
Safety of Insulin Degludec/Insulin Aspart in Patients with Diabetes Mellitus over a Period of 1 Year during Routine Clinical Care in India: SMART (Study of Management of Diabetes with Ryzodeg™ Treatment)


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Safety Assessments
2.4. Assessment of the Change in HbA1c, FPG, and PPG
2.5. Statistical Analyses
3. Results
3.1. Patient Disposition and Baseline Characteristics
3.2. Safety and Tolerability
3.2.1. Adverse Events
3.2.2. Adverse Drug Reactions
3.2.3. Hypoglycemic Events
3.2.4. Clinical Laboratory Findings and Vital Parameters
3.3. Change in HbA1c, FPG, and PPG
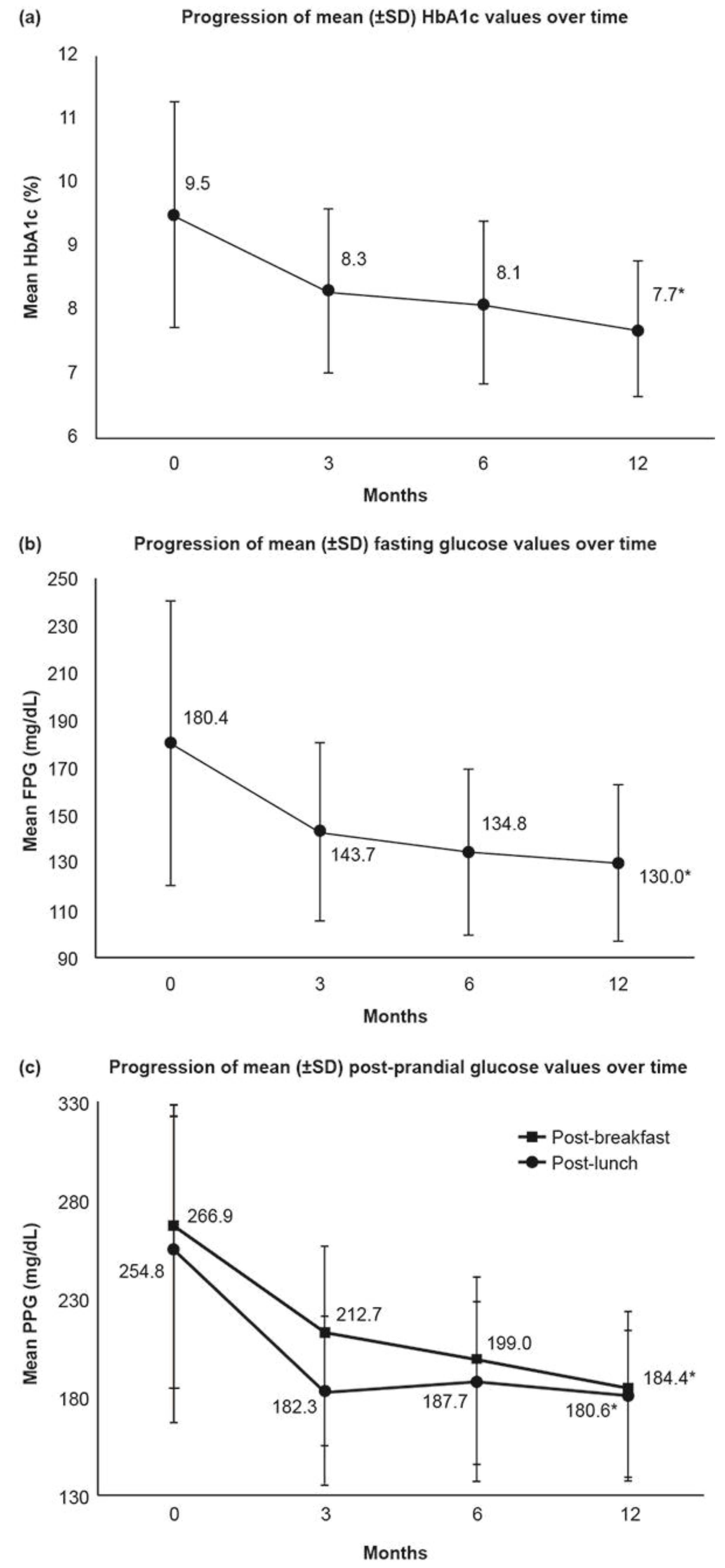
3.3.1. Glycosylated Hemoglobin
3.3.2. Fasting Plasma Glucose/Fasting Blood Glucose
3.3.3. Post-Prandial Plasma Glucose
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- IDF (International Diabetes Federation). IDF Diabetes Atlas, 9th ed.; IDF: Brussels, Belgium, 2019; Available online: https://www.idf.org/e-library/epidemiology-research/diabetes-atlas/159-idf-diabetes-atlas-ninth-edition-2019.html (accessed on 8 July 2021).
