
Presence of SARS-CoV-2 and Its Entry Factors in Oral Tissues and Cells: A Systematic Review

 , , ,
, , , 
Abstract
:1. Introduction
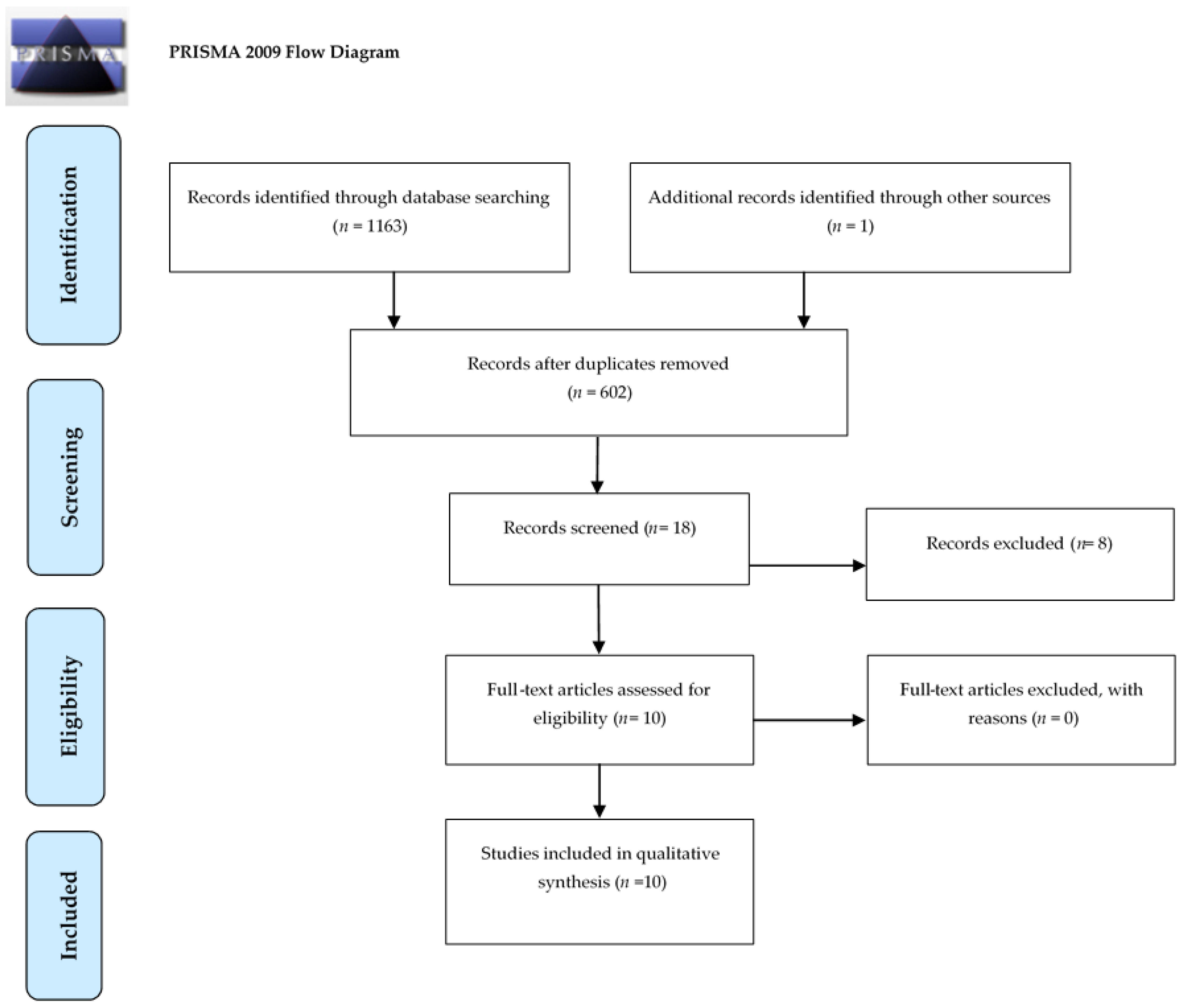
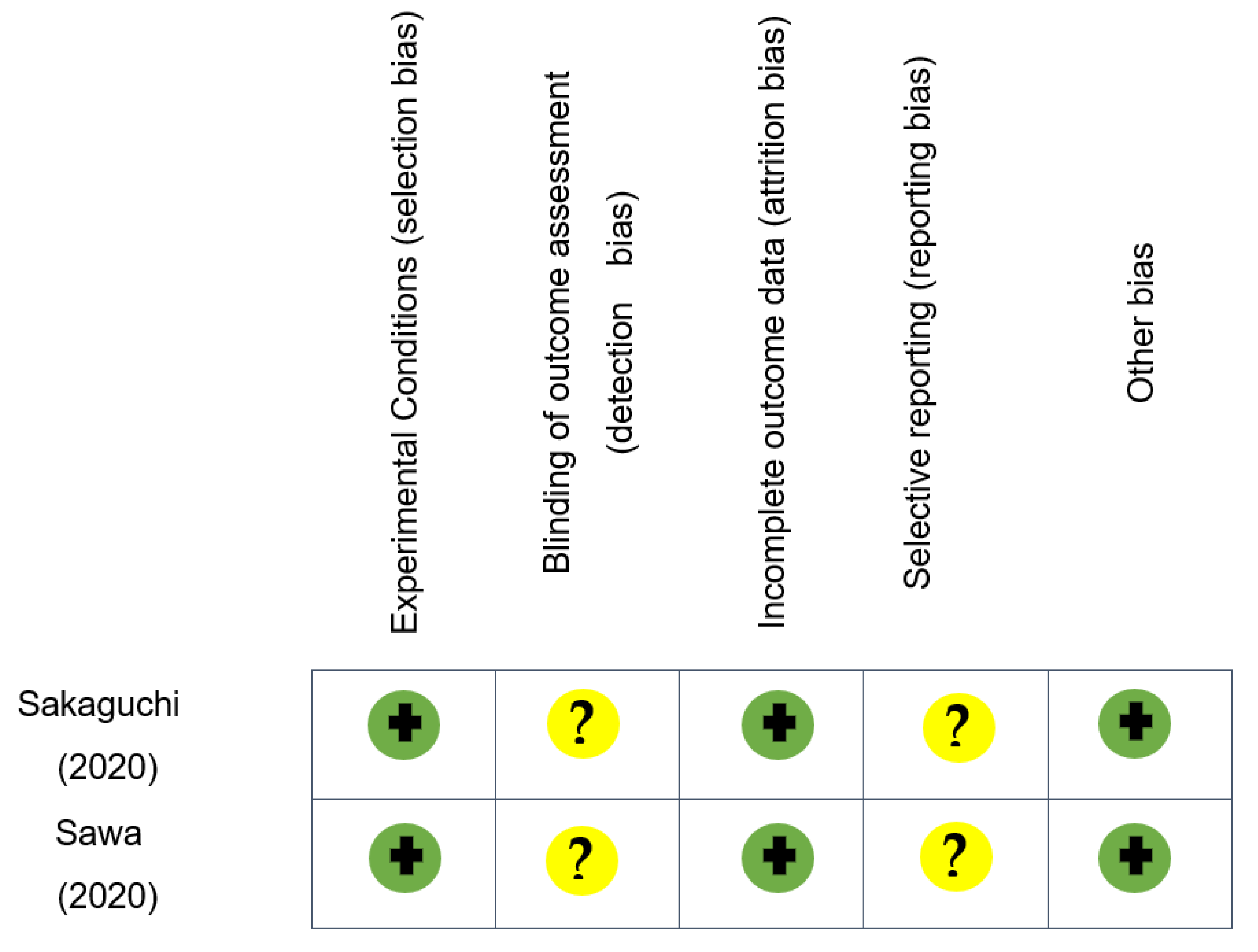
2. Materials and Methods
3. Results
3.1. Angiotensin-Converting Enzyme II (ACE2) Expression
3.2. Transmembrane Serine Proteases (TMPRSS) Expression
3.2.1. TMPRSS2 Expression
3.2.2. Other TMPRSS
3.3. Furin Expression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weekly Epidemiological Update—9 March 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-10-march-2021 (accessed on 10 March 2021).
