
Contribution of Global and Regional Longitudinal Strain for Clinical Assessment of HFpEF in Coronary and Hypertensive Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Populations
2.2. Clinical and Biochemical Evaluation
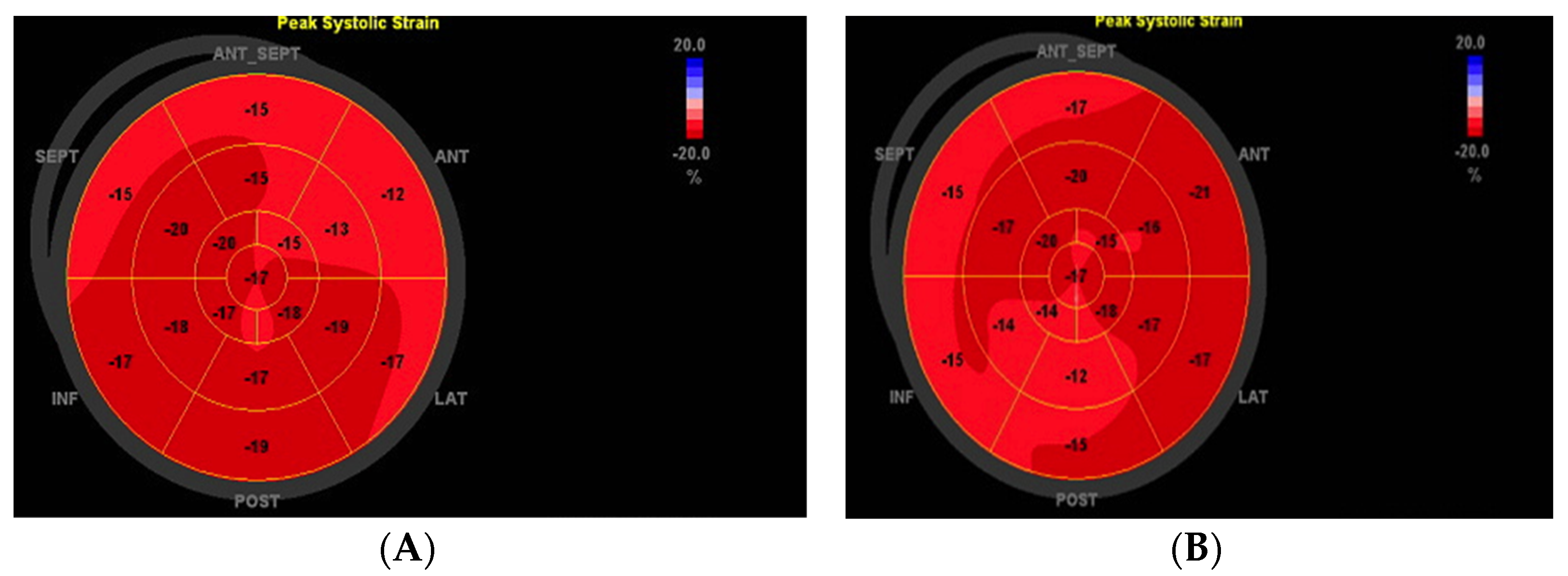
2.3. Determination of Echocardiographic Parameters and Speckle-Tracking Echocardiography (STE)—Strain Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Population and Characteristics
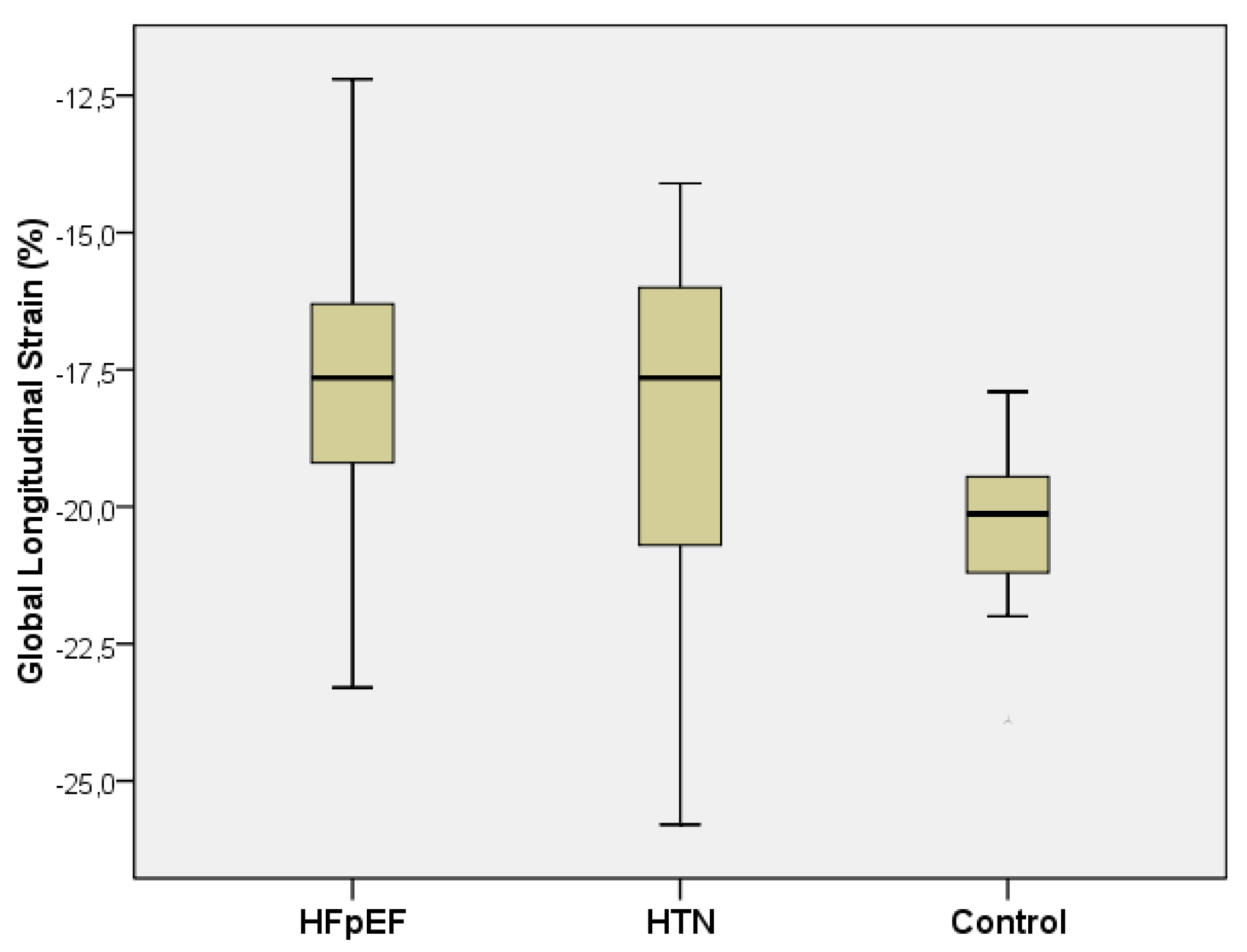
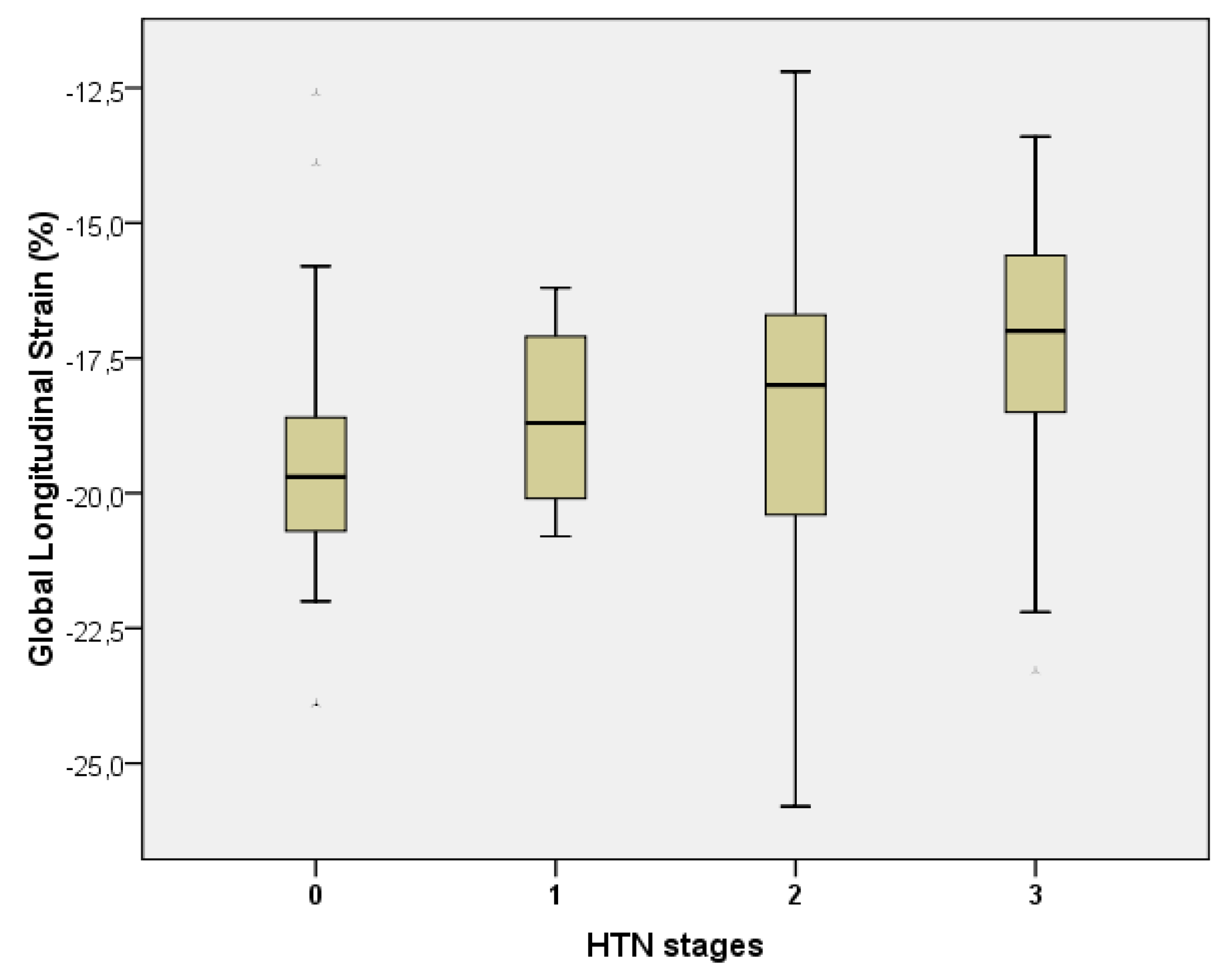
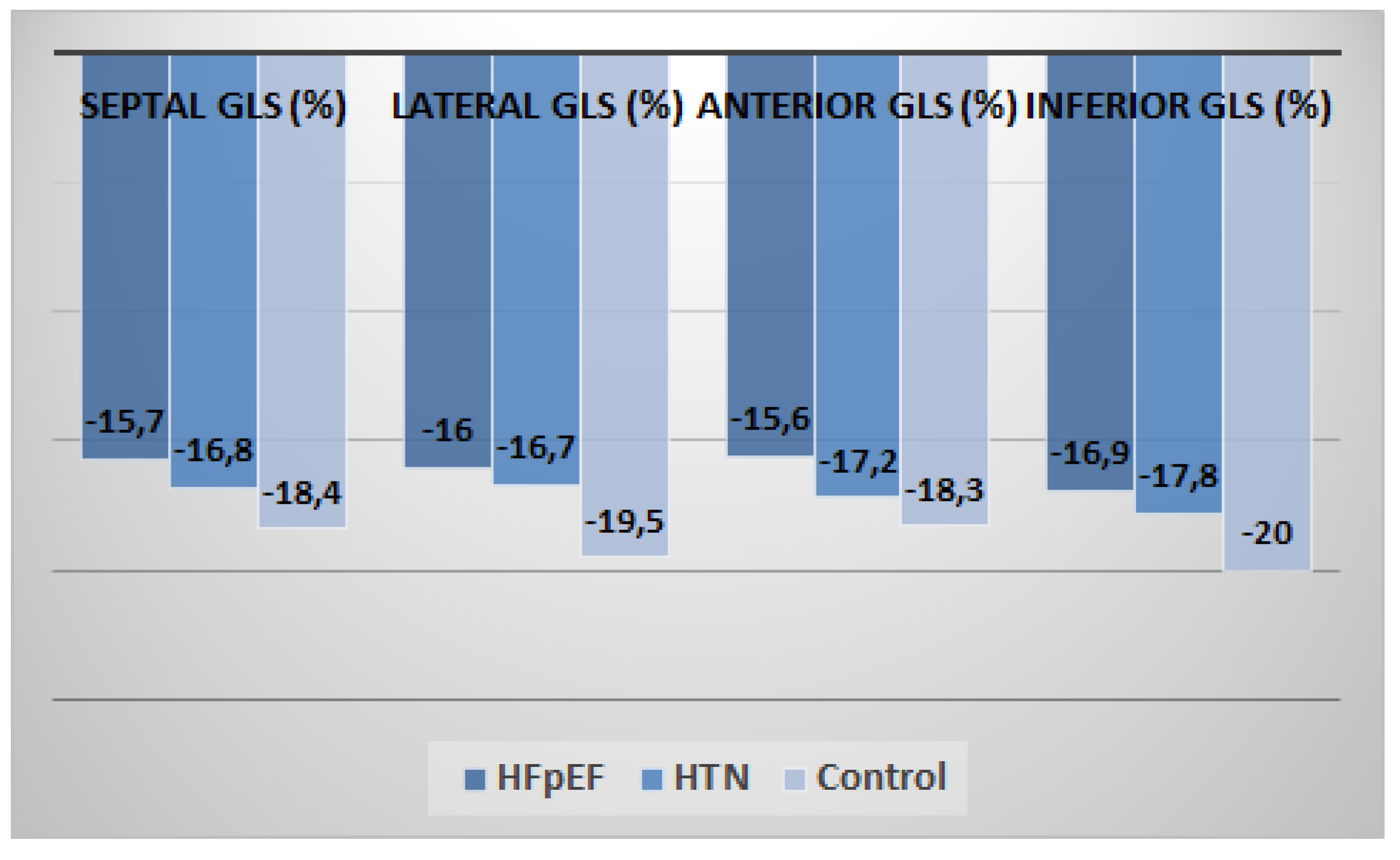
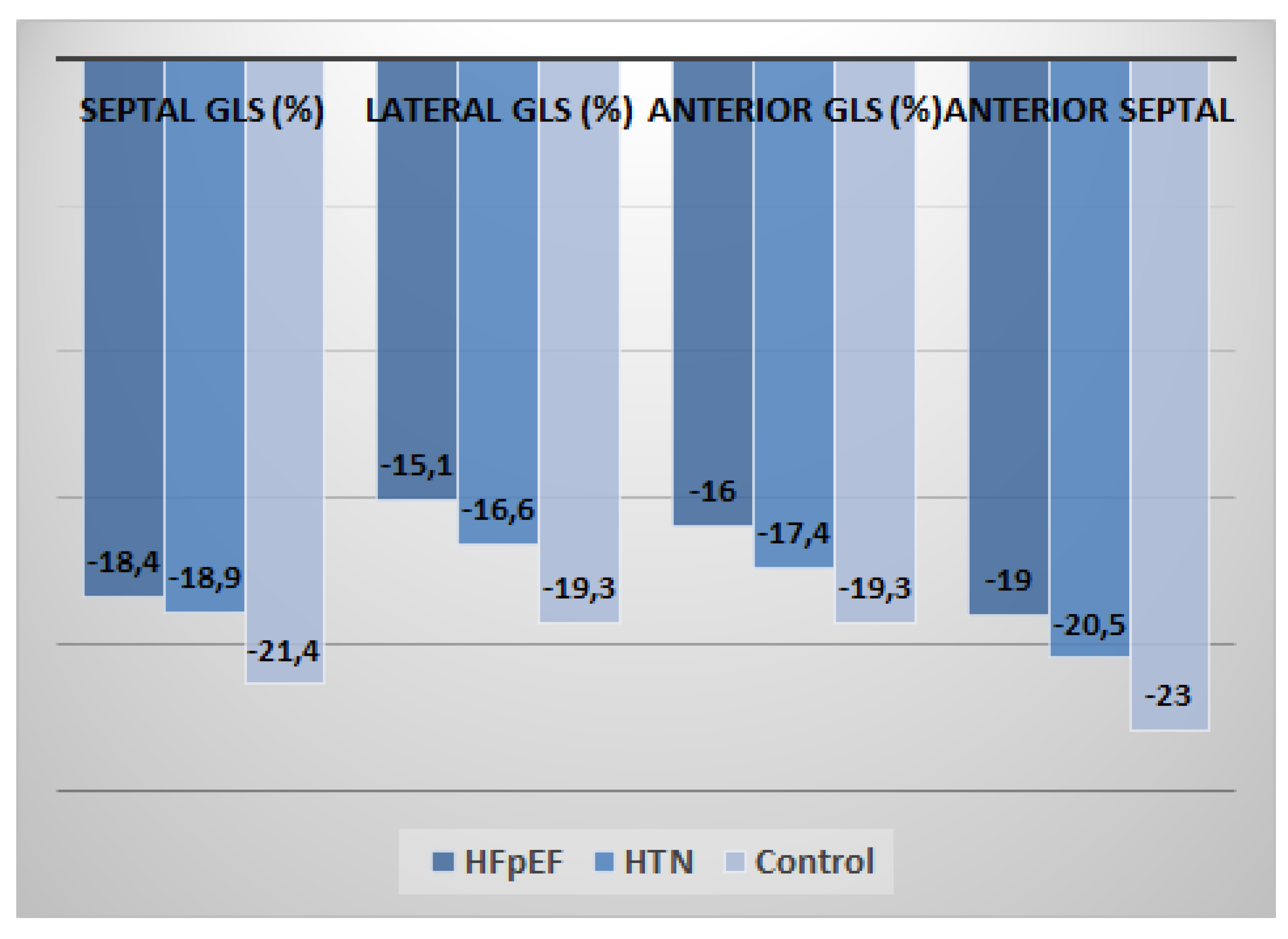
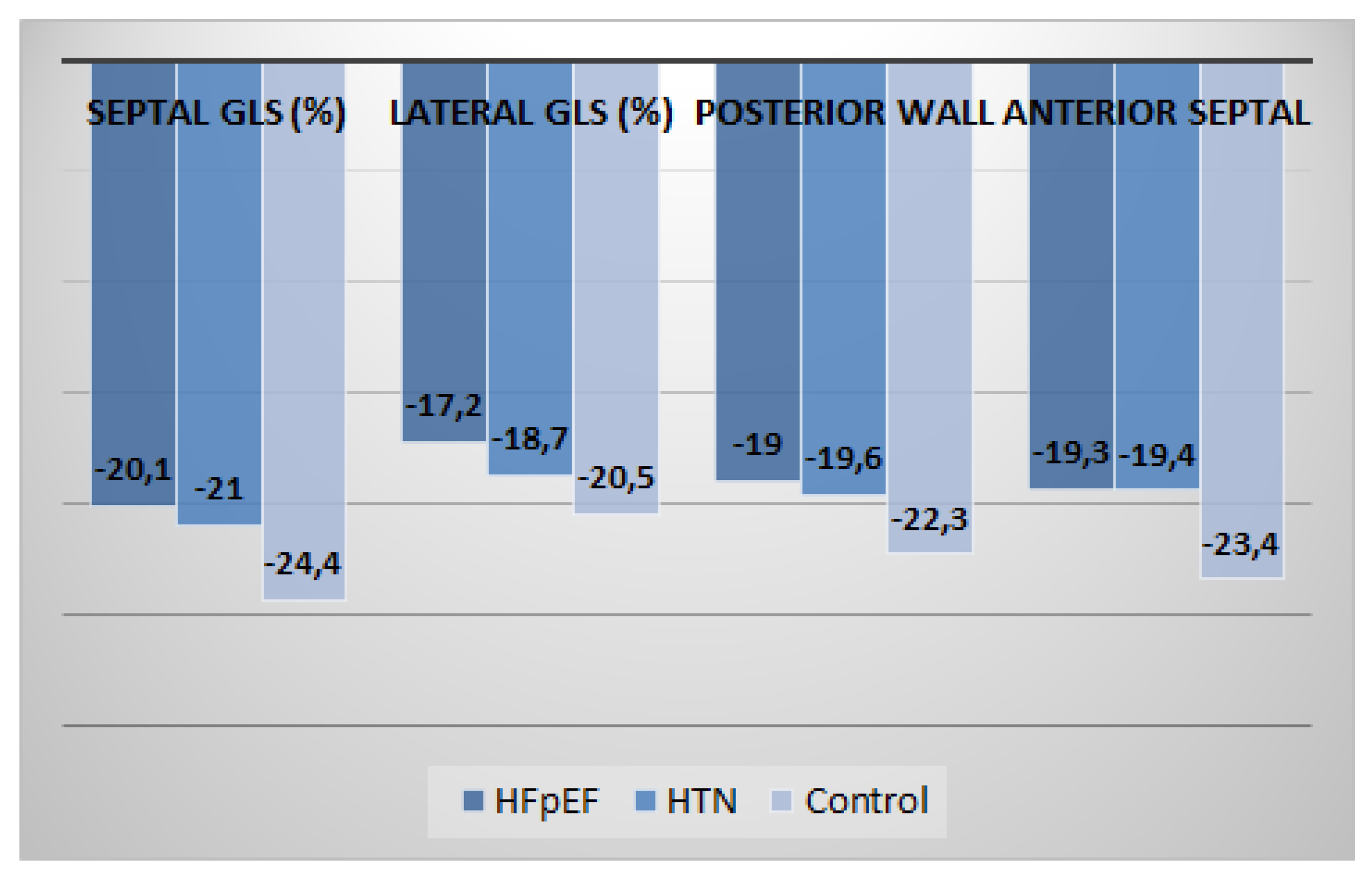
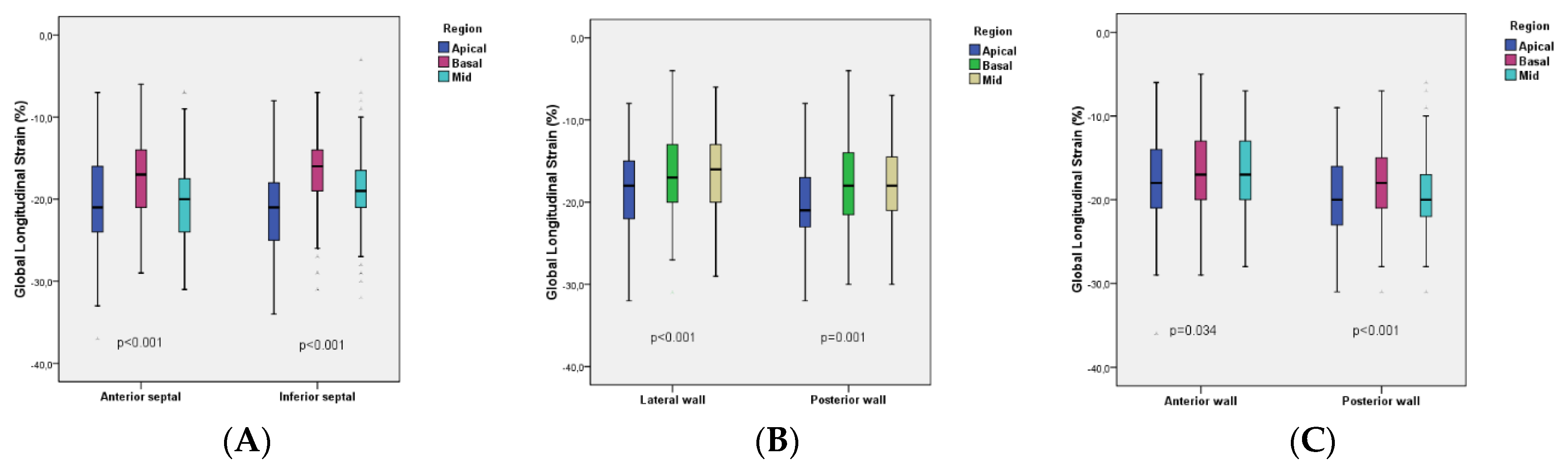
3.2. Speckle-Tracking Echocardiographic Parameters
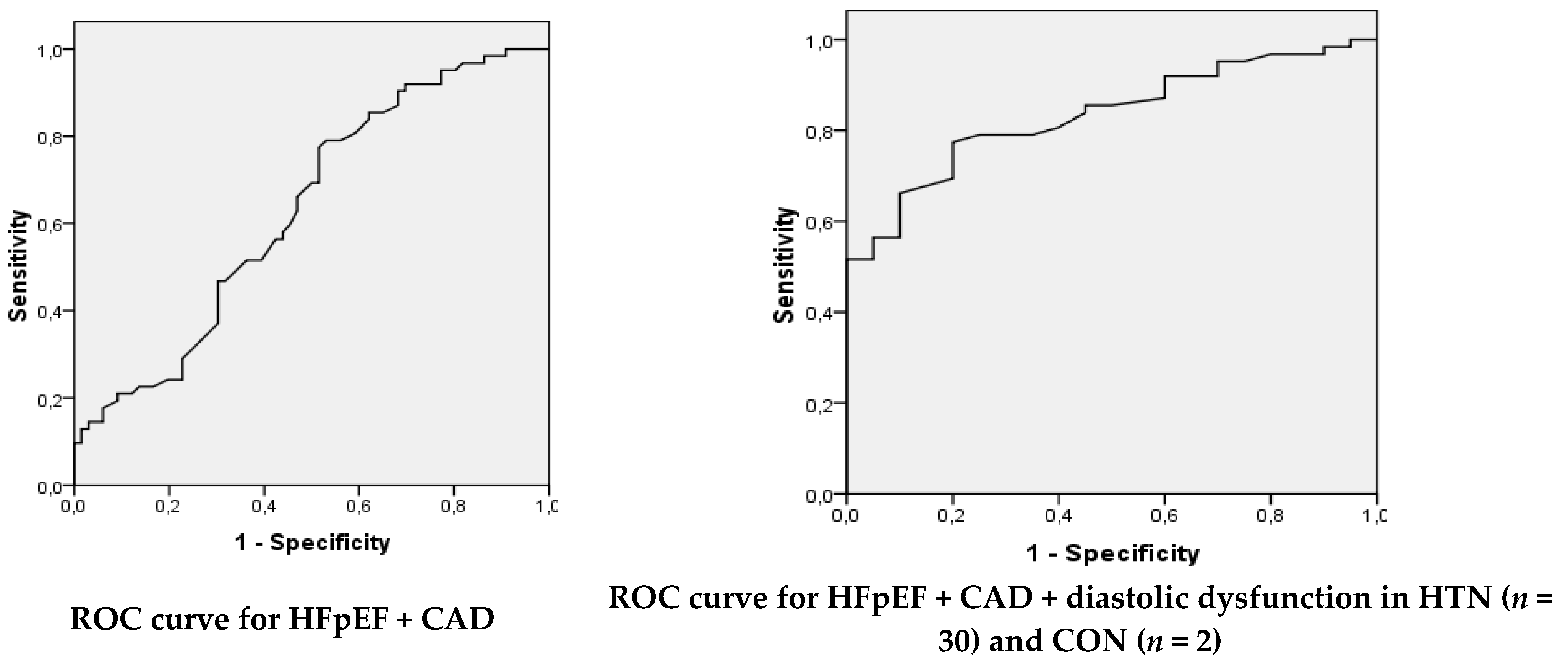
3.3. Diagnostic Performance of Global Longitudinal Strain
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Rigolli, M.; Whalley, G.A. Heart failure with preserved ejection fraction. J. Geriatr. Cardiol. 2013, 10, 369–376. [Google Scholar] [PubMed]
- Gunasekaran, P.; Panaich, S.; Briasoulis, A.; Cardozo, S.; Afonso, L. Incremental Value of Two Dimensional Speckle Tracking Echocardiography in the Functional Assessment and Characterization of Subclinical Left Ventricular Dysfunction. Curr. Cardiol. Rev. 2017, 13, 32–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsen, S.; Dahlslett, T.; Grenne, B.; Sjøli, B.; Smiseth, O.; Edvardsen, T.; Brunvand, H. Global longitudinal strain is a more reproducible measure of left ventricular function than ejection fraction regardless of echocardiographic training. Cardiovasc. Ultrasound 2019, 17, 18. [Google Scholar] [CrossRef] [Green Version]