- American Diabetes Association: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S1–S232. Available online: https://care.diabetesjournals.org/content/44/Supplement_1 (accessed on 8 July 2021). [CrossRef]
- Chawla, R.; Makkar, B.M.; Aggarwal, S.; Bajaj, S.; Das, A.K.; Ghosh, S.; Gupta, A.; Gupta, S.; Jaggi, S.; Jana, J.; et al. RSSDI consensus recommendations on insulin therapy in the management of diabetes. Int. J. Diabetes Dev. Ctries. 2019, 39, S43–S92. [Google Scholar] [CrossRef]
- Chawla, R.; Madhu, S.V.; Makkar, B.M.; Ghosh, S.; Saboo, B.; Kalra, S. RSSDI-ESI clinical practice recommendations for the management of type 2 diabetes mellitus 2020. Int. J. Diabetes Dev. Ctries. 2020, 24, 1–122. [Google Scholar] [CrossRef]
- Chan, J.C.; Bunnag, P.; Chan, S.P.; Tan, I.T.; Tsai, S.-T.; Gao, L.; Landgraf, W. Glycaemic responses in Asian and non-Asian people with type 2 diabetes initiating insulin glargine 100 units/mL: A patient-level pooled analysis of 16 randomised controlled trials. Diabetes Res. Clin. Pr. 2018, 135, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Woerle, H.J.; Neumann, C.; Zschau, S.; Tenner, S.; Irsigler, A.; Schirra, J.; Gerich, J.E.; Göke, B. Impact of fasting and postprandial glycemia on overall glycemic control in type 2 diabetes: Importance of postprandial glycemia to achieve target HbA1c levels. Diabetes Res. Clin. Pr. 2007, 77, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Mohan, V.; Unnikrishnan, R.; Shobana, S.; Malavika, M.; Anjana, R.; Sudha, V. Are excess carbohydrates the main link to diabetes & its complications in Asians? Indian J. Med. Res. 2018, 148, 531–538. [Google Scholar] [CrossRef]
- Mohan, V.; Kalra, S.; Kesavadev, J.; Singh, A.; Kumar, A.; Unnikrishnan, A.G.; Chawla, R.; Mukherjee, J.J.; Sahay, R.; Kumar, J.S.; et al. Consensus on Initiation and Intensification of Premix Insulin in Type 2 Diabetes Management. J. Assoc. Physicians India 2017, 65, 59–73. [Google Scholar]
- Sheldon, B.; Russell-Jones, D.; Wright, J. Insulin analogues: An example of applied medical science. Diabetes Obes. Metab. 2008, 11, 5–19. [Google Scholar] [CrossRef]
- Polonsky, W.H.; Fisher, L.; Guzman, S.; Villa-Caballero, L.; Edelman, S.V. Psychological Insulin Resistance in Patients with Type 2 Diabetes: The scope of the problem. Diabetes Care 2005, 28, 2543–2545. [Google Scholar] [CrossRef] [Green Version]
- Onishi, Y.; Ono, Y.; Rabol, R.; Endahl, L.; Nakamura, S. Superior glycemic control with once-daily insulin degludec/insulin aspart versus insulin glargine in Japanese adults with type 2 diabetes inadequately controlled with oral drugs: A randomized, controlled phase 3 trial. Diabetes Obes. Metab. 2013, 15, 826–832. [Google Scholar] [CrossRef]
