Diagnostic Workup and Evaluation of Patients with Prurigo Nodularis
by
 , ,
, ,
Christina D. Kwon
1,* ,
,
Raveena Khanna
1,
Kyle A. Williams
1,
Madan M. Kwatra
2 and
Shawn G. Kwatra
1 1
Department of Dermatology, Johns Hopkins University School of Medicine, Baltimore, MD 21231, USA
2
Department of Anesthesiology, Duke University School of Medicine, Durham, NC 27710, USA
*
Author to whom correspondence should be addressed.
Medicines 2019, 6(4), 97; https://0-doi-org.brum.beds.ac.uk/10.3390/medicines6040097
Submission received: 1 August 2019
/
Revised: 18 September 2019
/
Accepted: 23 September 2019
/
Published: 26 September 2019
(This article belongs to the Special Issue Pathogenesis and Treatment of Chronic Pruritus)
{kind=link}
{kind=link}
Abstract
:Prurigo nodularis (PN) is a chronic inflammatory skin disease characterized oftentimes by symmetrically distributed, severely pruritic nodules. Currently, the pathophysiology of PN remains to be fully elucidated, but emerging evidence suggests that neuroimmune alterations play principal roles in the pathogenesis of PN. There are several associated etiologic factors thought to be associated with PN, including dermatoses, systemic, infectious, psychiatric, and neurologic conditions. We conducted a systematic literature review to evaluate the clinical presentation, diagnosis, and etiologic factors of PN. In this review, we discuss common differential diagnoses of PN and recommend an evidence-based, standardized diagnostic evaluation for those with suspected PN.
1. Introduction
Prurigo nodularis (PN) is a chronic inflammatory skin disease characterized oftentimes by symmetrically distributed, severely pruritic nodules. Currently, the pathophysiology of PN remains to be fully elucidated, but emerging evidence suggests that neuroimmune alterations play principal roles in the pathogenesis of PN. PN is also associated with several disease comorbidities such as chronic renal failure, liver disease, HIV, and malignancy [1,2,3,4]. However, there are currently no FDA approved therapies for PN, and patients are often times recalcitrant to off-label therapies. The goal of the present study is to perform a systematic review in the literature to provide evidence for specific testing and diagnostic evaluation of PN patients.
2. Methods
Using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we searched the PubMed, MEDLINE and Embase databases for “prurigo nodularis” or “prurigo.” All articles, including case reports and series describing prurigo nodularis were included. English language articles were included before April 8, 2019. We limited the search to articles involving human subjects. All of the results were checked for relevance and suitability. No manufacturers or authors mentioned in these reports were contacted.
3. Results
Our search yielded a total of 791 records with redundancy from 1947 to 2019 containing the aforementioned key words. After removing duplicates, 342 unique records remained. Ultimately, 35 primary sources were included. We included case series and reports. In these sources, the clinical presentation, potential pathophysiology, histological characteristics and etiologic factors of PN were discussed.
4. Diagnosis
4.1. History and Physical
PN is a clinical diagnosis that is based upon information gathered from a thorough history and physical examination. In regard to history, patients will complain of severe itch that can be continuous, paroxysmal or sporadic. In addition to pruritus, patients may also describe the sensations as a burning or stinging [5].
