
Changes in the Plasma Apurinic/Apyrimidinic Endonuclease 1/Redox Factor-1(APE1/Ref-1) Level during Cancer Surgery: An Observational Study

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Anesthesia
2.3. Blinded Analysis
2.4. Blood Samples
2.5. Plasma APE1/Ref-1 Measurements
2.6. Statistical Analyses
2.6.1. Sample Size
2.6.2. Comparison between Two Groups
2.6.3. Propensity Matching
2.6.4. Comparison by Measurement Time within the Group
2.6.5. Correlation Analysis
2.6.6. Comparison by Type of Cancer
2.6.7. Non-Parametric Analysis
3. Results
3.1. Plasma APE1/Ref-1 Levels in The Overall Cohort
3.2. Comparison of Plasma APE1/Ref-1 Levels between Two Groups
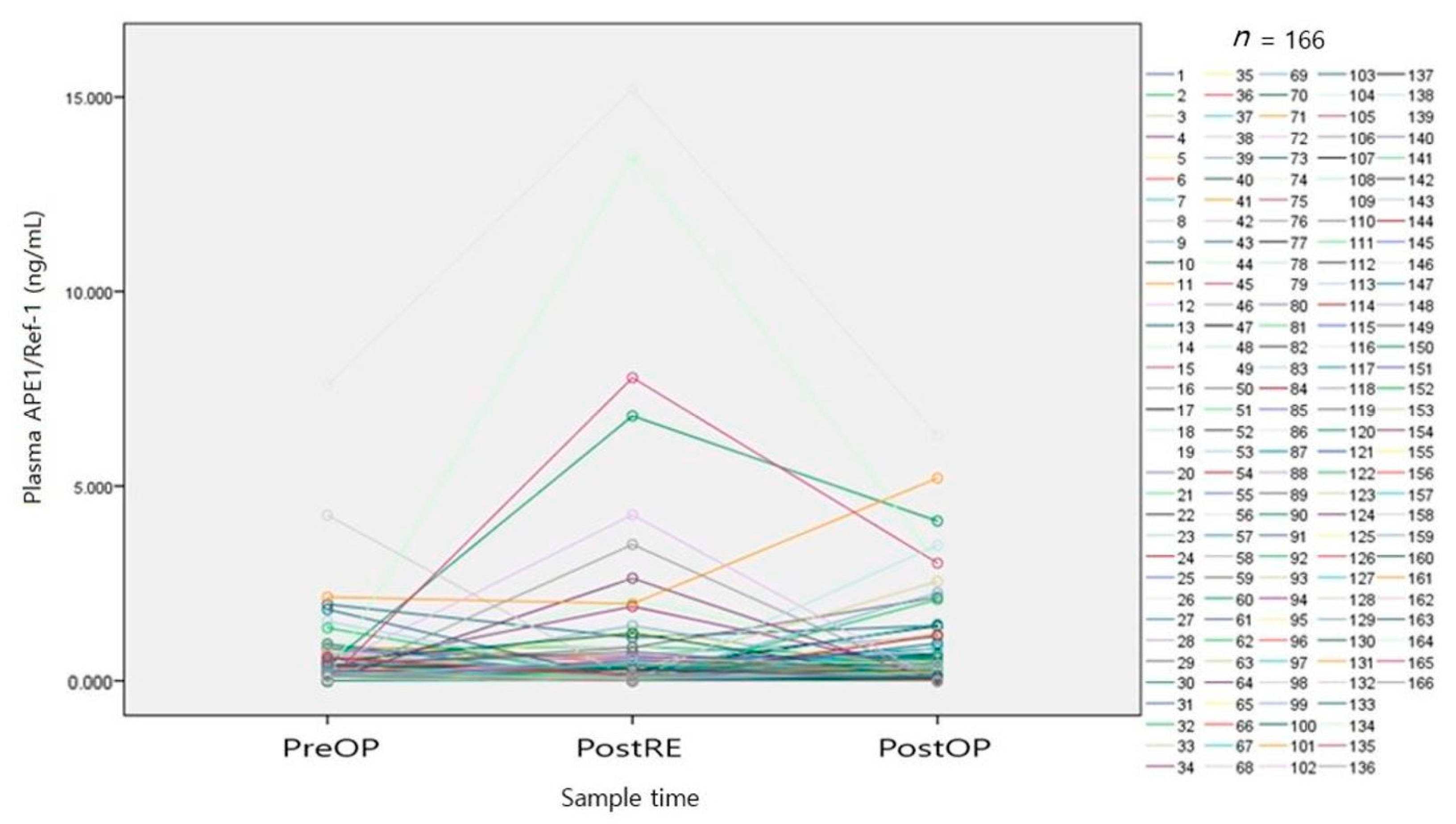
3.3. Comparison of Plasma APE1/Ref-1 Level according to Measurement Time
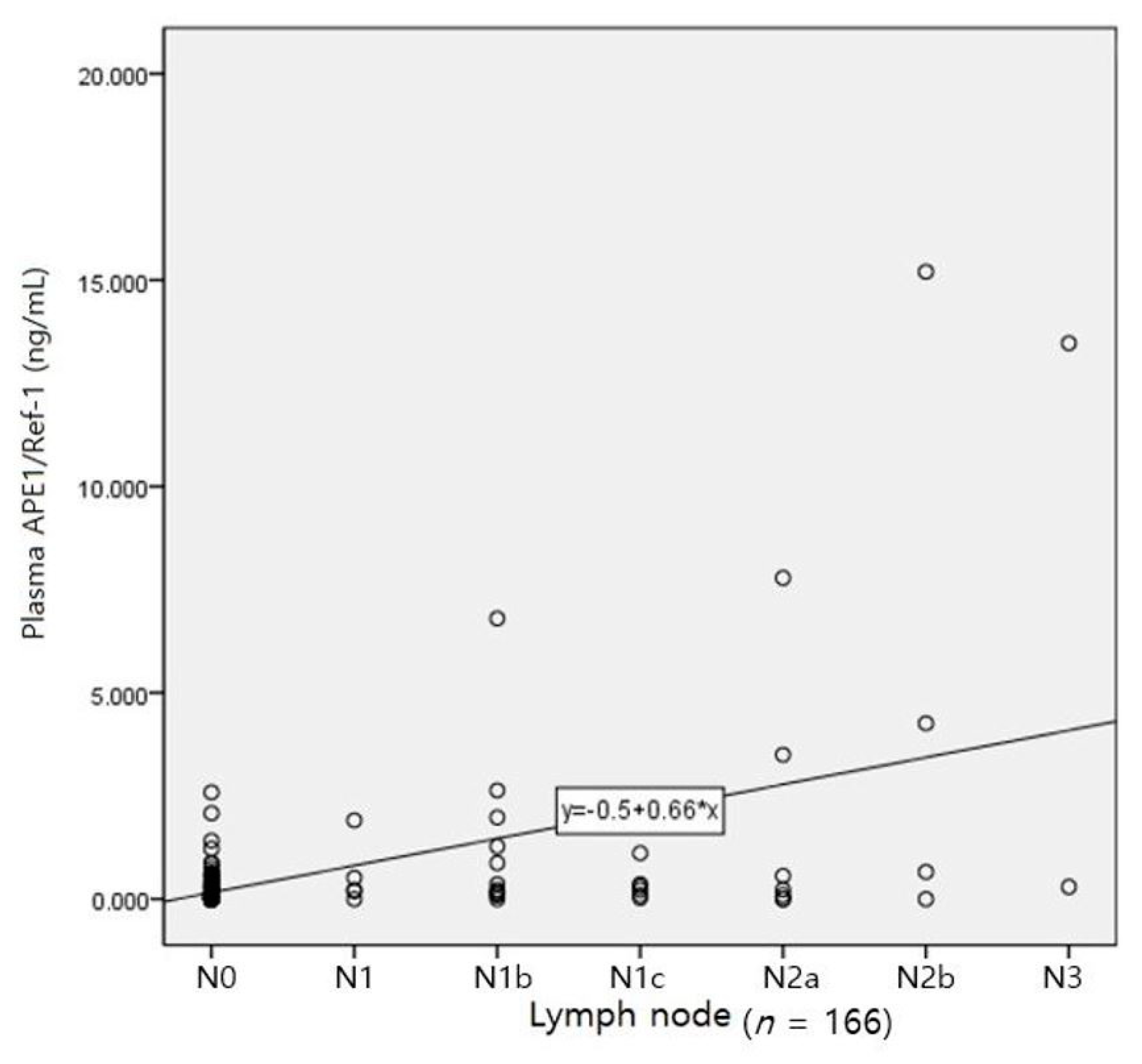
3.4. Analyses of Variables Correlated with Plasma APE1/Ref-1 Level
3.5. Change in Pattern of Plasma APE1/Ref-1 according to Cancer Type
3.6. Non-Parametric Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hooijmans, C.R.; Geessink, F.J.; Ritskes-Hoitinga, M.; Scheffer, G.J. A Systematic Review of the Modifying Effect of Anaesthetic Drugs on Metastasis in Animal Models for Cancer. PLoS ONE 2016, 11, e0156152. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Gao, J.; Yan, N.; Wu, B.; Ren, Y.; Li, H.; Liang, J. Propofol inhibits the growth and survival of gastric cancer cells in vitro through the upregulation of ING3. Oncol. Rep. 2016, 37, 587–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, N.; Liang, Y.; Yang, P.; Ji, F. Propofol suppresses LPS-induced nuclear accumulation of HIF-1α and tumor aggressiveness in non-small cell lung cancer. Oncol. Rep. 2017, 37, 2611–2619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wigmore, T.J.; Mohammed, K.; Jhanji, S. Long-term Survival for Patients Undergoing Volatile versus IV Anesthesia for Cancer Surgery: A Retrospective Analysis. Anesthesiology 2016, 124, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Liu, Y.; Huang, L.; Zhang, F.; Kang, R. Effects of propofol on cancer development and chemotherapy: Potential mechanisms. Eur. J. Pharmacol. 2018, 831, 46–51. [Google Scholar] [CrossRef]
