
The Prospect of Lactoferrin Use as Adjunctive Agent in Management of SARS-CoV-2 Patients: A Randomized Pilot Study

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Dhama, K.; Sharun, K.; Tiwari, R.; Sircar, S.; Bhat, S.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Coronavirus Disease 2019—COVID-19. Clin. Microbiol. Rev. 2020, 33, e00028-20. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus (COVID-19) Events as They Happen. 2020. Available online: https://www.who.int/emergencies/diseases/novelcoronavirus-2019/events-as-they-happen (accessed on 15 December 2020).
- Zhavoronkov, A.; Aladinskiy, V.; Zhebrak, A.; Zagribelnyy, B.; Terentiev, V.; Bezrukov, D.S.; Polykovskiy, D.; Shayakhmetov, R.; Filimonov, A.; Orekhov, P.; et al. Potential COVID-2019 3C-Like Protease Inhibitors Designed Using Generative Deep Learning Approaches; American Chemical Society (ACS): Washington, DC, USA, 2020. [Google Scholar]
- Angeletti, S.; Benvenuto, D.; Bianchi, M.; Giovanetti, M.; Pascarella, S.; Ciccozzi, M. COVID-2019: The role of the nsp2 and nsp3 in its pathogenesis. J. Med. Virol. 2020, 92, 584–588. [Google Scholar] [CrossRef] [Green Version]
- Costagliola, G.; Spada, E.; Comberiati, P.; Peroni, D.G. Could nutritional supplements act as therapeutic adjuvants in COVID-19? Ital. J. Pediatr. 2021, 47, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Cao, L.; Gao, H.; Wu, Y.; Wang, Y.; Fang, F.; Rao, Y. Discovery, optimization, and target identi-fication of novel potent broad-spectrum antiviral inhibitors. J. Med. Chem. 2019, 62, 4056–4073. [Google Scholar] [CrossRef]
- Feng, M.; Fei, S.; Xia, J.; Labropoulou, V.; Swevers, L.; Sun, J. Antimicrobial Peptides as Potential Antiviral Factors in Insect Antiviral Immune Response. Front. Immunol. 2020, 11. [Google Scholar] [CrossRef]
- Sienkiewicz, M.; Jaśkiewicz, A.; Tarasiuk, A.; Fichna, J. Lactoferrin: An overview of its main functions, immunomodulatory and antimicrobial role, and clinical significance. Crit. Rev. Food Sci. Nutr. 2021, 1–18. [Google Scholar] [CrossRef]
