
Clinical Outcome of Rotational Atherectomy in Calcified Lesions in Korea-ROCK Registry

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
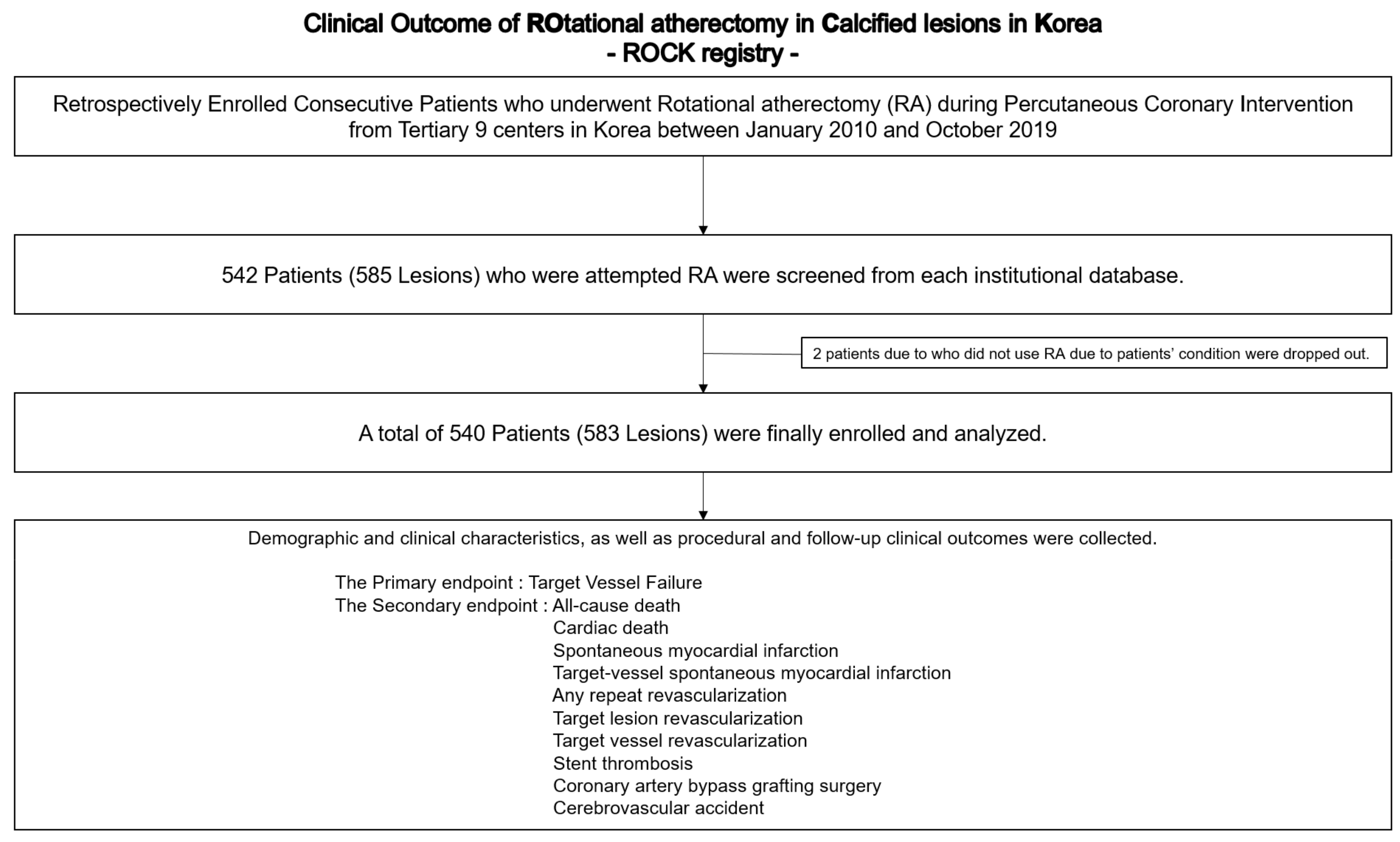
2.1. Study Design and Population
2.2. Procedure
2.3. Study Outcomes
2.4. Statistical Analyses
3. Results
3.1. Baseline Patient, Lesion, and Procedural Characteristics
3.2. Procedural Outcomes
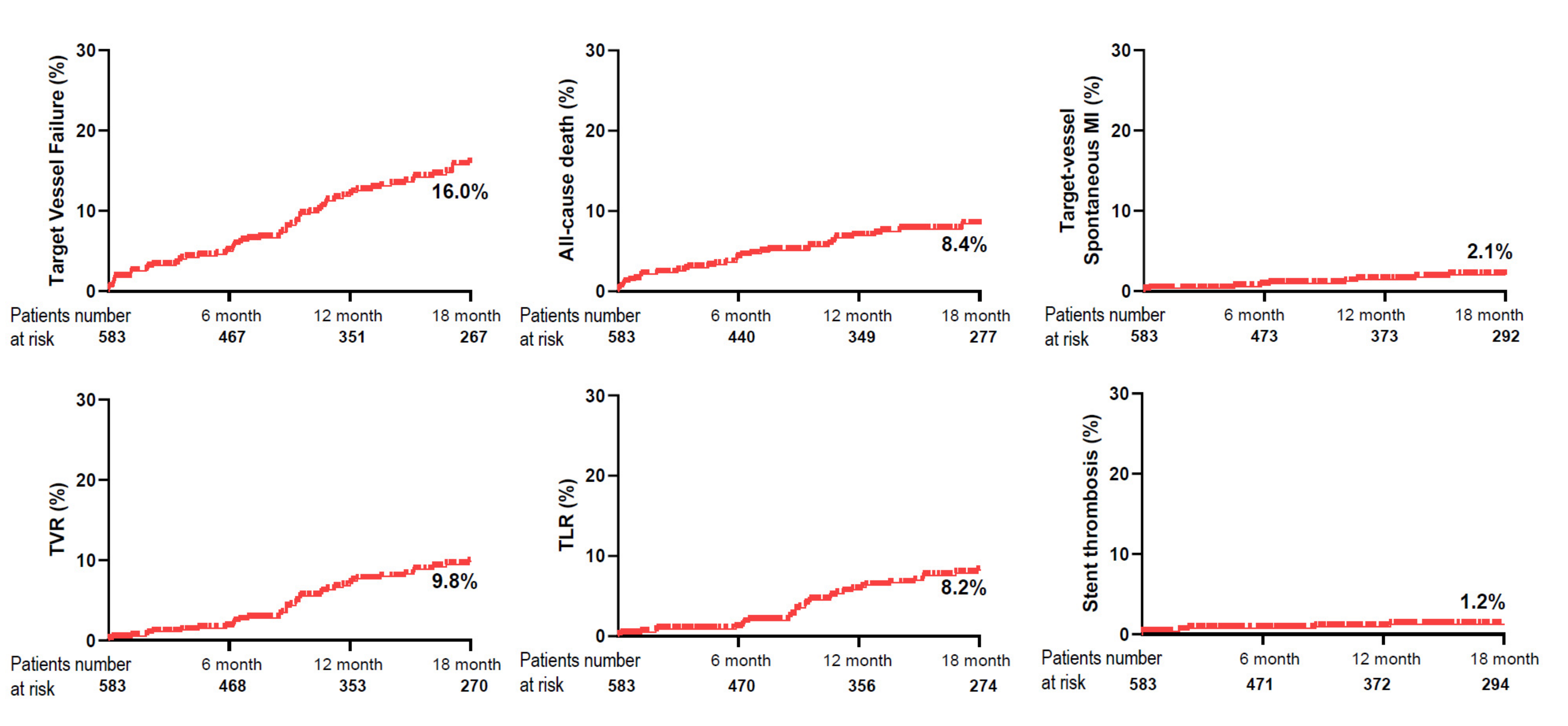
3.3. Clinical Outcomes
3.4. Subgroup Analysis among Patients that Received PCI Successfully According to Clinical Presentation
4. Discussion
Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Characteristics and Long-Term Outcomes of Rotational Atherectomy—J2T Multicenter Registry. Circ. J. Off. J. Jpn. Circ. Soc. 2018, 82, 369–375. [CrossRef] [Green Version]
- Hill, J.M.; Kereiakes, D.J.; Shlofmitz, R.A.; Klein, A.J.; Riley, R.F.; Price, M.J.; Herrmann, H.C.; Bachinsky, W.; Waksman, R.; Stone, G.W. Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Artery Disease. J. Am. Coll. Cardiol. 2020, 76, 2635–2646. [Google Scholar] [CrossRef] [PubMed]
- Barbato, E.; Carrié, D.; Dardas, P.; Fajadet, J.; Gaul, G.; Haude, M.; Khashaba, A.; Koch, K.; Meyer-Gessner, M.; Palazuelos, J.; et al. European expert consensus on rotational atherectomy. EuroIntervention 2015, 11, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Gordin, J.S.; Stone, G.W.; Sharma, S.K.; Saito, S.; Mahmud, E.; Chambers, J.; Généreux, P.; Shlofmitz, R. Orbital and rotational atherectomy during percutaneous coronary intervention for coronary artery calcification. Catheter. Cardiovasc. Interv. 2018, 92, 61–67. [Google Scholar] [CrossRef]
- De Maria, G.L.; Scarsini, R.; Banning, A.P. Management of Calcific Coronary Artery Lesions: Is it Time to Change Our Interventional Therapeutic Approach? JACC Cardiovasc. Interv. 2019, 12, 1465–1478. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.S.; Auth, D.; Marcus, D.R.; Moore, W.S. Removal of focal atheromatous lesions by angioscopically guided high-speed rotary atherectomy: Preliminary experimental observations. J. Vasc. Surg. 1988, 7, 292–300. [Google Scholar] [CrossRef] [Green Version]
