
A Systematic Review on Comparative Analyses between Ureteroscopic Lithotripsy and Shock-Wave Lithotripsy for Ureter Stone According to Stone Size




Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Search Strategy
2.3. Study Selection and Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
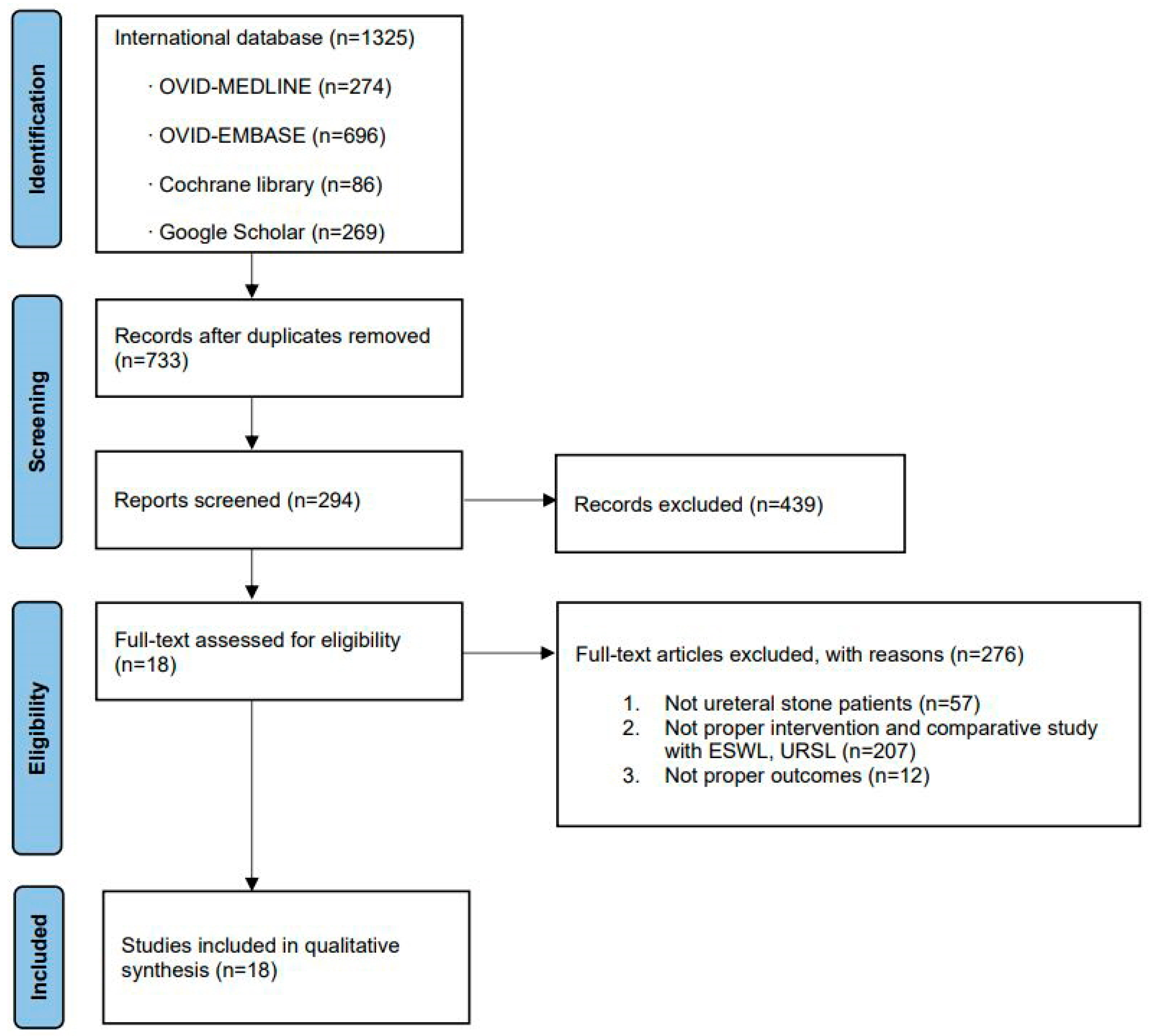
3.1. Eligible Studies
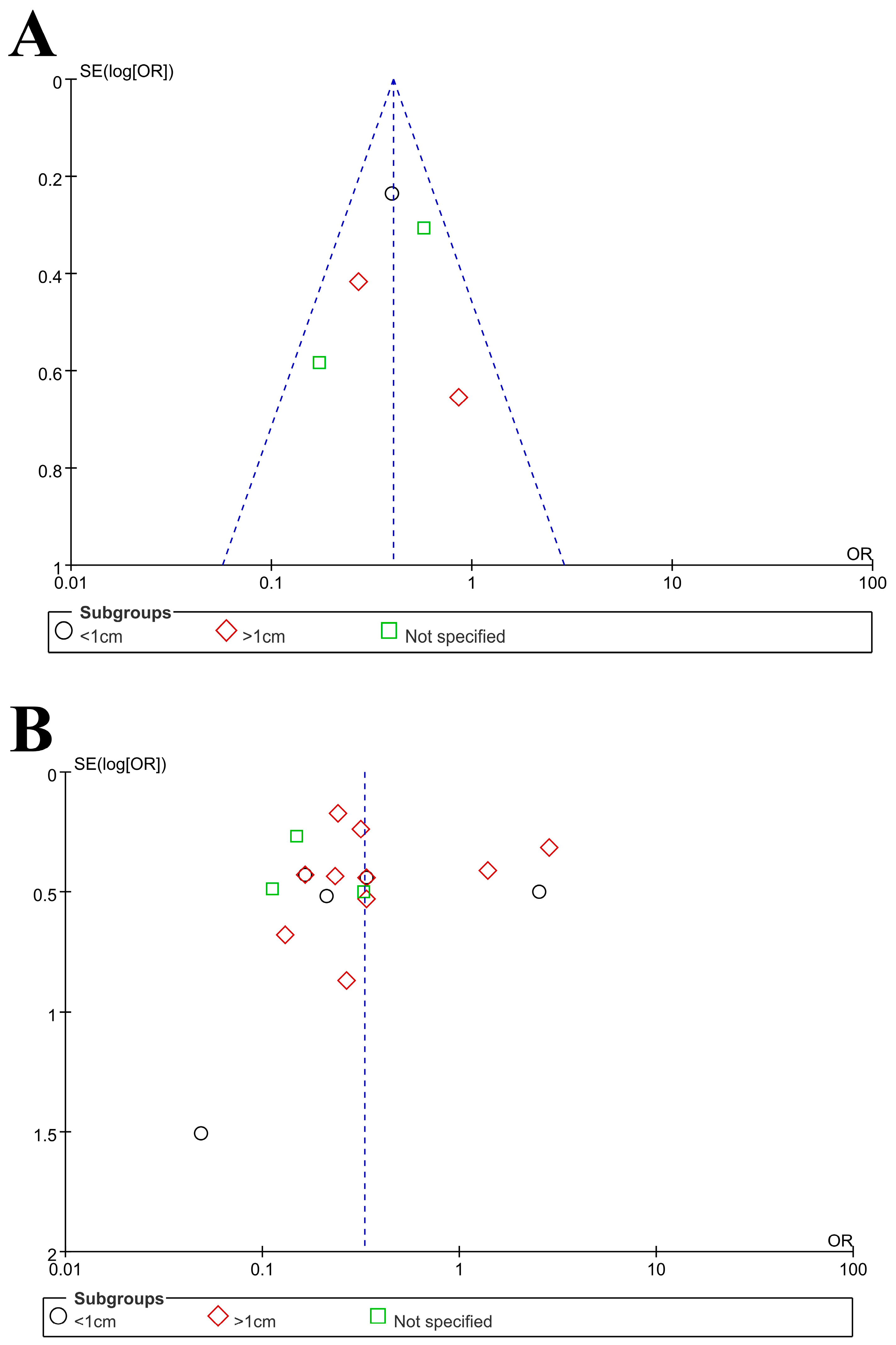
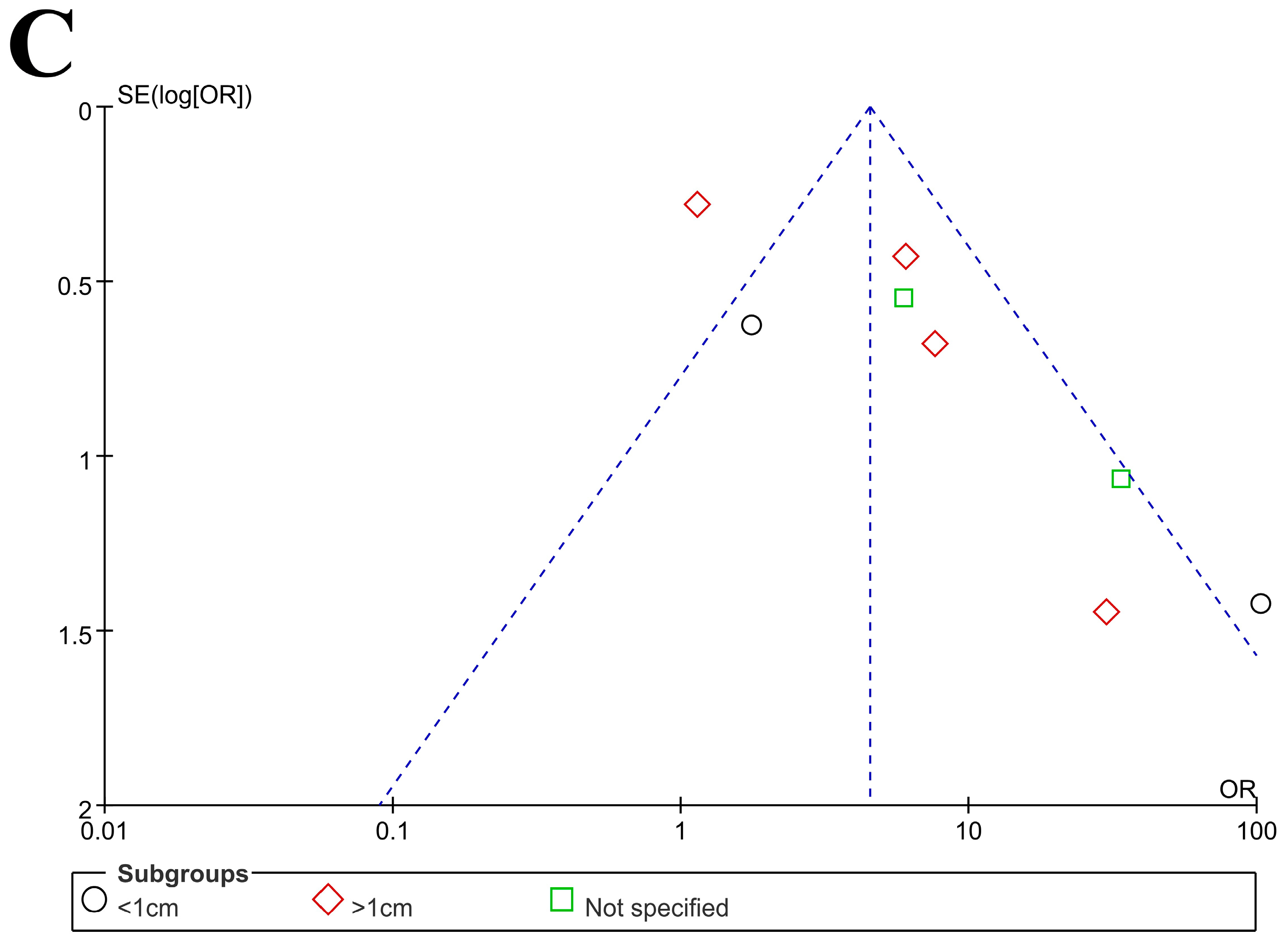
3.2. Characteristics of Included Studies with Quality Assessment and Publication Bias
3.3. Heterogeneity Assessment
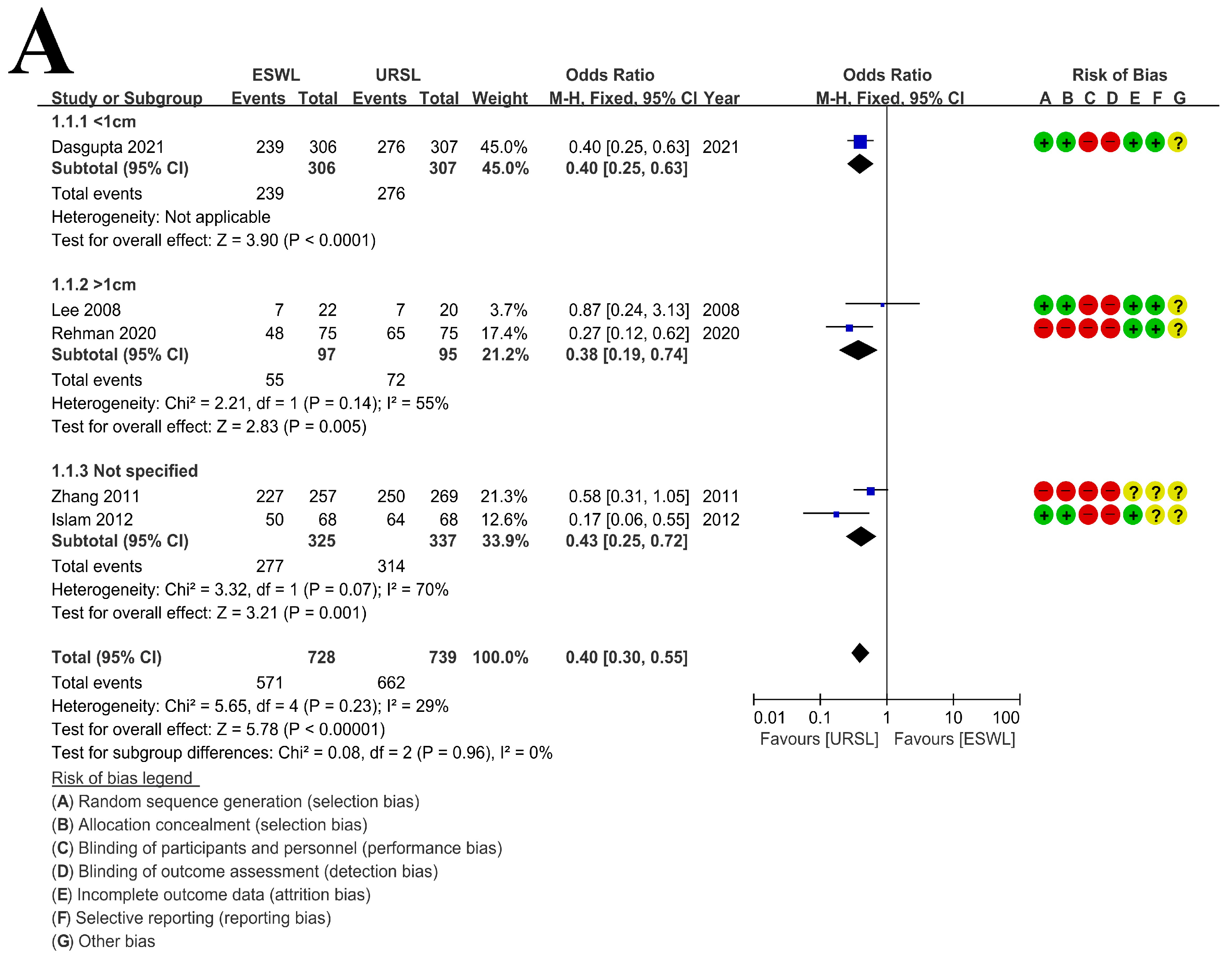
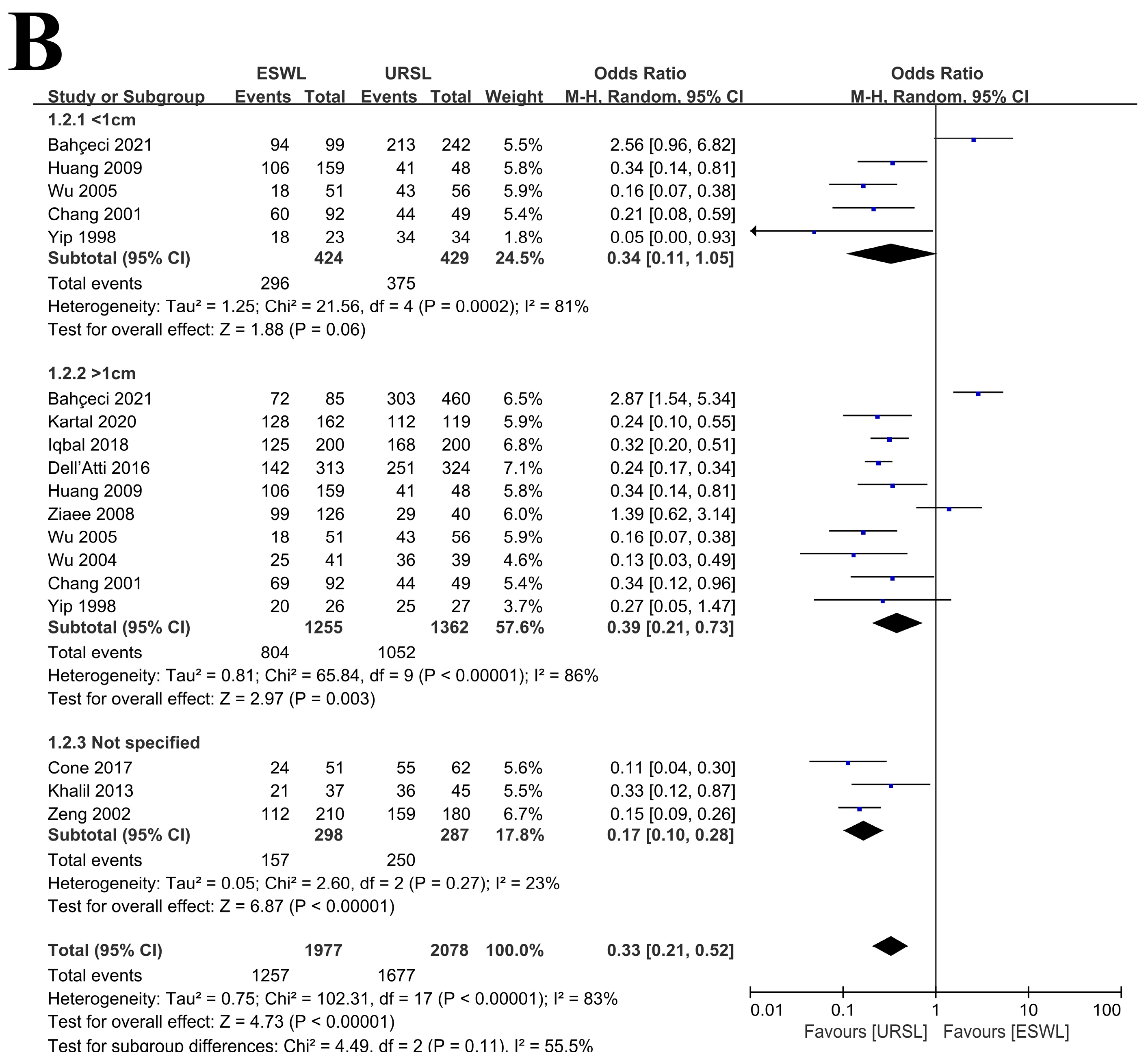
3.4. Stone-Free Rate
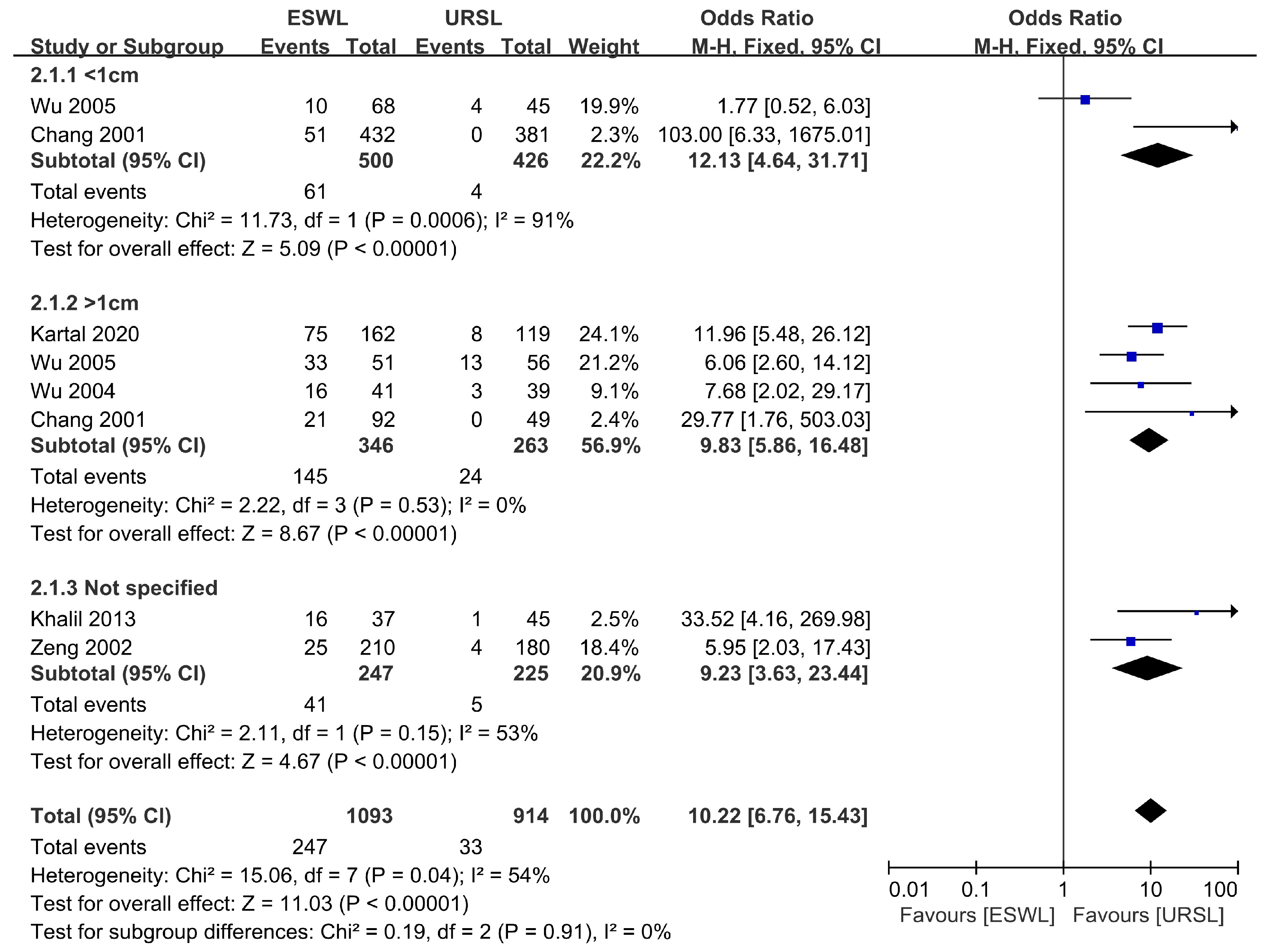
3.5. Retreatment Procedure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sorokin, I.; Mamoulakis, C.; Miyazawa, K.; Rodgers, A.; Talati, J.; Lotan, Y. Epidemiology of stone disease across the world. World J. Urol. 2017, 35, 1301–1320. [Google Scholar] [CrossRef]
- Wong, Y.; Cook, P.; Roderick, P.; Somani, B.K. Metabolic Syndrome and Kidney Stone Disease: A Systematic Review of Literature. J. Endourol. 2016, 30, 246–253. [Google Scholar] [CrossRef]
- Geraghty, R.M.; Proietti, S.; Traxer, O.; Archer, M.; Somani, B.K. Worldwide Impact of Warmer Seasons on the Incidence of Renal Colic and Kidney Stone Disease: Evidence from a Systematic Review of Literature. J. Endourol. 2017, 31, 729–735. [Google Scholar] [CrossRef]
- WJ, P.; JO, K.; TH, O. The Outcome of Laparoscopic Retroperitoneal Ureterolithotomy for the Management of Upper Ureteral Stones Larger than 10 mm: A Comparison with Rigid Ureteroscopic Removal of Stones with Lithoclast(R). Korean J. Urol. 2009, 50, 349–354. [Google Scholar]