- Buey, B.; Bellés, A.; Latorre, E.; Abad, I.; Pérez, M.D.; Grasa, L.; Sánchez, L. Comparative effect of bovine buttermilk, whey, and lactoferrin on the innate immunity receptors and oxidative status of intestinal epithelial cells. Biochem. Cell Biol. 2021, 99, 54–60. [Google Scholar] [CrossRef]
- Wang, B.; Timilsena, Y.P.; Blanch, E.; Adhikari, B. Lactoferrin: Structure, function, denaturation and digestion. Crit. Rev. Food Sci. Nutr. 2019, 59, 580–596. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, P.; Wang, H.; Luo, Y.; Wan, L.; Jiang, M.; Chu, Y. Lactoferrin for the treatment of COVID-19. Exp. Ther. Med. 2020, 20, 1. [Google Scholar]
- Serrano, G.; Kochergina, I.; Albors, A.; Diaz, E.; Oroval, M.; Hueso, G.; Serrano, J.M. Liposomal Lactoferrin as Potential Preventative and Cure for COVID-19. Int. J. Res. Health Sci. 2020, 8, 8–15. [Google Scholar] [CrossRef]
- Azhar, J.; Mohammadabadi, T.; Babar, M.E.; Hussain, T. Milk lactoferrin: A probable immunological agent against sars-cov-2: A review. Basrah J. Agric. Sci. 2020, 33, 138–146. [Google Scholar] [CrossRef]
- Hao, L.; Shan, Q.; Wei, J.; Ma, F.; Sun, P. Lactoferrin: Major Physiological Functions and Applications. Curr. Protein Pept. Sci. 2019, 20, 139–144. [Google Scholar] [CrossRef]
- Khajeh, E.; Jamshidian-Mojaver, M.; Naeemipour, M.; Farzin, H. The Identification of a Novel Peptide Derived from Lactoferrin Isolated from Camel Milk with Potential Antimicrobial Activity. Iran. J. Med. Microbiol. 2021, 15, 302–316. [Google Scholar]
- Kell, D.B.; Heyden, E.L.; Pretorius, E. The biology of lactoferrin, an iron-binding protein that can help de-fend against viruses and bacteria. Front. Immunol. 2020, 11, 1221. [Google Scholar] [CrossRef]
- Quintieri, L.; Caputo, L.; Monaci, L.; Cavalluzzi, M.M.; Denora, N. Lactoferrin-derived peptides as a con-trol strategy against skinborne staphylococcal biofilms. Biomedicines 2020, 8, 323. [Google Scholar] [CrossRef]