- Tomey, M.I.; Kini, A.S.; Sharma, S.K. Current status of rotational atherectomy. JACC Cardiovasc. Interv. 2014, 7, 345–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamekiyo, H.; Hayashi, Y.; Toyofuku, M.; Ueda, H.; Sakuma, T.; Okimoto, T.; Otsuka, M.; Imazu, M.; Kihara, Y. Clinical outcomes of sirolimus-eluting stenting after rotational atherectomy. Circ. J. Off. J. Jpn. Circ. Soc. 2009, 73, 2042–2049. [Google Scholar] [CrossRef] [Green Version]
- Mezilis, N.; Dardas, P.; Ninios, V.; Tsikaderis, D. Rotablation in the drug eluting era: Immediate and long-term results from a single center experience. J. Interv. Cardiol. 2010, 23, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Jinnouchi, H.; Kuramitsu, S.; Shinozaki, T.; Kobayashi, Y.; Hiromasa, T.; Morinaga, T.; Mazaki, T.; Sakakura, K.; Soga, Y.; Hyodo, M.; et al. Two-Year Clinical Outcomes of Newer-Generation Drug-Eluting Stent Implantation Following Rotational Atherectomy for Heavily Calcified Lesions. Circ. J. Off. J. Jpn. Circ. Soc. 2015, 79, 1938–1943. [Google Scholar] [CrossRef] [Green Version]
- Benezet, J.; Díaz de la Llera, L.S.; Cubero, J.M.; Villa, M.; Fernández-Quero, M.; Sánchez-González, A. Drug-eluting stents following rotational atherectomy for heavily calcified coronary lesions: Long-term clinical outcomes. J. Invasive Cardiol. 2011, 23, 28–32. [Google Scholar]
- Abdel-Wahab, M.; Baev, R.; Dieker, P.; Kassner, G.; Khattab, A.A.; Toelg, R.; Sulimov, D.; Geist, V.; Richardt, G. Long-term clinical outcome of rotational atherectomy followed by drug-eluting stent implantation in complex calcified coronary lesions. Catheter. Cardiovasc. Interv. 2013, 81, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. kidney Dis. Off. J. Natl. Kidney Found. 2009, 53, 982–992. