Acute Kidney Injury in Pediatric Patients on Extracorporeal Membrane Oxygenation: A Systematic Review and Meta-analysis


 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Method
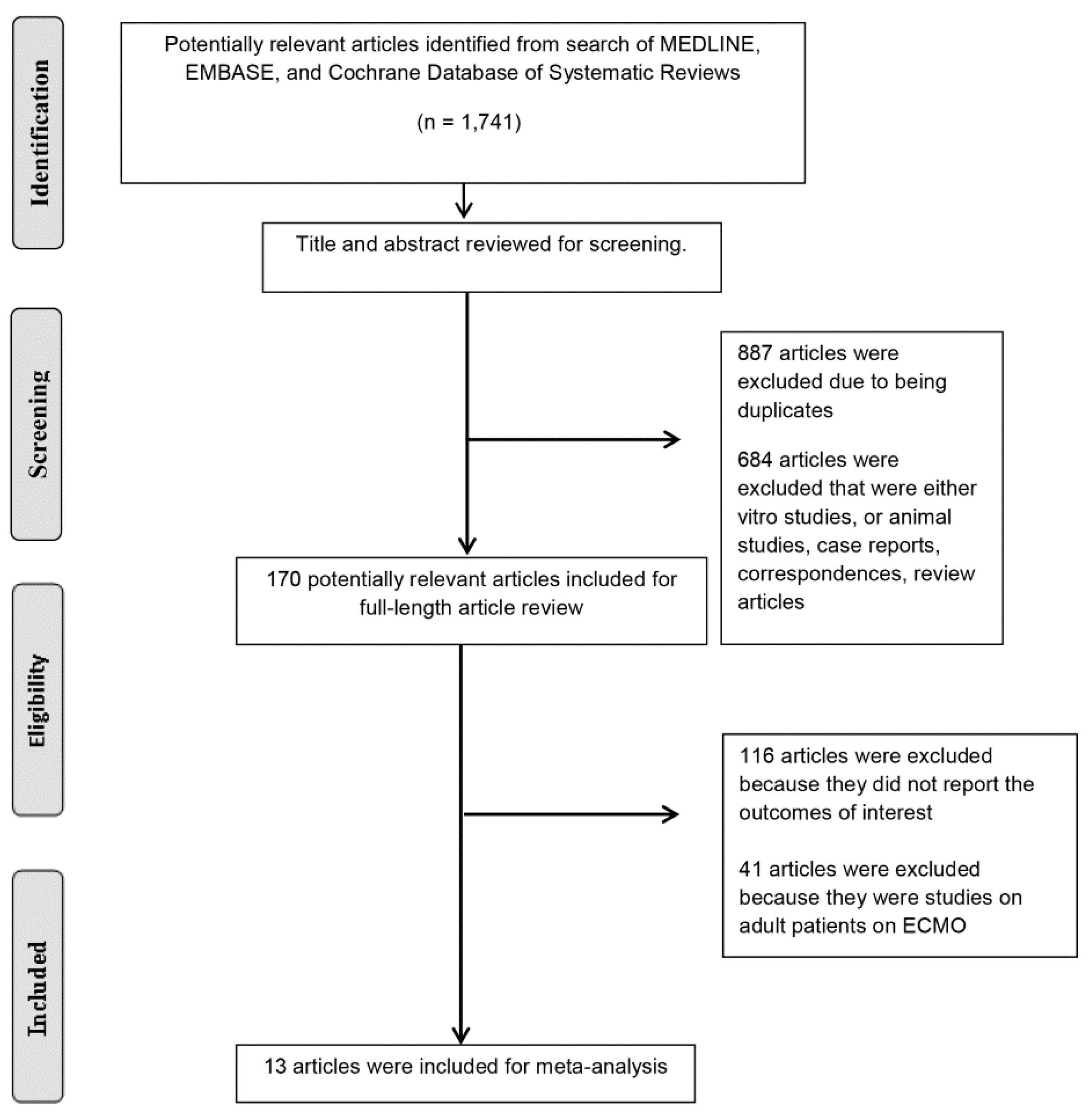
2.1. Literature Review and Search Strategy
2.2. Selection Criteria
2.3. Data Abstraction
2.4. Statistical Analysis
3. Results
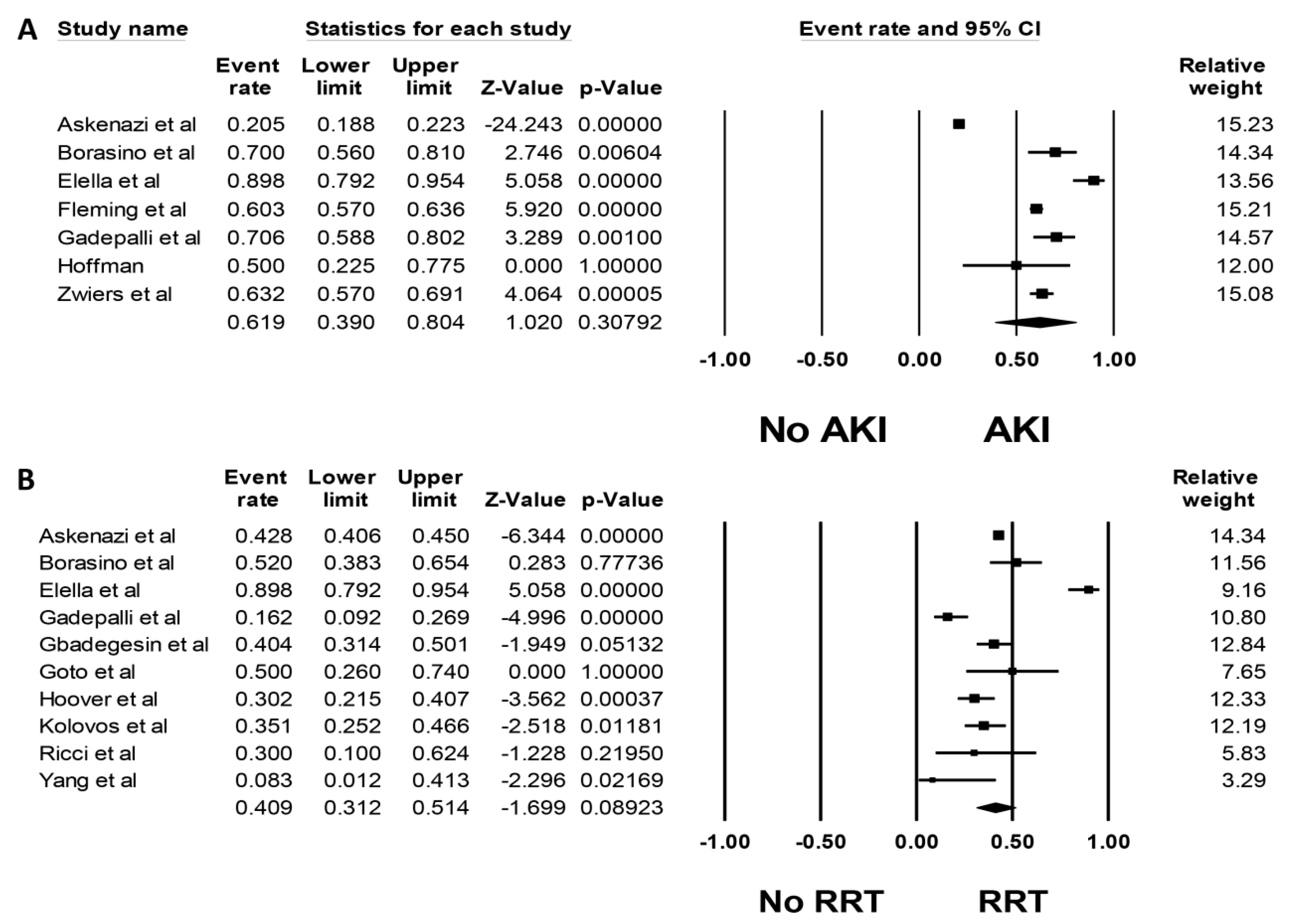
3.1. Incidence of AKI among Pediatric Patients on ECMO
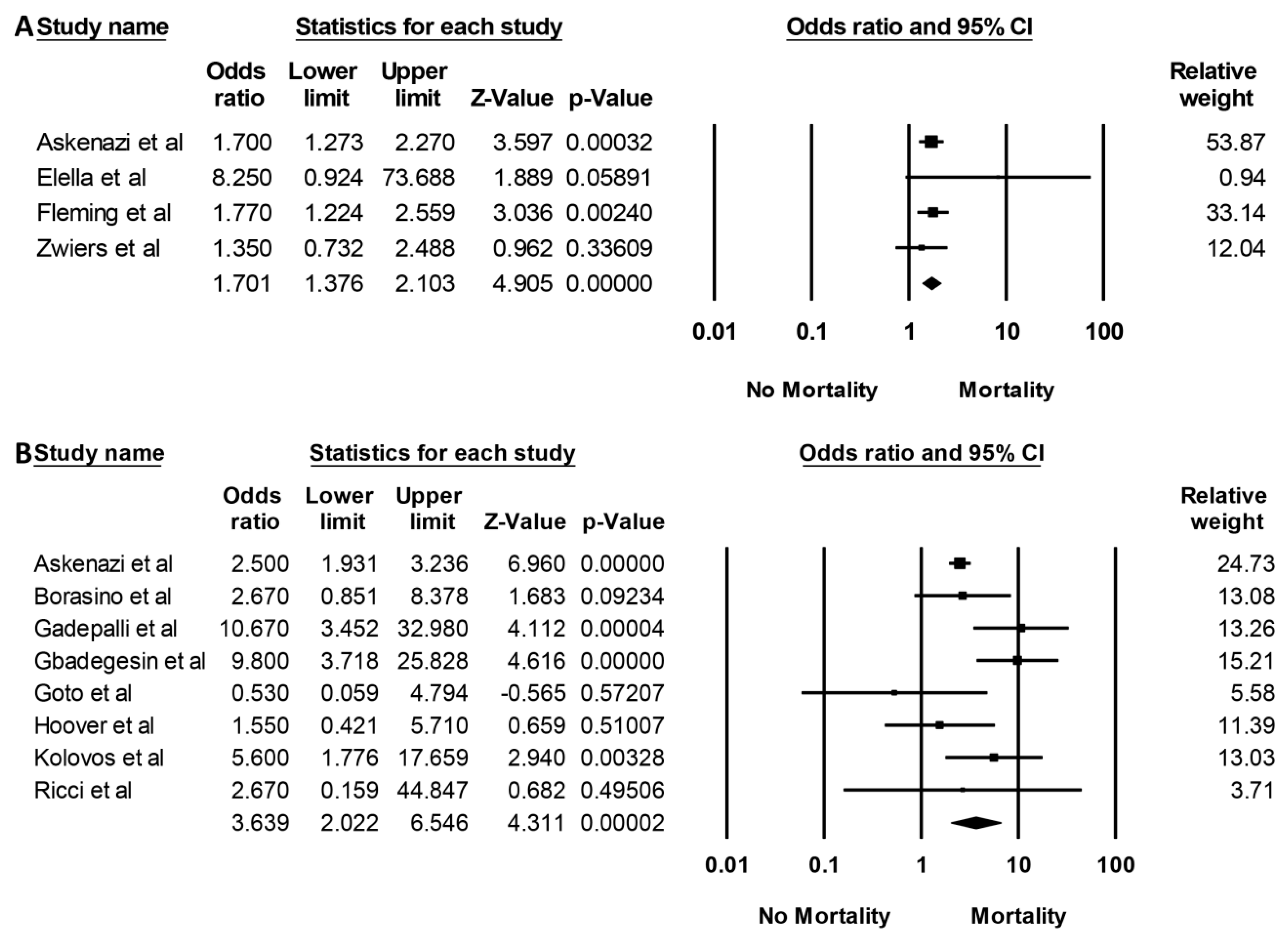
3.2. Mortality in Pediatric ECMO Patients with AKI
3.3. Assessment for Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Makdisi, G.; Wang, I.W. Extra Corporeal Membrane Oxygenation (ECMO) review of a lifesaving technology. J. Thorac. Dis. 2015, 7, 166–176. [Google Scholar]
- Askenazi, D.J.; Selewski, D.T.; Paden, M.L.; Cooper, D.S.; Bridges, B.C.; Zappitelli, M. Renal replacement therapy in critically ill patients receiving extracorporeal membrane oxygenation. Clin. J. Am. Soc. Nephrol. 2012, 7, 1328–1336. [Google Scholar] [CrossRef] [PubMed]
- De Jesus-Brugman, N.; Hobson, M.J.; Herrmann, J.L.; Friedman, M.L.; Cordes, T.; Mastropietro, C.W. Improved outcomes in neonates who require venoarterial extracorporeal membrane oxygenation after the Norwood procedure. Int. J. Artif. Organs 2019. [Google Scholar] [CrossRef] [PubMed]
- Constantinescu, A.R.; Adler, J.L.; Watkins, E.; Negroni-Balasquide, X.L.; Laufenberg, D.; Scholl, F.G.; Lavandosky, G.J. Aquapheresis (AQ) in Tandem with Extracorporeal Membrane Oxygenation (ECMO) in Pediatric Patients. J. Extra Corpor. Technol. 2019, 51, 163–168. [Google Scholar]
- Lopez-Herce, J.; Casado, E.; Diez, M.; Sanchez, A.; Fernandez, S.N.; Bellon, J.M.; Santiago, M.J. Renal function in children assisted with extracorporeal membrane oxygenation. Int. J. Artif. Organs 2019. [Google Scholar] [CrossRef]
