
Meditative Movement, Energetic, and Physical Analyses of Three Qigong Exercises: Unification of Eastern and Western Mechanistic Exercise Theory

Abstract
:1. Introduction
1.1 Study Rationale
1.2. Clinical Research Evidence
1.3. Theoretical and Conceptual Framework
1.4. Meditative Movement (MM)
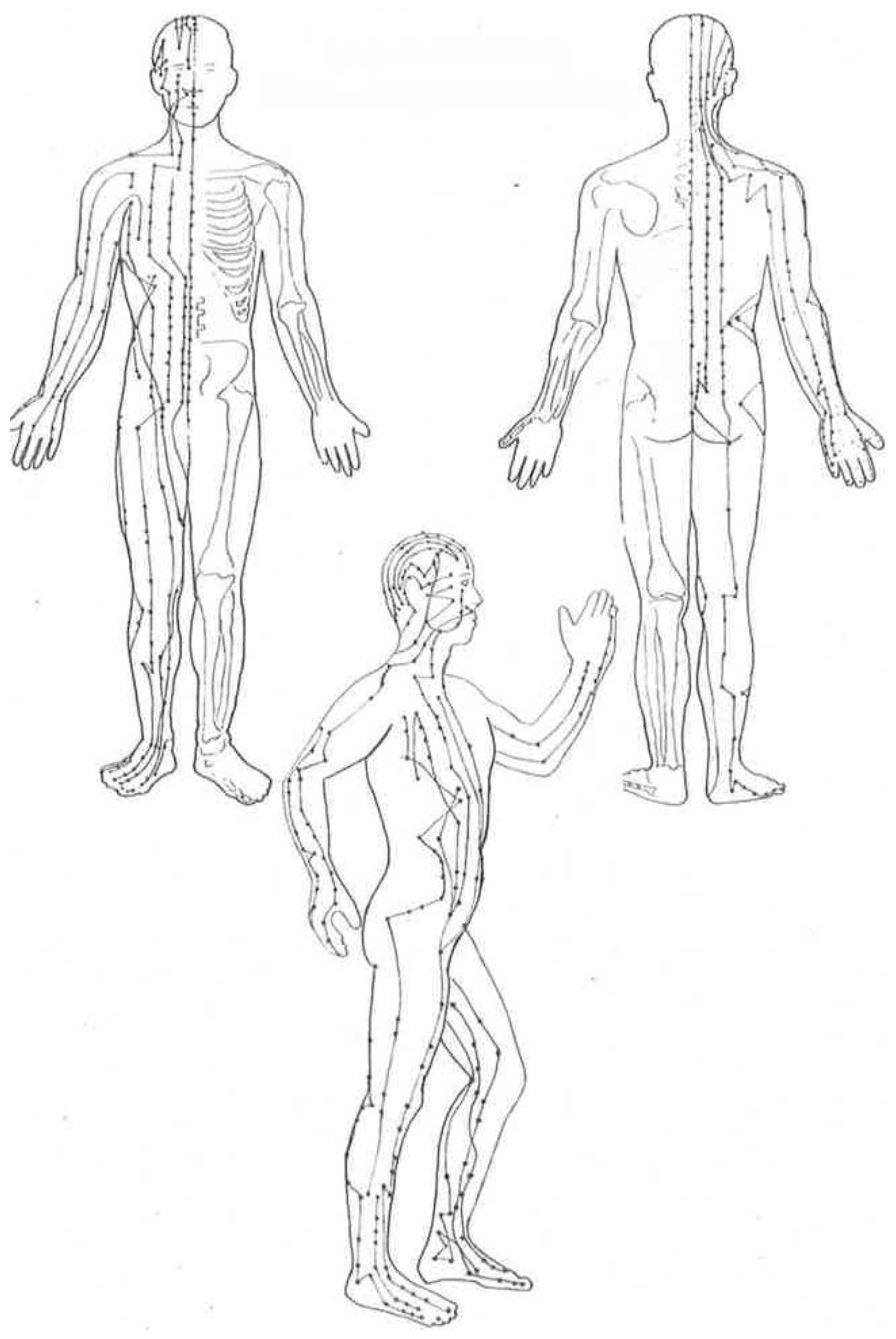
1.5. Energy Theory
1.6. Physical: Western Medicine and Modern Exercise Science Theory
1.7. Purpose
2. Methods
2.1. Design
2.2. Research Team
2.3. Exercise Selection Process
2.4. Data Extraction and Results
2.5. Data Analysis
3. Results
4. Analyses
4.1. Meditative Aspect
4.2. Energetic Aspect
4.3. Physical Aspect
4.4. Meditative Aspect
4.5. Energetic Aspect
4.6. Physical Aspect
4.7. Meditative Aspect
4.8. Energetic Aspect
4.9. Physical Aspect
5. Discussion
5.1. Meditative Aspects
5.2. Energetic Mechanisms
5.3. Physical Mechanisms
5.4. An Example of Application Challenge
5.5. Future Research
5.6. Limitations
6. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lui, T.; Qiang, X.M. (Eds.) Chinese Medical Qigon; Singing Dragon/Jessica Kingsley Publishers: London, UK, 2010; ISBN 978-0-85701-017-9. [Google Scholar]
- Liang, S.-Y.; Wu, W.C.; Breiter-Wu, D. Qigong Empowerment: A Guide to Medical, Taoist, Buddhist, and Wushu Energy Cultivation; Way of the Dragon: East Providence, RI, USA, 1997; ISBN 1-889659-02-9. [Google Scholar]
- Picard, G. Heal Yourself with Qigong; Spiral Graphics: Catharines, ON, Canada, 2009; ISBN 978-0-9865155-0-7. [Google Scholar]
- Chodzko-Zajko, W.; Jahnke, R. National Expert Meeting on Qigong and Tai Chi: Consensus Report; University of Illinois at Urbana-Champaign: Urbana, IL, USA, 2005; Available online: http://healerwithinfoundation.org/National_Expert_Meeting/ (accessed on 10 October 2016).