- Huang, N.-C.; Lee, M.-S.; Lai, H.-C.; Lin, H.-T.; Huang, Y.-H.; Lu, C.-H.; Hsu, C.-H.; Wu, Z.-F. Propofol-based total intravenous anesthesia improves survival compared to desflurane anesthesia in gastric cancer surgery: A retrospective analysis. Medicine 2020, 99, e20714. [Google Scholar] [CrossRef]
- Hong, B.; Lee, S.; Kim, Y.; Lee, M.; Youn, A.M.; Rhim, H.; Hong, S.H.; Kim, Y.H.; Yoon, S.H.; Lim, C. Anesthetics and long-term survival after cancer surgery-total intravenous versus volatile anesthesia: A retrospective study. BMC Anesthesiol. 2019, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Bapat, A.; Fishel, M.L.; Kelley, M.R. Going ape as an approach to cancer therapeutics. Antioxid. Redox Signal. 2009, 11, 651–667. [Google Scholar] [CrossRef]
- Ema, M.; Hirota, K.; Mimura, J.; Abe, H.; Yodoi, J.; Sogawa, K.; Poellinger, L.; Fujii-Kuriyama, Y. Molecular mechanisms of transcription activation by HLF and HIF1alpha in response to hypoxia: Their stabilization and redox signal-induced interaction with CBP/p300. EMBO J. 1999, 18, 1905–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaiddon, C.; Moorthy, N.C.; Prives, C. Ref-1 regulates the transactivation and pro-apoptotic functions of p53 in vivo. EMBO J. 1999, 18, 5609–5621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xanthoudakis, S.; Miao, G.; Wang, F.; Pan, Y.C.; Curran, T. Redox activation of Fos-Jun DNA binding activity is mediated by a DNA repair enzyme. EMBO J. 1992, 11, 3323–3335. [Google Scholar] [CrossRef]
- Pascut, D.; Sukowati, C.H.C.; Antoniali, G.; Mangiapane, G.; Burra, S.; Mascaretti, L.G.; Buonocore, M.R.; Crocè, L.S.; Tiribelli, C.; Tell, G. Serum AP-endonuclease 1 (sAPE1) as novel biomarker for hepatocellular carcinoma. Oncotarget 2019, 10, 383–394. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.H.; Choi, S.; Lee, Y.R.; Park, M.S.; Na, Y.G.; Irani, K.; Lee, S.D.; Park, J.B.; Kim, J.M.; Lim, J.S.; et al. APE1/Ref-1 as a Serological Biomarker for the Detection of Bladder Cancer. Cancer Res. Treat. 