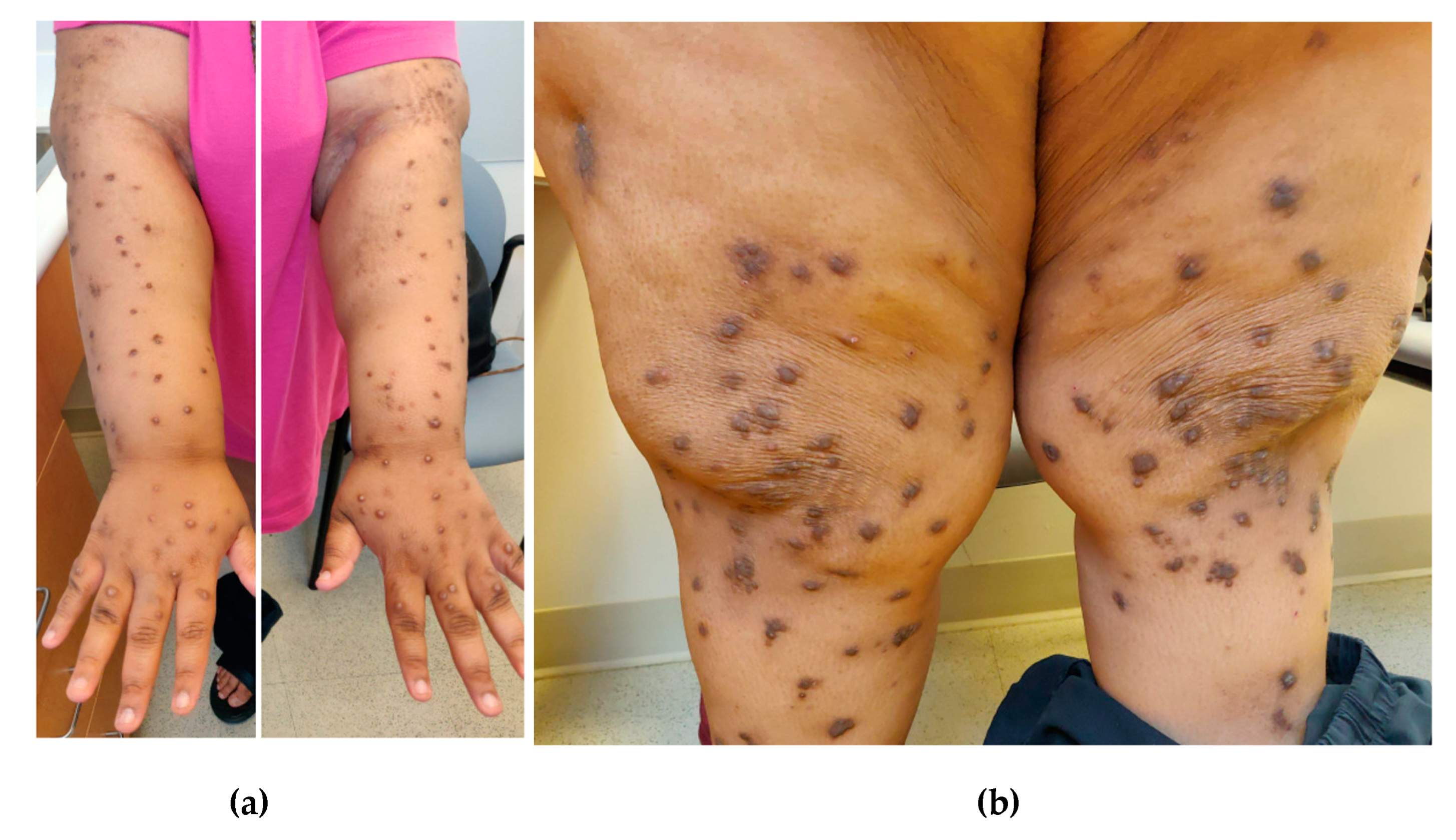
PN characteristically presents with excoriated, hyperkeratotic, and pruritic dome-shaped nodules, papules, or plaques that are often bilaterally distributed on the extensor surfaces of the extremities (Figure 1) [6]. In addition to affecting extremities, PN can also involve parts of the trunk that are accessible to scratching such as the upper back and abdomen. Patients with back involvement often present with the “butterfly” sign as they are unable to reach the central back and this area is spared, leaving a characteristic butterfly pattern [7]. The lesions can be variable in both quantity and quality. Cases range from patients having only a few lesions to several hundreds. The lesions also vary in size, from millimeters to centimeters, and color, ranging from flesh-colored to pink to brown or black.
4.2. Differential Diagnoses
There are several skin diseases that can mimic PN. We discuss several rare conditions that have been reported in the literature as being masqueraders of PN. Often, these diagnoses are only elucidated after the patient is refractory to treatment and worked-up further.
4.2.1. Pemphigoid Nodularis
Pemphigoid nodularis is a rare variant of bullous pemphigoid that has features of both prurigo nodularis and bullous pemphigoid. Compared to PN, pemphigoid nodularis is often characterized by larger plaques often with large areas of central erosion, ulceration, and/or blistering [8,9]. On biopsy, there is also evidence of subepidermal clefting and direct immunofluorescence (DIF) displays linear deposition of IgG and C3 at the basement membrane zone. Furthermore, patients will have circulating antibasement membrane zone autoantibodies [10,11,12].
4.2.2. Actinic Prurigo
Actinic prurigo is a rare type of photodermatosis presenting with acute eruptions of severely pruritic papules or nodules often accompanied by cheilitis and conjunctivitis. This condition is more common in young girls and they present with extreme photosensitivity to UVA and UVB [13].
4.2.3. Epidermolysis Bullosa
4.2.4. Hypertrophic Lichen Planus
Hypertrophic lichen planus (HLP) can also resemble PN clinically, presenting as hyperkeratotic plaques and nodules most commonly involving the shin and ankles. Histopathology can also be very similar with both demonstrating epidermal hyperplasia, hypergranulosis, compact hyperkeratosis, increased number of fibroblasts and capillaries. However, basal cell degeneration is confined to the tips of the rete ridges and band-like infiltration is often absent in HLP compared to PN [16].
4.2.5. Neurotic Excoriations
Neurotic excoriations, also known as dermatotillomania, can also lead to excoriations that can have slightly raised areas that resemble lesions seen in PN. Neurotic excoriations, however, is a psychiatric condition characterized by excessive picking of the skin.
5. Etiologic Factors and Associated Diseases
5.1. Dermatoses
Some studies have pointed to dermatological conditions as the predominant etiology of PN, up to 82% [5,19]. PN has been associated with a variety of dermatological conditions, most notably atopic dermatitis (up to 46%) [5,19,20,21,22]. Other dermatological conditions that have been associated with PN are cutaneous T-cell lymphoma, lichen planus, xerosis cutis, keratoacanthomas, and bullous pemphigoid [5,23,24]. One study found that 60% of its cohort of patients with PN (n = 80) had xerosis. In these patients with xerosis, there were higher rates of co-morbidities including diabetes and psychiatric causes, which is discussed below [21].