- Yang, G.-Y.; Wang, L.-Q.; Ren, J.; Zhang, Y.; Li, M.L.; Zhu, Y.T.; Cheng, Y.J.; Li, W.Y.; Wayne, P.M.; Liu, J.P. Evidence Base of Clinical Studies on Tai Chi: A Bibliometric Analysis. Scherer, R.W. Ed. PLoS ONE 2015, 10, e0120655. [Google Scholar] [CrossRef]
- Solloway, M.R.; Taylor, S.L.; Shekelle, P.G.; Miake-Lye, I.M.; Beroes, J.M.; Shanman, R.M.; Hemplel, S. An evidence map of the effect of Tai Chi on health outcomes. Syst. Rev. 2016, 5, 126. [Google Scholar] [CrossRef]
- Huang, Z.G.; Feng, Y.H.; Li, Y.H.; Lv, C.S. Systematic review and meta-analysis: Tai Chi for preventing falls in older adults. BMJ Open 2017, 7, e013661. [Google Scholar] [CrossRef]
- Kumar, A.; Delbaere, K.; Zijlstra, G.A.; Carpenter, H.; Iliffe, S.; Masud, T.; Skelton, D.; Morris, R.; Kendrick, D. Exercise for reducing fear of falling in older people living in the community: Cochrane systematic review and meta-analysis. Age Ageing 2016, 45, 345–352. [Google Scholar] [CrossRef]
- Li, F.; Harmer, P. Economic evaluation of a Tai JI Quan intervention to reduce falls in people with Parkinson disease, Oregon, 2008–20011. Pre. Chronic. Dis. 2015, 12, E120. [Google Scholar] [CrossRef]
- Klein, P.J.; Schneider, R.; Rhoads, C.J. Qigong in cancer care: A systematic review and construct analysis of Qigong therapy. Support. Care Cancer 2016, 24, 3209–3222. [Google Scholar] [CrossRef]
- Oh, B.; Butow, P.; Mullan, B.; Clarke, S.; Beale, P.; Pavlakis, N.; Kothe, E.; Lam, L.; Rosenthal, D. Impact of medical Qigong on quality of life, fatigue, mood and inflammation in cancer patients: A randomized controlled trial. Ann. Oncol. 2010, 21, 608–614. [Google Scholar] [CrossRef]
- Liu, P.; You, J.; Sun, Y.; He, Y.; Sit, H.; Jia, L.; Wong, M.; Xia, Z.; Zheng, X.; Wang, Z.; et al. The efficacy of Guolin-Qigong on the mind-body health of Chinese women with breast cancer: A randomized controlled trial. Qual. Life Res. 2017, 18, 1–11. [Google Scholar] [CrossRef]
- Irwin, M.R.; Olmstead, R.; Carrillo, C.; Sadeghi, N.; Nicassio, P.; Ganz, P.; Bower, J.E. Tai Chi Chih Compared With Cognitive Behavioral Therapy for the Treatment of Insomnia in Survivors of Breast Cancer: A Randomized, Partially Blinded, Noninferiority Trial. J. Clin. Oncol. 2017. [Google Scholar] [CrossRef]
- Zeng, Y.; Luo, T.; Xie, H.; Huang, M.; Cheng, A.S. Health benefits of qigong or Tai Chi for cancer patients: A systematic review and meta-analyses. Complement. Ther. Med. 2014, 22, 173–186. [Google Scholar] [CrossRef]
- Wang, X.-Q.; Pi, Y.-L.; Chen, P.-J.; Liu, Y.; Wang, R.; Li, X.; Chen, B.-L.; Zhu, Y.; Yang, Y.-J.; Niu, Z.-N. Traditional Chinese Exercise for Cardiovascular Diseases: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. AM Heart Assoc. 2016, 5, e002562. [Google Scholar] [CrossRef]
- Xiong, X.; Wang, P.; Zhang, Y. Qigong for hypertension: A systematic review Medicine (Baltimore). Medicine 2015, 94, e352. [Google Scholar] [CrossRef]
- Nery, R.M.; Zanini, M.; Ferrari, J.N.; Silva, C.A.; Farias, L.F.; Comel, J.C.; Belli, K.C.; da Silveira, A.D.; Santos, A.C.; Stein, R. Tai Chi Chuan for Cardiac Rehabilitation in Patients with Coronary Arterial Disease. Arq. Bras. Cardiol. 2014, 102, 588–592. [Google Scholar] [CrossRef]