- Buggey, J.; Alenezi, F.; Yoon, H.J.; Phelan, M.; DeVore, A.D.; Khouri, M.G.; Schulte, P.J.; Velazquez, E.J. Left ventricular global longitudinal strain in patients with heart failure with preserved ejection fraction: Outcomes following an acute heart failure hospitalization. ESC Heart Fail. 2017, 4, 432–439. [Google Scholar] [CrossRef]
- Kalam, K.; Otahal, P.; Marwick, T.H. Prognostic implications of global LV dysfunction: A systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart 2014, 100, 1673–1680. [Google Scholar] [CrossRef]
- Potter, E.; Marwick, T.H. Assessment of Left Ventricular Function by Echocardiography: The Case for Routinely Adding Global Longitudinal Strain to Ejection Fraction. JACC Cardiovasc. Imaging 2018, 11, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Marwick, T.H.; Shah, S.J.; Thomas, J.D. Myocardial Strain in the Assessment of Patients with Heart Failure: A Review. JAMA Cardiol. 2019, 4, 287–294. [Google Scholar] [CrossRef]
- Ma, C.; Luo, H.; Fan, L.; Liu, X.; Gao, C. Heart failure with preserved ejection fraction: An update on pathophysiology, diagnosis, treatment, and prognosis. Braz. J. Med. Biol. Res. 2020, 53, e9646. [Google Scholar] [CrossRef]
- Nieminen, M.S.; Brutsaert, D.; Dickstein, K.; Drexler, H.; Follath, F.; Harjola, V.P.; Hochadel, M.; Komajda, M.; Lassus, J.; Lopez-Sendon, J.L.; et al. EuroHeart Failure Survey II (EHFS II): A survey on hospitalized acute heart failure patients: Description of population. Eur. Heart J. 2006, 27, 2725–2736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gheorghiade, M.; Abraham, W.T.; Albert, N.M.; Greenberg, B.H.; O’Connor, C.M.; She, L.; Stough, W.G.; Yancy, C.W.; Young, J.B.; Fonarow, G.C. Systolic blood pressure