2015, 47, 823–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.R.; Joo, H.K.; Jeon, B.H. The Biological Role of Apurinic/Apyrimidinic Endonuclease1/Redox Factor-1 as a Therapeutic Target for Vascular Inflammation and as a Serologic Biomarker. Biomedicines 2020, 8, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joo, H.K.; Lee, Y.R.; Lee, E.-O.; Park, M.S.; Choi, S.; Kim, C.-S.; Park, J.-B.; Jeon, B.H. The extracellular role of Ref-1 as anti-inflammatory function in lipopolysaccharide-induced septic mice. Free. Radic. Biol. Med. 2019, 139, 16–23. [Google Scholar] [CrossRef]
- Loboda, A.; Stachurska, A.; Dorosz, J.; Zurawski, M.; Wegrzyn, J.; Kozakowska, M.; Jozkowicz, A.; Dulak, J. HIF-1 attenuates Ref-1 expression in endothelial cells: Reversal by siRNA and inhibition of geranylgeranylation. Vasc. Pharmacol. 2009, 51, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Logsdon, D.P.; Grimard, M.; Luo, M.; Shahda, S.; Jiang, Y.; Tong, Y.; Yu, Z.; Zyromski, N.; Schipani, E.; Carta, F.; et al. Regulation of HIF1α under Hypoxia by APE1/Ref-1 Impacts CA9 Expression: Dual Targeting in Patient-Derived 3D Pancreatic Cancer Models. Mol. Cancer Ther. 2016, 15, 2722–2732. [Google Scholar] [CrossRef] [Green Version]
- Herring, C.J.; West, C.M.L.; Wilks, D.P.; Davidson, S.E.; Hunter, R.D.; Berry, P.; Forster, G.; MacKinnon, J.; Rafferty, J.A.; Elder, R.H.; et al. Levels of the DNA repair enzyme human apurinic/apyrimidinic endonuclease (APE1, APEX, Ref-1) are associated with the intrinsic radiosensitivity of cervical cancers. Br. J. Cancer 1998, 78, 1128–1133. [Google Scholar] [CrossRef] [Green Version]
- Fishel, M.L.; He, Y.; Reed, A.M.; Chin-Sinex, H.; Hutchins, G.D.; Mendonca, M.S.; Kelley, M.R. Knockdown of the DNA repair and redox signaling protein Ape1/Ref-1 blocks ovarian cancer cell and tumor growth. DNA Repair. 2008, 7, 177–186. [Google Scholar] [CrossRef] [Green Version]
- Wei, X.; Li, Y.-b.; Li, Y.; Lin, B.-c.; Shen, X.-M.; Cui, R.-L.; Gu, Y.-J.; Gao, M.; Li, Y.-G.; Zhang, S. Prediction of Lymph Node Metastases in Gastric Cancer by Serum APE1 Expression. J. Cancer 2017, 8, 1492–1497. [Google Scholar] [CrossRef]
