
The Long-Term Functional Effect of Thrombectomy on Patients with Middle Cerebral Artery Occlusion Who Exhibit Moderate to Severe Disability

 ,
,
Abstract
:1. Importance
2. Introduction
3. Material and Methods
3.1. Study Design and Participants
3.2. Endovascular Intervention Protocols
3.3. Assessment
3.4. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dombovy, M.L.; Basford, J.R.; Whisnant, J.P.; Bergstralh, E.J. Disability and use of rehabilitation services following stroke in Rochester, Minnesota, 1975–1979. Stroke 1987, 18, 830–836. [Google Scholar] [CrossRef] [Green Version]
- Kwakkel, G.; van Peppen, R.; Wagenaar, R.C.; Dauphinee, S.W.; Richards, C.; Ashburn, A.; Miller, K.; Lincoln, N.; Partridge, C.; Wellwood, I.; et al. Effects of Augmented Exercise Therapy Time after Stroke: A Meta-Analysis. Stroke 2004, 35, 2529–2539. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.B.; Kim, J.S.; Hong, B.Y.; Lim, S.H. Clinical recovery from stroke lesions and related outcomes. J. Clin. Neurosci. 2017, 37, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Mundiyanapurath, S.; Möhlenbruch, M.; Ringleb, P.A.; Bösel, J.; Wick, W.; Bendszus, M.; Radbruch, A. Posterior Circulation Acute Stroke Prognosis Early Computed Tomography Score Using Hypointense Vessels on Susceptibility Weighted Imaging Independently Predicts Outcome in Patients with Basilar Artery Occlusion. PLoS ONE 2015, 10, e0132587. [Google Scholar] [CrossRef]
- Zheng, T.; Zhu, X.; Liang, H.; Huang, H.; Yang, J.; Wang, S. Impact of early enteral nutrition on short term prognosis after acute stroke. J. Clin. Neurosci. 2015, 22, 1473–1476. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.H.; Chang, C.H.; Lee, J.; Kim, C.S.; Seo, J.P.; Yeo, S.S. Functional Role of the Corticoreticular Pathway in Chronic Stroke Patients. Stroke 2013, 44, 1099–1104. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.B.; Kim, J.S.; Hong, B.Y.; Sul, B.; Song, S.; Sung, W.J.; Hwang, B.Y.; Lim, S.H. Brain lesions affecting gait recovery in stroke patients. Brain Behav. 2017, 7, e00868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sul, B.; Lee, K.B.; Hong, B.Y.; Kim, J.S.; Kim, J.; Hwang, W.S.; Lim, S.H. Association of Lesion Location With Long-Term Recovery in Post-stroke Aphasia and Language Deficits. Front. Neurol. 2019, 10, 776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, Y.J.; Kim, J.W.; Kim, J.S.; Hong, B.Y.; Lee, K.B.; Lim, S.H. Corticospinal Tract Integrity and Long-Term Hand Function Prognosis in Patients With Stroke. Front. Neurol. 2019, 10, 374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jovin, T.G.; Chamorro, A.; Cobo, E.; De Miquel, M.A.; Molina, C.A.; Rovira, A.; Román, L.S.; Serena, J.; Abilleira, S.; Ribó, M.; et al. Thrombectomy within 8 Hours after Symptom Onset in Ischemic Stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Yi, H.J.; Sung, J.H.; Lee, M.H.; Lee, N.H. Experience of the New FlowGate2 Device as a Balloon Guide Catheter for Ischemic Stroke Intervention. World Neurosurg. 2019, 126, e736–e742. [Google Scholar] [CrossRef]