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 10 March 2021).
- Wang, H.; Li, X.; Li, T.; Zhang, S.; Wang, L.; Wu, X.; Liu, J. The Genetic Sequence, Origin, and Diagnosis of SARS-CoV-2. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1629–1635. [Google Scholar] [CrossRef]
- Zhurakivska, K.; Troiano, G.; Pannone, G.; Caponio, V.C.A.; Muzio, L.L. An Overview of the Temporal Shedding of SARS-CoV-2 RNA in Clinical Specimens. Front. Public Health 2020, 8, 487. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic Characterisation and Epidemiology of 2019 Novel Coronavirus: Implications for Virus Origins and Receptor Binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Chen, P.; Wang, J.; Feng, J.; Zhou, H.; Li, X.; Zhong, W.; Hao, P. Evolution of the Novel Coronavirus from the Ongoing Wuhan Outbreak and Modeling of Its Spike Protein for Risk of Human Transmission. Sci. China Life Sci. 2020, 63, 457–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-Cell RNA-Seq Data Analysis on the Receptor ACE2 Expression Reveals the Potential Risk of Different Human Organs Vulnerable to 2019-NCoV Infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millet, J.K.; Whittaker, G.R. Host Cell Proteases: Critical Determinants of Coronavirus Tropism and Pathogenesis. Virus Res. 2015, 202, 120–134. [Google Scholar] [CrossRef] [PubMed]
- Bugge, T.H.; Antalis, T.M.; Wu, Q. Type II Transmembrane Serine Proteases. J. Biol. Chem. 2009, 284, 23177–23181. [Google Scholar] [CrossRef] [Green Version]
- Koletsi, D.; Iliadi, A.; Eliades, T.; Eliades, G. In Vitro Simulation and In Vivo Assessment of Tooth Wear: A Meta-Analysis of In Vitro and Clinical Research. Materials 2019, 12, 3575. [Google Scholar] [CrossRef] [Green Version]
- Hadley, E.E.; Richardson, L.S.; Torloni, M.R.; Menon, R. Gestational Tissue Inflammatory Biomarkers at Term Labor: A Systematic Review of Literature. Am. J. Reprod. Immunol. 2018, 79, e12776. [Google Scholar] [CrossRef]
- Galicia, J.C.; Guzzi, P.H.; Giorgi, F.M.; Khan, A.A. Predicting the Response of the Dental Pulp to SARS-CoV2 Infection: A Transcriptome-Wide Effect Cross-Analysis. Genes Immun. 2020, 21, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Matuck, B.F.; Dolhnikoff, M.; Maia, G.V.A.; Sendyk, D.I.; Zarpellon, A.; Gomes, S.C.; Duarte-Neto, A.N.; Pinho, J.R.R.; Gomes-Gouvêa, M.S.; Sousa, S.C.O.M.; et al. Periodontal Tissues Are Targets for Sars-Cov-2: A Post-Mortem Study. J. Oral Microbiol. 2021, 13, 1848135. [Google Scholar] [CrossRef] [PubMed]
- Pascolo, L.; Zupin, L.; Melato, M.; Tricarico, P.M.; Crovella, S. TMPRSS2 and ACE2 Coexpression in SARS-CoV-2 Salivary Glands Infection. J. Dent. Res. 2020, 99, 1120–1121. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, W.; Kubota, N.; Shimizu, T.; Saruta, J.; Fuchida, S.; Kawata, A.; Yamamoto, Y.; Sugimoto, M.; Yakeishi, M.; Tsukinoki, K. Existence of SARS-CoV-2 Entry Molecules in the Oral Cavity. Int. J. Mol. Sci. 2020, 21, 6000. [Google Scholar] [CrossRef] [PubMed]
- Sawa, Y.; Ibaragi, S.; Okui, T.; Yamashita, J.; Ikebe, T.; Harada, H. Expression of SARS-CoV-2 Entry Factors in Human Oral Tissue. J. Anat. 2021. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Li, Y.; Huang, X.; Chen, Z.; Li, Y.; Liu, C.; Chen, Z.; Duan, X. Systematic Analysis of ACE2 and TMPRSS2 Expression in Salivary Glands Reveals Underlying Transmission Mechanism Caused by SARS-CoV-2. J. Med. Virol. 2020, 92, 2556–2566. [Google Scholar] [CrossRef]