- Farid, A.; El Shemy, M.A.; Nafie, E.; Hegazy, A.M.; Abdelhiee, E.Y. Anti-inflammatory, anti-oxidant and hepatoprotective effects of lactoferrin in rats. Drug Chem. Toxicol. 2021, 44, 286–293. [Google Scholar] [CrossRef]
- Shahidi, F.; Roshanak, S.; Javadmanesh, A.; Yazdi, F.T.; Pirkhezranian, Z.; Azghandi, M. Evaluation of antimicrobial properties of bovine lactoferrin against foodborne pathogenic microorganisms in planktonic and bio-film forms (in vitro). J. Consum. Prot. Food Saf. 2020, 15, 277–283. [Google Scholar] [CrossRef]
- Padrão, J.; Ribeiro, S.; Lanceros-Méndez, S.; Rodrigues, L.R.; Dourado, F. Effect of bacterial nanocellulose binding on the bactericidal activity of bovine lactoferrin. Heliyon 2020, 6, e04372. [Google Scholar] [CrossRef]
- Lodhi, A.M.; Aslam, P.; Sajid, K.; Zulfiqar, K. Lactoferrin as Nutraceutical Protein from Milk. J. Nutraceuticals Food Sci. 2019, 4, 5. [Google Scholar]
- Peroni, D.G. Viral infections: Lactoferrin, a further arrow in the quiver of prevention. J. Pediat. Neonatal Individ. Med. (JPNIM) 2020, 9, e090142. [Google Scholar]
- Hu, Y.; Meng, X.; Zhang, F.; Xiang, Y.; Wang, J. The in vitro antiviral activity of lactoferrin against common human coronaviruses and SARS-CoV-2 is mediated by targeting the heparan sulfate co-receptor. Emerg. Microbes Infect. 2021, 10, 317–330. [Google Scholar] [CrossRef]
- Campione, E.; Lanna, C.; Cosio, T.; Rosa, L.; Conte, M.P.; Iacovelli, F.; Romeo, A.; Falconi, M.; del Vecchio, C.; Franchin, E.; et al. Lactoferrin as Potential Supplementary Nutraceutical Agent in COVID-19 Patients: In vitro and in vivo Preliminary Evidences. BioRxiv 2020. [Google Scholar] [CrossRef]
- World Health Organization. Laboratory Testing for 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases: Interim Guidance, 14 January 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Xu, Y.-H.; Dong, J.-H.; An, W.-M.; Lv, X.-Y.; Yin, X.-P.; Zhang, J.-Z.; Dong, L.; Ma, X.; Zhang, H.-J.; Gao, B.-L. Clinical and computed tomographic imaging features of novel coronavirus pneumonia caused by SARS-CoV-2. J. Infect. 2020, 80, 394–400. [Google Scholar] [CrossRef] [Green Version]