5.2. Systemic
Systemic and metabolic causes have been implicated in 38% to up to 50% of PN cases [25,26]. Some common systemic associations of PN are chronic renal failure, liver disease (chronic hepatitis B, primary biliary cholangitis, chronic autoimmune cholestatic hepatitis), HIV, thyroid disease, diabetes and malignances, specifically non-Hodgkin’s lymphoma [3,4,27,28,29,30,31,32,33,34,35,36]. A study (n = 16,925) by Larson et al. found that pruritus was most strongly associated with cancers of the liver, skin, and hematopoietic system [37]. Rarer malignancies that have been associated with PN are metastatic transitional cell carcinoma of the bladder and Hodgkin’s lymphoma [30,38,39]. Other less commonly associated systemic causes are gout, iron-deficiency anemia, and celiac disease [26,32,40,41].
5.3. Infectious
A number of infectious causes have been implicated in PN [42]. Some infectious or parasitic causes that have been reported are Mycobacterium tuberculosis and mucogenicum, Ascaris lumbricoides, Helicobacter pylori, Strongyloides stercoralis, and herpes zoster [42,43,44,45,46,47,48,49,50]. In some cases, it has been found that treatment and resolution of the infection have resolved the PN and pruritic symptoms. Although the aforementioned studies and reports have linked infectious agents with PN, there is still a lack of strong evidence for a direct causal association [42].
5.4. Medications
Medications have been reported as a cause of PN. There have been reports implicating mainly cancer therapy agents in cutaneous side effects [48,49]. In a study by Biswal et al., 384 out of 1000 patients undergoing chemotherapy developed cutaneous adversities. Of the 384, 0.8% (n = 3) developed prurigo nodularis [51]. Specifically, pembrolizumab, paclitaxel, and carboplatin have been associated with the development of PN [51,52]. With these therapy agents it is thought that the persistent activation of the immune system contributes to the pathogenesis of PN. For example, pembrolizumab is an antibody that works as an immune checkpoint inhibitor by blocking programmed death 1 protein.
5.5. Psychiatric
PN has been significantly associated with depression, anxiety, and dissociative experiences, all of which can cause psychogenic pruritus [1,53,54,55,56,57,58]. This psychogenic pruritus is then thought to lead to PN. However, psychogenic pruritus must be distinguished from neurotic excoriations (also known as dermatotillomania), which is characterized by excessive scratching or picking of the skin, leading to skin lesions. Of note, dermatotillomania is categorized as an impulse disorder and is frequently associated with other primary psychiatric impulse disorders [59].
5.6. Neurologic
Neuropathic itch is a pathological condition due to some neuronal or glial damage. It has many causes including local nerve fiber compression or degeneration. Although it is more common to involve the peripheral nervous system (PNS), neuropathic itch can also stem from damage within the central nervous system (CNS) [60]. Proximal PNS etiologies are polyneuropathies, post-herpetic neuralgia, brachioradial pruritus, notalgia paraesthetica, and other entrapment neuropathies [61]. Distal PNS etiologies include small-fiber neuropathies, sensitive skin, or post-burn itch [61].
6. Evaluation
6.1. Biopsy
Although PN is a clinical diagnosis, biopsies are often warranted for lesions that do not respond to first line therapies or those with secondary complications such as bleeding or ulceration. Weigelt et al. found that PN (n = 136) had characteristic features such as presence of thick orthohyperkeratotis, the hairy palm sign (folliculosebaceous units seen with a thick and compact cornified layer), irregular epidermal hyperplasia, hypergranulosis, fibrosis of the papillary dermis and increased fibroblasts and capillaries. However, these histologic characteristics often coincide with other scratch-induced conditions, such as lichen simplex. Thus, correlation of clinical and histological findings is still required to distinguish PN from other scratched-induced conditions [62].
Immunohistochemical studies have shown reduced intraepidermal nerve fiber density in lesional and nonlesional skin in patients with prurigo nodularis [63]. This observed hypoplasia has been suggested to indicate subclinical small fiber neuropathy PN [63]. However, recent studies have shown that there is no functional small fiber-neuropathy and the altered epidermal neuroanatomy is thought to be a consequence of chronic scratching [64]. As a result, we do not currently recommend routine intraepidermal nerve fiber density (IENFD) testing in patients unless underlying small fiber neuropathy is suspected. Direct immunofluorescence (DIF) is helpful for distinguishing PN from autoimmune diseases, such as bullous pemphigoid, pemphigoid nodularis, and epidermolysis bullosa, which may present similarly, or even concomitantly, with PN [23].
6.2. Laboratory Evaluation
As previously mentioned, PN can often have an associated systemic etiology. A thorough laboratory work-up should be pursued, especially for patients without a history of underlying dermatoses, such as PN arising secondary to atopic dermatitis. Systemic causes of chronic pruritus should be particularly evaluated for common systemic etiologies, such as chronic renal failure, liver disease, HIV, and thyroid disease. Infrequently, PN has presented in the context of gout, iron-deficiency anemia, celiac disease, non-Hodgkin’s lymphoma or infection.
Strongly suggested workup includes a complete blood cell count (CBC), complete metabolic panel (CMP), thyroid, liver and kidney function tests, HIV serology, and hepatitis B and C serologies (Figure 2). Optional workup based on clinical judgement and the patient’s clinical examination includes biopsy with a hematoxylin and eosin stain, direct immunofluorescence, chest radiograph, serum and urine protein electrophoresis, urinalysis, stool exam for ova and parasites, and iron studies.
