1. Introduction
The normal umbilical cord (UC) contains one umbilical vein which carries oxygenated blood and two umbilical arteries; the three vessels are surrounded throughout the whole length of the UC by a gelatinous tissue called Wharton’s jelly. The normal insertion of the UC is central or slightly eccentric, directly into the placental disk at one end and the umbilicus on the fetal abdominal wall at the other end. The average length of the umbilical cord at term is approximately 55 cm (increasing with advancing gestational age, from a mean of 32 cm at 20 weeks gestation to 60 cm at term) [
1]. The average diameter and circumference of the UC in a normal term infant are 1.5 and 3.6 cm, respectively.
Wharton’s jelly is a specialized connective tissue composed of myofibroblasts and extracellular matrix—proteoglycans, glycosaminoglycans, and hyaluronic acid—with the primary function of protecting the umbilical blood vessels [
2]. This structure neutralizes the external pressure influence on blood flow between the placenta and fetus, promoting adequate blood flow to the fetus in cases of umbilical cord compression during pregnancy or delivery [
3].
After delivery, all placentas should undergo a basic examination including color, length of the umbilical cord, thickness, number of cord vessels and weight of the placental disk. Complete gross and histopathologic examination of the placenta should be obtained when clinically indicated by adverse maternal, fetal or neonatal outcomes [
4]. Some findings have no clinical significance, but some structural changes are strongly associated with intrauterine growth restriction, fetal death, fetal distress in labor and increased incidence of cesarean delivery [
5]. A thin umbilical cord is a result of a deficiency of Wharton’s jelly. The vessels in a thin cord are more vulnerable to compression, which may explain the association between thin umbilical cords and intrauterine growth restriction and abnormal intrapartum fetal heart rate tracings [
6]. The loss of protection by Wharton’s jelly can lead to compromised fetoplacental circulation and subsequent fetal death [
7]. The complete or segmental absence of Wharton’s jelly is a very rare abnormality, with only a few cases reported in the literature.
The aim of this paper is to report a case where the absence of Wharton’s jelly was diagnosed postnatally in the setting of an abnormal labor with persistent modified CTG traces. A literature review of published cases of the absence of Wharton’s jelly is included.
2. Case Report
We present the case of a 29-year-old nulliparous, 39-week pregnant woman who was hospitalized for irregular contractions in early labor, no ruptured membranes, no bleeding and very good fetal movements. The pregnancy follow-up was uneventful, with both first and second-trimester anomaly scans within normal limits. There was no other associated pathological medical history. Clinical examination and vital signs were normal. At the ultrasound examination, the placenta was high posterior, there was normal amniotic volume, cephalic presentation and active fetal movements, and estimated fetal growth of 3500 g with normal umbilical, cerebral and uterine arteries doppler.