at admission, clinical characteristics, and outcomes in patients hospitalized with acute heart failure. JAMA 2006, 296, 2217–2226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mentz, R.J.; Kelly, J.P.; von Lueder, T.G.; Voors, A.A.; Lam, C.S.P.; Cowie, M.R.; Kjeldsen, K.; Jankowska, E.A.; Atar, D.; Butler, J.; et al. Noncardiac Comorbidities in Heart Failure with Reduced Versus Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2014, 64, 2281–2293. [Google Scholar] [CrossRef] [Green Version]
- Halliday, B.P.; Senior, R.; Pennell, D.J. Assessing left ventricular systolic function: From ejection fraction to strain analysis. Eur. Heart J. 2021, 42, 789–797. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [PubMed]
- Levey, A.S.; Inker, L.A.; Coresh, J. GFR estimation: From physiology to public health. Am. J. Kidney Dis. 2014, 63, 820–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [PubMed]
- Haji, K.; Marwick, T.H. Clinical Utility of Echocardiographic Strain and Strain Rate Measurements. Curr. Cardiol. Rep. 2021, 23, 18. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Park, S.J.; Lee, S.C.; Chang, S.Y.; Kim, E.K.; Chang, S.A.; Choi, J.O.; Park, S.W.; Kim, S.M.; Choe, Y.H.; et al. Comparison of global and regional myocardial strains in patients with heart failure with a preserved ejection fraction vs hypertension vs age-matched control. Cardiovasc. Ultrasound 2020, 18, 44. [Google Scholar] [CrossRef] [PubMed]
- Kraigher-Krainer, E.; Shah, A.M.; Gupta, D.K.; Santos, A.; Claggett, B.; Pieske, B.; Zile, M.R.; Voors, A.A.; Lefkowitz, M.P.; Packer, M.; et al. Impaired systolic function by strain imaging in heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. 