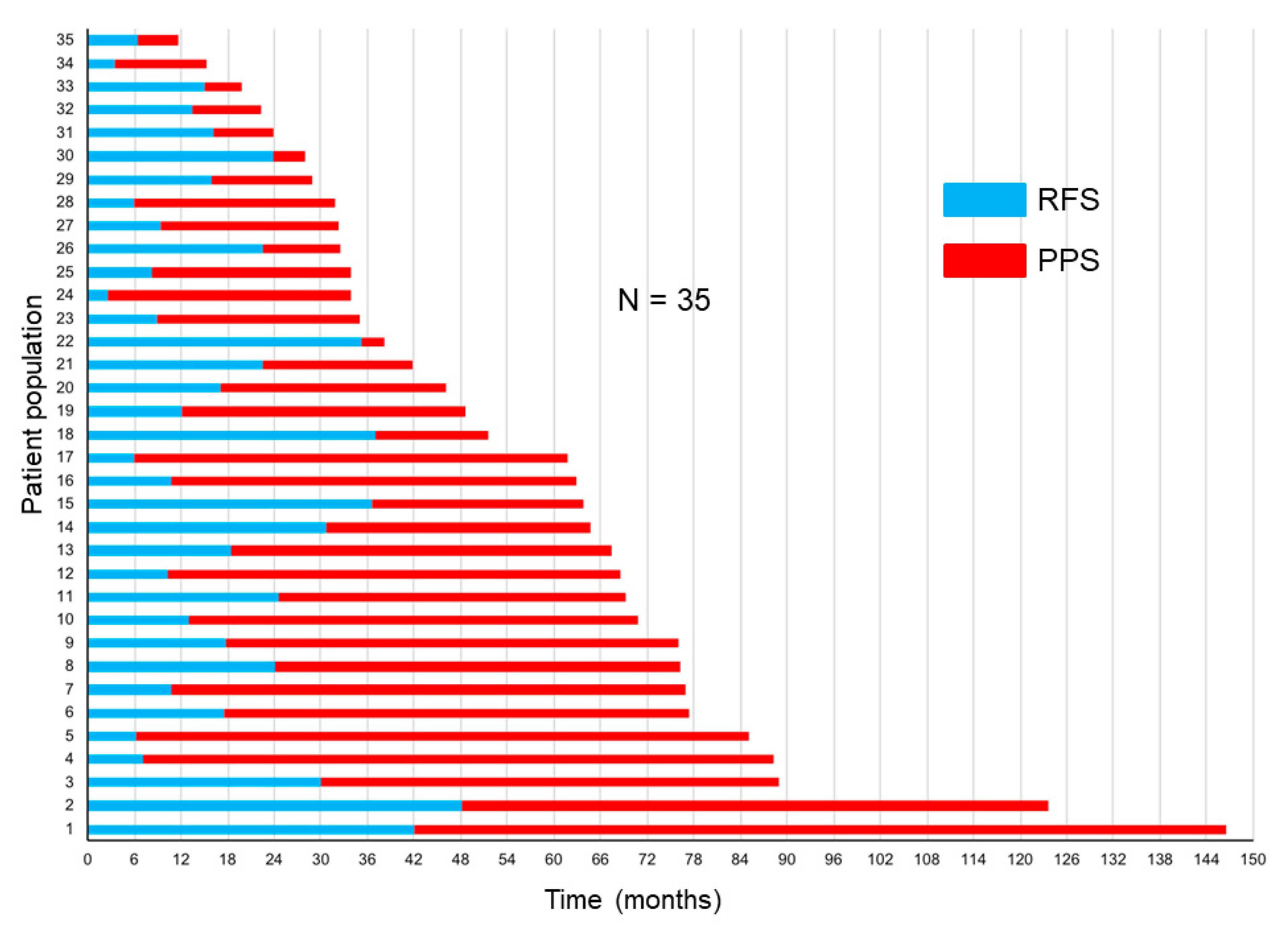
3.2. Correlations of RFS and PPS with OS
3.3. Clinical Factors Affecting PPS
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Arriagada, R.; Bergman, B.; Dunant, A.; Le Chevalier, T.; Pignon, J.-P.; Vansteenkiste, J. International Adjuvant Lung Cancer Trial Collaborative Group Cisplatin-Based Adjuvant Chemotherapy in Patients with Completely Resected Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2004, 350, 351–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugimura, H.; Nichols, F.C.; Yang, P.; Allen, M.S.; Cassivi, S.D.; Deschamps, C.; Williams, B.A.; Pairolero, P.C. Survival After Recurrent Nonsmall-Cell Lung Cancer After Complete Pulmonary Resection. Ann. Thorac. Surg. 2007, 83, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Saisho, S.; Yasuda, K.; Maeda, A.; Yukawa, T.; Okita, R.; Hirami, Y.; Shimizu, K.; Nakata, M. Post-recurrence survival of patients with non-small-cell lung cancer after curative resection with or without induction/adjuvant chemotherapy. Interact. Cardiovasc. Thorac. Surg. 2012, 16, 166–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soria, J.C.; Massard, C.; Le Chevalier, T. Should progression-free survival be the primary measure of efficacy for advanced NSCLC therapy? Ann. Oncol. 2010, 21, 2324–2332. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Von Pawel, J.; Zatloukal, P.; Ramlau, R.; Gorbounova, V.; Hirsh, V.; Leighl, N.; Mezger, J.; Archer, V.; Moore, N.; et al. Phase III Trial of Cisplatin Plus Gemcitabine with Either Placebo or Bevacizumab as First-Line Therapy for Nonsquamous Non–Small-Cell Lung Cancer: AVAiL. J. Clin. Oncol. 2009, 27, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Hotta, K.; Kiura, K.; Fujiwara, Y.; Takigawa, N.; Hisamoto, A.; Ichihara, E.; Tabata, M.; Tanimoto, M. Role of survival post-progression in phase III trials of systemic chemotherapy in advanced non-small-cell lung cancer: A systematic review. PLoS ONE 2011, 6, e26646. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, H.; Okamoto, I.; Morita, S.; Taguri, M.; Nakagawa, K. Postprogression survival for first-line chemotherapy of patients with advanced non-small-cell lung cancer. Ann. Oncol. 2012, 23, 1537–1541. [Google Scholar] [CrossRef]
- Broglio, K.R.; Berry, D.A. Detecting an Overall Survival Benefit that Is Derived from Progression-Free Survival. J. Natl. Cancer Inst. 2009, 101, 1642–1649. [Google Scholar] [CrossRef]
- Imai, H.; Kaira, K.; Mori, K.; Kotake, M.; Mitani, M.; Kawashima, N.; Hisada, T.; Minato, K. Post-progression survival is highly linked to overall survival in patients with non-small-cell lung cancer harboring sensitive EGFR mutations treated with first-line epidermal growth factor receptor-tyrosine kinase inhibitors. Thorac. Cancer 2019, 10, 2200–2208. [Google Scholar] [CrossRef] [Green Version]