- Mallory, P.P.; Selewski, D.T.; Askenazi, D.J.; Cooper, D.S.; Fleming, G.M.; Paden, M.L.; Murphy, L.; Sahay, R.; King, E.; Zappitelli, M.; et al. Acute Kidney Injury, Fluid Overload, and Outcomes in Children Supported With Extracorporeal Membrane Oxygenation for a Respiratory Indication. ASAIO J. 2019. [Google Scholar] [CrossRef]
- Chen, S.W.; Lu, Y.A.; Lee, C.C.; Chou, A.H.; Wu, V.C.; Chang, S.W.; Fan, P.C.; Tian, Y.C.; Tsai, F.C.; Chang, C.H. Long-term outcomes after extracorporeal membrane oxygenation in patients with dialysis-requiring acute kidney injury: A cohort study. PLoS ONE 2019, 14, 0212352. [Google Scholar] [CrossRef]
- Nemoto, M. Experimental evaluation of the influence of complete artificial circulation on renal circulation and tissue metabolism -comparative study of pulsatile vs nonpulsatile circulation. Ann. Thorac. Cardiovasc. Surg. 2003, 9, 355–364. [Google Scholar]
- Pappalardo, F.; Montisci, A. Neurologic complications during V-V extracorporeal membrane oxygenation: Still counting. J. Thorac. Dis. 2017, 9, 2774–2776. [Google Scholar] [CrossRef]
- Thiagarajan, R.R.; Barbaro, R.P.; Rycus, P.T.; McMullan, D.M.; Conrad, S.A.; Fortenberry, J.D.; Paden, M.L. Extracorporeal Life Support Organization Registry International Report 2016. Asaio J. 2017, 63, 60–67. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Lertjitbanjong, P.; Aeddula, N.R.; Bathini, T.; Watthanasuntorn, K.; Srivali, N.; Mao, M.A.; Kashani, K. Incidence and Impact of Acute Kidney Injury in Patients Receiving Extracorporeal Membrane Oxygenation: A Meta-Analysis. J. Clin. Med. 2019, 8, 981. [Google Scholar] [CrossRef] [PubMed]
- Askenazi, D.J.; Ambalavanan, N.; Hamilton, K.; Cutter, G.; Laney, D.; Kaslow, R.; Keith, G.; Douglas, C.B.; Reed, A.D. Acute kidney injury and renal replacement therapy independently predict mortality in neonatal and pediatric noncardiac patients on extracorporeal membrane oxygenation. Pediatr. Crit. Care Med. 2011, 12, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.Y.; Lin, P.J.; Tsai, F.C.; Haung, Y.K.; Liu, K.S.; Tsai, F.C. Impact of preexisting organ dysfunction on extracorporeal life support for non-postcardiotomy cardiopulmonary failure. Resuscitation 2008, 79, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS ONE Med. 2009, 6, 1000097. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Easterbrook, P.J.; Berlin, J.A.; Gopalan, R.; Matthews, D.R. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- Kolovos, N.S.; Bratton, S.L.; Moler, F.W.; Bove, E.L.; Ohye, R.G.; Bartlett, R.H.; Kulik, T.J. Outcome of pediatric patients treated with extracorporeal life support after cardiac surgery. Ann. Thorac. Surg. 2003, 76, 1435–1441. [Google Scholar] [CrossRef]
- Hoover, N.G.; Heard, M.; Reid, C.; Wagoner, S.; Rogers, K.; Foland, J.; Paden, M.L.; Fortenberry, J.D. Enhanced fluid management with continuous venovenous hemofiltration in pediatric respiratory failure patients receiving extracorporeal membrane oxygenation support. Intensive Care Med. 2008, 34, 2241–2247. [Google Scholar] [CrossRef] [PubMed]
- Gbadegesin, R.; Zhao, S.; Charpie, J.; Brophy, P.D.; Smoyer, W.E.; Lin, J.J. Significance of hemolysis on extracorporeal life support after cardiac surgery in children. Pediatr. Nephrol. 2009, 24, 589–595. [Google Scholar] [CrossRef]
- Gadepalli, S.K.; Selewski, D.T.; Drongowski, R.A.; Mychaliska, G.B. Acute kidney injury in congenital diaphragmatic hernia requiring extracorporeal life support: An insidious problem. J. Pediatr. Surg. 2011, 46, 630–635. [Google Scholar] [CrossRef] [PubMed]
- Goto, T.; Suzuki, Y.; Suzuki, Y.; Osanai, A.; Aoki, K.; Yamazaki, A.; Daitoku, K.; Fukuda, I. The impact of extracorporeal membrane oxygenation on survival in pediatric patients with respiratory and heart failure: Review of our experience. Artif. Organs 2011, 35, 1002–1009. [Google Scholar] [CrossRef] [PubMed]