- Gu, Q.; Wu, S.J.; Zheng, Y.; Zhang, Y.; Liu, C.; Hou, J.C.; Zhang, K.; Fang, X.M. Tai Chi Exercise for Patients with Chronic Heart Failure: A Meta-analysis of Randomized Controlled Trials. Am. J. Phys. Med. Rehabil. 2017. [Google Scholar] [CrossRef]
- Ngai, S.P.; Jones, A.Y.; Tam, W.W. Tai Chi for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2016, 7, CD009953. [Google Scholar] [CrossRef]
- Guo, J.B.; Chen, B.L.; Lu, Y.M.; Zhang, W.Y.; Zhu, Z.J.; Yang, Y.J.; Zhu, Y. Tai Chi for improving cardiopulmonary function ad quality of life in patients with chronic obstructive pulmonary disease. Clin. Rehabil. 2016, 30, 750–764. [Google Scholar] [CrossRef]
- Song, R.; Grabowska, W.; Park, M.; Osypiuk, K.; Vergara-Diaz, G.P.; Bonato, P.; Hausdorff, J.M.; Fox, M.; Sudarsky, L.R.; Macklin, E.; et al. The impact of Tai Chi and Qigong mind-body exercises on motor and non-motor function and quality of life in Parkinson’s disease: A systematic review and meta-analysis. Parkinsonism Relat. Disord. 2017, 41, 3–13. [Google Scholar] [CrossRef]
- Zhou, J.; Yin, T.; Gao, Q.; Yang, X.C. A Meta-Analysis on the Efficacy of Tai Chi in Patients with Parkinson’s Disease between 2008 and 2014. Evid.-Based Complement. Altern. Med. eCAM 2015, 2015. [Google Scholar] [CrossRef]
- Xiang, Y.; Lu, L.; Chen, W. Does Tai Chi relieve fatigue? A systematic review and meta-analysis of randomized controlled trials. PLoS ONE 2017, 12, e0174872. [Google Scholar] [CrossRef]
- Chan, J.S.M.; Ho, R.T.H.; Chung, F.-F.; Wang, C.-W.; Yao, T.-W.; Ng, S.-N.; Chan, C.L.W. Qigong Exercise Alleviates Fatigue, Anxiety, and Depressive Symptoms, Improves Sleep Quality, and Shortens Sleep Latency in Persons with Chronic Fatigue Syndrome-Like Illness. Evid. Based Complement. Altern. Med. 2014, 2014. [Google Scholar] [CrossRef]
- Wong, A.; Figueroa, A.; Sanchez-Gonzalez, M.A.; Son, W.M.; Chernykh, O.; Park, S.Y. Effectiveness of Tai Chi on Cardiac Autonomic Function and Symptomatology in women with fibromyalgia: A randomized controlled trial. J. Aging Phys. Act. 2017, 28, 1–26. [Google Scholar] [CrossRef]
- Lynch, M.; Sawynok, J.; Hiew, C.; Marcon, D. A randomized controlled trial of qigong for fibromyalgia. Arthr. Res. Ther. 2012, 14, R178. [Google Scholar] [CrossRef]
- Zou, L.; SasaKi, J.E.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M. A Systematic Review and Meta-Analysis Baduanjin Qigong for Health Benefit: Randomized Controlled Trials. Evid. Based Complement. Altern. Med. 2017, 2017, 4548706. [Google Scholar] [CrossRef]
- Huston, P.; McFarlane, B. Health benefits of Tai Chi. What is the evidence? Can. Fam. Phys. 2016, 62, 881–890. [Google Scholar]
- Larkey, L.; Jahnke, R.; Etnier, J.; Gonzalez, J. Meditative movement as a category of exercise: Implications for research. J. Phys. Act. Health. 2009, 6, 230–238. [Google Scholar] [CrossRef]
- Payne, P.; Crane-Godreau, M.A. Meditative Movement for Depression and Anxiety. Front. Psychiatry 2013, 4, 71. [Google Scholar] [CrossRef]
- Benson, H. The Relaxation Response; HarperCollins e-books: New York, NY, USA, 2009. [Google Scholar]
- Pal, G.K.; Velkumary, S. Effect of short-term practice of breathing exercises on autonomic functions in normal human volunteers. Indian J. Med. Res. 2004, 120, 115–121. [Google Scholar]