- Kosaka, T.; Yatabe, Y.; Onozato, R.; Kuwano, H.; Mitsudomi, T. Prognostic implication of EGFR, KRAS, and TP53 gene mu-tations in a large cohort of Japanese patients with surgically treated lung adenocarcinoma. J. Thorac. Oncol. 2009, 4, 22–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takamochi, K.; Oh, S.; Matsunaga, T.; Suzuki, K. Prognostic impacts of EGFR mutation status and subtype in patients with surgically resected lung adenocarcinoma. J. Thorac. Cardiovasc. Surg. 2017, 154, 1768–1774.e1. [Google Scholar] [CrossRef] [Green Version]
- Mok, T.S.; Wu, Y.-L.; Thongprasert, S.; Yang, C.-H.; Chu, D.-T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or Carboplatin–Paclitaxel in Pulmonary Adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or Chemotherapy for Non–Small-Cell Lung Cancer with Mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef] [Green Version]
- Mitsudomi, T.; Morita, S.; Yatabe, Y.; Negoro, S.; Okamoto, I.; Tsurutani, J.; Seto, T.; Satouchi, M.; Tada, H.; Hirashima, T.; et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): An open label, randomised phase 3 trial. Lancet Oncol. 2010, 11, 121–128. [Google Scholar] [CrossRef]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Zhou, C.; Wu, Y.L.; Chen, G.; Feng, J.; Liu, X.-Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Final overall survival results from a randomised, phase III study of erlotinib versus chemotherapy as first-line treatment of EGFR mutation-positive advanced non-small-cell lung cancer (OPTIMAL, CTONG-0802). Ann. Oncol. 2015, 26, 1877–1883. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.; Wu, Y.L.; Schuler, M.; Sebastian, M.; Popat, S.; Yamamoto, N.; Zhou, C.; Hu, C.P.; O’Byrne, K.; Feng, J.; et al. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): Analysis of overall survival data from two random-ised, phase 3 trials. Lancet Oncol. 2015, 16, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef]
- Kobayashi, S.; Boggon, T.J.; Dayaram, T.; Janne, P.A.; Kocher, O.; Meyerson, M.; Johnson, B.E.; Eck, M.J.; Tenen, D.G.; Halmos, B. EGFR mutation and resistance of non-small-cell lung cancer to gefitinib. N. Engl. J. Med. 2005, 352, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Oxnard, G.R.; Arcila, M.E.; Sima, C.S.; Riely, G.J.; Chmielecki, J.; Kris, M.G.; Pao, W.; Ladanyi, M.; Miller, V.A. Acquired re-sistance to EGFR tyrosine kinase inhibitors in EGFR-mutant lung cancer: Distinct natural history of patients with tumors har-boring the T790M mutation. Clin. Cancer Res. 2011, 17, 1616–1622. [Google Scholar] [CrossRef] [Green Version]