6.3. Pruritic Intensity and Quality of Life
In addition to the above, evaluation should also take pruritic symptoms and quality of life into consideration given the severe pruritus that PN patients often experiences [65]. There is a wide range of different scales that have been used to assess pruritic symptoms. In terms of pruritic intensity, there are monodimensional tools that have shown high reliability and concurrent validity, such as the Visual Analogue Scale (VAS), Itch Numerical Rating Scale (Itch NRS), Worst Itch Numeric Rating Scale (WI-NRS), and Verbal Rating Scale (VRS) [65,66]. The VAS uses a 10 cm scale with endpoints marked with “0” and “10” to correlate with “no itch” and “worst imaginable itch,” respectively [65]. With the NRS, patients are asked to rate their itch intensity from 0 for “no itch” to 10 for “worst imaginable itch.” Lastly, the VRS asks patients to describe their itch symptom intensity with a list of adjectives such as “0 = no itch” and “1 = mild itch” [67].
There are also multidimensional scales to assess pruritus intensity. These include the Itch Severity Scale (ISS) and the Pruritus Grading System (PGS). These multidimensional scales encompass questions around the time of day pruritic symptoms occur, the quality, intensity and location of itch, and effects on sexual symptom and sleep [68].
In terms of assessing scratch activity and lesions, there are tools available such as the Scratch Symptom Score (SSS), Prurigo Activity Score (PAS), wrist actigraphy, and accelerometers. The SSS measures individual scratch lesions standardized against the body surface [65]. The PAS is a seven-item questionnaire designed to monitor the distribution and activity of chronic prurigo lesions [69]. Although wrist actigraphy and accelerometers may prove useful in assessing activity, they have yet to be validated and may not be easily conducted in a clinic setting [65,70].
In addition to the above scales and questionnaires that often capture a patient’s itch symptoms at one point in time, there are also several tools available to monitor the course of pruritus. These include: the Dynamic Pruritus Score, Itch-Free Days, 5-D Itch Scale, Patient Benefit Index, and ItchApp [65]. These various tools encompass the course of itch intensity and location, patient satisfaction with treatment, changing symptoms and disability over different points in time.
As previously mentioned, there are high rates of psychiatric comorbidities associated with PN. Some tools used to assess depression and anxiety include: the Beck Depression Inventory, Hospital Anxiety and Depression Scale, and Hamilton Rating Scale for Depression [71,72,73,74]. In addition to assessing for psychiatric comorbidities, chronic pruritus also negatively impairs sleep as well as quality of life (QOL). Tools to measure sleep impairment include the Athens Insomnia Scale, Stanford Sleepiness Scale, Pittsburgh Sleep Quality Index, and Epworth Sleepiness Scale [75,76,77,78].
Tools to assess quality of life commonly include the ItchyQoL, 36-item short form (SF-36) and Dermatological Life Quality Index (DLQI) [79,80,81]. The ItchyQoL questionnaire is specific to pruritic symptoms effects on the quality of life and is comprised of 22 items. Its questions cover symptoms, function, patients’ emotions and self-perception in regard to their pruritus. The SF-36 focuses on similar aspects such as limitations and emotional impairment but is also used for conditions other than chronic pruritus [81]. Lastly, the DLQI is a validated questionnaire asking about the impact of a patient’s dermatological disease and its treatment on the quality of life [80].
7. Discussion
Prurigo nodularis is an orphan disease with no standardized diagnostic or treatment regimen and has been understudied compared to other inflammatory skin diseases. Given the highly pruritic and chronic nature of this disease, there is a very high burden of disease, including high rates of associated anxiety and depression among PN patients [82]. These quality of life issues are compounded by the poor management of patients and lack of effective therapies. Greater attention is needed to formulate standardized diagnostic algorithms in the evaluation of PN patients. In particular, from our systematic review, we would like to highlight the need for a targeted clinical examination and laboratory evaluation to exclude other diagnoses and associated etiologic factors.
More randomized controlled studies with large patient cohorts are needed for uncovering more targeted treatments. As several agents are in the pipeline, greater recognition of PN and an evidence-based diagnostic workup is necessary for optimal patient management.
8. Conclusions
PN is a chronic inflammatory skin disease that often has an immense psychosocial impact on patients’ quality of life. Due to its varying clinical presentations and several mimickers, we propose a diagnostic workup for those with clinically-suspected PN. More consistent diagnoses of PN could improve future studies on PN and help discover more effective therapies for patients.
Author Contributions
The following contributions were made by the authors: conceptualization: C.D.K., R.K., K.A.W., M.M.K., and S.G.K.; methodology: C.D.K., R.K., K.A.W., M.M.K., and S.G.K.; writing—original draft preparation: C.D.K.; writing—review and editing: C.D.K. and S.G.K.; visualization: C.D.K. and S.G.K.; supervision: S.G.K.
Funding
This research received no external funding.
Conflicts of Interest
Shawn G. Kwatra is an advisory board member for Menlo and Trevi Therapeutics and has received grant funding from Kiniksa Pharmaceuticals. He is also the recipient of a Dermatology Foundation Medical Dermatology Career Development Award.