- Turk, C.; Petrik, A.; Sarica, K.; Seitz, C.; Skolarikos, A.; Straub, M.; Knoll, T. EAU Guidelines on Interventional Treatment for Urolithiasis. Eur. Urol. 2016, 69, 475–482. [Google Scholar] [CrossRef]
- Betschart, P.; Zumstein, V.; Jichlinski, P.; Herrmann, T.R.W.; Knoll, T.; Engeler, D.S.; Müllhaupt, G.; Schmid, H.P.; Abt, D. Spoilt for Choice: A Survey of Current Practices of Surgical Urinary Stone Treatment and Adherence to Evidence-Based Guidelines among Swiss Urologists. Urol. Int. 2019, 103, 357–363. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.; Malik, A. Ureteroscopic pneumatic versus extracorporeal shock wave lithotripsy for lower ureteral stones. J. Coll. Physicians Surg. Pak. 2012, 22, 444–447. [Google Scholar]
- Zhang, J.; Shi, Q.; Wang, G.Z.; Wang, F.; Jiang, N. Cost-effectiveness analysis of ureteroscopic laser lithotripsy and shock wave lithotripsy in the management of ureteral calculi in eastern China. Urol. Int. 2011, 86, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Tsai, J.Y.; Jiaan, B.P.; Wu, T.; Yu, C.C. Prospective randomized trial comparing shock wave lithotripsy and ureteroscopic lithotripsy for management of large upper third ureteral stones. Urology 2006, 67, 480–484. [Google Scholar] [CrossRef]
- Cone, E.B.; Pareek, G.; Ursiny, M.; Eisner, B. Cost-effectiveness comparison of ureteral calculi treated with ureteroscopic laser lithotripsy versus shockwave lithotripsy. World J. Urol. 2017, 35, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Dell’Atti, L.; Papa, S. Ten-year experience in the management of distal ureteral stones greater than 10 mm in size. G. Chir. 2016, 37, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Khalil, M. Management of impacted proximal ureteral stone: Extracorporeal shock wave lithotripsy versus ureteroscopy with holmium: YAG laser lithotripsy. Urol. Ann. 2013, 5, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Chen, S.S.; Chen, L.K. Cost-effectiveness of treating ureteral stones in a Taipei City Hospital: Shock wave lithotripsy versus ureteroscopy plus lithoclast. Urol. Int. 2009, 83, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Ziaee, S.A.; Halimiasl, P.; Aminsharifi, A.; Shafi, H.; Beigi, F.M.; Basiri, A. Management of 10–15-mm proximal ureteral stones: Ureteroscopy or extracorporeal shockwave lithotripsy? Urology 2008, 71, 28–31. [Google Scholar] [CrossRef]
- Wu, C.F.; Chen, C.S.; Lin, W.Y.; Shee, J.J.; Lin, C.L.; Chen, Y.; Huang, W.S. Therapeutic options for proximal ureter stone: Extracorporeal shock wave lithotripsy versus semirigid ureterorenoscope with holmium:yttrium-aluminum-garnet laser lithotripsy. Urology 2005, 65, 1075–1079. [Google Scholar] [CrossRef]
- Wu, C.F.; Shee, J.J.; Lin, W.Y.; Lin, C.L.; Chen, C.S. Comparison between extracorporeal shock wave lithotripsy and semirigid ureterorenoscope with holmium:YAG laser lithotripsy for treating large proximal ureteral stones. J. Urol. 2004, 172, 1899–1902. [Google Scholar] [CrossRef]
- Zeng, G.Q.; Zhong, W.D.; Cai, Y.B.; Dai, Q.S.; Hu, J.B.; Wei, H.A. Extracorporeal shock-wave versus pneumatic ureteroscopic lithotripsy in treatment of lower ureteral calculi. Asian J. Androl. 2002, 4, 303–305. [Google Scholar]
- Chang, C.P.; Huang, S.H.; Tai, H.L.; Wang, B.F.; Yen, M.Y.; Huang, K.H.; Jiang, H.J.; Lin, J. Optimal treatment for distal ureteral calculi: Extracorporeal shockwave lithotripsy versus ureteroscopy. J. Endourol. 2001, 15, 563–566. [Google Scholar] [CrossRef]
- Yip, S.K.; Lee, F.C.; Tam, P.C.; Leung, S.Y. Outpatient treatment of middle and lower ureteric stones: Extracorporeal shock wave lithotripsy versus ureteroscopic laser lithotripsy. Ann. Acad. Med. Singap. 1998, 27, 515–519. [Google Scholar] [PubMed]