2014, 63, 447–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soufi Taleb Bendiab, N.; Meziane-Tani, A.; Ouabdesselam, S.; Methia, N.; Latreche, S.; Henaoui, L.; Monsuez, J.-J.; Benkhedda, S. Factors associated with global longitudinal strain decline in hypertensive patients with normal left ventricular ejection fraction. Eur. J. Prev. Cardiol. 2017, 24, 1463–1472. [Google Scholar] [CrossRef]
- Galderisi, M.; Esposito, R.; Schiano-Lomoriello, V.; Santoro, A.; Ippolito, R.; Schiattarella, P.; Strazzullo, P.; de Simone, G. Correlates of global area strain in native hypertensive patients: A three-dimensional speckle-tracking echocardiography study. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 730–738. [Google Scholar] [CrossRef] [Green Version]
- Ayoub, A.M.; Keddeas, V.W.; Ali, Y.A.; Okl, R.A.E. Subclinical LV Dysfunction Detection Using Speckle Tracking Echocardiography in Hypertensive Patients with Preserved LV Ejection Fraction. Clin. Med. Insights Cardiol. 2016, 10, CMC.S38407. [Google Scholar] [CrossRef] [Green Version]
- Ma, H.; Wu, W.C.; Xie, R.A.; Gao, L.J.; Wang, H. Correlation of Global Strain Rate and Left Ventricular Filling Pressure in Patients with Coronary Artery Disease: A 2-D Speckle-Tracking Study. Ultrasound Med. Biol. 2016, 42, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Biering-Sørensen, T.; Hoffmann, S.; Mogelvang, R.; Zeeberg Iversen, A.; Galatius, S.; Fritz-Hansen, T.; Bech, J.; Jensen, J.S. Myocardial strain analysis by 2-dimensional speckle tracking echocardiography improves diagnostics of coronary artery stenosis in stable angina pectoris. Circ. Cardiovasc. Imaging 2014, 7, 