- Ricci, Z.; Morelli, S.; Favia, I.; Garisto, C.; Brancaccio, G.; Picardo, S. Neutrophil gelatinase-associated lipocalin levels during extracorporeal membrane oxygenation in critically ill children with congenital heart disease: Preliminary experience. Pediatr. Crit. Care Med. 2012, 13, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, S.B.; Massaro, A.N.; Soler-Garcia, A.A.; Perazzo, S.; Ray, P.E. A novel urinary biomarker profile to identify acute kidney injury (AKI) in critically ill neonates: A pilot study. Pediatr. Nephrol. 2013, 28, 2179–2188. [Google Scholar] [CrossRef]
- Zwiers, A.J.; de Wildt, S.N.; Hop, W.C.; Dorresteijn, E.M.; Gischler, S.J.; Tibboel, D.; Cransberg, K. Acute kidney injury is a frequent complication in critically ill neonates receiving extracorporeal membrane oxygenation: A 14-year cohort study. Crit. Care 2013, 17, R151. [Google Scholar] [CrossRef]
- Fleming, G.M.; Sahay, R.; Zappitelli, M.; King, E.; Askenazi, D.J.; Bridges, B.C.; Paden, M.L.; Selewski, D.T.; Cooper, D.S. The Incidence of Acute Kidney Injury and Its Effect on Neonatal and Pediatric Extracorporeal Membrane Oxygenation Outcomes: A Multicenter Report From the Kidney Intervention During Extracorporeal Membrane Oxygenation Study Group. Pediatr. Crit. Care Med. 2016, 17, 1157–1169. [Google Scholar] [CrossRef]
- Yang, Z.H.; Ning, B.T.; Zhang, C.M.; Lin, R.; Ye, S.; Liu, T. Clinical application of extracorporeal membrane oxygenation in children with refractory cardiopulmonary failure. World J. Pediatr. 2016, 12, 364–367. [Google Scholar] [CrossRef]
- Elella, R.A.; Habib, E.; Mokrusova, P.; Joseph, P.; Aldalaty, H.; Ahmadi, M.A.; Al Halees, Z. Incidence and outcome of acute kidney injury by the pRIFLE criteria for children receiving extracorporeal membrane oxygenation after heart surgery. Ann. Saudi Med. 2017, 37, 201–206. [Google Scholar] [CrossRef] [Green Version]
- Borasino, S.; Kalra, Y.; Elam, A.R.; Carlisle O’Meara, L.; Timpa, J.G.; Goldberg, K.G.; Leslie Collins Gaddis, J.; Alten, J.A. Impact of Hemolysis on Acute Kidney Injury and Mortality in Children Supported with Cardiac Extracorporeal Membrane Oxygenation. J. Extra Corpor. Technol. 2018, 50, 217–224. [Google Scholar]