- Zhong, M.; Lin, B.; Pathak, J.L.; Gao, H.; Young, A.J.; Wang, X.; Liu, C.; Wu, K.; Liu, M.; Chen, J. ACE2 and Furin Expressions in Oral Epithelial Cells Possibly Facilitate COVID-19 Infection via Respiratory and Fecal—Oral Routes. Front. Med. 2020, 7, 580793. [Google Scholar] [CrossRef]
- Xu, H.; Zhong, L.; Deng, J.; Peng, J.; Dan, H.; Zeng, X.; Li, T.; Chen, Q. High Expression of ACE2 Receptor of 2019-NCoV on the Epithelial Cells of Oral Mucosa. Int. J. Oral Sci. 2020, 12, 1–5. [Google Scholar] [CrossRef]
- Huang, N.; Perez, P.; Kato, T.; Mikami, Y.; Okuda, K.; Gilmore, R.C.; Domínguez Conde, C.; Gasmi, B.; Stein, S.; Beach, M.; et al. Integrated Single-Cell Atlases Reveal an Oral SARS-CoV-2 Infection and Transmission Axis. medRxiv 2020. [Google Scholar] [CrossRef]
- Chen, L.; Zhao, J.; Peng, J.; Li, X.; Deng, X.; Geng, Z.; Shen, Z.; Guo, F.; Zhang, Q.; Jin, Y.; et al. Detection of SARS-CoV-2 in Saliva and Characterization of Oral Symptoms in COVID-19 Patients. Cell Prolif. 2020, 53, e12923. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef] [PubMed]
- Brandão, T.B.; Gueiros, L.A.; Melo, T.S.; Prado-Ribeiro, A.C.; Nesrallah, A.C.F.A.; Prado, G.V.B.; Santos-Silva, A.R.; Migliorati, C.A. Oral Lesions in Patients with SARS-CoV-2 Infection: Could the Oral Cavity Be a Target Organ? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, e45–e51. [Google Scholar] [CrossRef] [PubMed]
- Tapia, R.O.C.; Labrador, A.J.P.; Guimaraes, D.M.; Valdez, L.H.M. Oral Mucosal Lesions in Patients with SARS-CoV-2 Infection. Report of Four Cases. Are They a True Sign of COVID-19 Disease? Spec. Care Dentist. 2020, 40, 555–560. [Google Scholar] [CrossRef]
- Hjelmesæth, J.; Skaare, D. Loss of Smell or Taste as the Only Symptom of COVID-19. Tidsskr. Den. Nor. Laegeforening 2020, 140. [Google Scholar] [CrossRef]
- Amirfakhryan, H. Kawasaki-like Disease in Children with COVID-19: A Hypothesis. Med. Hypotheses 2020, 143, 110117. [Google Scholar] [CrossRef]
- Ross, R.; Conti, P. COVID-19 Induced by SARS-CoV-2 Causes Kawasaki-like Disease in Children: Role of pro-Inflammatory and Anti-Inflammatory Cytokines. J. Biol. Regul. Homeost. Agents 2020, 34, 767–773. [Google Scholar]
- Finsterer, J.; Stollberger, C. Causes of Hypogeusia/Hyposmia in SARS-CoV2 Infected Patients. J. Med. Virol. 2020, 92, 1793–1794. [Google Scholar] [CrossRef] [Green Version]
- Yachou, Y.; El Idrissi, A.; Belapasov, V.; Benali, S.A. Neuroinvasion, Neurotropic, and Neuroinflammatory Events of SARS-CoV-2: Understanding the Neurological Manifestations in COVID-19 Patients. Neurol. Sci. 2020, 41, 2657–2669. [Google Scholar] [CrossRef]
- Bohmwald, K.; Espinoza, J.A.; González, P.A.; Bueno, S.M.; Riedel, C.A.; Kalergis, A.M. Central Nervous System Alterations Caused by Infection with the Human Respiratory Syncytial Virus. Rev. Med. Virol. 2014, 24, 407–419. [Google Scholar] [CrossRef] [PubMed]
- Existing Bitter Medicines for Fighting 2019-nCoV-associated Infectious Diseases-Li-2020-The FASEB Journal-Wiley Online Library. Available online: https://0-faseb-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/full/10.1096/fj.202000502 (accessed on 17 February 2021).