- Sequist, L.V.; Waltman, B.A.; Dias-Santagata, D.; Digumarthy, S.; Turke, A.B.; Fidias, P.; Bergethon, K.; Shaw, A.T.; Gettinger, S.; Cosper, A.K.; et al. Genotypic and Histological Evolution of Lung Cancers Acquiring Resistance to EGFR Inhibitors. Sci. Transl. Med. 2011, 3, 75ra26. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.A.; Arcila, M.E.; Rekhtman, N.; Sima, C.S.; Zakowski, M.F.; Pao, W.; Kris, M.G.; Miller, V.A.; Ladanyi, M.; Riely, G.J. Analysis of Tumor Specimens at the Time of Acquired Resistance to EGFR-TKI Therapy in 155 Patients with EGFR-Mutant Lung Cancers. Clin. Cancer Res. 2013, 19, 2240–2247. [Google Scholar] [CrossRef] [Green Version]
- Mok, T.S.; Wu, Y.L.; Ahn, M.J.; Garassino, M.C.; Kim, H.R.; Ramalingam, S.S.; Shepherd, F.A.; He, Y.; Akamatsu, H.; Theelen, W.S.; et al. Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung cancer. N. Engl. J. Med. 2017, 376, 629–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, M.; Miyata, Y.; Tsutani, Y.; Ito, H.; Nakayama, H.; Imai, K.; Ikeda, N.; Okada, M. Positive EGFR mutation status is a risk of recurrence in pN0–1 lung adenocarcinoma when combined with pathological stage and histological subtype: A retrospective multi-center analysis. Lung Cancer 2020, 141, 107–113. [Google Scholar] [CrossRef] [PubMed]
- He, Q.; Xin, P.; Zhang, M.; Jiang, S.; Zhang, J.; Zhong, S.; Liu, Y.; Guo, M.; Chen, X.; Xia, X.; et al. The impact of epidermal growth factor receptor mutations on the prognosis of resected non-small cell lung cancer: A meta-analysis of literatures. Transl. Lung Cancer Res. 2019, 8, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Imai, H.; Kaira, K.; Minato, K. Clinical significance of post-progression survival in lung cancer. Thorac. Cancer 2017, 8, 379–386. [Google Scholar] [CrossRef]
- Goldstraw, P.; Crowley, J.; Chansky, K.; Giroux, D.J.; Groome, P.A.; Rami-Porta, R.; Postmus, P.E.; Rusch, V.; Sobin, L. The IASLC Lung Cancer Staging Project: Proposals for the Revision of the TNM Stage Groupings in the Forthcoming (Seventh) Edition of the TNM Classification of Malignant Tumours. J. Thorac. Oncol. 2007, 2, 706–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagai, Y.; Miyazawa, H.; Huqun; Tanaka, T.; Udagawa, K.; Kato, M.; Fukuyama, S.; Yokote, A.; Kobayashi, K.; Kanazawa, M.; et al. Genetic Heterogeneity of the Epidermal Growth Factor Receptor in Non–Small Cell Lung Cancer Cell Lines Revealed by a Rapid and Sensitive Detection System, the Peptide Nucleic Acid-Locked Nucleic Acid PCR Clamp. Cancer Res. 2005, 65, 7276–7282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yatabe, Y.; Hida, T.; Horio, Y.; Kosaka, T.; Takahashi, T.; Mitsudomi, T. A Rapid, Sensitive Assay to Detect EGFR Mutation in Small Biopsy Specimens from Lung Cancer. J. Mol. Diagn. 