- Mourya, M.; Mahajan, A.S.; Singh, N.P.; Jain, A.K. Effect of slow- and fast-breathing exercises on autonomic functions in patients with essential hypertension. J. Altern. Complement. Med. 2009, 15, 711–717. [Google Scholar] [CrossRef]
- Sawynok, J. Qigong, Parasympathetic Function and Fibromyagia. Fibrom Open Access. 2016, 1, 107. [Google Scholar] [CrossRef]
- Tsakiris, M.; Tajadura-Jimenez, A.; Costantini, M. Just a heartbeat away from one’s body: Interoceptive sensitivity predicts malleability of body-representations. Proc. R. Soc. B 2011, 278, 2470–2476. [Google Scholar] [CrossRef]
- Ahn, A.C.; Colbert, A.P.; Anderson, B.J.; Martinsen, O.G.; Hammerschiag, R.; Cina, S.; Wayne, P.M.; Lanagevin, H.M. Electrical properties of acupuncture points and meridians: A systematic review. Bioelectromagnetics 2008, 29, 245–256. [Google Scholar] [CrossRef]
- Jayasuriya, A. Clinical Acupuncture; B. Jain Publishers: New Delhi, India, 2002. [Google Scholar]
- Grolleau-Julius, A.; Ray, D.; Yung, R.L. The Role of Epigenetics in Aging and Autoimmunity. Clin. Rev. Allergy Immunol. 2010, 39, 42–50. [Google Scholar] [CrossRef]
- Lin, H.C.; Lin, H.P.; Yu, H.H.; Wang, L.C.; Lee, J.H.; Lin, Y.T.; Yang, Y.H.; Li, P.Y.; Sun, W.Z.; Chiang, B.L. Tai-Chi-Chuan Exercise Improves Pulmonary Function and Decreases Exhaled Nitric Oxide Level in Both Asthmatic and Nonasthmatic Children and Improves Quality of Life in Children with Asthma. Evid. Based Complement. Altern. Med. 2017, 2017, 6287642. [Google Scholar] [CrossRef]
- Xia, W.G.; Zheng, C.J.; Zheng, X.; Wang, J. Effects of “nourishing liver and kidney” acupuncture therapy on expression of brain derived neurotrophic factor and synaptophysin after cerebral ischemia reperfusion in rats. J. Huazhong Univ. Sci. Technol. Med. 2017, 37, 271–278. [Google Scholar] [CrossRef]
- Yin, C.; Buchheit, T.E.; Park, J.I. Acupuncture for chronic pain: An update and critical overview. Curr. Opin. Anaesthesiol. 2017, 30, 583–592. [Google Scholar] [CrossRef]
- Schroeder, S.; Burnis, J.; Denton, A.; Krasnow, A.; Raghu, T.S.; Mathis, K. Effectiveness of Acupuncture Therapy on Stress in a Large Urban College Population. Acupunct. Meridian Stud. 2017, 10, 165–170. [Google Scholar] [CrossRef]
- Ural, F.G.; Öztürk, G.T. The Acupuncture Effect on Median Nerve Morphology in Patients with Carpal Tunnel Syndrome: An Ultrasonographic Study. Evid. Based Complement. Altern. Med. 2017, 2017, 7420648. [Google Scholar] [CrossRef]
- McDonald, J.L.; Smith, P.K.; Smith, C.A.; Changli Xue, C.; Golianu, B.; Cripps, A.W. Effect of acupuncture on house dust mite specific IgE, substance P, and symptoms in persistent allergic rhinitis. Ann. Allergy Asthma Immunol. 2016, 116, 497–505. [Google Scholar] [CrossRef]
- Stoicea, N.; Gan, T.; Joseph, N.; Uribe, A.; Pandya, J.; Dalal, R.; Bergese, S.D. Alternative Therapies for the Prevention of Postoperative Nausea and Vomiting. Front. Med. 2015, 2, 87. [Google Scholar] [CrossRef]
- Zhang, R.Q.; Tan, J.; Li, F.Y.; Ma, Y.H.; Han, L.X.; Yang, X.L. Acupuncture for the treatment of obesity in adults: A systematic review and meta-analysis. Postgrad. Med. J. 2017. [Google Scholar] [CrossRef]