- Arzneimittelinduzierte Störungen Des Geruchs-Und Geschmackssinns. Available online: https://www.der-arzneimittelbrief.de/de/Artikel.aspx?J=2010%26S=81 (accessed on 17 February 2021).
- Vaira, L.A.; Salzano, G.; Fois, A.G.; Piombino, P.; Riu, G.D. Potential Pathogenesis of Ageusia and Anosmia in COVID-19 Patients. Int. Forum Allergy Rhinol. 2020, 10, 1103–1104. [Google Scholar] [CrossRef]
- Milanetti, E.; Miotto, M.; Rienzo, L.D.; Monti, M.; Gosti, G.; Ruocco, G. In-Silico Evidence for Two Receptors Based Strategy of SARS-CoV-2. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Giacomelli, A.; Pezzati, L.; Conti, F.; Bernacchia, D.; Siano, M.; Oreni, L.; Rusconi, S.; Gervasoni, C.; Ridolfo, A.L.; Rizzardini, G.; et al. Self-Reported Olfactory and Taste Disorders in Patients With Severe Acute Respiratory Coronavirus 2 Infection: A Cross-Sectional Study. Clin. Infect. Dis. 2020, 71, 889–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, C.H.; Faraji, F.; Prajapati, D.P.; Boone, C.E.; DeConde, A.S. Association of Chemosensory Dysfunction and COVID-19 in Patients Presenting with Influenza-like Symptoms. Int. Forum Allergy Rhinol. 2020, 10, 806–813. [Google Scholar] [CrossRef] [Green Version]
- Nataf, S. An Alteration of the Dopamine Synthetic Pathway Is Possibly Involved in the Pathophysiology of COVID-19. J. Med. Virol. 2020, 92, 1743–1744. [Google Scholar] [CrossRef] [PubMed]
- Mariz, B.A.L.A.; Brandão, T.B.; Ribeiro, A.C.P.; Lopes, M.A.; Santos-Silva, A.R. New Insights for the Pathogenesis of COVID-19-Related Dysgeusia. J. Dent. Res. 2020, 99, 1206–1206. [Google Scholar] [CrossRef] [PubMed]
- Casas, C.G.; Català, A.; Hernández, G.C.; Rodríguez-Jiménez, P.; Fernández-Nieto, D.; Rodríguez-Villa Lario, A.; Navarro Fernández, I.; Ruiz-Villaverde, R.; Falkenhain-López, D.; Velasco, M.L.; et al. Classification of the Cutaneous Manifestations of COVID-19: A Rapid Prospective Nationwide Consensus Study in Spain with 375 Cases. Br. J. Dermatol. 2020, 183, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.; Liu, L.; Zhang, M.; Hu, Y.; Yang, Q.; Guo, J.; Guo, Y.; Dai, Y.; Xu, Y.; Cai, Y.; et al. Co-Infections of SARS-CoV-2 with Multiple Common Respiratory Pathogens in Infected Patients. Sci. China Life Sci. 2020, 63, 606–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Wu, Q.; Xu, W.; Qiao, B.; Wang, J.; Zheng, H.; Jiang, S.; Mei, J.; Wu, Z.; Deng, Y.; et al. Clinical Diagnosis of 8274 Samples with 2019-Novel Coronavirus in Wuhan. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Huttner, B.; Catho, G.; Pano-Pardo, J.R.; Pulcini, C.; Schouten, J. COVID-19: Don’t Neglect Antimicrobial Stewardship Principles! Clin. Microbiol. Infect. 2020, 26, 808–810. [Google Scholar] [CrossRef]