- Bahçeci, T.; Kızılay, F.; Çal, A.Ç.; Şimşir, A. Comparison of shockwave lithotripsy and laser ureterolithotripsy for ureteral stones. J. Urol. Surg. 2021, 8, 167–172. [Google Scholar] [CrossRef]
- Dasgupta, R.; Cameron, S.; Aucott, L.; MacLennan, G.; Thomas, R.E.; Kilonzo, M.M.; Lam, T.B.L.; N’Dow, J.; Norrie, J.; Anson, K.; et al. Shockwave Lithotripsy Versus Ureteroscopic Treatment as Therapeutic Interventions for Stones of the Ureter (TISU): A Multicentre Randomised Controlled Non-inferiority Trial. Eur. Urol. 2021, 80, 46–54. [Google Scholar] [CrossRef]
- Iqbal, N.; Malik, Y.; Nadeem, U.; Khalid, M.; Pirzada, A.; Majeed, M.; Malik, H.A.; Akhter, S. Comparison of ureteroscopic pneumatic lithotripsy and extracorporeal shock wave lithotripsy for the management of proximal ureteral stones: A single center experience. Turk. J. Urol. 2018, 44, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Kartal, I.; Yalçınkaya, F.; Baylan, B.; Cakıcı, M.C.; Sarı, S.; Selmi, V.; Ozdemir, H. Comparison of semirigid ureteroscopy, flexible ureteroscopy, and shock wave lithotripsy for initial treatment of 11–20 mm proximal ureteral stones. Arch. Ital. Urol. E Androl. 2020, 92, 39–44. [Google Scholar] [CrossRef]
- Ur Rehman, M.F.; Adnan, M.; Hassan, A., 3rd; Humayun Akhtar, F.; Javed, N.; Ali, F. Comparison of Ureteroscopic Pneumatic Lithotripsy and Extracorporeal Shock Wave Lithotripsy for Proximal Ureteral Calculi. Cureus 2020, 12, e7840. [Google Scholar] [CrossRef] [Green Version]
- Chaussy, C.; Brendel, W.; Schmiedt, E. Extracorporeally induced destruction of kidney stones by shock waves. Lancet 1980, 2, 1265–1268. [Google Scholar] [CrossRef]
- Rassweiler, J.; Rassweiler, M.C.; Frede, T.; Alken, P. Extracorporeal shock wave lithotripsy: An opinion on its future. Indian J. Urol. 2014, 30, 73–79. [Google Scholar] [CrossRef]