- Yi, H.J.; Lee, D.H.; Sung, J.H. Comparison of FlowGate2 and Merci as balloon guide catheters used in mechanical thrombectomies for stroke intervention. Exp. Ther. Med. 2020, 20, 1129–1136. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized Assessment of Rapid Endovascular Treatment of Ischemic Stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Wollenweber, F.A.; Tiedt, S.; Alegiani, A.; Alber, B.; Bangard, C.; Berrouschot, J.; Bode, F.J.; Boeckh-Behrens, T.; Bohner, G.; Bormann, A.; et al. Functional Outcome Following Stroke Thrombectomy in Clinical Practice. Stroke 2019, 50, 2500–2506. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.; Hong, B.; Jo, L.; Kim, J.-S.; Park, J.; Shin, B.; Lim, S. Effects of Age on Long-Term Functional Recovery in Patients with Stroke. Medicina 2020, 56, 451. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Yi, H.J.; Lee, D.H.; Sung, J.H. Safety and Feasibility of Using Argatroban Immediately After Mechanical Thrombectomy for Large Artery Occlusion. World Neurosurg. 2019, 132, e341–e349. [Google Scholar] [CrossRef]
- Yi, H.J.; Lee, D.H.; Kim, S.U. Effectiveness of Trevo stent retriever in acute ischemic stroke: Comparison with Solitaire stent. Medicine 2018, 97, e10747. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Min, D.; Lee, E.-O.; Kang, E.K. Impact of Co-occurring Dysarthria and Aphasia on Functional Recovery in Post-stroke Patients. Ann. Rehabil. Med. 2016, 40, 1010–1017. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.C.; Shin, Y.-I.; Ko, S.H.; Kim, D.Y.; Lee, J.; Sohn, M.K.; Lee, S.-G.; Oh, G.-J.; Lee, Y.-S.; Joo, M.C.; et al. Factors Associated to Returning Home in the First Year after Stroke. Brain Neurorehabilit. 2020, 13. [Google Scholar] [CrossRef]
- Nam, K.E.; Jo, L.; Jun, S.Y.; Sung, W.J.; Kim, J.S.; Hong, B.Y.; Sul, B.; Lim, S.H. Long-term effect of repetitive transcranial magnetic stimulation on disability in patients with stroke. J. Clin. Neurosci. 2018, 47, 218–222. [Google Scholar] [CrossRef]
- Van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.J.; Van Gijn, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Neil, K.H.; Purdy, M.; Falk, J.; Gallo, L. The Dysphagia Outcome and Severity Scale. Dysphagia 1999, 14, 139–145. [Google Scholar] [CrossRef]
- SantaLucia, P.; Pezzella, F.; Sessa, M.; Monaco, S.; Torgano, G.; Anticoli, S.; Zanoli, E.; Baronello, M.M.; Paciaroni, M.; Caso, V. Sex differences in clinical presentation, severity and outcome of stroke: Results from a hospital-based registry. Eur. J. Intern. Med. 2013, 24, 167–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viticchi, G.; Falsetti, L.; Plutino, A.; Bartolini, M.; Buratti, L.; Silvestrini, M. Sex influence in ischemic stroke severity and outcome among metabolically unhealthy overweight patients. J. Neurol. Sci. 2020, 416, 116955. [Google Scholar] [CrossRef] [PubMed]