- Sarode, G.S.; Sarode, S.C.; Gadbail, A.R.; Gondivkar, S.; Sharma, N.K.; Patil, S. Are Oral Manifestations Related to SARS-CoV-2 Mediated Hemolysis and Anemia? Med. Hypotheses 2021, 146, 110413. [Google Scholar] [CrossRef] [PubMed]
- Carsetti, A.; Damiani, E.; Casarotta, E.; Scorcella, C.; Domizi, R.; Montomoli, J.; Gasparri, F.; Gabbanelli, V.; Pantanetti, S.; Carozza, R.; et al. Sublingual Microcirculation in Patients with SARS-CoV-2 Undergoing Veno-Venous Extracorporeal Membrane Oxygenation. Microvasc. Res. 2020, 132, 104064. [Google Scholar] [CrossRef]
- Gupta, S.; Mohindra, R.; Chauhan, P.K.; Singla, V.; Goyal, K.; Sahni, V.; Gaur, R.; Verma, D.K.; Ghosh, A.; Soni, R.K.; et al. SARS-CoV-2 Detection in Gingival Crevicular Fluid. J. Dent. Res. 2020. [Google Scholar] [CrossRef]
- Takahashi, Y.; Watanabe, N.; Kamio, N.; Kobayashi, R.; Iinuma, T.; Imai, K. Aspiration of Periodontopathic Bacteria Due to Poor Oral Hygiene Potentially Contributes to the Aggravation of COVID-19. J. Oral Sci. 2021, 63, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Roganović, J.R. MicroRNA-146a And-155, Upregulated by Periodontitis and Type 2 Diabetes in Oral Fluids, Are Predicted to Regulate SARS-CoV-2 Oral Receptors Genes. J. Periodontol. 2020. [Google Scholar] [CrossRef]
- Marouf, N.; Cai, W.; Said, K.N.; Daas, H.; Diab, H.; Chinta, V.R.; Hssain, A.A.; Nicolau, B.; Sanz, M.; Tamimi, F. Association between Periodontitis and Severity of COVID-19 Infection: A Case-Control Study. J. Clin. Periodontol. 2021, 48, 483–491. [Google Scholar] [CrossRef]
- Azzi, L.; Maurino, V.; Baj, A.; Dani, M.; d’Aiuto, A.; Fasano, M.; Lualdi, M.; Sessa, F.; Alberio, T. Diagnostic Salivary Tests for SARS-CoV-2. J. Dent. Res. 2021, 100, 115–123. [Google Scholar] [CrossRef]
- Pappalardo, F.; Russo, G.; Tshinanu, F.M.; Viceconti, M. In Silico Clinical Trials: Concepts and Early Adoptions. Brief. Bioinform. 2019, 20, 1699–1708. [Google Scholar] [CrossRef] [PubMed]
- Soltani, P.; Patini, R. Retracted COVID-19 Articles: A Side-Effect of the Hot Race to Publication. Scientometrics 2020, 125, 819–822. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| First Author | Year | Design | Samples | Methods | Molecules | Main Finding |
|---|---|---|---|---|---|---|
| Xu | 2020 | In silico | Humans | RNA sequencing (RNA-seq) | Angiotensin Converting Enzyme 2 (ACE2) | High expression of ACE2 receptor in tongue |
| Song | 2020 | In silico | Humans | RNA-seq | ACE2 Transmembrane protease serine 2 (TMPRSS2) | ACE2 and TMPRSS2 are expressed in salivary glands |
| Sakaguchi | 2020 | In silico | Humans | Real-Time Polymerase Chain Reaction(RT-PCR) | ACE2 | ACE2, TMPRSS2 and furin are expressed in tongue, |
| In vitro | Western Blot | Furin | gingiva, taste buds and saliva | |||
| In vivo | Immunohistochemistry | TMPRSS2 | ||||