- Young, H.H.; McKay, R.W. Congenital valve obstruction of the prostatic urethra. Surg Gynecol Obstet 1929, 48, 509. [Google Scholar]
- Marshall, V.F. Fiber Optics in Urology. J. Urol. 1964, 91, 110–114. [Google Scholar] [CrossRef]
- Talso, M.; Tefik, T.; Mantica, G.; Rodriguez Socarras, M.; Kartalas Goumas, I.; Somani, B.K.; Esperto, F. Extracorporeal shockwave lithotripsy: Current knowledge and future perspectives. Minerva Urol. Nefrol. 2019, 71, 365–372. [Google Scholar] [CrossRef]
- Assimos, D.; Krambeck, A.; Miller, N.L.; Monga, M.; Murad, M.H.; Nelson, C.P.; Pace, K.T.; Pais, V.M., Jr.; Pearle, M.S.; Preminger, G.M.; et al. Surgical Management of Stones: American Urological Association/Endourological Society Guideline, PART I. J. Urol. 2016, 196, 1153–1160. [Google Scholar] [CrossRef]
- Drake, T.; Grivas, N.; Dabestani, S.; Knoll, T.; Lam, T.; Maclennan, S.; Petrik, A.; Skolarikos, A.; Straub, M.; Tuerk, C.; et al. What are the Benefits and Harms of Ureteroscopy Compared with Shock-wave Lithotripsy in the Treatment of Upper Ureteral Stones? A Systematic Review. Eur. Urol. 2017, 72, 772–786. [Google Scholar] [CrossRef]
- Xu, Y.; Lu, Y.; Li, J.; Luo, S.; Liu, Y.; Jia, Z.; Chen, P.; Guo, Y.; Zhao, Q.; Ma, X.; et al. A meta-analysis of the efficacy of ureteroscopic lithotripsy and extracorporeal shock wave lithotripsy on ureteral calculi. Acta Cir. Bras. 2014, 29, 346–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, X.; Ji, F.; Yan, H.; Ou, T.W.; Jia, C.S.; He, X.Z.; Gao, W.; Wang, Q.; Cui, B.; Wu, J.T. Comparison between extracorporeal shock wave lithotripsy and ureteroscopic lithotripsy for treating large proximal ureteral stones: A meta-analysis. Urology 2015, 85, 748–756. [Google Scholar] [CrossRef]