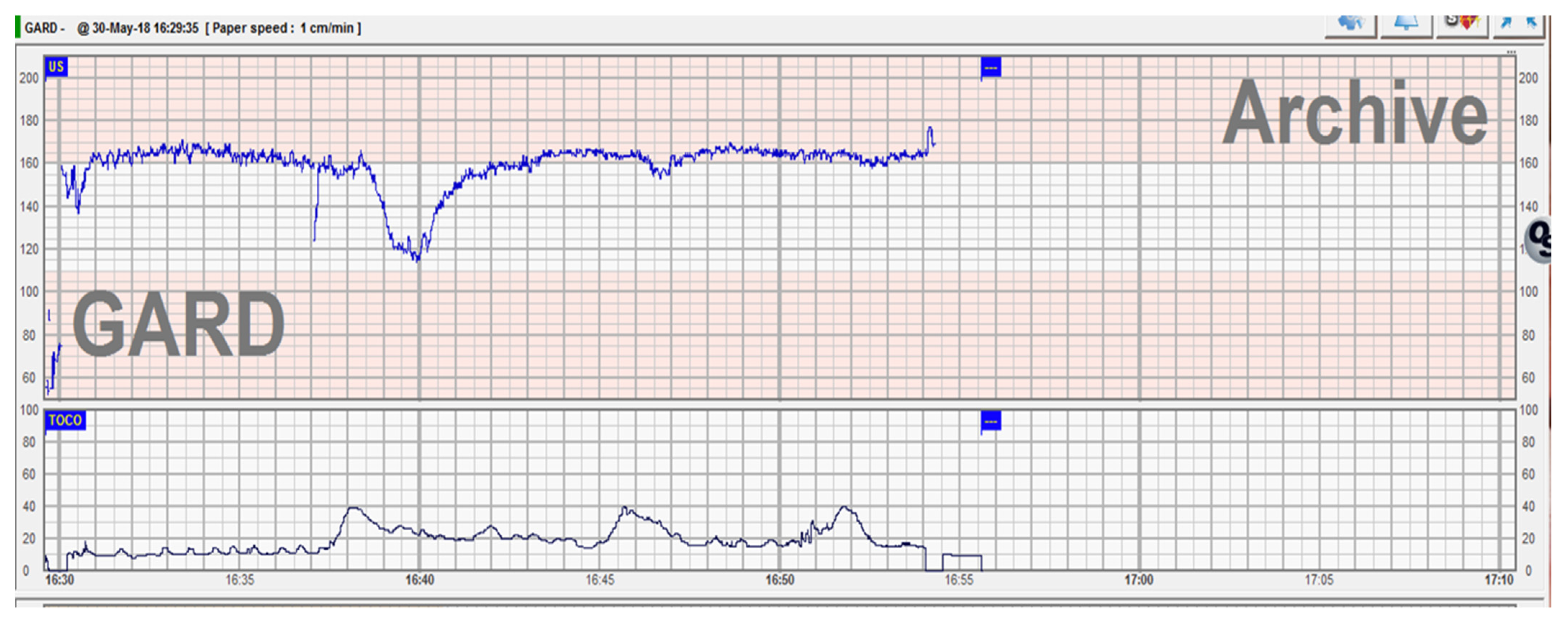
During routine cardiotocography, a pathological trace was recorded—tachycardia and late deceleration (
Figure 1). As per guidelines [
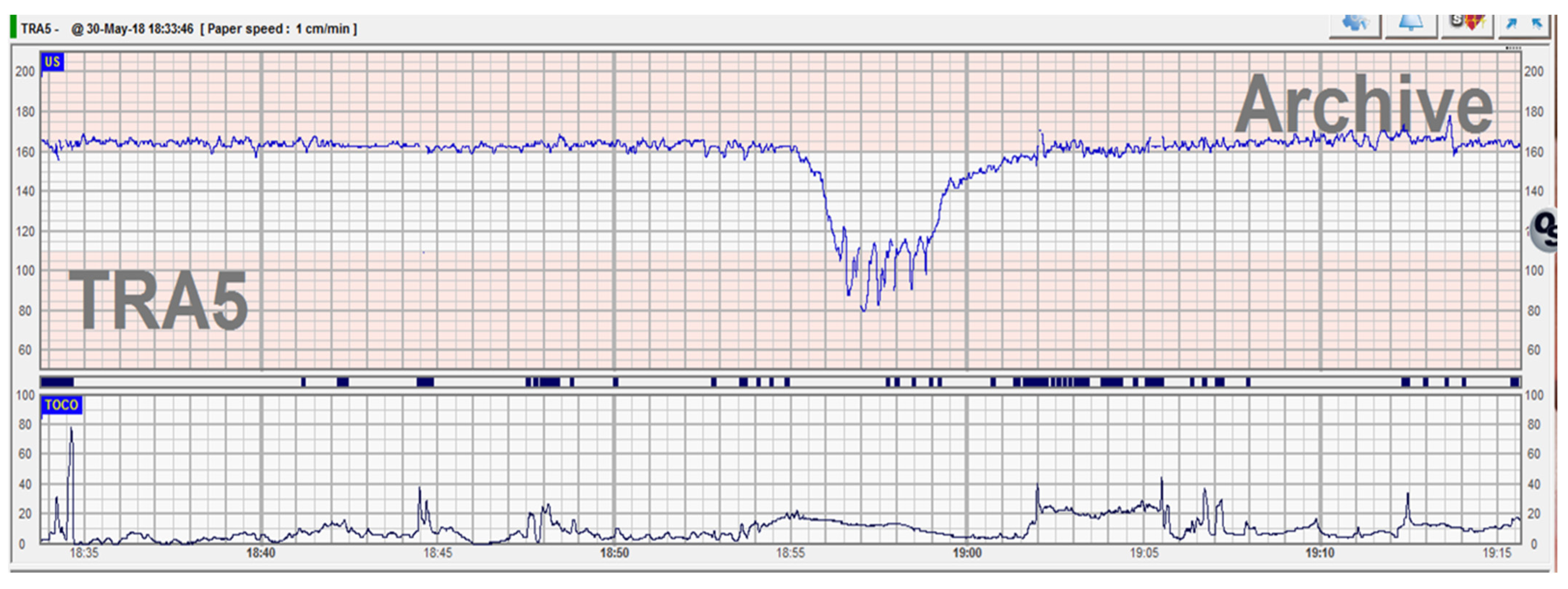
8], immediate action to correct reversible causes and additional methods to evaluate fetal oxygenation were required. Because the patient requested a vaginal delivery and chronic hypoxia needed to be excluded, the artificial rupture of membranes was performed to rule out the presence of meconium and to assess other possible causes of fetal hypoxia. The amniotic fluid had a normal aspect, with no signs of meconium, blood or foul smell. Having excluded infection and chronic hypoxia, and because the trace was reassuring with stable baseline and normal variability, the plan was to reassess progress in 2 h under continuous CTG monitoring, IV hydration and maternal repositioning. Two hours later, another event raised the concern of suspected fetal compromise—a prolonged 4 min late deceleration immediately after a high amplitude fetal movement (
Figure 2)
A decision was made for a category 2 cesarean section. A healthy 3500 g male was delivered in good condition (Apgar score 8). The macroscopic placental examination was normal. During the first routine clinical examination of the neonate, a Wharton’s jelly anomaly was identified at the abdominal umbilical cord insertion. For approximately 1 cm of length, umbilical cord vessels were completely uncovered by Wharton’s jelly. The condition required surgical thread elective ligation of exposed umbilical cord vessels (
Figure 3).