- Sorour, K.; El-Menshawy, H. A Proposed Protocol for the Management of COVID-19 in Egypt. AfricArXiv 2020. [Google Scholar] [CrossRef]
- Elmenam, H.S.; Farouk, M.H. Bovine lactoferrin in preterm labor with sterile inflammation. Sci. J. Al-Azhar Med. Fac. Girls 2021, 5, 299. [Google Scholar]
- Sullivan, L.M.; Weinberg, J.; Keaney, J.F., Jr. Common statistical pitfalls in basic science research. J. Am. Heart Assoc. 2016, 5, e004142. [Google Scholar] [CrossRef]
- Chang, R.; Ng, T.B.; Sun, W.-Z. Lactoferrin as potential preventative and adjunct treatment for COVID-19. Int. J. Antimicrob. Agents 2020, 56, 106118. [Google Scholar] [CrossRef]
- Salaris, C.; Scarpa, M.; Elli, M.; Bertolini, A.; Guglielmetti, S.; Pregliasco, F.; Castagliuolo, I. Protective effects of lactoferrin against SARS-CoV-2 infection in vitro. Nutrients 2021, 13, 328. [Google Scholar] [CrossRef]
- Niaz, B.; Saeed, F.; Ahmed, A.; Imran, M.; Maan, A.A.; Khan, M.K.I.; Tufail, T.; Anjum, F.M.; Hussain, S.; Suleria, H.A.R. Lactoferrin (LF): A natural antimicrobial protein. Int. J. Food Prop. 2019, 22, 1626–1641. [Google Scholar] [CrossRef] [Green Version]
- Kruzel, M.L.; Olszewska, P.; Pazdrak, B.; Krupinska, A.M.; Actor, J.K. New insights into the systemic effects of oral lactoferrin: Transcriptome profiling. Biochem. Cell Biol. 2021, 99, 47–53. [Google Scholar] [CrossRef]
- Cavezzi, A.; Troiani, E.; Corrao, S. COVID-19: Hemoglobin, Iron, and Hypoxia beyond Inflammation. A Narrative Review. Clin. Pract. 2020, 10, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Anurag, A.; Jha, P.K.; Kumar, A. Differential white blood cell count in the COVID-19: A cross-sectional study of 148 patients. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 2099–2102. [Google Scholar] [CrossRef] [PubMed]
- Wool, G.D.; Miller, J.L. The Impact of COVID-19 Disease on Platelets and Coagulation. Pathobiology 2021, 88, 15–27. [Google Scholar] [CrossRef]