- Matlaga, B.R.; Jansen, J.P.; Meckley, L.M.; Byrne, T.W.; Lingeman, J.E. Treatment of ureteral and renal stones: A systematic review and meta-analysis of randomized, controlled trials. J. Urol. 2012, 188, 130–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aboumarzouk, O.M.; Kata, S.G.; Keeley, F.X.; McClinton, S.; Nabi, G. Extracorporeal shock wave lithotripsy (ESWL) versus ureteroscopic management for ureteric calculi. Cochrane Database Syst. Rev. 2011, 12, Cd006029. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author Year | Country | Design | Procedure | Stone Size (cm) | No. Patients | Mean Age | Quality Assessment (SIGN) |
|---|---|---|---|---|---|---|---|
| Dasgupta et al. | UK | RCT | ESWL | ≤1 | 302 | 52.1 | 1+ |
| 2021 [23] | URSL | 302 | 50 | ||||
| Bahçeci et al. | Turkey | Retrospective | ESWL | <1 | 94 | 46 | 2+ |
| 2021 [22] | ≥1 | 72 | |||||
| URSL | <1 | 213 | 46 | ||||
| ≥1 | 403 | ||||||
| Kartal et al. | Turkey | Retrospective | ESWL | 1.3 ± 0.3 | 162 | 43.6 ± 12.6 | 2+ |
| 2020 [25] | URSL | 1.4 ± 0.3 | 119 | 43.9 ± 13.1 | |||
| fURSL | 1.4 ± 0.2 | 201 | 44.5 ± 13.1 | ||||
| Rehman et al. | USA | RCT | ESWL | 1.01 ± 0.2 | 75 | 41.2 ± 3.2 | 1- |
| 2020 [26] | URSL | 2.4 ± 0.2 | 75 | 40.9 ± 3.7 | |||
| Iqbal et al. | Pakistan | Retrospective | ESWL | 1.0 ± 0.4 | 36 | 39.2 ± 13.4 | 2+ |
| 2018 [24] | URSL | 1.4 ± 0.7 | 37 | 43.1 ± 13.7 | |||
| Cone et al. | USA | Retrospective | ESWL | <1.5 | 51 | 53 ± 14 | 2+ |
| 2017 [12] | URSL | 62 | 54 ± 16 | ||||
| Dell’Atti et al. | Italy | Retrospective | ESWL | ≥1 | 313 | 46.2 ± 1.5 | 2+ |
| 2016 [13] | URSL | 324 | 49.4 ± 2.1 | ||||
| Khalil | Kuwait | Prospective | ESWL | <2 | 37 | 37.1 ± 8.8 | 2+ |
| 2013 [14] | URSL | 45 | 35.2 ± 10.4 | ||||
| Islam et al. | Pakistan | RCT | ESWL | <2.5 | 68 | 35.4 ± 9.2 | 2+ |