- Lin, C.Y.; Chen, Y.C.; Tsai, F.C.; Tian, Y.C.; Jenq, C.C.; Fang, J.T.; Yang, C.W. RIFLE classification is predictive of short-term prognosis in critically ill patients with acute renal failure supported by extracorporeal membrane oxygenation. Nephrol. Dial. Transplant. 2006, 21, 2867–2873. [Google Scholar] [CrossRef] [Green Version]
- Bhatia, I.; Ho, K.C.; Rocha, B.A.; Yam, N.; Lun, K.S.; Yung, T.C.; Au, W.K.T. Pediatric ventricular assist device therapy for advanced heart failure-Hong Kong experience. J. Artif. Organs 2019, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Westaby, S.; Piggot, D.; Dudnikov, S.; Robson, D.; Catarino, P.A.; Clelland, C.; Nojiri, C. End-organ function during chronic nonpulsatile circulation. Ann. Thorac. Surg. 2002, 74, 1080–1085. [Google Scholar] [CrossRef]
- Semmekrot, B.A.; Pesman, G.J.; Span, P.N.; Sweep, C.G.; van Heijst, A.F.; Monnens, L.A.; van de Bor, M.; Tanke, R.B.; van der Staak, F.H.J.M. Serial plasma concentrations of atrial natriuretic peptide, plasma renin activity, aldosterone, and antidiuretic hormone in neonates on extracorporeal membrane oxygenation. Asaio J. 2002, 48, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Yu, W.; Shi, J.; Chen, Q.; Shen, J.; Lin, Z.; He, C.; Li, N.; Li, J. Effects of continuous renal replacement therapy on renal inflammatory cytokines during extracorporeal membrane oxygenation in a porcine model. J. Cardiothorac. Surg. 2013, 8, 113. [Google Scholar]
- McI, R.B.; Timpa, J.G.; Kurundkar, A.R.; Holt, D.W.; Kelly, D.R.; Hartman, Y.E.; Neel, M.L.; Karnatak, R.K.; Schelonka, R.L.; Anantharamaiah, G.M.; et al. Plasma concentrations of inflammatory cytokines rise rapidly during ECMO-related SIRS due to the release of preformed stores in the intestine. Lab. Investig. 2010, 90, 128–139. [Google Scholar]