References
- Boozalis, E.; Tang, O.; Patel, S.; Semenov, Y.R.; Pereira, M.P.; Ständer, S.; Kang, S.; Kwatra, S.G. Ethnic differences and comorbidities of 909 prurigo nodularis patients. J. Am. Acad. Dermatol. 2018, 79, 714–719.e3. [Google Scholar] [CrossRef] [PubMed]
- Larson, V.A.; Tang, O.; Stander, S.; Miller, L.S.; Kang, S.; Kwatra, S.G. Association between prurigo nodularis and malignancy in middle-aged adults. J. Am. Acad. Dermatol. 2019. [Google Scholar] [CrossRef]
- Whang, K.A.; Kang, S.; Kwatra, S.G. Inpatient Burden of Prurigo Nodularis in the United States. Medicines 2019, 6, 88. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.H.; Canner, J.K.; Khanna, R.; Kang, S.; Kwatra, S.G. Real-world prevalence of prurigo nodularis and burden of associated diseases. J. Investig. Dermatol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Iking, A.; Grundmann, S.; Chatzigeorgakidis, E.; Phan, N.Q.; Klein, D.; Ständer, S. Prurigo as a symptom of atopic and non-atopic diseases: Aetiological survey in a consecutive cohort of 108 patients. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Zeidler, C.; Yosipovitch, G.; Ständer, S. Prurigo Nodularis and Its Management. Dermatol. Clin. 2018, 36, 189–197. [Google Scholar] [CrossRef]
- Schedel, F.; Schürmann, C.; Metze, D.; Ständer, S. [Prurigo. Clinical definition and classification]. Hautarzt 2014, 65, 684–690. [Google Scholar] [CrossRef]
- Al-Salhi, W.; Alharithy, R. Pemphigoid nodularis. J. Cutan. Med. Surg. 2015, 19, 153–155. [Google Scholar] [CrossRef]
- Kwong, H.L.; Lim, S.P. Pemphigoid nodularis mimicking nodular prurigo in an immune-suppressed patient with rheumatoid arthritis. Acta Derm. Venereol. 2015, 95, 237–238. [Google Scholar] [CrossRef]
- Ray, J.; Michael, C. Pemphigoid nodularis: Two new cases demonstrating distinguishing clinical clues from prurigo nodularis. J. Am. Acad. Dermatol. 2009, 60, AB103–AB104. [Google Scholar]
- Ross, J.S.; McKee, P.H.; Smith, N.P.; Shimizu, H.; Griffiths, W.A.D.; Bhogal, B.S.; Black, M.M. Unusual variants of pemphigoid: From pruritus to pemphigoid nodularis. J. Cutan. Pathol. 1992, 19, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Powell, A.M.; Albert, S.; Gratian, M.J.; Bittencourt, R.; Bhogal, B.S.; Black, M.M. Pemphigoid nodularis (non-bullous): A clinicopathological study of five cases. Br. J. Dermatol. 2002, 147, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.; Fischer, A. Actinic prurigo. J. Am. Acad. Dermatol. 2016, 74, AB224. [Google Scholar]
- Pustover, K.; Fivenson, D. Epidermolysis bullosa acquisita: A unique clinical presentation with Blaschkoid acral distribution. J. Am. Acad. Dermatol. 2017, 76, AB124. [Google Scholar]
- Pai, V.; Naveen, K.; Athanikar, S.; Rai, V.; Shastry, D. Epidermolysis bullosa pruriginosa: A report of two cases. Indian Dermatol. Online J. 2014, 5, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Ankad, B.S.; Beergouder, S.L. Hypertrophic lichen planus versus prurigo nodularis: A dermoscopic perspective. Dermatol. Pract. Concept. 2016, 6, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Werbel, T.; Hinds, B.R.; Cohen, P.R. Scabies presenting as cutaneous nodules or malar erythema: Reports of patients with scabies surrepticius masquerading as prurigo nodularis or systemic lupus erythematosus. Dermatol. Online J. 2018. [Google Scholar]
- Wick, M.R. Psoriasiform dermatitides: A brief review. Semin. Diagn. Pathol. 2017, 34, 220–225. [Google Scholar] [CrossRef]
- Tan, W.S.; Tey, H.L. Extensive prurigo nodularis: Characterization and etiology. Dermatology 2014, 228, 276–280. [Google Scholar] [CrossRef]
- Lee, S.; Wang, H.Y.; Kim, E.; Hwang, H.J.; Choi, E.; Lee, H.; Choi, E.H. Clinical characteristics and genetic variation in atopic dermatitis patients with and without allergic contact dermatitis. Eur. J. Dermatol. 2018, 28, 637–643. [Google Scholar]
- Akarsu, S.; Ozbagcivan, O.; Ilknur, T.; Semiz, F.; Inci, B.B.; Fetil, E. Xerosis cutis and associated co-factors in women with prurigo nodularis. An. Bras. Dermatol. 2018, 93, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Miyachi, Y.; Okamoto, H.; Furukawa, F.; Imamura, S. Prurigo nodularis. A possible relationship to atopy. J. Dermatol. 1980, 7, 281–283. [Google Scholar] [CrossRef] [PubMed]
- Roenigk, R.K.; Dahl, M.V. Bullous pemphigoid and prurigo nodularis. J. Am. Acad. Dermatol. 1986, 14 Pt 2, 944–947. [Google Scholar] [CrossRef]