- Baldwin, A.L.; Trent, N.L. An integrative review of scientific evidence for reconnective healing. J. Altern. Complement. Med. 2017. [Google Scholar] [CrossRef]
- McKee, P.; Hannah, S.; Priganc, V.W. Orthotic considerations for dense connective tissue and articular cartilage—The need for optimal movement and stress. J. Hand Ther. 2012, 25, 233–242. [Google Scholar] [CrossRef]
- Mow, V.C.; Proctor, C.S.; Kelly, M.A. Biomechanics of articular cartilage. In Basic Biomechanics of the Musculoskeletal System, 3rd ed.; Nordin, M., Frankel, V.H., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Cummings, G.S.; Tillman, L.J. Remodeling of dense connective tissue in normal adult tissues. In Dynamics of Human Biologic Tissues; Currier, D.P., Nelson, R.M., Eds.; F.A. Davis Company: Philadelphia, PA, USA, 1992; pp. 45–73. [Google Scholar]
- Salter, R.B. The physiologic basis of continuous passive motion for articular cartilage healing and regeneration. Hand Clin. 1994, 10, 211–219. [Google Scholar]
- Salter, R.B. Continuous Passive Motion (CPM): A Biological Concept for the Healing and Regeneration of Articular Cartilage, Ligaments, and Tendons: From Its Origination to Research to Clinical Applications; Williams & Wilkins: Philadelphia, PA, USA, 1993. [Google Scholar]
- Findley, T.; Schleip, R. Introduction. In Fascia Research: Basic Science and Implications for Conventional and Complementary Health Care; Findley & R Schleip, T.W., Ed.; Elsevier: Munich, Germany, 2007; p. 2e9. [Google Scholar]
- Schleip, R.; Findley, T.W.; Chaitow, L.; Huijing, P.A. (Eds.) Fascia: The Tensional Network of the Human Body; Churchill Livingstone Elsevier: Edinburgh, UK, 2012. [Google Scholar]
- Barker, D. The morphology of muscle receptors. In Handbook of Sensory Physiology, Vol III: Muscle Receptors; Barker, D., McIntyre, A., Eds.; Springer: New York, NY, USA, 2012. [Google Scholar]
- Schleip, R. Fascial plasticity—A new neurobiological explanation. J. Bodyw. Mov. Ther. 2003, 7, 11–19. [Google Scholar] [CrossRef]
- Ratey, J.J.; Loehr, J.E. The positive impact of physical activity on cognition during adulthood: A review of underlying mechanisms, evidence and recommendations. Rev. Neurosci. 2011, 22, 171–185. [Google Scholar] [CrossRef]
- Al-Yahya, E.; Dawes, H.; Smith, L.; Dennis, A.; Howells, K.; Cockburn, J. Cognitive motor interference while walking: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2011, 35, 715–728. [Google Scholar] [CrossRef]
- Wollesen, B.; Voelcker-Rehage, C. Training effects on motor-cognitive dual-task performance in older adults: A systematic review. EURAPA 2014, 11, 5–24. [Google Scholar] [CrossRef]
- Eggenberger, P.; Theill, N.; Holenstein, S.; Schumacher, V.; de Bruin, E.D. Multicomponent physical exercise with simultaneous cognitive training to enhance dual-task walking of older adults: A secondary analysis of a 6-month randomized controlled trial with I-year follow-up. Clin. Interv. Aging 2015, 28, 1711–1732. [Google Scholar] [CrossRef]
- Wayne, P.M.; Manor, B.; Novak, V.; Costa, M.D.; Hausdorff, J.M.; Goldberger, A.L.; Ahn, A.C.; Yeh, G.Y.; Peng, C.-K.; Lough, M.; et al. A systems biology approach to studying Tai Chi, physiological complexity and healthy aging: Design and rationale of a pragmatic randomized controlled trial. Contemp. Clin. Trials 2014, 34, 21–34. [Google Scholar] [CrossRef]