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger, C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention, 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease, 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction, 2014 AHA/ACC Guideline for the Management of Patients With Non-ST-Elevation Acute Coronary Syndromes, and 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery. Circulation 2016, 134, e123–e155. [Google Scholar] [CrossRef] [Green Version]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Catheter. Cardiovasc. Interv. 2013, 82, E266–E355. [Google Scholar] [CrossRef] [PubMed]
- Moussa, I.D.; Klein, L.W.; Shah, B.; Mehran, R.; Mack, M.J.; Brilakis, E.S.; Reilly, J.P.; Zoghbi, G.; Holper, E.; Stone, G.W. Consideration of a new definition of clinically relevant myocardial infarction after coronary revascularization: An expert consensus document from the Society for Cardiovascular Angiography and Interventions (SCAI). J. Am. Coll. Cardiol. 2013, 62, 1563–1570. [Google Scholar] [CrossRef] [Green Version]
- 2019 ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Atherosclerosis 2019, 290, 140–205. [CrossRef] [Green Version]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [CrossRef]
- Rathore, S.; Matsuo, H.; Terashima, M.; Kinoshita, Y.; Kimura, M.; Tsuchikane, E.; Nasu, K.; Ehara, M.; Asakura, Y.; Katoh, O.; et al. Rotational atherectomy for fibro-calcific coronary artery disease in drug eluting stent era: Procedural outcomes and angiographic follow-up results. Catheter. Cardiovasc. Interv. 2010, 75, 919–927. [Google Scholar] [CrossRef]
- Kawamoto, H.; Latib, A.; Ruparelia, N.; Ielasi, A.; D’Ascenzo, F.; Pennacchi, M.; Sardella, G.; Garbo, R.; Meliga, E.; Moretti, C.; et al. In-hospital and midterm clinical outcomes of rotational atherectomy followed by stent implantation: The ROTATE multicentre registry. EuroIntervention 2016, 12, 1448–1456. [Google Scholar] [CrossRef]
- Cortese, B.; Aranzulla, T.C.; Godino, C.; Chizzola, G.; Zavalloni, D.; Tavasci, E.; De Benedictis, M.; Ettori, F.; Presbitero, P.; Colombo, A. Drug-eluting stent use after coronary atherectomy: Results from a multicentre experience—The ROTALINK I study. J. Cardiovasc. Med. 2016, 17, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.R.; Calhoon, J.H.; Dehmer, G.J.; Grantham, J.A.; Maddox, T.M.; Maron, D.J.; Smith, P.K. ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 Appropriate Use Criteria for Coronary Revascularization in Patients With Stable Ischemic Heart Disease: A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society of Thoracic Surgeons. J. Am. Coll. Cardiol. 2017, 69, 2212–2241. [Google Scholar] [CrossRef] [PubMed]
- Roffi, M.; Patrono, C.; Collet, J.P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 267–315. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Mean ± SD, n (%) or Median (IQR) (n = 540) |
|---|---|
| Age (years) | 71.4 ± 0.4 |
| Male | 323 (59.8) |
| BMI (kg/m2) | 24.2 ± 3.9 |
| Diabetes mellitus | 305 (56.5) |
| Insulin use | 72 (13.3) |
| Hypertension | 415 (76.9) |
| Hyperlipidemia | 235 (43.5) |
| Current smoker | 103 (19.1) |
| Clinical presentation | |
| Silent ischemia | 37 (6.9) |
| Stable angina | 176 (32.6) |
| Unstable angina | 175 (32.4) |
| NSTEMI | 133 (24.6) |
| STEMI | 19 (3.5) |
| Presented as ACS | 327 (60.6) |
| Chronic kidney disease | 96 (17.8) |
| Prior MI | 66 (12.2) |
| Prior PCI | 138 (25.6) |
| Prior CABG | 24 (4.4) |
| Peripheral vascular disease | 39 (7.2) |
| History of heart failure | 77 (14.3) |
| Atrial fibrillation | 49 (9.1) |
| LV EF, % | 53.0 ± 13.4 |
| Medication at discharge | |
| Aspirin | 529 (98.0) |
| P2Y12 Inhibitor | 530 (98.1) |
| DAPT | 518 (95.9) |
| B-blocker | 381 (70.6) |
| ACEI/ARB | 341 (63.1) |
| Statin | 499 (92.4) |
| NOAC | 17 (2.9) |
| Characteristics | Mean ± SD, n (%) or Median (IQR) (n = 583) |
|---|---|
| ACC/AHA classification | |
| Type B2/C | 59 (10.1)/480 (82.4) |
| Target vessel | |
| LAD | 384 (65.9) |
| LCX | 59 (10.1) |
| RCA | 140 (24.0) |
| LM disease | 82 (14.1) |
| Multivessel disease | 467 (80.1) |
| Femoral approach | 323 (55.4) |
| Treatment type | |
| POBA | 6 (1.0) |
| DEB | 17 (2.9) |
| Stent implantation | 548 (94.0) |
| Failure | 12 (2.0) |
| IVUS or OCT | 268 (46.0) |
| Escalation of Burr | 91 (15.6) |
| Maximum Burr size, mm | |
| 1.25 | 157 (26.9) |
| 1.5 | 308 (52.9) |
| 1.75 | 107 (18.4) |
| 2.0 | 10 (1.7) |
| 2.5 | 1 (0.2) |