- Wu, T.P.; Miller, K.; Cohen, D.E.; Stein, J.A. Keratoacanthomas arising in association with prurigo nodules in pruritic, actinically damaged skin. J. Am. Acad. Dermatol. 2013, 69, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Rowland Payne, C.M.; Wilkinson, J.D.; McKee, P.H.; Jurecka, W.; Black, M.M. Nodular prurigo—A clinicopathological study of 46 patients. Br. J. Dermatol. 1985, 113, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Winhoven, S.; Gawkrodger, D. Nodular prurigo: Metabolic diseases are a common association. Clin. Exp. Dermatol. 2006, 32, 224–225. [Google Scholar] [CrossRef] [PubMed]
- Matthews, S.N.; Cockerell, C.J. Prurigo nodularis in HIV-infected individuals. Int. J. Dermatol. 1998, 37, 401–409. [Google Scholar] [CrossRef]
- Rien, B.E.; Lemont, H.; Cohen, R.S. Prurigo nodularis: As association with uremia. J. Am. Podiatry Assoc. 1982, 72, 321–323. [Google Scholar] [CrossRef]
- Rishi, R.; Ringwala, S.; Tracy, J.; Fatteh, S. Prurigo nodularis and Hashimoto thyroiditis. Ann. Allergy Asthma Immunol. 2014, 113, 673–674. [Google Scholar] [CrossRef]
- Dumont, S.; Péchère, M.; Toutous Trellu, L. Chronic Prurigo: An Unusual Presentation of Hodgkin Lymphoma. Case Rep. Dermatol. 2018, 10, 122–126. [Google Scholar] [CrossRef]
- Seshadri, P.; Rajan, S.J.; George, I.A.; George, R. A sinister itch: Prurigo nodularis in Hodgkin lymphoma. J. Assoc. Physicians India 2009, 57, 715–716. [Google Scholar] [PubMed]
- Parcheta, P.; Stepien, P.; Zarebska-Michaluk, D.; Krecisz, B. Nodular prurigo as first manifestation of primary biliary cholangitis successfully treated with rifampin and sertraline. Acta Derm. Venereol. 2017, 97, 1056. [Google Scholar]
- Savoia, F.; Casadio, C.; Tabanelli, M.; Spadola, G.; Zago, S.; Maio, V.; Giacomoni, P.; Gaddoni, G.; Patrizi, A.; Lanzanova, G. Prurigo nodularis as the first manifestation of a chronic autoimmune cholestatic hepatitis. Int. J. Dermatol. 2011, 50, 1588–1589. [Google Scholar] [CrossRef] [PubMed]
- Neri, S.; Raciti, C.; D’Angelo, G.; Ierna, D.; Bruno, C.M. Hyde’s prurigo nodularis and chronic HCV hepatitis. J. Hepatol. 1998, 28, 161–164. [Google Scholar] [CrossRef]
- Böhme, T.; Heitkemper, T.; Mettang, T.; Phan, N.Q.; Ständer, S. [Clinical features and prurigo nodularis in nephrogenic pruritus]. Hautarzt 2014, 65, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Kremer, A.E.; Wolf, K.; Ständer, S. [Intrahepatic cholestasis of pregnancy: Rare but important]. Hautarzt 2017, 68, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Larson, V.A.; Tang, O.; Ständer, S.; Kang, S.; Kwatra, S.G. Association between itch and cancer in 16,925 patients with pruritus: Experience at a tertiary care center. J. Am. Acad. Dermatol. 2019, 80, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.T.; Wang, W.H.; Yen, C.C.; Yu, I.T.; Chen, P.M. Prurigo nodularis as initial presentation of metastatic transitional cell carcinoma of the bladder. J. Urol. 2002, 168, 631–632. [Google Scholar] [CrossRef]
- Fina, L.; Grimalt, R.; Berti, E.; Caputo, R. Nodular prurigo associated with Hodgkin’s disease. Dermatologica 1991, 182, 243–246. [Google Scholar] [CrossRef]
- Stefanini, G.F.; Resta, F.; Marsigli, L.; Gaddoni, G.; Baldassarri, L.; Caprio, G.P.; Degli Azzi, I.; Foschi, F.G.; Gasbarrini, G. Prurigo nodularis (Hyde’s prurigo) disclosing celiac disease. Hepatogastroenterology 1999, 46, 2281–2284. [Google Scholar]
- McKenzie, A.W.; Stubbing, D.G.; Elvy, B.L. Prurigo nodularis and gluten enteropathy. Br. J. Dermatol. 1976, 95, 89–92. [Google Scholar] [PubMed]
- Saporito, L.; Florena, A.M.; Colomba, C.; Pampinella, D.; Di Carlo, P. Prurigo nodularis due to Mycobacterium tuberculosis. J. Med. Microbiol. 2009, 58 Pt 12, 1649–1651. [Google Scholar] [CrossRef]
- Gulin, S.J.; Čeović, R.; Lončarić, D.; Ilić, I.; Radman, I. Nodular prurigo associated with mycosis fungoides—Case report. Acta Dermatovenerol. Croat. 2015, 23, 203. [Google Scholar]
- Menni, S.; Boccardi, D.; Gualandri, L.; Cainarca, M. Prurigo nodularis in a young child with a parasitic infestation with Ascaris lumbricoides. Eur. J. Pediatr. Dermatol. 2009, 19, 31–34. [Google Scholar]
- Guarneri, C.; Lotti, J.; Fioranelli, M.; Roccia, M.G.; Lotti, T.; Guarneri, F. Possible role of Helicobacter pylori in diseases of dermatological interest. J. Biol. Regul. Homeost. Agents 2017, 31 (Suppl. 2), 57–77. [Google Scholar] [PubMed]