- Cutone, A.; Ianiro, G.; Lepanto, M.S.; Rosa, L.; Valenti, P.; Bonaccorsi di Patti, M.C.; Musci, G. Lactoferrin in the Prevention and Treatment of Intestinal Inflammatory Pathologies Associated with Colorectal Cancer Development. Cancers 2020, 12, 3806. [Google Scholar] [CrossRef] [PubMed]
- El-Khawaga, A.; Abdelmaksoud, H. Effect of Lactoferrin Supplementation on Iron Deficiency Anemia in Primary School Children. Int. J. Med. Arts 2019. [Google Scholar] [CrossRef]
- Cai, Q.; Huang, D.; Yu, H.; Zhu, Z.; Xia, Z.; Su, Y.; Li, Z.; Zhou, G.; Gou, J.; Qu, J.; et al. COVID-19: Abnormal liver function tests. J. Hepatol. 2020, 73, 566–574. [Google Scholar] [CrossRef]
- Bertolini, A.; Van De Peppel, I.P.; Bodewes, F.A.; Moshage, H.; Fantin, A.; Farinati, F.; Fiorotto, R.; Jonker, J.W.; Strazzabosco, M.; Verkade, H.J.; et al. Abnormal Liver Function Tests in Patients with COVID-19: Relevance and Potential Pathogenesis. Hepatology 2020, 72, 1864–1872. [Google Scholar] [CrossRef]
- Bajwa, H.; Riaz, Y.; Ammar, M.; Farooq, S.; Yousaf, A. The Dilemma of Renal Involvement in COVID-19: A Systematic Review. Cureus 2020, 12, e8632. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-M.; Xie, J.; Chen, M.-M.; Zhang, X.; Cheng, X.; Li, H.; Zhou, F.; Qin, J.-J.; Lei, F.; Chen, Z.; et al. Kidney Function Indicators Predict Adverse Outcomes of COVID-19. Med 2021, 2, 38–48.e2. [Google Scholar] [CrossRef]
- Hsu, Y.-H.; Chiu, I.-J.; Lin, Y.-F.; Chen, Y.-J.; Lee, Y.-H.; Chiu, H.-W. Lactoferrin Contributes a Renoprotective Effect in Acute Kidney Injury and Early Renal Fibrosis. Pharmaceutics 2020, 12, 434. [Google Scholar] [CrossRef]
- Wang, G.; Wu, C.; Zhang, Q.; Wu, F.; Yu, B.; Lv, J.; Li, Y.; Li, T.; Zhang, S.; Wu, C.; et al. C-Reactive Protein Level May Predict the Risk of COVID-19 Aggravation. Open Forum Infect. Dis. 2020, 7, ofaa153. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Li, H.; Li, L.; Liu, C.; Yan, S.; Chen, H.; Li, Y. Ferritin in the coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. J. Clin. Lab. Anal. 2020, 34, e23618. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; Aggarwal, G.; Wong, J.; Benoit, S.; Vikse, J.; Plebani, M.; Lippi, G. Lactate dehydrogenase levels predict coronavirus disease 2019 (COVID-19) severity and mortality: A pooled analysis. Am. J. Emerg. Med. 2020, 38, 1722–1726. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Control Group | Group I | Group II | p-Value |