| 2012 [9] | URSL | 68 | 35.3 ± 9.5 | ||||
| Zhang et al. | China | RCT | ESWL | 0.5–2.5 | 257 | 49 | 1+ |
| 2011 [10] | URSL | 269 | 50 | ||||
| Huang et al. | Taiwan | Prospective | ESWL | <1 | 201 | 52.5 ± 16.1 | 2+ |
| 2009 [15] | ≥1 | 159 | |||||
| URSL | <1 | 40 | 49.5 ± 12.7 | ||||
| ≥1 | 48 | ||||||
| Ziaee et al. | Iran | Prospective | ESWL | ≥1 | 126 | 42.5 | 2+ |
| 2008 [16] | URSL | 40 | 40.5 | ||||
| Lee et al. | Taiwan | RCT | ESWL | ≥1 | 22 | 54.2 ± 16.7 | 1- |
| 2008 [11] | URSL | 20 | 48.5 ± 13.3 | ||||
| Wu et al. | Taiwan | Prospective | ESWL | <1 | 68 | 47.5 ± 1.5 | 2+ |
| 2005 [17] | ≥1 | 51 | 51.5 ± 1.9 | ||||
| URSL | <1 | 45 | 51.0 ± 2.0 | ||||
| ≥1 | 56 | 53.8 ± 1.5 | |||||
| Wu et al. | Taiwan | Prospective | ESWL | ≥1 | 41 | 51 | 2+ |
| 2004 [18] | URSL | 39 | 51 | ||||
| Zeng et al. | China | Prospective | ESWL | 0.5–2.1 | 210 | 51 | 2- |
| 2002 [19] | URSL | 180 | 40 | ||||
| Chang et al. | Taiwan | Retrospective | ESWL | <1 | 432 | 48.2 | 2- |
| 2001 [20] | ≥1 | 92 | |||||
| URSL | <1 | 381 | 48.3 | ||||
| ≥1 | 49 | ||||||
| Yip et al. | Singapore | Retrospective | ESWL | <1 | 23 | 54 | 2- |
| 1998 [21] | ≥1 | 26 | |||||
| URSL | <1 | 34 | 47 | ||||
| ≥1 | 27 |
| A Clearly Stated Aim | Inclusion of Consecutive Samples | Prospective Collection of Data | Endpoints Appropriate to the Aim of the Study | Unbiased Assessment of the Study Endpoint | Follow-up Period Appropriate to the Aim of the Study | Loss to Follow up Less than 5% | Prospective Calculation of the Study Size | An Adequate Control Group | Contemporary Groups | Baseline Equivalence of Groups | Adequate Statistical Analyses | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bahçeci et al. 2021 [22] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 19 |