- Heise, T.; Tack, C.J.; Cuddihy, R.; Davidson, J.; Gouet, D.; Liebl, A.; Romero, E.; Mersebach, H.; Dykiel, P.; Jorde, R. A new-generation ultra-long-acting basal insulin with a bolus boost compared with insulin glargine in insulin-naive people with type 2 diabetes: A randomized, controlled trial. Diabetes Care 2011, 34, 669–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niskanen, L.; Leiter, L.A.; Franek, E.; Weng, J.; Damci, T.; Muñoz-Torres, M.; Donnet, J.-P.; Endahl, L.; Skjøth, T.V.; Vaag, A. Comparison of a soluble co-formulation of insulin degludec/insulin aspart vs biphasic insulin aspart 30 in type 2 diabetes: A randomised trial. Eur. J. Endocrinol. 2012, 167, 287–294. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, I.B.; Bode, B.; Courreges, J.-P.; Dykiel, P.; Franek, E.; Hermansen, K.; King, A.; Mersebach, H.; Davies, M. Insulin degludec/insulin aspart administered once daily at any meal, with insulin aspart at other meals versus a standard basal-bolus regimen in patients with type 1 diabetes: A 26-week, phase 3, randomized, open-label, treat-to-target trial. Diabetes Care 2012, 35, 2174–2181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodbard, H.W.; Cariou, B.; Pieber, T.R.; Endahl, L.A.; Zacho, J.; Cooper, J.G. Treatment intensification with an insulin degludec (IDeg)/insulin aspart (IAsp) co-formulation twice daily compared with basal IDeg and prandial IAsp in type 2 diabetes: A randomized, controlled phase III trial. Diabetes Obes. Metab. 2016, 18, 274–280. [Google Scholar] [CrossRef]
- Philis-Tsimikas, A.; Astamirova, K.; Gupta, Y.; Haggag, A.; Roula, D.; Bak, B.A.; Fita, E.G.; Nielsen, A.M.; Demir, T. Similar glycemic control with less nocturnal hypoglycaemia in a 38-week trial comparing the IDegAsp co-formulation with insulin glargine U100 and insulin aspart in basal insulin-treated subjects with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2019, 147, 157–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novo Nordisk Company Announcement. Ryzodeg® (Insulin Degludec/Insulin Aspart) Approved in Japan. 25 December 2012. Available online: https://www.novonordisk.com/content/nncorp/global/en/news-and-media/news-and-ir-materials/news-details.html?id=2111 (accessed on 8 July 2021).
- Fierce Biotech. FDA Approves Two New Drug Treatments for Diabetes Mellitus. Available online: https://www.fiercebiotech.com/biotech/fda-approves-two-new-drug-treatments-for-diabetes-mellitus (accessed on 8 July 2021).
- The Economic Times. Novo Nordisk Launches Diabetes Drug Ryzodeg in India. Available online: https://health.economictimes.indiatimes.com/news/pharma/novo-nordisk-launches-diabetes-drug-ryzodeg-in-india/45941727 (accessed on 8 July 2021).