|---|---|---|---|---|
| Age (years) (mean ± SD) | 48.93 ± 9.4 | 49.07 ± 8.5 | 47.87 ± 11.3 | - |
| Female Sex, n (%) | 10 (55.6%) | 5 (27.8%) | 7 (38.9%) | - |
| Male Sex, n (%) | 8 (44.4%) | 13 (72.2%) | 11 (61.1%) | - |
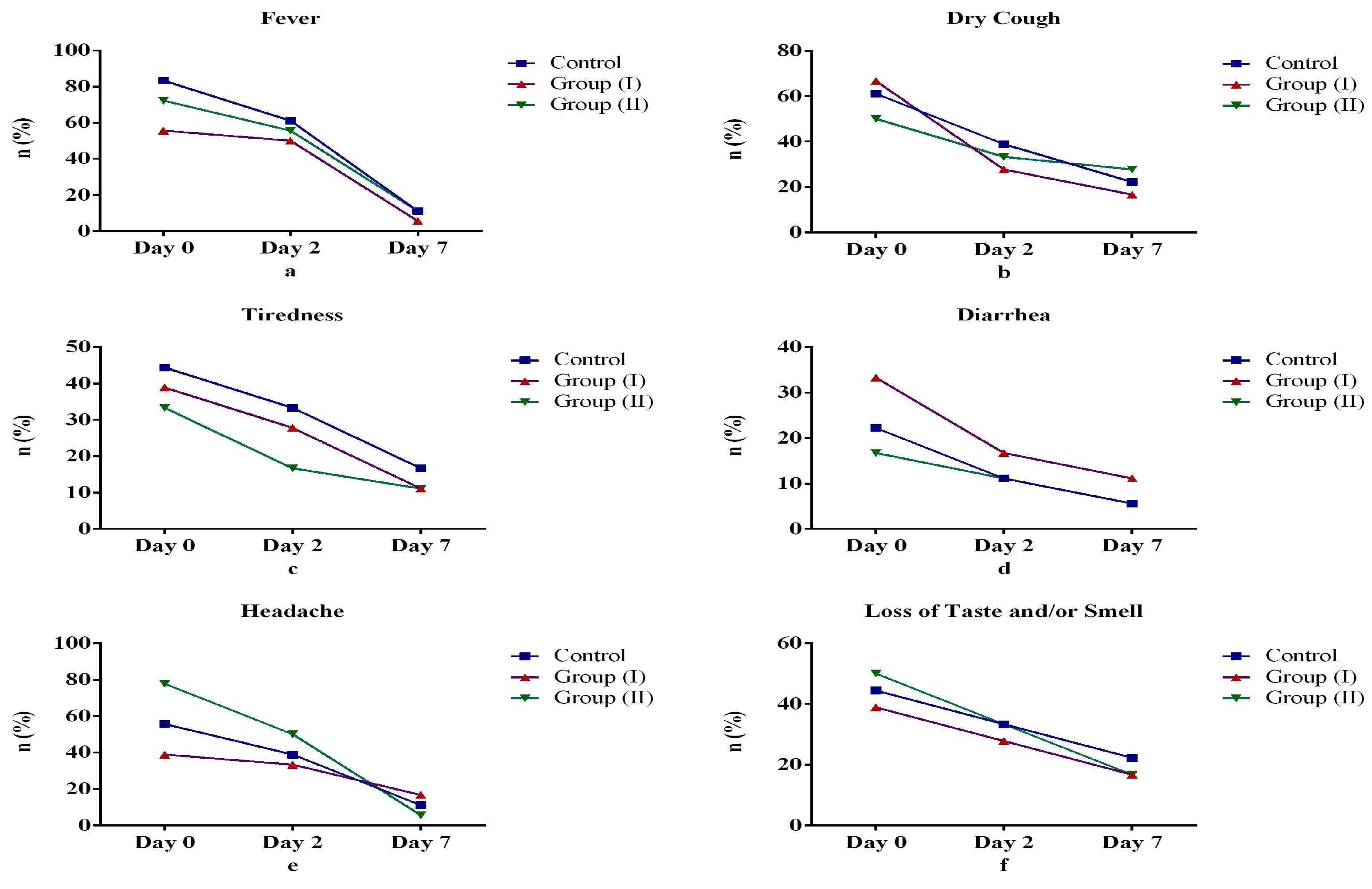
| Fever | ||||
| Day 0 | 15 (83.3%) | 10 (55.6%) | 13 (72.2%) | 0.185 |
| Day 2 | 11 (61.1%) | 9 (50.0%) | 10 (55.6%) | 0.799 |
| Day 7 | 2 (11.1%) | 1 (5.6%) | 2 (11.1%) | 0.802 |
| Dry Cough | ||||
| Day 0 | 11 (61.1%) | 12 (66.7%) | 9 (50.0%) | 0.585 |
| Day 2 | 7 (38.9%) | 5 (27.8%) | 6 (33.3%) | 0.779 |
| Day 7 | 4 (22.2%) | 3 (16.7%) | 5 (27.8%) | 0.725 |
| Tiredness | ||||
| Day 0 | 8 (44.4%) | 7 (38.9%) | 6 (33.3%) | 0.792 |
| Day 2 | 6 (33.3%) | 5 (27.8%) | 3 (16.7%) | 0.509 |
| Day 7 | 3 (16.7%) | 2 (11.1%) | 2 (11.1%) | 0.849 |
| Diarrhea | ||||
| Day 0 | 4 (22.2%) | 6 (33.3%) | 3 (16.7%) | 0.492 |
| Day 2 | 2 (11.1%) | 3 (16.7%) | 2 (11.1%) | 0.849 |
| Day 7 | 1 (5.6%) | 2 (11.1%) | 1 (5.6%) | 0.763 |
| Headache | ||||
| Day 0 | 10 (55.6%) | 12 (38.9%) | 14 (77.8%) | 0.368 |
| Day 2 | 7 (38.9%) | 6 (33.3%) | 9 (50.0%) | 0.585 |
| Day 7 | 2 (11.1%) | 3 (16.7%) | 1 (5.6%) | 0.570 |
| Loss of Taste and/or Smell | ||||
| Day 0 | 8 (44.4%) | 7 (38.9%) | 9 (50.0%) | 0.799 |
| Day 2 | 6 (33.3%) | 5 (27.8%) | 6 (33.3%) | 0.918 |
| Day 7 | 4 (22.2%) | 3 (16.7%) | 3 (16.7%) | 0.885 |
| Variables | Control Group | Group I | Group II | p-Value |
|---|---|---|---|---|
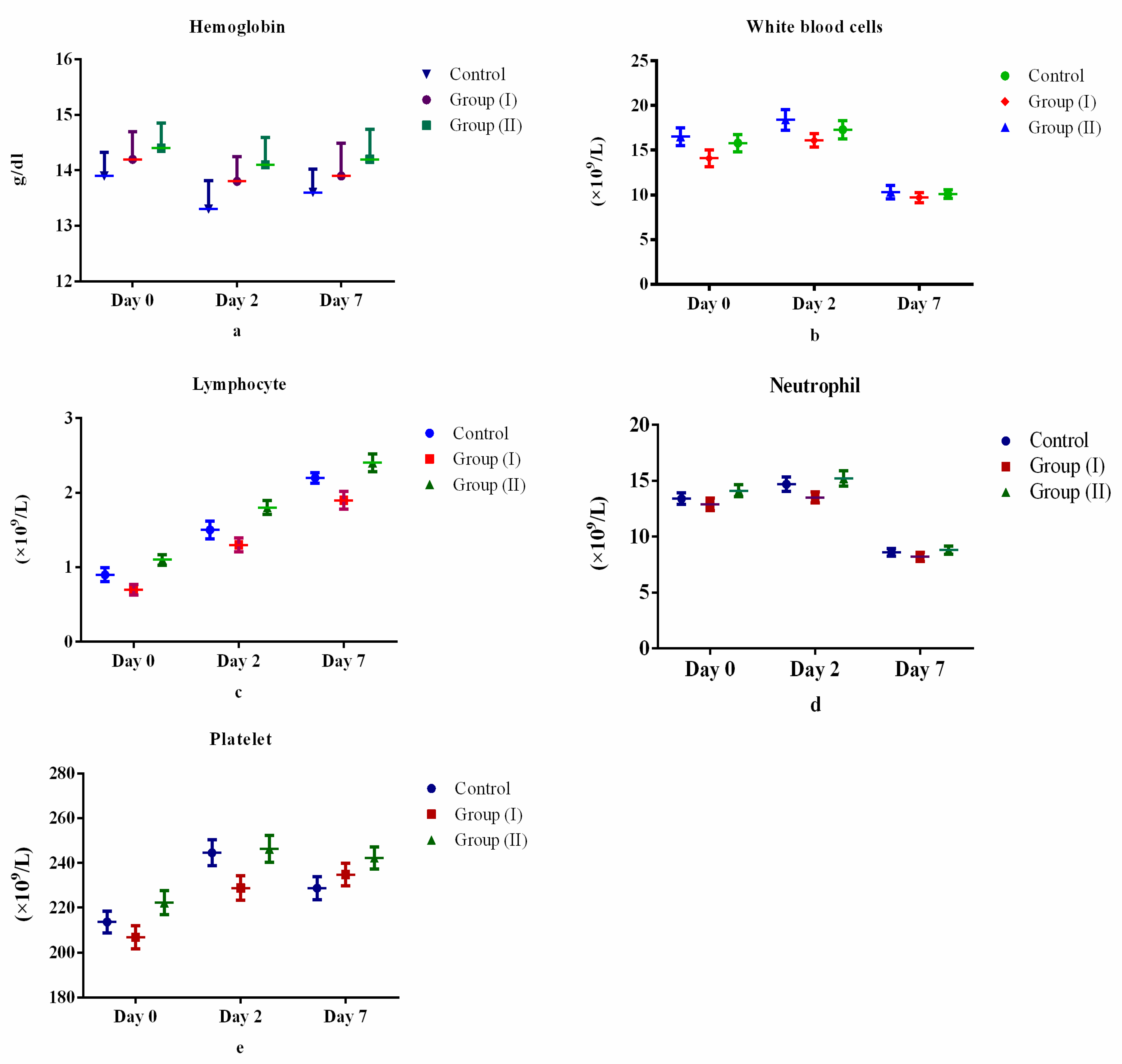
| Hemoglobin (g/dL) | ||||
| Day 0 | 13.9 ± 2.2 | 14.2 ± 1.9 | 14.4 ± 2.1 | 0.797 |
| Day 2 | 13.3 ± 1.8 | 13.8 ± 2.5 | 14.1 ± 1.9 | 0.474 |
| Day 7 | 13.6 ± 1.8 | 13.9 ± 2.1 | 14.2 ± 2.3 | 0.657 |
| White blood cells (×109/L) | ||||