- Chan, W.-H.; Lee, M.-S.; Lin, C.; Wu, C.-C.; Lai, H.-C.; Chan, S.-M.; Lu, C.-H.; Cherng, C.-H.; Wu, Z.-F. Comparison of Anesthesia-Controlled Operating Room Time between Propofol-Based Total Intravenous Anesthesia and Desflurane Anesthesia in Open Colorectal Surgery: A Retrospective Study. PLoS ONE 2016, 11, e0165407. [Google Scholar] [CrossRef]
- Huajun, W.; Ying, F.; Hongxing, Z.; Weifeng, S.; Pingyang, S.; Mingde, H.; Guoguang, L. Clinical value of combined detection of serum APE1-Aabs and CEACAM-1 in the diagnosis of colorectal cancer. Eur. Rev. Med Pharmacol. Sci. 2018, 22, 1286–1289. [Google Scholar] [CrossRef]
- Kim, J.-M.; Yeo, M.-K.; Lim, J.S.; Song, I.-S.; Chun, K.; Kim, K.-H. APEX1 Expression as a Potential Diagnostic Biomarker of Clear Cell Renal Cell Carcinoma and Hepatobiliary Carcinomas. J. Clin. Med. 2019, 8, 1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juhnke, M.; Heumann, A.; Chirico, V.; Höflmayer, D.; Menz, A.; Hinsch, A.; Hube-Magg, C.; Kluth, M.; Lang, D.S.; Möller-Koop, C.; et al. Apurinic/apyrimidinic endonuclease 1 (APE1/Ref-1) overexpression is an independent prognostic marker in prostate cancer without TMPRSS2:ERG fusion. Mol. Carcinog. 2017, 56, 2135–2145. [Google Scholar] [CrossRef] [PubMed]
- Kelley, M.R.; Cheng, L.; Foster, R.; Tritt, R.; Jiang, J.; Broshears, J.; Koch, M. Elevated and altered expression of the multifunctional DNA base excision repair and redox enzyme Ape1/ref-1 in prostate cancer. Clin. Cancer. Res. 2001, 7, 824–830. [Google Scholar] [PubMed]
- Zhang, S.; He, L.; Dai, N.; Guan, W.; Shan, J.; Yang, X.; Zhong, Z.; Qing, Y.; Jin, F.; Chen, C.; et al. Serum APE1 as a predictive marker for platinum-based chemotherapy of non-small cell lung cancer patients. Oncotarget 2016, 7, 77482–77494. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | T | N | M |
|---|---|---|---|
| 1 | Tis | N0 | M0 |
| 2 | T1 | N1 | M1a, b |
| 3 | T1b | N1b | M1c |
| 4 | T1c | N1c | |
| 5 | T2 | N2a | |
| 6 | T2b | N2b | |
| 7 | T2c | N3 | |
| 8 | T3 | ||
| 9 | T4a |
| Overall Patients | Matched Patients | |||||
|---|---|---|---|---|---|---|
| Variables | VIA (n = 129) | TIVA (n = 37) | p-Value | VIA (n = 37) | TIVA (n = 37) | p-Value |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |||
| Age (years) | ||||||