58–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcidi, G.M.; Esposito, R.; Evola, V.; Santoro, C.; Lembo, M.; Sorrentino, R.; Lo Iudice, F.; Borgia, F.; Novo, G.; Trimarco, B.; et al. Normal reference values of multilayer longitudinal strain according to age decades in a healthy population: A single-centre experience. Eur. Heart J. Cardiovasc. Imaging 2017, 19, 1390–1396. [Google Scholar] [CrossRef]
- Menting, M.E.; McGhie, J.S.; Koopman, L.P.; Vletter, W.B.; Helbing, W.A.; van den Bosch, A.E.; Roos-Hesselink, J.W. Normal myocardial strain values using 2D speckle tracking echocardiography in healthy adults aged 20 to 72 years. Echocardiography 2016, 33, 1665–1675. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Khoury, D.S.; Yue, Y.; Torre-Amione, G.; Nagueh, S.F. Preserved left ventricular twist and circumferential deformation, but depressed longitudinal and radial deformation in patients with diastolic heart failure. Eur. Heart J. 2008, 29, 1283–1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | HFpEF | HTN | Control | P test |
|---|---|---|---|---|
| n | 62 | 46 | 40 | |
| Age, years | 62.9 ± 8.57 | 61 ± 11.72 | 60.2 ± 8.73 | 0.385 b |
| Male sex, n (%) | 42 (67.7%) | 24 (52.2%) | 11 (55.0%) | 0.231 b |
| SBP, mmHg | 122.4 ± 21.61 | 136.5 ± 18.19 | 125.3 ± 9.89 | 0.018 a* |
| DBP, mmHg | 81.5 ± 12.91 | 79 ± 11.86 | 78.6 ± 9.16 | 0.458 a |
| HR, bpm | 72.5 ± 19.94 | 71 ± 12.56 | 74.1 ± 10.75 | 0.768 a |
| AF, n (%) | 8 (17.4%) | 3 (4.8%) | 0 (0.0%) | 0.010 b* |
| CKD # (yes) | 6 (9.7%) | 10 (21.7%) | 0 (0.0%) | 0.032 b* |
| NYHA classification at admission | ||||
| 0 | 9 (14.5%) | 46 (100.0%) | 40 (100.0%) | <0.001 b* |
| II | 37 (59.7%) | 0 (0.0%) | 0 (0.0%) | |
| III | 16 (25.8%) | 0 (0.0%) | 0 (0.0%) | |