| Access size | |
| 5 F | 5 (0.9) |
| 6 F | 215 (36.9) |
| 7 F | 326 (55.9) |
| 8 F | 37 (6.3) |
| Total number of stents | 2.38 ± 1.18 |
| Number of stents (target-vessel) | 1.66 ± 0.68 |
| Mean stent diameter, mm (target-vessel) | 2.99 ± 0.38 |
| Total stent length, mm | 69.02 ± 35.66 |
| Stent length, mm (target-vessel) | 49.48 ± 21.13 |
| Mean ± SD, n (%) or Median (IQR) | |
|---|---|
| Technical success | 562 (96.4) |
| Procedural success | 508 (87.1) |
| Contrast amount, mL | 210 (150–300) |
| Procedure time, min | 63.4 (45.0–97.0) |
| Radiation dose, mGy | 2685 (1512–4800) |
| In-hospital MACCEs | 62 (10.6) |
| In-hospital death | 11 (1.9) |
| Procedure-related myocardial infarction | 46 (7.9) |
| Urgent revascularization | 9 (1.5) |
| In-hospital stroke | 2 (0.3) |
| Procedural Complications | |
| Cardiac tamponade requiring intervention | 3 (0.5) |
| Coronary perforation | 11 (1.9) |
| Severe coronary dissection immediate after RA procedure * | 35 (6.0) |
| Temporary pacemaker during RA procedure | 19 (3.3) |
| Contrast-Induced Nephropathy | 19 (3.3) |
| In-hospital bleeding | 27 (4.6) |
| Univariate | Multivariate * | |||
|---|---|---|---|---|
| Variables | HR (95% CI) | p | HR (95% CI) | p |
| Age | 0.99 (0.97–1.01) | 0.43 | ||
| Male gender | 1.12 (0.74–1.70) | 0.59 | ||
| Current smoker | 1.67 (1.06–2.65) | 0.028 | 1.92 (1.17–3.16) | 0.01 |
| HTN | 0.97 (0.60–1.57) | 0.91 | ||
| Diabetes mellitus | 1.39 (0.91–2.11) | 0.13 | ||
| Hyperlipidemia | 0.59 (0.38–0.92) | 0.018 | ||
| Chronic kidney disease | 2.12 (1.34–3.35) | 0.001 | 1.87 (1.14–3.08) | 0.013 |
| Family history of CAD | 1.50 (0.37–6.11) | 0.57 | ||
| Prior MI | 0.60 (0.28–1.29) | 0.19 | ||
| Prior PCI | 1.10 (0.69–1.73) | 0.70 | ||
| Prior CABG | 0.91 (0.33–2.48) | 0.85 | ||
| History of cerebrovascular attack | 2.15 (1.32–3.50) | 0.002 | 2.14 (1.24–3.68) | 0.006 |
| Peripheral artery disease | 1.69 (0.88–3.25) | 0.12 | ||
| Atrial fibrillation | 1.54 (0.82–2.90) | 0.18 | ||
| LV EF (%) | 0.98 (0.96–0.99) | 0.003 | 0.98 (0.97–0.999) | 0.037 |