- Tomita, H.; Hagii, J.; Metoki, N.; Saito, S.; Shiroto, H.; Hitomi, H.; Kamada, T.; Seino, S.; Takahashi, K.; Baba, Y.; et al. Impact of Sex Difference on Severity and Functional Outcome in Patients with Cardioembolic Stroke. J. Stroke Cerebrovasc. Dis. 2015, 24, 2613–2618. [Google Scholar] [CrossRef] [PubMed]
- Renoux, C.; Coulombe, J.; Li, L.; Ganesh, A.; Silver, L.; Rothwell, P.M. Confounding by Pre-Morbid Functional Status in Studies of Apparent Sex Differences in Severity and Outcome of Stroke. Stroke 2017, 48, 2731–2738. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Thrombectomy (n = 15) | Control (n = 30) | p Values |
|---|---|---|---|
| Sex, M/F (n) | 10/5 | 17/13 | 0.519 |
| Age, (mean ± SD, (range)) | 64.9 ± 12.3 (45–85) | 61.7 ± 8.6 (46–80) | 0.262 |
| Side of stroke, R/L (n) | 9/6 | 14/16 | 0.399 |
| Predisposing disease (%) | |||
| High blood pressure | 66.7 | 63.3 | |
| Diabetes | 26.7 | 30 | |
| Arterial Fibrillation | 46.7 | 23.3 | |
| Dyslipidemia | 60 | 46.7 |
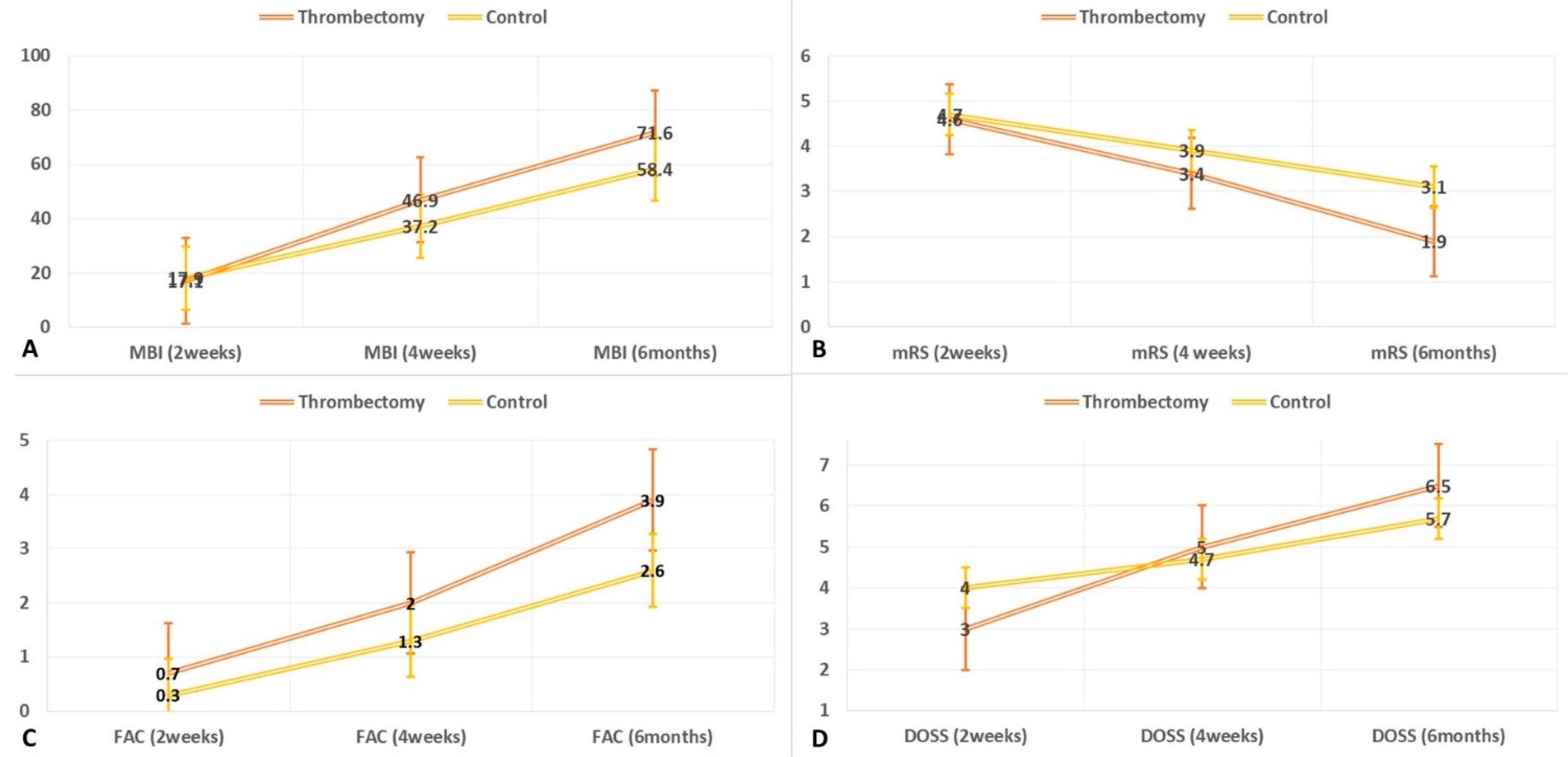
| Thrombectomy (n = 15) | Control (n = 30) | p Value (Time) | p Value (Time*Group) | ||
|---|---|---|---|---|---|
| Modified Rankin Scale (0–6) | 2 weeks | 4.6 ± 0.6 | 4.7 ± 0.5 | <0.001 1 | <0.001 1 |
| 4 weeks | 3.4 ± 1.0 | 3.9 ± 0.8 | |||
| 6 months | 1.9 ± 0.8 | 3.1 ± 1.0 | |||
| Modified Barthel Index (0–100) | 2 weeks | 17.1 ± 22.5 | 17.9 ± 19.1 | <0.001 2 | 0.037 2 |
| 4 weeks | 46.9 ± 25.2 | 37.5 ± 20.7 | |||
| 6 months | 71.6 ± 19.6 | 59.1 ± 21.2 | |||
| Functional Ambulation Category (0–5) | 2 weeks | 0.7 ± 1.0 | 0.3 ± 0.8 | <0.001 1 | 0.009 1 |
| 4 weeks | 2.0 ± 1.3 | 1.3 ± 1.2 | |||
| 6 months | 3.9 ± 1.0 | 2.6 ± 1.4 | |||
| Dysphagia Outcome Severity Scale (1–7) | 2 weeks | 3.0 ± 1.0 | 4.0 ± 1.4 | <0.001 2 | <0.001 2 |
| 4 weeks | 5.0 ± 1.5 | 4.7 ± 1.1 | |||
| 6 months | 6.5 ± 0.8 | 5.7 ± 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, H.-J.; Lee, D.-H.; Hong, B.-Y.; Song, S.-Y.; Yoo, Y.-J.; Yoon, M.-J.; Sung, J.-H.; Lim, S.-H. The Long-Term Functional Effect of Thrombectomy on Patients with Middle Cerebral Artery Occlusion Who Exhibit Moderate to Severe Disability. Medicina 2021, 57, 509. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050509
Yi H-J, Lee D-H, Hong B-Y, Song S-Y, Yoo Y-J, Yoon M-J, Sung J-H, Lim S-H. The Long-Term Functional Effect of Thrombectomy on Patients with Middle Cerebral Artery Occlusion Who Exhibit Moderate to Severe Disability. Medicina. 2021; 57(5):509. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050509
Chicago/Turabian StyleYi, Ho-Jun, Dong-Hoon Lee, Bo-Young Hong, Seung-Yoon Song, Yeun-Jie Yoo, Mi-Jeong Yoon, Jae-Hoon Sung, and Seong-Hoon Lim. 2021. "The Long-Term Functional Effect of Thrombectomy on Patients with Middle Cerebral Artery Occlusion Who Exhibit Moderate to Severe Disability" Medicina 57, no. 5: 509. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57050509