| NYHA classification at discharge | ||||
| 0 | 13 (21.0%) | 46 (100.0%) | 40 (100.0%) | <0.001 b* |
| I | 24 (38.7%) | 0 (0.0%) | 0 (0.0%) | |
| II | 24 (38.7%) | 0 (0.0%) | 0 (0.0%) | |
| III | 1 (1.6%) | 0 (0.0%) | 0 (0.0%) | |
| HTN stages | ||||
| 0 | 0 (0%) | 0 (0.0%) | 40 (100.0%) | <0.001 b* |
| 1 | 10 (16.1%) | 3 (6.5%) | 0 (0.0%) | |
| 2 | 22 (35.5%) | 28 (60.9%) | 0 (0.0%) | |
| 3 | 30 (48.4%) | 15 (32.6%) | 0 (0.0%) | |
| Hemoglobin (g/dL) | 14.1 ± 1.64 | 14 ± 1.45 | 13.5 ± 1.46 | 0.339 a |
| WBCs (×109/L) | 7.8 ± 2.59 | 7.0 ± 1.58 | 7.7 ± 1.64 | 0.186 a |
| Fasting blood glucose (mg/dL) | 117.5 ± 40.08 | 116.6 ± 43.25 | 99.2 ± 6.26 | 0.159 a |
| Creatinine (mg/dL) | 1.0 ± 0.23 | 1.1 ± 0.41 | 0.9 ± 0.14 | 0.011 a* |
| K+ (mmEq/L) | 4.2 ± 0.42 | 4.2 ± 0.39 | 4.2 ± 0.24 | 0.939 a |
| Na+ (mmEq/L) | 140.5 ± 5.83 | 140.8 ± 4.17 | 142.4 ± 2.23 | 0.300 a |
| Risk factors | ||||
| Hypertension (yes) | 53 (85.48%) | 46 (100%) | 0 (0%) | <0.001 b* |
| Smoking (yes) | 17 (27.41%) | 15 (32.60%) | 9 (22.5%) | <0.001 b* |
| BMI, kg/m2 | 29.9 ± 4.47 | 28.4 ± 4.31 | 25.5 ± 2.08 | <0.001 a* |
| TC, mg/dL | 174.5 ± 31.45 | 181.8 ± 34.21 | 165 ± 19.75 | 0.021 a* |
| LDL-c, mg/dL | 109.8 ± 44.78 | 120.7 ± 53.13 | 88.9 ± 17.12 | 0.034 a* |
| HDL-c, mg/dL | 42.13 ± 8.55 | 39.46 ± 9.31 | 51.38 ± 9.66 | <0.001 a* |
| TG, mg/dL | 142.4 ± 65.45 | 144.0 ± 85.37 | 114.9 ± 23.72 | 0.249 a |
| T2DM, n (%) | 15 (24.2%) | 16 (34.8%) | 0 (0.0%) | 0.010 b* |
| Variables | HFpEF | HTN | Control | P test |
|---|---|---|---|---|
| n | 62 | 46 | 40 | |
| Medications | ||||
| ACEi or ARB | 29 (46.8%) | 25 (54.34%) | 0 (0.0%) | 0.043 b* |
| Beta-Blocker | 41 (66.1%) | 18 (39.2%) | 1 (2.5%) | <0.001 b* |