- Neri, S.; Ierna, D.; D’Amico, R.A.; Giarratano, G.; Leotta, C. Helicobacter pylori and prurigo nodularis. Hepatogastroenterology 1999, 46, 2269–2272. [Google Scholar] [PubMed]
- Jacob, C.I.; Patten, S.F. Strongyloides stercoralis infection presenting as generalized prurigo nodularis and lichen simplex chronicus. J. Am. Acad. Dermatol. 1999, 41 Pt 2, 357–361. [Google Scholar] [CrossRef]
- Mattila, J.O.; Katila, M.L.; Vornanen, M. Slowly growing mycobacteria and chronic skin disorders. Clin. Infect. Dis. 1996, 23, 1043–1048. [Google Scholar] [CrossRef]
- Wang, L.S.; Wu, T.S.; Wang, C.C.J.; Ku, C.L.; Hsu, Y.H.; Chang, P.Y. Mycobacterium mucogenicum infection presenting with generalized follicular hyperplasia and prurigo nodularis in an immunocompetent patient. Int. J. Antimicrob. Agents 2017, 50, S97–S98. [Google Scholar]
- De, D.; Dogra, S.; Kanwar, A.J. Prurigo nodularis in healed herpes zoster scar: An isotopic response. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 711–712. [Google Scholar] [CrossRef]
- Biswal, S.G.; Mehta, R.D. Cutaneous Adverse Reactions of Chemotherapy in Cancer Patients: A Clinicoepidemiological Study. Indian J. Dermatol. 2018, 63, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Fattore, D.; Panariello, L.; Annunziata, M.C.; Fabbrocini, G. Prurigo nodularis and pembrolizumab: A therapeutic challenge. Eur. J. Cancer 2019, 110, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Stefanini, G.F.; Resta, F.; Marsigli, L.; Gaddoni, G.; Baldassarri, L.; Caprio, G.P.; Degli Azzi, I.; Foschi, F.G.; Gasbarrini, G. Clinical classification of itch: A position paper of the International Forum for the Study of Itch. Acta Derm. Venereol. 2007, 87, 291–294. [Google Scholar]
- Lee, H.G.; Stull, C.; Yosipovitch, G. Psychiatric disorders and pruritus. Clin. Dermatol. 2017, 35, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Radmanesh, M.; Shafiei, S. Underlying psychopathologies of psychogenic pruritic disorders. Psychosom. Dermatol. Psychosom. 2001, 2, 130–133. [Google Scholar] [CrossRef]
- Dazzi, C.; Erma, D.; Piccinno, R.; Veraldi, S.; Caccialanza, M. Psychological factors involved in prurigo nodularis: A pilot study. J. Dermatol. Treat. 2011, 22, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Lotti, T.; Buggiani, G.; Prignano, F. Prurigo nodularis and lichen simplex chronicus. Dermatol. Ther. 2008, 21, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Brenaut, E.; Halvorsen, J.A.; Dalgard, F.J.; Lien, L.; Balieva, F.; Sampogna, F.; Linder, D.; Evers, A.W.; Jemec, G.B.; Gieler, U.; et al. The self-assessed psychological comorbidities of prurigo in European patients: A multicentre study in 13 countries. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 157–162. [Google Scholar] [CrossRef]
- Gieler, U.; Tomas-Aragones, L.; Linder, D.; Jemec, G.; Poot, F.; Szepietowski, J.; Korte, J.; Taube, K.; Lvov, A.; Consoli, S. Self-inflicted lesions in dermatology: Terminology and classification—A position paper from the European Society for Dermatology and Psychiatry (ESDaP). Acta Derm. Venereol. 2013, 93, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Hachisuka, J.; Chiang, M.C.; Ross, S.E. Itch and neuropathic itch. Pain 2018, 159, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Misery, L.; Brenaut, E.; Le Garrec, R.; Abasq, C.; Genestet, S.; Marcorelles, P.; Zagnoli, F. Neuropathic pruritus. Nat. Rev. Neurol. 2014, 10, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Weigelt, N.; Metze, D.; Ständer, S. Prurigo nodularis: Systematic analysis of 58 histological criteria in 136 patients. J. Cutan. Pathol. 2010, 37, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Schuhknecht, B.; Marziniak, M.; Wissel, A.; Phan, N.; Pappai, D.; Dangelmaier, J.; Metze, D.; Ständer, S. Reduced intraepidermal nerve fibre density in lesional and nonlesional prurigo nodularis skin as a potential sign of subclinical cutaneous neuropathy. Br. J. Dermatol. 2011, 165, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.P.; Pogatzki-Zahn, E.; Snels, C.; Vu, T.-H.; Üçeyler, N.; Loser, K.; Sommer, C.; Evers, A.W.M.; Van Laarhoven, A.I.M.; Agelopoulos, K.; et al. There is no functional small-fibre neuropathy in prurigo nodularis despite neuroanatomical alterations. Exp. Dermatol. 2017, 26, 969–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, M.P.; Ständer, S. Assessment of severity and burden of pruritus. Allergol. Int. 2017, 66, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Reich, A.; Heisig, M.; Phan, N.; Taneda, K.; Takamori, K.; Takeuchi, S.; Furue, M.; Blome, C.; Augustin, M.; Ständer, S.; et al. Visual analogue scale: Evaluation of the instrument for the assessment of pruritus. Acta Derm. Venereol. 2012, 92, 497–501. [Google Scholar] [CrossRef]