3. Discussion
We present a case where the absence of Wharton’s jelly was observed after the delivery of a healthy term baby with abnormal acute CTG trace modifications during labor.
The absence of Wharton’s jelly is a rare event with only several cases reported in the literature. We conducted a review of the literature in the PubMed database using the search terms ‘Wharton’s’ or Wharton jelly’ and ‘absence’ or ‘absent’. There were sixty-one results retrieved from the beginning of indexing to 2021. We excluded manuscripts not presenting clinical cases. Ten cases were found that matched our search, published between 1985 and 2020. Only two cases reported neonates that were discharged in good condition, six cases were associated with perinatal death, one case was associated with a congenital malformation, a persistent vitellointestinal duct, and the other one had severe neonatal morbidity (
Table 1).
Changes in the consistency of Wharton’s jelly affect umbilical cord blood flow and can contribute to intrauterine growth restriction (IUGR) and even fetal demise. The segmental absence of Wharton’s jelly is an extremely dangerous condition, as umbilical vessels are directly exposed to compression or damage. The absence of Wharton’s jelly can lead to fetal chronic hypoxia [
5,
10,
14,
15]. In our case, there were no signs of fetal hypoxemia before or after delivery. The acute modifications seen on the CTG trace recorded in our case could be explained by the fact that umbilical arteries and veins were suddenly severely compressed at the abdominal insertion portion during active fetal movements.