| Presented as ACS | 1.61 (1.03–2.51) | 0.035 | 1.54 (0.95–2.51) | 0.08 |
| MVD | 0.95 (0.56–1.61) | 0.86 | ||
| LM disease | 1.68 (1.02–2.75) | 0.041 | 1.94 (1.11–3.37) | 0.019 |
| Mean stent diameter per target vessel | 0.97 (0.55–1.71) | 0.92 | ||
| Total number of stents | 1.23 (1.04–1.44) | 0.014 | 1.19 (0.996–1.41) | 0.06 |
| Total stent length | 1.007 (1.001–1.012) | 0.026 | ||
| All Study Population | Era | Technical Success, % | Follow-Up Duration | All-Cause Death, % | TVR, % | TLR, % | ST, % | CVA, % | |
|---|---|---|---|---|---|---|---|---|---|
| Okai et al. [1] | 1090 | DES | 96.2 | 3.8 (IQR 1.9–6.1) years | 24.2 | 21.4 | 16.2 | 1.3 | 4.7 |
| Kawamoto et al. [20] | 985 | 8.8% BMS91.2% DES | 99.1 | 2 years | 9.5 | 19.8 | 16.6 | 1.8 | 1.0 |
| Cortese et al. [21] | 1397 | 17% POBA40.7% BMS42% DES | 99.3 | 2.4 (0.8–5.7) years | 6.4 | - | 11.7 | 1.4 | - |
| Rathore et al. [19] | 516 | 24.2% BMS75.8% DES | 99.4 | 6–9 months | - | - | 14.4 | 0.8 * | - |
| Abdel-Wahab et al. [12] | 205 | DES | 98.0 | 1.3 (0.08–7) years | 9.0 | 11.2 | 7.9 | 1.0 | - |
| Our study ** | 540 | DES | 96.4 | 1.5 (IQR 0.7–2.9) years | 8.4 | 9.8 | 8.2 | 1.2 | 2.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.; Jung, J.-h.; Lee, M.; Kim, D.-W.; Park, M.-W.; Choi, I.-J.; Lee, J.-H.; Lee, J.-H.; Lee, S.-R.; Lee, P.-H.; et al. Clinical Outcome of Rotational Atherectomy in Calcified Lesions in Korea-ROCK Registry. Medicina 2021, 57, 694. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070694
Lee K, Jung J-h, Lee M, Kim D-W, Park M-W, Choi I-J, Lee J-H, Lee J-H, Lee S-R, Lee P-H, et al. Clinical Outcome of Rotational Atherectomy in Calcified Lesions in Korea-ROCK Registry. Medicina. 2021; 57(7):694. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070694
Chicago/Turabian StyleLee, Kyusup, Ji-hoon Jung, Myunhee Lee, Dae-Won Kim, Mahn-Won Park, Ik-Jun Choi, Jae-Hwan Lee, Jang-Hoon Lee, Sang-Rok Lee, Pil-Hyung Lee, and et al. 2021. "Clinical Outcome of Rotational Atherectomy in Calcified Lesions in Korea-ROCK Registry" Medicina 57, no. 7: 694. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070694