| 66 (8.7) | 66 (8.9) | 0.771 | 68 (5.3) | 67 (8.9) | 0.266 | |
| Height (cm) | ||||||
| 162 (8.3) | 161 (7.4) | 0.455 | 160 (7.9) | 161 (7.4) | 0.561 | |
| Weight (kg) | ||||||
| 63 (10.1) | 64 (11.8) | 0.771 | 65 (10.9) | 64 (11.8) | 0.615 | |
| BMI (kg/m2) | ||||||
| 24 (3.4) | 24 (3.3) | 0.491 | 25 (3.3) | 24 (3.3) | 0.258 | |
| Anesthesia | ||||||
| OP time (min) | 199 (85.1) | 170 (55.8) | 0.015 * | 192 (83.0) | 170 (55.8) | 0.194 |
| AN time (min) | 235 (88.0) | 208 (60.8) | 0.032 * | 226 (87.3) | 208 (60.8) | 0.293 |
| Propofol (mg) | 1424 (428) | 1424 (428) | ||||
| Remifentanil (mg) | 2.2 (0.7) | 2.1 (0.7) | 0.592 | 2.1 (0.7) | 2.1 (0.7) | 0.870 |
| n (%) | n (%) | n (%) | n (%) | |||
| Sex | ||||||
| Male Female | 93 (72) 36 (28) | 28 (75) 9 (25) | 0.668 | 26 (70) 11 (30) | 28 (75) 9 (25) | 0.794 |
| ASA | ||||||
| I II III IV | 7 (5) 101 (78) 19 (15) 2 (2) | 1 (3) 31 (83) 5 (14) 0 | 0.859 | 1 (3) 25 (67) 11 (30) | 1 (3) 31 (83) 5 (14) | 0.235 |
| Cancer | ||||||
| Colon Liver Lung Kidney Prostate | 73 (57) 12 (9) 28 (22) 4 (3) 12 (9) | 16 (43) 1 (3) 11 (30) 3 (8) 6 (16) | 0.043 * | 18 (49) 4 (11) 7 (19) 2 (5) 6 (16) | 16 (43) 1 (3) 11 (30) 3 (8) 6 (16) | 0.557 |
| BMI | ASA | Age | Sex | T | N | M | ||
|---|---|---|---|---|---|---|---|---|
| BMI (kg/m2) | r | 1.000 | 0.083 | 0.020 | 0.166 * | −0.107 | −0.049 | −0.121 |
| p | 0.289 | 0.794 | 0.032 | 0.170 | 0.528 | 0.122 | ||
| ASA (I/II/III/IV) | r | 0.083 | 1.000 | 0.220 ** | 0.004 | 0.034 | 0.031 | 0.042 |
| p | 0.289 | 0.004 | 0.955 | 0.666 | 0.693 | 0.591 | ||
| Age (years) | r | 0.020 | 0.220 ** | 1.000 | 0.210 ** | 0.036 | 0.072 | 0.041 |
| p | 0.794 | 0.004 | 0.007 | 0.641 | 0.355 | 0.597 | ||
| Sex (M:1, F:2) | r | 0.166 * | 0.004 | 0.210 ** | 1.000 | 0.006 | 0.192 * | −0.055 |
| p | 0.032 | 0.955 | 0.007 | 0.941 | 0.013 | 0.483 | ||
| T | r | −0.107 | 0.034 | 0.036 | 0.006 | 1.000 | 0.367 ** | 0.281 ** |
| p | 0.170 | 0.666 | 0.641 | 0.941 | 0.000 | 0.000 | ||
| N | r | −0.049 | 0.031 | 0.072 | 0.192 * | 0.367 ** | 1.000 | 0.366 ** |
| p | 0.528 | 0.693 | 0.355 | 0.013 | 0.000 | 0.000 | ||
| M | r | −0.121 | 0.042 | 0.041 | −0.055 | 0.281 ** | 0.366 ** | 1.000 |