| Huang | 2020 | In silico | Humans | RNA-seq | ACE2 | SARS-COV-2 entry factors are expressed in salivary |
| In vivo | In situ hybridization | TMPRSS2 | glands, mucosa and saliva | |||
| TMPRSS4 | ||||||
| TMPRSS11D | ||||||
| Fernandes Matuck | 2021 | In vivo | Humans | RT-PCR | E and | SARS-CoV-2 was detected in periodontal tissue |
| Histopathological analysis | RdRp genes | (junctional epithelium, adjacent oral gingival | ||||
| epithelium and connective tissue) | ||||||
| Pascolo | 2020 | In silico | Humans | RNA-seq | ACE2 | ACE2 and TMPRSS RNA and proteins were found |
| Protein Expression | TMPRSS2 | in salivary glands | ||||
| Galicia | 2020 | In silico | Humans | RNA-seq | ACE2 | ACE2 and TPMRSS2 are expressed in the dental pulp |
| TMPRSS2 | ||||||
| Sawa | 2020 | In vitro | Humans | RT-PCR | ACE2 | ACE2 and TMPRSS2 expression was detected in |
| In vivo | Mice | Microarray | TMPRSS2 | tongue, lip and cheek | ||
| Immunostaining | ||||||
| Zhong | 2020 | In silico | Humans | RNA-seq | ACE2 | ACE2 and Furin expression on epithelial cells from |
| Immunohistochemistry | Furin | different oral anatomical sites | ||||
| Chen | 2020 | In silico | Humans | RNA-seq | ACE2 | ACE2 expression in salivary glands |
| In vivo | RT-PCR |
| Item | Sakaguchi | Huang | Fernandes Matuck | Sawa | Chen |
|---|---|---|---|---|---|
| 2020 | 2020 | 2021 | 2020 | 2020 | |
| 1 | 2 | 2 | 2 | 2 | 2 |
| 2 | 2 | 2 | 1 | 2 | 2 |
| 3 | 2 | 2 | 1 | 2 | 0 |
| 4 | 2 | 2 | 1 | 2 | 0 |
| 5 | 2 | 2 | 2 | 2 | 2 |
| 6 | 2 | 2 | 1 | 1 | 2 |
| 7 | 2 | 2 | 0 | 0 | 0 |
| 8 | 2 | 2 | 0 | 2 | 0 |
| 9 | 2 | 2 | 1 | 2 | 1 |
| 10 | 2 | 2 | 1 | 2 | 2 |
| Score | 20 | 20 | 10 | 17 | 11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salas Orozco, M.F.; Niño-Martínez, N.; Martínez-Castañón, G.-A.; Patiño Marín, N.; Sámano Valencia, C.; Dipp Velázquez, F.A.; Sosa Munguía, P.d.C.; Casillas Santana, M.A. Presence of SARS-CoV-2 and Its Entry Factors in Oral Tissues and Cells: A Systematic Review. Medicina 2021, 57, 523. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060523
Salas Orozco MF, Niño-Martínez N, Martínez-Castañón G-A, Patiño Marín N, Sámano Valencia C, Dipp Velázquez FA, Sosa Munguía PdC, Casillas Santana MA. Presence of SARS-CoV-2 and Its Entry Factors in Oral Tissues and Cells: A Systematic Review. Medicina. 2021; 57(6):523. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060523
Chicago/Turabian StyleSalas Orozco, Marco Felipe, Nereyda Niño-Martínez, Gabriel-Alejandro Martínez-Castañón, Nuria Patiño Marín, Carolina Sámano Valencia, Farid Alonso Dipp Velázquez, Paulina del Carmen Sosa Munguía, and Miguel Angel Casillas Santana. 2021. "Presence of SARS-CoV-2 and Its Entry Factors in Oral Tissues and Cells: A Systematic Review" Medicina 57, no. 6: 523. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57060523