- Kashani, K.; Cheungpasitporn, W.; Ronco, C. Biomarkers of acute kidney injury: The pathway from discovery to clinical adoption. Clin. Chem. Lab. Med. 2017, 55, 1074–1089. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Year | Country | Patient Population | Number | Definition of AKI | Incidence of AKI | Mortality |
|---|---|---|---|---|---|---|---|
| Kolovos et al. [18] | 2003 | USA | Patients on ECMO within seven days after cardiac surgery | 74 | RRT | RRT 26/74 (35%) | Hospital mortality RRT 20/26 (77%) |
| Hoover et al. [19] | 2008 | USA | Patients aged 1 month to 18 years with respiratory failure requiring ECMO | 86 | CRRT | CRRT 26/86 (30%) | Hospital mortality RRT 7/26 (27%) |
| Gbadegesin et al. [20] | 2009 | USA | Patients aged < 3 years requiring ECMO after cardiac surgery | 104 | CRRT | CRRT 42/104 (40%) | Hospital mortality RRT 35/42 (83%) |
| Gadepalli et al. [21] | 2010 | USA | Congenital diaphragmatic hernia patients requiring ECMO | 68 | AKI: RIFLE | AKI 48/68 (71%) RIFLE—failure AKI 33/68 (49%) CRRT 11/68 = 16% | Mortality RIFLE—failure AKI 24/33 (73%) |
| Goto et al. [22] | 2011 | USA | Patients aged 19 days to 20 years with respiratory failure and/or heart failure requiring ECMO | 14 | RRT | RRT 7/14 (50%) | Hospital mortality RRT 2/7 (29%) |
| Askenazi et al. [12] | 2011 | USA | All non-cardiac patients requiring ECMO | 9903 Neonates -7941 Children -1962 | SCr > 1.5 mg/dL or ICD-9 for acute renal failure | Neonates AKI—638/7941 (8%) RRT—1786/7941 (22%) Children AKI—402/1962 (20%) RRT—840/1962 (43%) | Neonates Hospital mortality AKI—413/638 (65%) RRT—863/1786 (48%) Children Hospital mortality AKI—264/402 (66%) RRT—487/840 (58%) |
| Ricci et al. [23] | 2012 | Italy | Patients aged 13 days to 13 years on VA ECMO after cardiac surgery | 10 | CRRT | CRRT 3/10 (30%) | Hospital mortality RRT 2/3 (66%) |