2006, 8, 335–341. [Google Scholar] [CrossRef] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tu-mours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Taniguchi, K.; Okami, J.; Kodama, K.; Higashiyama, M.; Kato, K. Intratumor heterogeneity of epidermal growth factor receptor mutations in lung cancer and its correlation to the response to gefitinib. Cancer Sci. 2008, 99, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.C.; Reis-Filho, J.S. Genetic heterogeneity and cancer drug resistance. Lancet Oncol. 2012, 13, e178–e185. [Google Scholar] [CrossRef]
- Park, J.H.; Kim, T.M.; Keam, B.; Jeon, Y.K.; Lee, S.-H.; Kim, D.-W.; Chung, D.H.; Kim, Y.T.; Kim, Y.W.; Heo, D.S. Tumor Burden is Predictive of Survival in Patients with Non–Small-Cell Lung Cancer and With Activating Epidermal Growth Factor Receptor Mutations Who Receive Gefitinib. Clin. Lung Cancer 2013, 14, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.R.; Ringland, C.; Stokes, B.J.; Anthony, D.M.; Freemantle, N.; Irs, A.; Hill, S.R.; Ward, R.L. Response rate or time to progression as predictors of survival in trials of metastatic colorectal cancer or non-small-cell lung cancer: A meta-analysis. Lancet Oncol. 2006, 7, 741–746. [Google Scholar] [CrossRef]
- Hotta, K.; Fujiwara, Y.; Matsuo, K.; Kiura, K.; Takigawa, N.; Tabata, M.; Tanimoto, M. Time to Progression as a Surrogate Marker for Overall Survival in Patients with Advanced Non-small Cell Lung Cancer. J. Thorac. Oncol. 2009, 4, 311–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weir, C.J.; Walley, R.J. Statistical evaluation of biomarkers as surrogate endpoints: A literature review. Stat. Med. 2005, 25, 183–203. [Google Scholar] [CrossRef]
- Fleischer, F.; Gaschler-Markefski, B.; Bluhmki, E. A statistical model for the dependence between progression-free survival and overall survival. Stat. Med. 2009, 28, 2669–2686. [Google Scholar] [CrossRef]
- Hayashi, H.; Okamoto, I.; Taguri, M.; Morita, S.; Nakagawa, K. Postprogression Survival in Patients with Advanced Non–Small-Cell Lung Cancer Who Receive Second-Line or Third-Line Chemotherapy. Clin. Lung Cancer 2013, 14, 261–266. [Google Scholar] [CrossRef]
- Imai, H.; Takahashi, T.; Mori, K.; Ono, A.; Akamatsu, H.; Shukuya, T.; Taira, T.; Kenmotsu, H.; Naito, T.; Murakami, H.; et al. Individual-level data on the relationships of progression-free survival, post-progression survival, and tumor response with overall survival in patients with advanced non-squamous non-small cell lung cancer. Neoplasma 2014, 61, 233–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imai, H.; Mori, K.; Wakuda, K.; Ono, A.; Akamatsu, H.; Shukuya, T.; Taira, T.; Kenmotsu, H.; Naito, T.; Kaira, K.; et al. Progression-free survival, post-progression survival, and tumor response as surrogate markers for overall survival in patients with extensive small cell lung cancer. Ann. Thorac. Med. 2015, 10, 61–66. [Google Scholar] [PubMed]