| Amiodarone | 7 (11.3%) | 1 (2.17%) | 0 (0.0%) | 0.019 b* |
| Aldosterone Antagonists | 22 (35.5%) | 12 (26.1%) | 0 (0.0%) | 0.001 b* |
| Furosemide | 21 (33.9%) | 5 (10.9%) | 0 (0.0%) | 0.002 b* |
| Aspirin | 48 (77.4%) | 23 (50.0%) | 0 (0.0%) | <0.001 b* |
| Antiplatelet Agent | 40 (64.5%) | 19 (41.3%) | 0 (0.0%) | <0.001 b* |
| Anticoagulant | 6 (9.7%) | 5 (10.9%) | 0 (0.0%) | 0.035 b* |
| Statin | 54 (87.1%) | 37 (80.4%) | 0 (0.0%) | <0.001 b* |
| Calcium Channel Blocker | 11 (17.7%) | 9 (19.56%) | 0 (0.0%) | 0.002 b* |
| Fibrates | 8 (12.9%) | 5 (10.9%) | 0 (0.0%) | 0.011 b* |
| Oral antidiabetic agents (metformin, sitagliptin) | 15 (24.2%) | 15 (32.60%) | 0 | <0.001 b* |
| Insulin | 3 (4.83%) | 1 (2.17) | 0 | 0.005 b* |
| Variables | HFpEF |
|---|---|
| n | 62 |
| The type of cardiovascular revascularization procedures | |
| CABG (yes) | 20 (32.25%) |
| PTCA (yes) | 32 (51.61%) |
| Thrombolyzed myocardial infarction (yes) | 10 (16.1%) |
| The coronary arteries involved | |
| RCA (yes) | 30 (48.38%) |
| LAD (yes) | 23 (37.1%) |
| Cx (yes) | 20 (32.3%) |
| Variables | HFpEF | HTN | Control | P test |
|---|---|---|---|---|
| n | 62 | 46 | 40 | |
| Echocardiographic parameter | ||||
| IVSd (cm) | 1.1 ± 0.2 | 1.1 ± 0.2 | 1.0 ± 0.1 | 0.252 b* |
| LVPWd (cm) | 1.1 ± 0.1 | 1.1 ± 0.2 | 1.0 ± 0.1 | 0.273 b* |
| LVEDD (cm) | 4.7 ± 0.4 | 4.5 ± 0.5 | 4.5 ± 0.2 | 0.103 a |
| LVEDV (mL) | 90.0 ± 11.5 | 100.0 ± 33.5 | 86.0 ± 10.5 | <0.001 b* |
| LVESV (mL) | 39.5 ± 9 | 40.0 ± 6.5 | 32.0 ± 2.8 | <0.001 b* |
| LAVI by area-length method (mL/m2) | 37.7 ± 6.7 | 37.5 ± 5.5 | 35.3 ± 5.6 | 0.293 a |
| LVEF (%) | 55.0 ± 5.0 | 56.0 ± 8 | 56.0 ± 4.0 | 0.262 b |
| E (m/s) | 0.8 ± 0.2 | 0.6 ± 0.4 | 0.8 ± 0.1 | 0.002 b* |