- Phan, N.; Blome, C.; Fritz, F.; Gerss, J.; Reich, A.; Ebata, T.; Augustin, M.; Szepietowski, J.; Ständer, S. Assessment of pruritus intensity: Prospective study on validity and reliability of the visual analogue scale, numerical rating scale and verbal rating scale in 471 patients with chronic pruritus. Acta Derm. Venereol. 2012, 92, 502–507. [Google Scholar] [CrossRef]
- Majeski, C.J.; Johnson, J.A.; Davison, S.N.; Lauzon, C.J. Itch Severity Scale: A self-report instrument for the measurement of pruritus severity. Br. J. Dermatol. 2007, 156, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Pölking, J.; Zeidler, C.; Schedel, F.; Osada, N.; Augustin, M.; Metze, D.; Pereira, M.P.; Yosipovitch, G.; Bernhard, J.D.; Ständer, S. Prurigo Activity Score (PAS): Validity and reliability of a new instrument to monitor chronic prurigo. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1754–1760. [Google Scholar] [CrossRef]
- Ständer, S.; Zeidler, C.; Riepe, C.; Steinke, S.; Fritz, F.; Bruland, P.; Soto-Rey, I.; Storck, M.; Agner, T.; Augustin, M.; et al. European EADV network on assessment of severity and burden of Pruritus (PruNet): First meeting on outcome tools. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1144–1147. [Google Scholar] [CrossRef]
- Herrmann, C. International experiences with the Hospital Anxiety and Depression Scale—A review of validation data and clinical results. J. Psychosom. Res. 1997, 42, 17–41. [Google Scholar] [CrossRef]
- Snaith, R.P. The hospital anxiety and depression scale. Br. J. Gen. Pract. 1990, 40, 305. [Google Scholar] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Guth, D.; Steer, R.A.; Ball, R. Screening for major depression disorders in medical inpatients with the Beck Depression Inventory for Primary Care. Behav. Res. Ther. 1997, 35, 785–791. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Doneh, B. Epworth Sleepiness Scale. Occup. Med. (Lond.) 2015, 65, 508. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.A.; Hicks, G.; Nino-Murcia, G. Validity and reliability of a scale to assess fatigue. Psychiatry Res. 1991, 36, 291–298. [Google Scholar] [CrossRef]
- MacLean, A.W.; Fekken, G.C.; Saskin, P.; Knowles, J.B. Psychometric evaluation of the Stanford Sleepiness Scale. J. Sleep Res. 1992, 1, 35–39. [Google Scholar] [CrossRef]
- Desai, N.S.; Poindexter, G.B.; Monthrope, Y.M.; Bendeck, S.E.; Swerlick, R.A.; Chen, S.C. A pilot quality-of-life instrument for pruritus. J. Am. Acad. Dermatol. 2008, 59, 234–244. [Google Scholar] [CrossRef]
- Twiss, J.; Meads, D.M.; Preston, E.P.; Crawford, S.R.; McKenna, S.P. Can we rely on the Dermatology Life Quality Index as a measure of the impact of psoriasis or atopic dermatitis? J. Investig. Dermatol. 2012, 132, 76–84. [Google Scholar] [CrossRef]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, K.M.; Egeberg, A.; Gislason, G.H.; Skov, L.; Thyssen, J.P. Anxiety, depression and suicide in patients with prurigo nodularis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, e106–e107. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(a) Nodules in bilateral distribution on arms and (b) legs in a patient diagnosed with prurigo nodularis.
Figure 1.
(a) Nodules in bilateral distribution on arms and (b) legs in a patient diagnosed with prurigo nodularis.

Figure 2.
Diagnostic approach and workup for patients with prurigo nodularis.

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kwon, C.D.; Khanna, R.; Williams, K.A.; Kwatra, M.M.; Kwatra, S.G. Diagnostic Workup and Evaluation of Patients with Prurigo Nodularis. Medicines 2019, 6, 97. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines6040097
AMA Style
Kwon CD, Khanna R, Williams KA, Kwatra MM, Kwatra SG. Diagnostic Workup and Evaluation of Patients with Prurigo Nodularis. Medicines. 2019; 6(4):97. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines6040097
Chicago/Turabian StyleKwon, Christina D., Raveena Khanna, Kyle A. Williams, Madan M. Kwatra, and Shawn G. Kwatra. 2019. "Diagnostic Workup and Evaluation of Patients with Prurigo Nodularis" Medicines 6, no. 4: 97. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines6040097
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.