Normal placental function and fetal oxygenation are prenatally assessed by the ultrasound evaluation of fetal growth, Doppler evaluation of umbilical artery blood flow, the amount of amniotic fluid and maternal perception of fetal movements. Unfortunately, none of these markers were proven to be useful in predicting adverse outcomes related to abnormal Wharton’s jelly, as all the cases reported so far had a sudden occurrence, mostly in normally growing fetuses with normal amniotic fluid. In our case, the Doppler evaluation of the umbilical artery before delivery was normal. Abnormal CTG monitoring with decreased variability and persistent late decelerations was the only prenatal finding which indicated an emergency delivery, and this is in accordance with other reported cases [
5,
10,
14].
Previously reported cases of the absence of Wharton’s jelly describe an association with either meconium-stained liquor [
5] or oligohydramnios, fetal growth restriction, preterm delivery and perinatal death [
3]. None of these findings were true in our case.
The prenatal evaluation of Wharton’s jelly is not part of routine practice, but modifications in its amount and composition have been linked to unfavorable outcomes. [
16]. Most studies investigating the amount of Wharton’s jelly and its implications examined the size of the umbilical cord on a cross-sectional plane. Growth-restricted fetuses have a smaller cross-sectional area of the umbilical cord when compared with normally growing fetuses and these differences are related to the amount of Wharton’s jelly and umbilical vein size [
17]. Moreover, some reports showed that the amount of Wharton’s jelly expressed as the umbilical cord cross-sectional area is correlated with neonatal birth weight [
18].
The proposed theories in the pathogenesis of absent Wharton’s jelly are related to possible degeneration, early incomplete fusion of amniotic and mesenchymal umbilical tissue, or hypoplasia of amnion and secondary loss of Wharton’s jelly [
9]. However, a clear explanation for this rare abnormality is not known.
In our case, the absence of Wharton’s jelly at the abdominal wall insertion could also meet the prerequisites for umbilical cord rupture. Therefore, when an abnormal CTG is associated with active fetal movements, a high grade of suspicion is required for this rare condition and a low threshold regarding the decision for delivery is needed.
4. Conclusions
The absence of Wharton’s jelly is one of the rarest conditions seen in the professional life of an obstetrician. The segmental absence of Wharton’s jelly is almost impossible to diagnose during prenatal ultrasound evaluations and most of the ultrasound markers used in assessing fetal well-being are not good predictors of fetal complications in cases associated with Wharton’s jelly abnormalities. Here we present a fortunate case, where persistent an abnormal CTG trace without any other explanation announced this rare finding—the absence of the Wharton’s jelly. We argue that in the presence of a persistently abnormal CTG trace, in a pregnancy with no clinical settings suggestive for either chronic or acute fetal hypoxemia, the absence of Wharton’s jelly should be taken into consideration in the differential diagnosis.