| A (m/s) | 0.6 ± 0.1 | 0.7 ± 0.2 | 0.5 ± 0.1 | <0.001 a* |
| E/A < 1 (yes) | 62 (100%) | 30 (65.21%) | 2 (5%) | <0.001 b* |
| LVH (yes) | 62 (100%) | 36 (78.26%) | 0 (0%) | 0.001 b* |
| Sample | Cutoff | AUC | Std. Error | Asymptotic Sig. | Asymptotic 95% Confidence Interval | SN (%) | SP (%) | PPV (%) | NPV (%) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||||||
| HFpEF + CAD | −19.45 | 0.632 | 0.049 | 0.010 * | 0.536 | 0.728 | 79.03 | 46.97 | 58.33 | 70.45 |
| HFpEF + CAD + diastolic dysf in HTN (n = 30) and CON (n = 2) | −19.35 | 0.833 | 0.045 | <0.001 * | 0.746 | 0.921 | 77.42 | 80.00 | 92.31 | 53.33 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoichescu-Hogea, G.; Buleu, F.N.; Christodorescu, R.; Sosdean, R.; Tudor, A.; Ember, A.; Brie, D.M.; Drăgan, S. Contribution of Global and Regional Longitudinal Strain for Clinical Assessment of HFpEF in Coronary and Hypertensive Patients. Medicina 2021, 57, 1372. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121372
Stoichescu-Hogea G, Buleu FN, Christodorescu R, Sosdean R, Tudor A, Ember A, Brie DM, Drăgan S. Contribution of Global and Regional Longitudinal Strain for Clinical Assessment of HFpEF in Coronary and Hypertensive Patients. Medicina. 2021; 57(12):1372. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121372
Chicago/Turabian StyleStoichescu-Hogea, Gheorghe, Florina Nicoleta Buleu, Ruxandra Christodorescu, Raluca Sosdean, Anca Tudor, Andreea Ember, Daniel Miron Brie, and Simona Drăgan. 2021. "Contribution of Global and Regional Longitudinal Strain for Clinical Assessment of HFpEF in Coronary and Hypertensive Patients" Medicina 57, no. 12: 1372. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57121372