| Day 0 | 15.8 ± 4.1 | 14.1 ± 3.9 | 16.5 ± 4.2 | 0.215 |
| Day 2 | 17.3 ± 4.3 | 16.1 ± 3.2 | 18.4 ± 4.8 | 0.254 |
| Day 7 | 10.1 ± 2.1 | 9.7 ± 2.5 | 10.3 ± 3.2 | 0.786 |
| Lymphocyte (×109/L) | ||||
| Day 0 | 0.9 ± 0.4 | 0.7 ± 0.3 | 1.1 ± 0.3 | 0.005 |
| Day 2 | 1.5 ± 0.5 | 1.3 ± 0.4 | 1.8 ± 0.4 | 0.003 |
| Day 7 | 2.2 ± 0.3 | 1.9 ± 0.5 | 2.4 ± 0.5 | 0.002 |
| Neutrophil (×109/L) | ||||
| Day 0 | 13.4 ± 2.2 | 12.9 ± 2.4 | 14.1 ± 2.3 | 0.311 |
| Day 2 | 14.7 ± 2.7 | 13.5 ± 2.1 | 15.2 ± 2.9 | 0.139 |
| Day 7 | 8.6 ± 1.5 | 8.2 ± 1.7 | 8.8 ± 1.5 | 0.58 |
| Platelet (×109/L) | ||||
| Day 0 | 213.6 ± 20.5 | 206.8 ± 21.5 | 222.2 ± 99.7 | 0.744 |
| Day 2 | 244.5 ± 24.5 | 234.5 ± 21.1 | 246.2 ± 99.5 | 0.822 |
| Day 7 | 228.7 ± 21.5 | 216.3 ± 23.4 | 242.2 ± 91.8 | 0.392 |
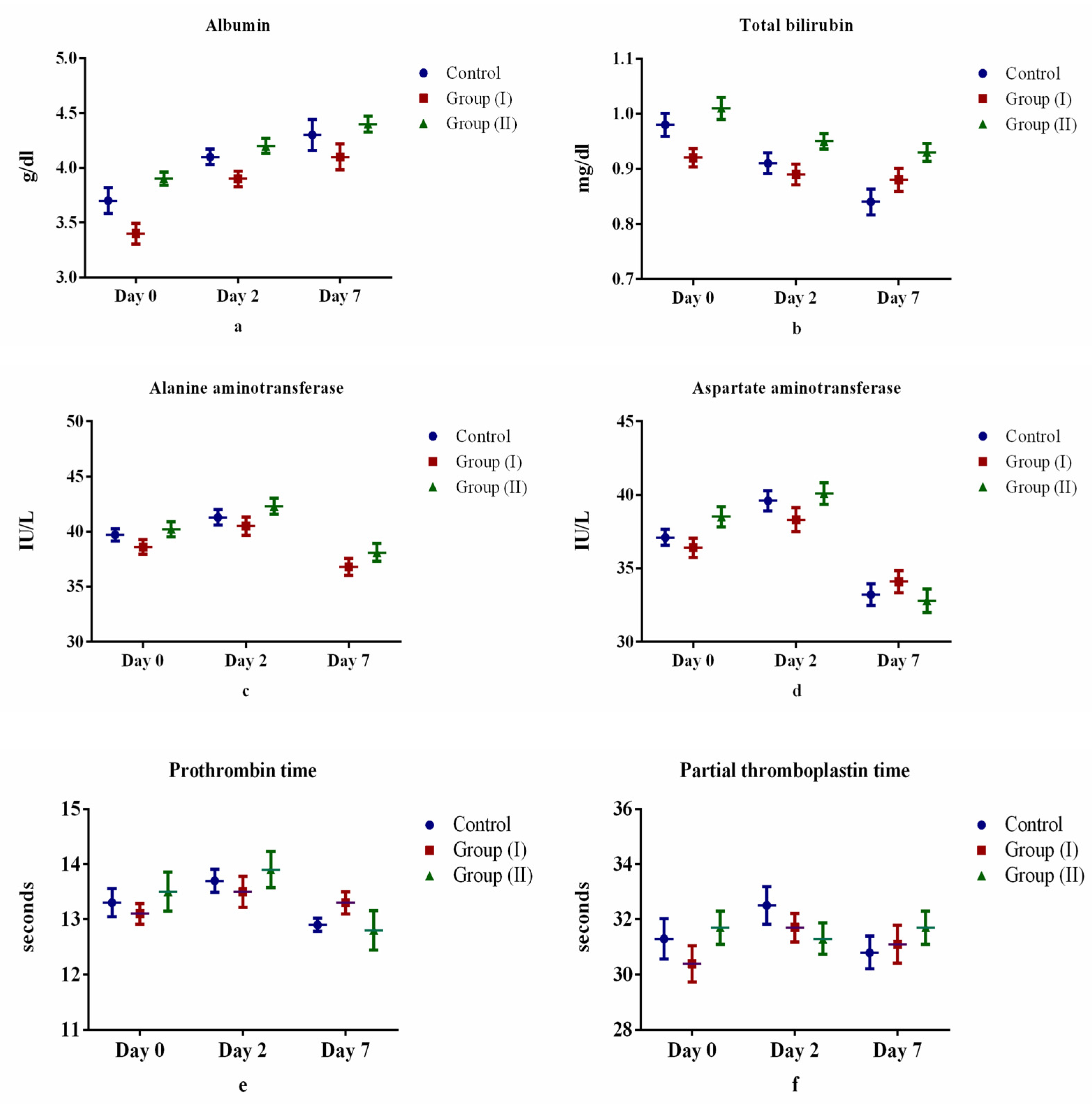
| Albumin (g/dL) | ||||
| Day 0 | 3.7 ± 0.5 | 3.4 ± 0.4 | 3.9 ± 0.2 | 0.006 |
| Day 2 | 4.1 ± 0.3 | 3.9 ± 0.3 | 4.2 ± 0.3 | 0.014 |
| Day 7 | 4.3 ± 0.6 | 4.1 ± 0.5 | 4.4 ± 0.3 | 0.22 |
| Total bilirubin (mg/dL) | ||||
| Day 0 | 0.98 ± 0.1 | 0.92 ± 04 | 1.01 ± 0.2 | 0.559 |
| Day 2 | 0.91 ± 0.1 | 0.89 ± 0.1 | 0.95 ± 0.3 | 0.592 |
| Day 7 | 0.84 ± 0.2 | 0.88 ± 0.3 | 0.93 ± 0.1 | 0.334 |
| Alanine aminotransferase (IU/L) | ||||
| Day 0 | 39.7 ± 2.3 | 38.6 ± 2.8 | 40.2 ± 2.9 | 0.163 |
| Day 2 | 41.3 ± 2.9 | 40.5 ± 3.5 | 42.3 ± 3.1 | 0.208 |
| Day 7 | 37.5 ± 3.1 | 36.8 ± 3.2 | 38.1 ± 3.4 | 0.454 |
| Aspartate aminotransferase (IU/L) | ||||
| Day 0 | 37.1 ± 2.9 | 36.4 ± 3.5 | 38.5 ± 3.1 | 0.139 |
| Day 2 | 39.6 ± 2.3 | 38.3 ± 2.8 | 40.1 ± 2.9 | 0.103 |
| Day 7 | 33.2 ± 3.1 | 34.1 ± 3.2 | 32.8 ± 3.4 | 0.456 |
| Prothrombin time (seconds) | ||||
| Day 0 | 13.3 ± 1.1 | 13.1 ± 0.8 | 13.5 ± 1.5 | 0.536 |
| Day 2 | 13.7 ± 0.9 | 13.5 ± 1.2 | 13.9 ± 1.4 | 0.484 |
| Day 7 | 12.9 ± 0.5 | 13.3 ± 0.9 | 12.8 ± 1.5 | 0.044 |
| Partial thromboplastin time (seconds) | ||||
| Day 0 | 31.3 ± 3.1 | 30.4 ± 2.8 | 31.3 ± 2.4 | 0.577 |
| Day 2 | 32.5 ± 2.9 | 31.7 ± 2.2 | 31.7 ± 2.5 | 0.575 |
| Day 7 | 30.8 ± 2.5 | 31.1 ± 2.9 | 29.7 ± 2.3 | 0.23 |