| Hoffman et al. [24] | 2013 | USA | Patients with persistent hypoxia or cardiovascular instability requiring ECMO | 10 | AKI; (1) urine output < 1 ml/kg/h with SCr > 1 mg/dL for 24 hours, (2) SCr of > 1.5 mg/dL, (3) failure to improve creatinine clearance by > 50% | AKI 5/10 (50%) | N/A |
| Zwiers et al. [25] | 2013 | Netherlands | Neonates aged < 28 days requiring ECMO | 242 | AKI: RIFLE | AKI 153/242 (63%) | Hospital mortality AKI 43/153 (28%) |
| Fleming et al. [26] | 2016 | USA | Pediatric patients aged < 18 requiring ECMO | 832 | AKI: KDIGO | AKI by SCr—502/832 (60%) AKI by SCr + renal support therapy—615/832 (74%) | N/A |
| Yang et al. [27] | 2016 | China | Patients aged 1 to 13 years with refractory cardiopulmonary failure requiring ECMO | 12 | CRRT | CRRT 1/12 (8%) | Hospital mortality RRT 0/1 (0%) |
| Elella et al. [28] | 2017 | Saudi Arabia | Pediatric patients requiring VA-ECMO after cardiac surgery | 59 | AKI pRIFLE | AKI 53/59 (90%) RRT 29/59 (49%) | Hospital mortality AKI 33/53 (62%) |
| Borasino et al. [29] | 2018 | USA | Pediatric cardiac patient on ECMO in CICU | 50 | AKI: increase in SCr of 200% from baseline | AKI 35/50 (70%) RRT 26/50 (52%) | Hospital mortality RRT 16/26 (61%) |
| Study | Mortality Rate | OR for Mortality |
|---|---|---|
| Kolovos et al. [18] | Hospital mortality RRT 20/26 (77%) | Hospital mortality RRT: OR 5.6 (1.8–17.9) |
| Hoover et al. [19] | Hospital mortality RRT 7/26 (27%) | Hospital mortality CRRT: 1.55 (0.42–5.70) |
| Gbadegesin et al. [20] | Hospital mortality RRT 35/42 (83%) | Hospital mortality CRRT: 9.8 (3.7–25.7) |
| Gadepalli et al. [21] | Mortality RIFLE—failure AKI 24/33 (73%) | Hospital mortality RIFLE—Failure AKI: 10.67 (3.45–32.96) |
| Goto et al. [22] | Hospital mortality RRT 2/7 (29%) | Hospital mortality RRT: 0.53 (0.06–4.91) |
| Askenazi et al. [12] | Neonates Hospital mortality AKI—413/638 (65%) RRT—863/1786 (48%) Children Hospital mortality AKI—264/402 (66%) RRT—487/840 (58%) | Hospital mortality Neonates AKI: 3.2 (2.6–4.0) RRT: 1.9 (1.6–2.2) Children AKI: 1.7 (1.3–2.3) RRT: 2.5 (1.9–3.2) |