- Zheng, G.; Liu, F.; Li, S.; Huang, M.; Tao, J.; Chen, L. Tai Chi and the protection of cognitive ability: A systematic review of prospective studies in healthy adults. J. Prev. Med. 2015, 49, 89–97. [Google Scholar] [CrossRef]
- Tao, J.; Chen, X.; Egorova, N.; Liu, J.; Xue, X.; Wang, Q.; Zheng, G.; Li, M.; Hong, W.; Sun, S.; et al. Tai Chi Chuan and Baduanjin practice modulates functional connectivity of the cognitive control network in older adults. Sci. Rep. 2017, 7, 41581. [Google Scholar] [CrossRef]
- Voss, D.E.; Ionta, M.K.; Myers, J.W. Proprioceptive Neuromuscular Facilitation: Patterns and Techniques, 3rd ed.; Lippencott-Raven Publishers: Philadelphia, PA, USA, 1985; ISBN 0061425958. [Google Scholar]
- Ho, R.H.; Chan, M.P.H.; Wang, C.-W.; Lau, B.W.M.; Therefore, K.F.; Yuen, L.P.; Sham, J.S.T.; Chan, C.L.W. A randomized controlled trial of qigong exercise on fatigue symptoms, functioning, and telomerase activity in persons with chronic fatigue or Chronic Fatigue Syndrome. Ann. Behav. Med. 2012, 44, 160–170. [Google Scholar] [CrossRef] [Green Version]
- Schmalzl, L.; Crane-Godreau, M.A.; Payne, P. Movement-based embodied contemplative practices: Definitions and paradigms. Front. Hum. Neurosci. 2014, 14, 205. [Google Scholar] [CrossRef]
- Wu, H. A Life Dedicated to Marial Artsand Healin. In Chi-Kung, Tai-Chi and Fan; Available online: Helen Wu/www.masterhelenwu.com (accessed on 1 August 2017).
- People’s Medical Publishing House, Beijing, China. The Chinese Way to a Long and Healthy Life; Bell Publishing: New York, NY, USA, 1987. [Google Scholar]
- Cohen, K.S. The Way of Qigong; Ballintine Books: New York, NY, USA, 1997. [Google Scholar]
- Koskimies, K.; Sutinene, P.; Aaito, H.; Starck, J.; Toppila, E.; Kaksonen, R.; Ishizaki, H.; Alaranta, H.; Pyykkó, I. Postural stability, neck proprioception and tension neck. Acta Otolarvngol. Suppl. 1997, 529, 95–97. [Google Scholar] [CrossRef]
- Magnusson, M.; Anderson, G.; Gomez, S.; Johansson, R.; Mártensson, A.; Karlberg, M.; Fransson, P.A. Cervical muscle afferents play a dominant role over vestibular afferents during bilateral vibration of neck muscles. J. Vestib. Res. 2006, 16, 127–136. [Google Scholar]
- Gracovetsky, S. The Spinal Engine; Springer: New York, NY, USA, 1989. [Google Scholar]
- Schleip, R. Fascial plasticity—A new neurobiological explanation. J. Bodyw. Mov. Ther. 2003, 7 Pt 1, 11–19. [Google Scholar]
- Boissonnault, W.; Donatelli, R. The Influence of Hallux Extension on the Foot during Ambulation. JOSPT 1984, 5, 240–242. [Google Scholar] [CrossRef]
- Voss, D. Proprioceptive Neuromuscular Facilitation; Harper and Row: Philadelphia, PA, USA, 1985. [Google Scholar]
- Acevedo, B.P.; Pospos, S.; Lavretsky, H. The Neural Mechanisms of Meditative Practices: Novel Approaches for Healthy Aging. Curr. Behav. Neurosci. Rep. 2016, 3, 328–339. [Google Scholar] [CrossRef]
- Hölzel, B.K.; Carmody, J.; Vangel, M.; Congleton, C.; Yerramsetti, S.M.; Gard, T.; Lazar, S.W. Mindfulness practice leads to increases in regional brain gray matter density. Psychiatry Res. 2011, 191, 36–43. [Google Scholar] [CrossRef]