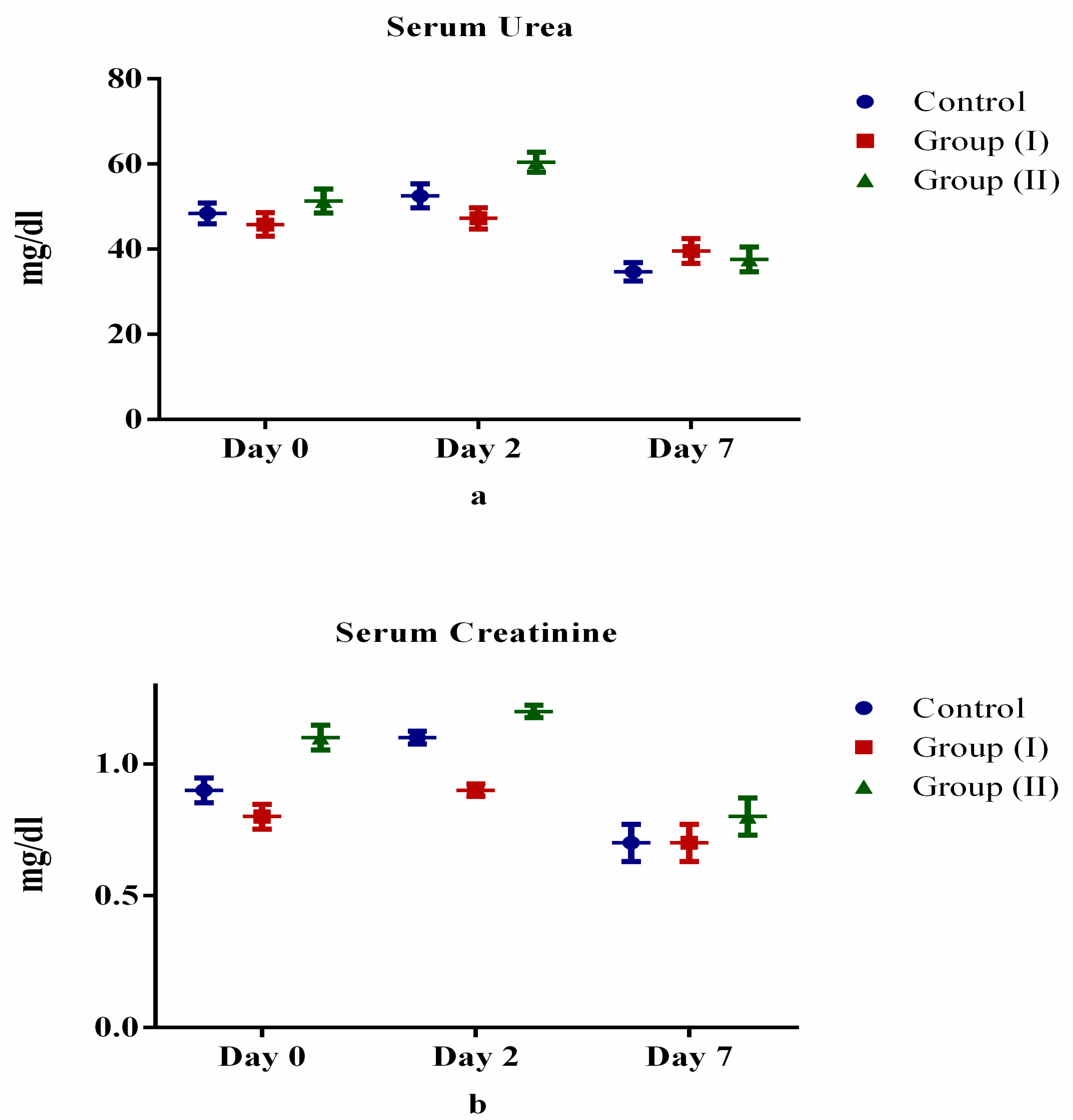
| Serum urea (mg/dL) | ||||
| Day 0 | 48.4 ± 10.3 | 45.8 ± 11.8 | 51.3 ± 11.9 | 0.243 |
| Day 2 | 52.5 ± 11.9 | 47.2 ± 10.5 | 60.4 ± 10.1 | 0.002 |
| Day 7 | 34.7 ± 9.1 | 39.6 ± 12.2 | 37.6 ± 12.4 | 0.444 |
| Serum creatinine (mg/dL) | ||||
| Day 0 | 0.9 ± 0.2 | 0.8 ± 0.2 | 1.1 ± 0.2 | 0.000 |
| Day 2 | 1.1 ± 0.1 | 0.9 ± 0.1 | 1.2 ± 0.1 | 0.000 |
| Day 7 | 0.7 ± 0.3 | 0.7 ± 0.3 | 0.8 ± 0.3 | 0.349 |
| C-reactive protein (mg/L) | ||||
| Day 0 | 10.2 ± 1.2 | 9.8 ± 1.4 | 10.4 ± 1.3 | 0.368 |
| Day 2 | 14.3 ± 1.7 | 12.4 ± 1.1 | 12.9 ± 1.9 | 0.003 |
| Day 7 | 12.8 ± 1.1 | 11.7 ± 1.1 | 10.6 ± 1.1 | 0.000 |
| Ferritin (ng/mL) | ||||
| Day 0 | 488.9 ± 83.6 | 443.1 ± 110.3 | 501.1 ± 101.8 | 0.195 |
| Day 2 | 516.3 ± 90.2 | 524.6 ± 100.6 | 531 ± 95.1 | 0.898 |
| Day 7 | 306.3 ± 71.6 | 323 ± 90.3 | 341.5 ± 80.7 | 0.436 |
| Lactate dehydrogenase (U/L) | ||||
| Day 0 | 369.3 ± 81.2 | 344.6 ± 110.8 | 391.2 ± 100.4 | 0.382 |
| Day 2 | 414.4 ± 90.1 | 384.2 ± 100.6 | 403.5 ± 95.9 | 0.647 |
| Day 7 | 236.8 ± 70.3 | 229.5 ± 90.4 | 231.4 ± 80.7 | 0.961 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Algahtani, F.D.; Elabbasy, M.T.; Samak, M.A.; Adeboye, A.A.; Yusuf, R.A.; Ghoniem, M.E. The Prospect of Lactoferrin Use as Adjunctive Agent in Management of SARS-CoV-2 Patients: A Randomized Pilot Study. Medicina 2021, 57, 842. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080842
Algahtani FD, Elabbasy MT, Samak MA, Adeboye AA, Yusuf RA, Ghoniem ME. The Prospect of Lactoferrin Use as Adjunctive Agent in Management of SARS-CoV-2 Patients: A Randomized Pilot Study. Medicina. 2021; 57(8):842. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080842
Chicago/Turabian StyleAlgahtani, Fahad Dhafer, Mohamed Tharwat Elabbasy, Mai A. Samak, Adeniyi A. Adeboye, Rafeek A. Yusuf, and Mohamed E. Ghoniem. 2021. "The Prospect of Lactoferrin Use as Adjunctive Agent in Management of SARS-CoV-2 Patients: A Randomized Pilot Study" Medicina 57, no. 8: 842. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080842