| Ricci et al. [23] | Hospital mortality RRT 2/3 (66%) | Hospital mortality CRRT: 2.67 (0.16–45.14) |
| Zwiers et al. [25] | Hospital mortality AKI 43/153 (28%) | Hospital mortality AKI: 1.35 (0.73–2.48) |
| Fleming et al. [26] | N/A | Hospital mortality AKI-SCr: 1.77 (1.22–2.55) AKI-SCr+RST: 2.50 (1.61–3.90) |
| Yang et al. [27] | Hospital mortality RRT 0/1 (0%) | Hospital mortality CRRT: 0/1 vs. 4/11 |
| Elella et al. [28] | Hospital mortality AKI 33/53 (62%) | Hospital mortality AKI: 8.25 (0.90–75.79) |
| Borasino et al. [29] | Hospital mortality RRT 16/26 (61%) | Hospital morality RRT: 2.67 (0.85–8.37) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hansrivijit, P.; Lertjitbanjong, P.; Thongprayoon, C.; Cheungpasitporn, W.; Aeddula, N.R.; Salim, S.A.; Chewcharat, A.; Watthanasuntorn, K.; Srivali, N.; Mao, M.A.; et al. Acute Kidney Injury in Pediatric Patients on Extracorporeal Membrane Oxygenation: A Systematic Review and Meta-analysis. Medicines 2019, 6, 109. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines6040109
Hansrivijit P, Lertjitbanjong P, Thongprayoon C, Cheungpasitporn W, Aeddula NR, Salim SA, Chewcharat A, Watthanasuntorn K, Srivali N, Mao MA, et al. Acute Kidney Injury in Pediatric Patients on Extracorporeal Membrane Oxygenation: A Systematic Review and Meta-analysis. Medicines. 2019; 6(4):109. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines6040109
Chicago/Turabian StyleHansrivijit, Panupong, Ploypin Lertjitbanjong, Charat Thongprayoon, Wisit Cheungpasitporn, Narothama Reddy Aeddula, Sohail Abdul Salim, Api Chewcharat, Kanramon Watthanasuntorn, Narat Srivali, Michael A. Mao, and et al. 2019. "Acute Kidney Injury in Pediatric Patients on Extracorporeal Membrane Oxygenation: A Systematic Review and Meta-analysis" Medicines 6, no. 4: 109. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines6040109