- Upledger, J.E. CranioSacral Therapy: What It Is, How It Works; North Atlantic Books/Berkeley: Berkeley, CA, USA, 2008. [Google Scholar]
- Voukelatos, A.; Cumming, R.G.; Lord, S.R.; Rissel, C. A randomized, controlled trial of tai chi for the prevention of falls: The Central Sydney tai chi trial. J. Am. Geriatr. Soc. 2007, 55, 1185–1191. [Google Scholar] [CrossRef]
- Wayne, P.M.; Hausdorff, J.M.; Lough, M.; Gow, B.J.; Lipsitz, L.; Novak, V.; Manor, B. Tai Chi Training may Reduce Dual Task Gait Variability, a Potential Mediator of Fall Risk, in Healthy Older Adults: Cross-Sectional and Randomized Trial Studies. Front. Hum. Neurosci. 2015, 9, 332. [Google Scholar] [CrossRef]
- Guo, L.Y.; Yang, C.P.; You, Y.L.; Chen, S.K.; Yang, C.H.; Hou, Y.Y.; Wu, W.L. Underlying mechanisms of Tai-Chi-Chuan training for improving balance ability in the elders. Chin. J. Integr. Med. 2014, 20, 409–415. [Google Scholar] [CrossRef]
- Wayne, P.M. The Harvard Medical School Guide to Tai Chi; Shambhala Publishers: Boulder, CO, USA, 2013; ISBN 9781590309421. [Google Scholar]
- Kerr, C. Translating “mind-in-body”: Two models of patient experience underlying a randomized controlled trial of qigong. Cult. Med. Psychiatry 2002, 26, 419–447. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Concept | ‘Plucking the Stars’ | ‘Lotus Leaves Rustle in the Wind’ | ‘Pacing Forwards and Backwards’ |
|---|---|---|---|
| Meditative Aspect | |||
| Relaxation response | Intent on exhale | Intent on exhale | Intent on exhale |
| Interoception and exteroception | Heightened awareness of internal and external sensations | Heightened awareness of internal and external sensations | Heightened awareness of internal and external sensations |
| Energetic Aspect Analysis | |||
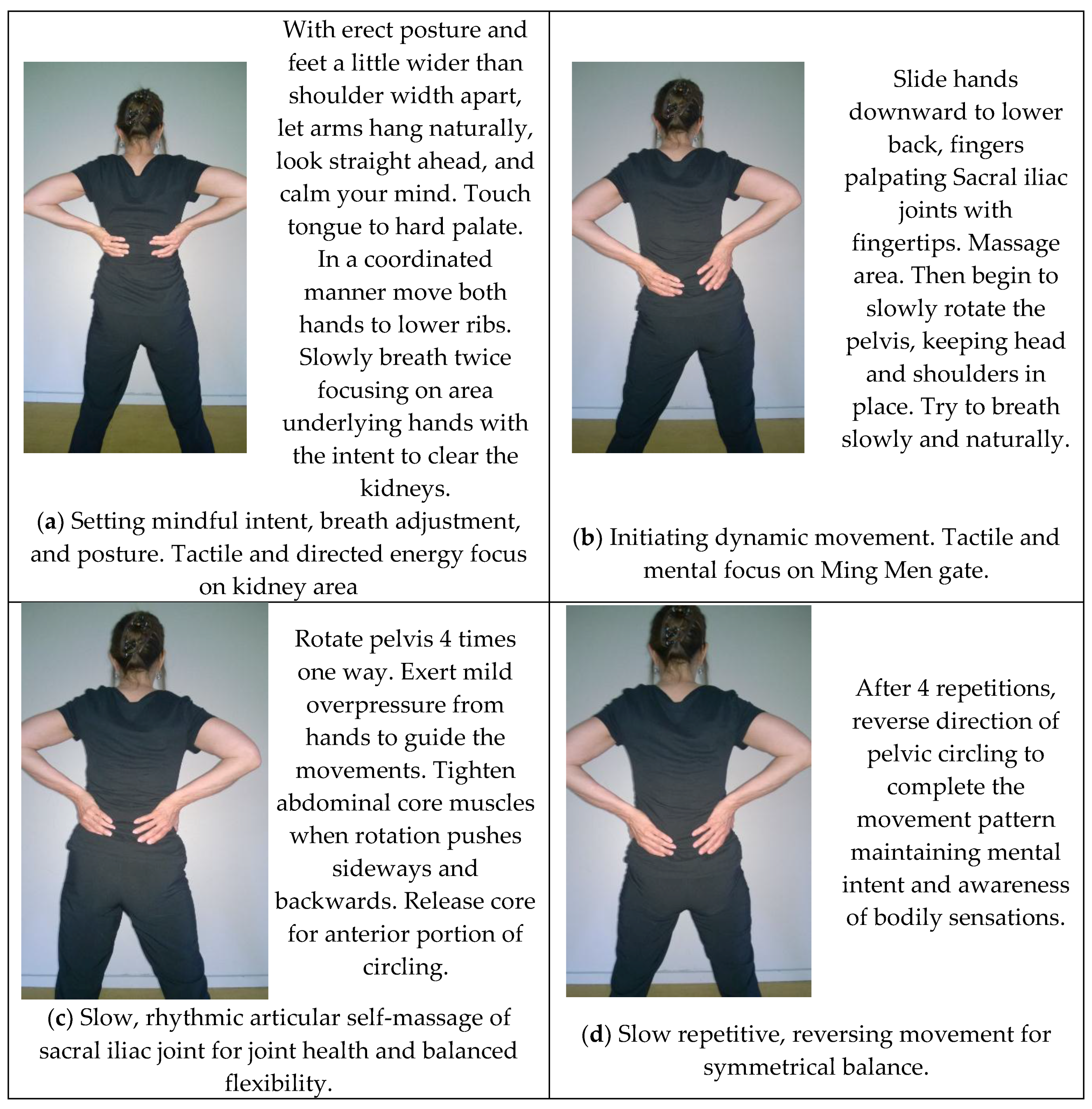
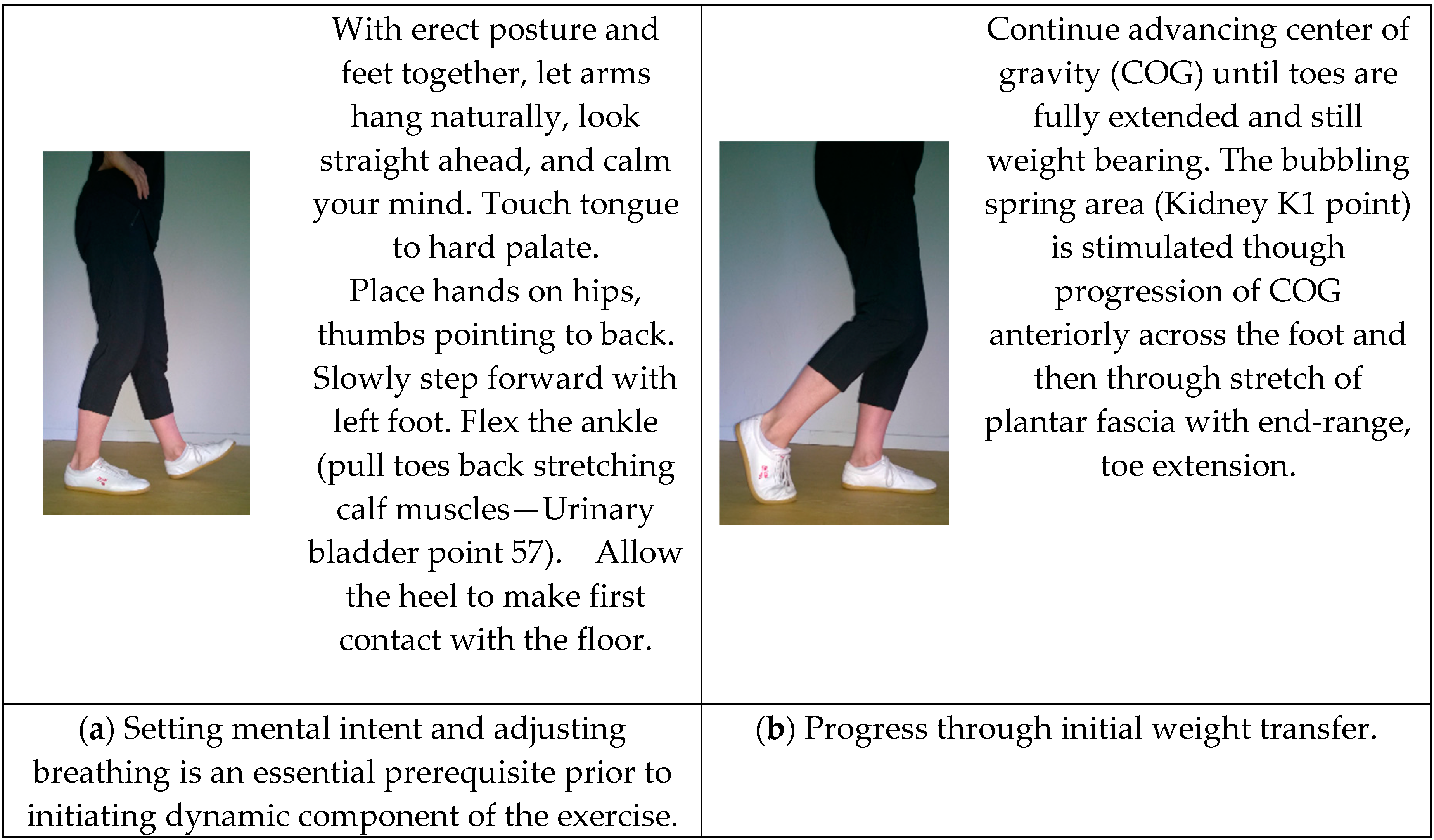
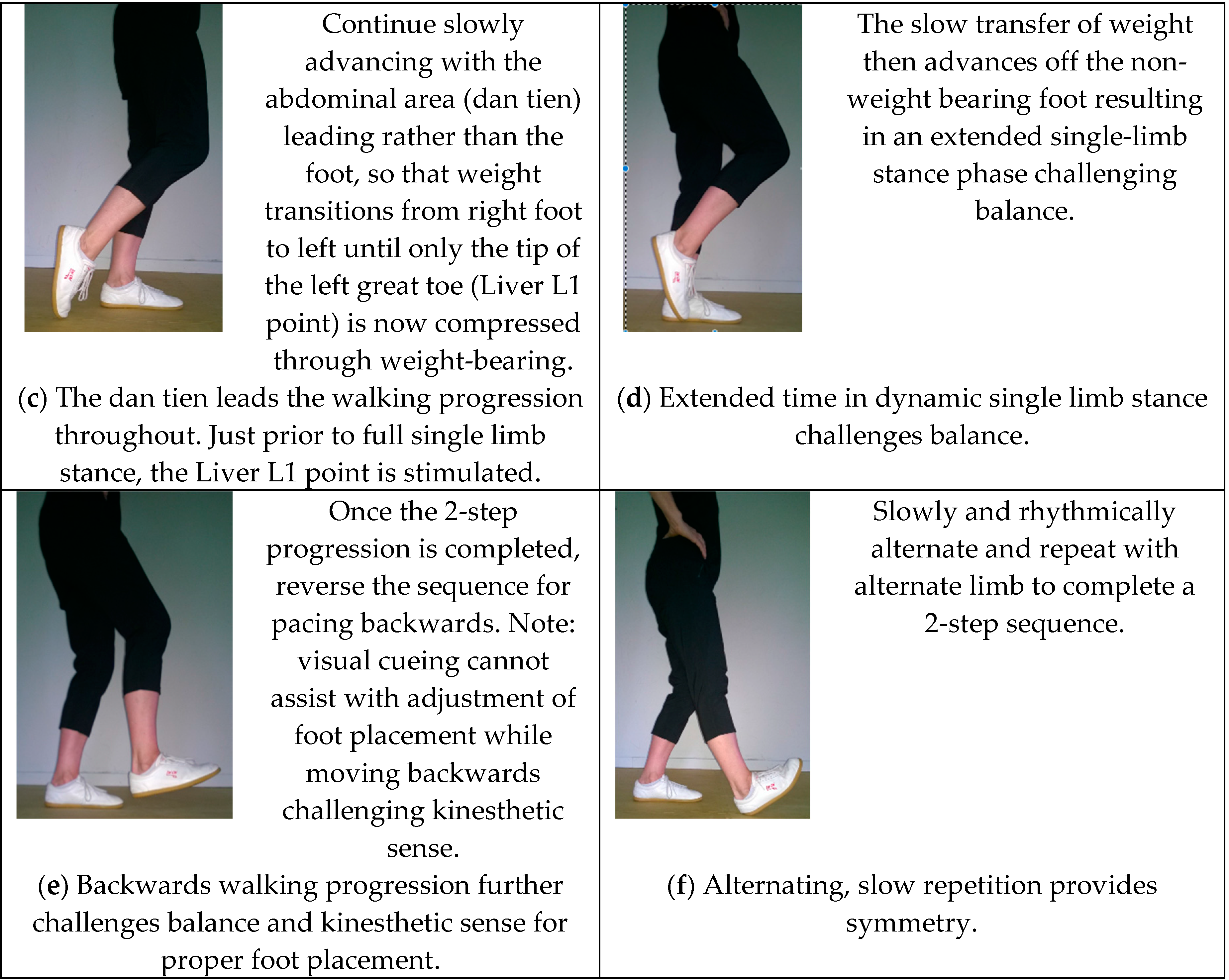
| Cultivating energy flow by stimulation of acupuncture points through muscle contracting, stretching and fascial compressing of soft tissue and organs. (In addition to general stimulation of all meridians) | Upper extremity and cervical and upper thoracic spine, internal organ meridians. | Internal visceral points: Urinary bladder UB57—mid calf, and additional points along the abdominal core, and gluteal areas. | Lower extremity including Urinary bladder UB57—mid calf when flexing the ankle; and additional points along in the lateral thigh and kidney and liver points within the foot |
| Mental Intent | Intent leads Qi: Eyes follow hand throughout the movement (Yi dao, Qi dao). through the Conception and Governing vessels and the biofield. | Clearing the kidneys and mobility of pelvic system. Opening of the Ming Men gate. | Intent to lead movement progression with the Dan Tien (located at center of body mass) rather than the foot or leg. |
| Self-massage | Biofield stroking | Hand placement over kidney area. | -- |
| Physical Analysis | |||
| Flexibility | Maintenance of gleno-humeral rhythm and shoulder range; Cervical rotation | Lower thoracic, costovertebral joints; sacroiliac joints. | Great toe extension; ankle; plantar fascia, heel cords. |
| Strength | Scapular stablizers; Shoulder movers. | Lateral costals; Spinal stablizers and core muscles. | Lower limb muscles involved in ankle righting, quadriceps, hip movers and stablizers, trunk core, |