- Imai, H.; Mori, K.; Ono, A.; Akamatsu, H.; Taira, T.; Kenmotsu, H.; Naito, T.; Kaira, K.; Murakami, H.; Endo, M.; et al. Individual-level data on the relationships of progression-free survival and post-progression survival with overall survival in patients with advanced non-squamous non-small cell lung cancer patients who received second-line chemotherapy. Med. Oncol. 2014, 31, 88. [Google Scholar] [CrossRef] [PubMed]
- Imai, H.; Mori, K.; Watase, N.; Fujimoto, S.; Kaira, K.; Yamada, M.; Minato, K. Clinical significance of the relationship between progression-free survival or postprogression survival and overall survival in patients with extensive disease-small-cell lung cancer treated with carboplatin plus etoposide. Can. Respir. J. 2016, 2016, 5405810. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | N = 35 |
|---|---|
| Sex | |
| Male/female | 17/8 |
| Median age at treatment (years) | 69 (44–83) |
| Performance status (PS) | |
| 0/1/2/≥3 | 20/11/3/1 |
| Smoking history | |
| Yes/no/unknown | 18/17/0 |
| Histology | |
| Adenocarcinoma/others | 35/0 |
| Pathological stage at diagnosis | |
| I/II/III/IV | 15/10/10/0 |
| Operation | |
| Lobectomy/pneumonectomy | 35/0 |
| Mutation type | |
| exon 19 del/exon 21 L858R/G719X/Compound */ex 19 duplication | 14/16/2/2/1 |
| Adjuvant chemotherapy | |
| Yes/no | 19/16 |
| Treatment with EGFR-TKI | |
| Yes/no | 30/5 |
| Presence of a T790 mutation at recurrence | |
| Positive/negative or unknown | 4/31 |
| Rechallenge with a first- or second-generation EGFR-TKI | |
| Yes/no | 3/32 |
| Treatment with osimertinib | |
| Yes/no | 3/32 |
| Treatment with immune checkpoint inhibitors | |
| Yes/no | 3/32 |
| Recurrent pattern | |
| Local recurrence/distant metastasis | 6/29 |
| Intracranial metastases at recurrence | |
| Yes/no/unknown | 9/26 |
| Liver metastases at recurrence | |
| Yes/no/unknown | 4/31 |
| Bone metastases at recurrence | |
| Yes/no/unknown | 12/23 |
| Postoperative radiation after recurrence | |
| Yes/no | 20/15 |
| Number of therapies after postoperative relapse | |
| 0/1/2/3/≥4 | 4/16/8/6/1 |
| Median (range) | 1 (0–7) |
| First Line | Second Line | Third Line | ≥Fourth Line | Total | |
|---|---|---|---|---|---|
| Gefitinib | 14 | 2 | 0 | 0 | 16 |
| Erlotinib | 3 | 1 | 0 | 0 | 4 |
| Afatinib | 5 | 1 | 0 | 0 | 6 |
| Osimertinib | 4 | 1 | 2 | 0 | 7 |
| Platinum combination | 1 | 3 | 1 | 0 | 5 |
| Platinum combination + ICIs | 0 | 1 | 0 | 0 | 1 |
| Docetaxel | 2 | 0 | 0 | 0 | 2 |
| Pemetrexed | 0 | 0 | 3 | 0 | 3 |
| S-1 | 0 | 0 | 1 | 2 | 3 |
| First- or second-generation EGFR-TKI rechallenge | - | 3 | 0 | 0 | 3 |
| Immune checkpoint inhibitors | 0 | 0 | 1 | 1 | 2 |
| Chemoradiotherapy | 1 | 0 | 0 | 0 | 1 |
| Definitive thoracic radiotherapy | 4 | 0 | 0 | 0 | 4 |