| p | 0.122 | 0.591 | 0.597 | 0.483 | 0.000 | 0.000 | ||
| PreOP | r | −0.016 | −0.009 | 0.008 | −0.074 | 0.079 | 0.165 * | 0.135 |
| p | 0.839 | 0.907 | 0.915 | 0.342 | 0.315 | 0.033 | 0.083 | |
| PostRE | r | −0.025 | 0.051 | −0.104 | −0.021 | 0.083 | 0.300 ** | 0.243 ** |
| p | 0.745 | 0.515 | 0.181 | 0.789 | 0.287 | 0.000 | 0.002 | |
| PostOP | r | −0.062 | 0.088 | −0.015 | −0.169 * | 0.089 | 0.084 | 0.154 * |
| p | 0.425 | 0.257 | 0.852 | 0.030 | 0.252 | 0.282 | 0.048 | |
| Sum Square | Mean Square | NumDF | F Value | p | |
|---|---|---|---|---|---|
| Time | 8.78 | 4.39 | 2 | 5.23 | 0.005 ** |
| Anesthesia type | 0.03 | 0.03 | 1 | 0.04 | 0.832 |
| Time × Anesthetic type | 2.71 | 1.35 | 2 | 1.61 | 0.199 |
| Cancer | Author | Control level | Plasma APE1/Ref-1 | Our Study (ng/mL) |
|---|---|---|---|---|
| Colon | Huajun | 1.83 ± 0.31 ng/mL | 2.68 ± 0.34 ng/mL | 0.38 ± 0.10 |
| Kidney | Kim | <0.202 ng/mL | >0.202 ng/mL | 0.24 ± 0.07 |
| Prostate | 0.23 ± 0.05 | |||
| Liver | Pascut | 10.8 pg/mL | 75.8 pg/mL | 0.20 ± 0.07 |
| Lung | Zhang | 0.091 ng/mL | 0.159 ng/mL | 0.18 ± 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jo, Y.; Kim, Y.; Park, E.; Lee, Y.; Kim, J.; Kang, M.; Lim, J.; Song, I.; Lim, C.; Jeon, B. Changes in the Plasma Apurinic/Apyrimidinic Endonuclease 1/Redox Factor-1(APE1/Ref-1) Level during Cancer Surgery: An Observational Study. Medicina 2021, 57, 1280. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57111280
Jo Y, Kim Y, Park E, Lee Y, Kim J, Kang M, Lim J, Song I, Lim C, Jeon B. Changes in the Plasma Apurinic/Apyrimidinic Endonuclease 1/Redox Factor-1(APE1/Ref-1) Level during Cancer Surgery: An Observational Study. Medicina. 2021; 57(11):1280. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57111280
Chicago/Turabian StyleJo, Yumin, Yeojung Kim, Eunhye Park, Yuran Lee, Jiyeon Kim, Minwoong Kang, Jaesung Lim, Insang Song, Chaeseong Lim, and Byeonghwa Jeon. 2021. "Changes in the Plasma Apurinic/Apyrimidinic Endonuclease 1/Redox Factor-1(APE1/Ref-1) Level during Cancer Surgery: An Observational Study" Medicina 57, no. 11: 1280. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57111280