| Articular stimulation | Shoulder capsule; cervical rotation. | Pelvic Sacroiliac joint; L3/4, L4/5, L5/S1; acetabulum rotates around the head of the femur | Foot joint mobility; gentle loading and unloading of all weight bearing joints. |
| Neuro-integration | Complex synergistic movement pattern. | Isolated body segment (pelvic rotation) movement pattern. | Complex, whole task synergistic movement pattern. |
| Cognitive effect | New learning; meditative mind/body practice; adjustment of the mind. | New learning; meditative mind/body practice; adjustment of the mind. | New learning; meditative mind/body practice; adjustment of the mind. |
| Respiratory effect | Improved PO2; decreased CO2. | Improved PO2; decreased CO2. | Improved PO2; decreased CO2. |
| Fascial stretch | Full body fascial stretch | Mild reciprocating stimulation of fascia supporting viscera. | Lower leg fascial stretch; plantar fascia stretch. |
| Visceral massage | Fascial stretch | Pelvic rotation | Pelvic rotation |
| Balance challenge | Rising on toes—foot/lower leg strength and anterior/posterior balance challenge; vestibular challenge in turning of the head; visual cueing. | Controlled anterior/posterior and lateral weight-shift. | Extended time in single limb stance; ankle righting challenge; foot placement challenge; foot as a mobile adaptor and stablizer. |
| CranioSacral pump | Rhythmic softening of the knees coordinated with pelvic tilting and breathing. | Rhythmic softening of the knees coordinated with pelvic tilting and breathing. | Rhythmic softening of the knees coordinated with pelvic tilting and breathing. |
| Lymphatic, venous return, glandular stimulation | Salivary gland stimulation; upper chest and axillary lymphatics; upper arm venous return. | Abdominal and Pelvic lymphatics | Abdominal core engagement for pelvic lymphatic return; calf muscle pump for lower leg venous return. |
| Physiologic response re: Relaxation effect (mind/body connection) | Vagal response; Changes in EEG; mental calm; sense of well-being. | Vagal response; Changes in EEG; mental calm; sense of well being. | Vagal response; Changes in EEG; mental calm; sense of well-being. |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klein, P.; Picard, G.; Baumgarden, J.; Schneider, R. Meditative Movement, Energetic, and Physical Analyses of Three Qigong Exercises: Unification of Eastern and Western Mechanistic Exercise Theory. Medicines 2017, 4, 69. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines4040069
Klein P, Picard G, Baumgarden J, Schneider R. Meditative Movement, Energetic, and Physical Analyses of Three Qigong Exercises: Unification of Eastern and Western Mechanistic Exercise Theory. Medicines. 2017; 4(4):69. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines4040069
Chicago/Turabian StyleKlein, Penelope, George Picard, Joseph Baumgarden, and Roger Schneider. 2017. "Meditative Movement, Energetic, and Physical Analyses of Three Qigong Exercises: Unification of Eastern and Western Mechanistic Exercise Theory" Medicines 4, no. 4: 69. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines4040069