| Others (anticancer agents) | 0 | 0 | 1 | 2 | 3 |
| Best supportive care | 1 | - | - | - | - |
| Post-Progression Survival | ||||||
|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||||
| Factor | Hazard Ratio | 95% CI | p | Hazard Ratio | 95% CI | p |
| Sex | ||||||
| Male/female | 0.86 | 0.37–2.00 | 0.73 | |||
| Pathological stage at diagnosis | ||||||
| I/II–III | 1.68 | 0.61–4.61 | 0.30 | |||
| Age at relapse | 1.08 | 1.02–1.16 | <0.001 | 1.09 | 1.03–1.17 | 0.0018 |
| PS at relapse | 2.64 | 1.53–4.44 | <0.001 | 3.07 | 1.69–5.58 | 0.0004 |
| EGFR mutation type | ||||||
| Major mutation/minor mutation | 2.78 | 0.91–12.1 | 0.07 | |||
| Adjuvant chemotherapy | ||||||
| Yes/no | 0.36 | 0.12–0.97 | 0.044 | |||
| Presence of T790 mutation | ||||||
| Positive/negative or unknown | 1.57 | 0.45–4.03 | 0.43 | |||
| Rechallenge with first- or second-generation EGFR-TKI | ||||||
| Yes/no | 1.16 | 0.81–4.18 | 0.84 | |||
| First-line treatment with osimertinib | ||||||
| Yes/no | 1.66 | 0.26–5.96 | 0.52 | |||
| Treatment with immune checkpoint inhibitors | ||||||
| Yes/no | 1.91 | 0.29–7.15 | 0.43 | |||
| Recurrent pattern | ||||||
| Local recurrence/distant metastasis | 0.46 | 0.16–1.13 | 0.09 | |||
| Intracranial metastases at relapse | ||||||
| Yes/no/unknown | 1.13 | 0.36–2.98 | 0.81 | |||
| Liver metastases at relapse | ||||||
| Yes/no/unknown | 4.33 | 0.92–15.7 | 0.06 | |||
| Bone metastases at relapse | ||||||
| Yes/no/unknown | 3.41 | 0.99–1.04 | 0.009 | |||
| Postoperative radiation after relapse | ||||||
| Yes/no | 1.11 | 0.48–2.68 | 0.79 | |||
| Number of therapies after postoperative relapse | 0.86 | 0.56–1.23 | 0.46 | □ | □ | □ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imai, H.; Onozato, R.; Ginnan, M.; Kobayashi, D.; Kaira, K.; Minato, K. Post-Progression Survival Is Strongly Associated with Overall Survival in Patients Exhibiting Postoperative Relapse of Non-Small-Cell Lung Cancer Harboring Sensitizing EGFR Mutations. Medicina 2021, 57, 508. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050508
Imai H, Onozato R, Ginnan M, Kobayashi D, Kaira K, Minato K. Post-Progression Survival Is Strongly Associated with Overall Survival in Patients Exhibiting Postoperative Relapse of Non-Small-Cell Lung Cancer Harboring Sensitizing EGFR Mutations. Medicina. 2021; 57(5):508. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050508
Chicago/Turabian StyleImai, Hisao, Ryoichi Onozato, Maiko Ginnan, Daijiro Kobayashi, Kyoichi Kaira, and Koichi Minato. 2021. "Post-Progression Survival Is Strongly Associated with Overall Survival in Patients Exhibiting Postoperative Relapse of Non-Small-Cell Lung Cancer Harboring Sensitizing EGFR Mutations" Medicina 57, no. 5: 508. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050508