| Kartal et al. 2020 [25] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 20 |
| Iqbal et al. 2018 [24] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 20 |
| Cone et al. 2017 [12] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 19 |
| Dell’Atti et al. 2016 [13] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 20 |
| Khalil 2013 [14] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 20 |
| Huang et al. 2009 [15] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 20 |
| Ziaee et al. 2008 [16] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 19 |
| WU et al. 2005 [17] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 19 |
| Wu et al. 2004 [18] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 19 |
| Zeng et al. 2002 [19] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 19 |
| Chang et al. 2001 [20] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 19 |
| Yip et al. 1998 [21] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, H.D.; Hong, Y.; Lee, J.Y.; Lee, S.H. A Systematic Review on Comparative Analyses between Ureteroscopic Lithotripsy and Shock-Wave Lithotripsy for Ureter Stone According to Stone Size. Medicina 2021, 57, 1369. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121369
Jung HD, Hong Y, Lee JY, Lee SH. A Systematic Review on Comparative Analyses between Ureteroscopic Lithotripsy and Shock-Wave Lithotripsy for Ureter Stone According to Stone Size. Medicina. 2021; 57(12):1369. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121369
Chicago/Turabian StyleJung, Hae Do, Youna Hong, Joo Yong Lee, and Seon Heui Lee. 2021. "A Systematic Review on Comparative Analyses between Ureteroscopic Lithotripsy and Shock-Wave Lithotripsy for Ureter Stone According to Stone Size" Medicina 57, no. 12: 1369. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121369