Author Contributions
Conceptualization, R.B., S.R. and N.G.; methodology, R.B. and A.M.P.; software, R.B. and N.G.; validation, A.M.C. and N.G.; formal analysis, A.M.C. and S.R.; investigation, R.B. and S.R.; resources, R.B.; data curation, R.B., A.M.C. and A.M.P.; writing—original draft preparation, R.B. and N.G.; writing—review and editing, G.P.; visualization, A.M.P.; supervision, G.P.; project administration, R.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Naeye, R.L. Umbilical cord length: Clinical significance. J. Pediatrics 1985, 107, 278–281. [Google Scholar] [CrossRef]
- Oliveira, C.C.; Dufloth, R.M.; Coelho, K.I.R. Absence of Wharton’s jelly: Case report. J. Bras. Patol. Med. Lab. 2014, 50, 452–455. [Google Scholar] [CrossRef] [Green Version]
- Barbieri, C.; Cecatti, J.G.; Surita, F.G.; Costa, M.L.; Marussi, E.F.; Costa, J.V. Area of Wharton’s jelly as an estimate of the thickness of the umbilical cord and its relationship with estimated fetal weight. Reprod. Health 2011, 8, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baergen, R.N. Indications for submission and macroscopic examination of the placenta. APMIS 2018, 126, 544–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, J.; Israfil-Bayli, F. Wharton’s jelly: The significance of absence. J. Obs. Gynaecol. 2016, 36, 500–501. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, F.; Raio, L.; Günter Duwe, D.; Cromi, A.; Karousou, E.; Dürig, P. Sonographic umbilical vessel morphometry and perinatal outcome of fetuses with a lean umbilical cord. J. Clin. Ultrasound 2005, 33, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.Q.; Levitin-Smith, M.; Rochelson, B.; Kahn, E. Umbilical cord stricture and overcoiling are common causes of fetal demise. Pediatric Dev. Pathol. 2006, 9, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Ayres-de-Campos, D.; Spong, C.Y.; Chandraharan, E.; FIGO Intrapartum Fetal Monitoring Expert Consensus Panel. FIGO consensus guidelines on intrapartum fetal monitoring: Cardiotocography. Int. J. Gynaecol. Obs. 2015, 131, 13–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergman, P.; Lundin, P.; Malmstrom, T. Mucoid degeneration of Wharton’s jelly. An umbilical cord anomaly threatening foetal life. Acta Obs. Gynecol. Scand. 1961, 40, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Labarrere, C.; Sebastiani, M.; Siminovich, M.; Torassa, E.; Althabe, O. Absence of Wharton’s jelly around the umbilical arteries: An unusual cause of perinatal mortality. Placenta 1985, 6, 555–559. [Google Scholar] [CrossRef]
- Kulkarni, M.L.; Matadh, P.S.; Ashok, C.; Pradeep, N.; Avinash, T.; Kulkarni, A.M. Absence of Wharton’s jelly around the umbilical arteries. Indian J. Pediatrics 2007, 74, 787–789. [Google Scholar] [CrossRef] [PubMed]
- Thomson, L.L.; Hoo, J.J. Linear disruption of umbilical cord: A rare anomaly of the cord associated with acute fetal distress and perinatal death/profound psychomotor retardation. Am. J. Med. Genet. 1996, 62, 348–349. [Google Scholar] [CrossRef]
- Damasceno, E.B.; de Lima, P.P. Wharton’s jelly absence: A possible cause of stillbirth. Autops Case Rep. 2013, 3, 43–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, S.J.; Deegan, N.; O’Leary, B.D.; McParland, P. Absence of Wharton’s jelly. BMJ Case Rep. 2020, e237222. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.; Chandraharan, E. Recognition of chronic hypoxia and pre-existing foetal injury on the cardiotocograph (CTG): Urgent need to think beyond the guidelines. Porto Biomed. J. 2017, 2, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Benirschke, K. Obstetrically important lesions of the umbilical cord. J. Reprod. Med. 1994, 39, 262–272. [Google Scholar] [PubMed]
- Bruch, J.F.; Sibony, O.; Benali, K.; Challer, C.; Blot, P.; Nessmann, C. Computerized microscope morphometry of umbilical vessels from pregnancies with intrauterine growth retardation and abnormal umbilical artery Doppler. Hum. Pathol. 1997, 28, 1139–1145. [Google Scholar] [CrossRef]
- Raio, L.; Ghezzi, F.; Di Naro, E.; Gomez, R.; Mueller, M.D.; Maymon, E.; Mazor, M. Sonographic measurements of the umbilical cord and fetal anthropometric parameters. Eur. J. Obs. Gynecol. Reprod. Biol. 1999, 83, 135. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 





{kind=link}
{kind=link}
{kind=link}