- Kumar, A.; Sharma, S.K.; Gupta, A.; Dasgupta, A.; Asirvatham, A.J.; Talwalkar, P.G.; Das, A.K.; Mohan, V. Indian reality of managing type 2 diabetes: An expert review of global and national guidelines for optimum insulin use. J. Diabetol. 2020, 11, 148. [Google Scholar] [CrossRef]
- Hompesch, M.; Morrow, L.; Watkins, E.; Roepstorff, C.; Thomsen, H.F.; Haahr, H. Pharmacokinetic and pharmacodynamic responses of insulin degludec in African American, White, and Hispanic/Latino patients with type 2 diabetes mellitus. Clin. Ther. 2014, 36, 507–515. [Google Scholar] [CrossRef] [Green Version]
- Heise, T.; Korsatko, S.; Nosek, L.; Coester, H.V.; Deller, S.; Roepstorff, C.; Segel, S.; Kapur, R.; Haahr, H.; Hompesch, M. Steady state is reached within 2–3 days of once-daily administration of degludec, a basal insulin with an ultralong duration of action. J. Diabetes 2015, 8, 132–138. [Google Scholar] [CrossRef]
- Kesavadev, J.; Saboo, B.D.; Shankar, A.; David, A.; Warrier, R.; Krishnan, G.; Ramachandran, L.; Jothydev, S. IDegAsp improves glycemic control with minimal hypoglycemia—An Indian real-world study in T2D subjects. Diabetes 2018, 67, 389. [Google Scholar] [CrossRef]
- Franek, E.; Haluzik, M.; Varžić, S.C.; Sargin, M.; Macura, S.; Zacho, J.; Christiansen, J.S. Twice-daily insulin degludec/insulin aspart provides superior fasting plasma glucose control and a reduced rate of hypoglycaemia compared with biphasic insulin aspart 30 in insulin-naïve adults with Type 2 diabetes. Diabet. Med. 2015, 33, 497–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalra, S.; Baruah, M.P. Insulin degludec aspart: One-year real world experience. Indian J. Endocrinol. Metab. 2016, 20, 369–371. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Category | Enrolled Population (N = 1029) n (%) |
|---|---|
| Patients in safety analysis set a | 1029 (100) |
| Patients in efficacy analysis set b | 1003 (97.5) |
| Patients completed study | 971 (94.4) |
| Patients discontinued study | 58 (5.6) |
| Reason for discontinuation c | |
| Lost to follow-up | 41 (4.0) |
| Adverse drug reaction | 0 |
| IDegAsp discontinued | 12 (1.2) |
| Other | 6 (0.6) |
| Parameters | N = 1029 |
|---|---|
| Men, n (%) | 671 (65.2) |
| Age (completed years), mean ± SD | 55.0 ± 12.2 a |
| Hip circumference (cm), mean ± SD | 98.7 ± 12.5 b |
| Waist circumference (cm), mean ± SD | 95.2 ± 11.6 c |
| Weight (kg), mean ± SD | 73.2 ± 12.5 d |
| Microvascular complications, n (%) | |
| Peripheral neuropathy | 214 (20.8) |
| Nephropathy | 74 (7.2) |
| Autonomic neuropathy | 72 (7.0) |
| Retinopathy | 63 (6.1) |
| Macrovascular complications, n (%) | |
| Coronary heart disease | 76 (7.4) |
| Stroke | 22 (2.1) |
| Macroangiopathy including peripheral vascular disease | 20 (1.9) |
| Reasons to start IDegAsp, n (%) | |
| Improve HbA1c | 895 (87.0) |
| Improve PPG | 645 (62.7) |
| Improve FPG | 593 (57.6) |
| Reduce risk of hypoglycemia | 413 (40.1) |
| Need for flexibility in timing of injection | 228 (22.2) |
| Patients dissatisfaction with previous therapy | 153 (14.9) |
| Side effects from previous therapy | 27 (2.6) |
| Improve weight control | 126 (12.2) |
| Improve beta cell function | 73 (7.1) |
| Other | 6 (0.6) |
| Adverse Event (N = 1029) n (%) | Adverse Drug Reaction (N = 1029) n (%) | |
|---|---|---|
| Total number of AEs/ADRs reported | 30 | 7 |
| Patients reporting any AEs/ADRs | 23 (2.2) {30} | 5 (0.5) {7} |
| Patients reporting 1 AEs/ADRs | 18 (1.7) {18} | 4 (0.4) {4} |
| Patients reporting >1 AEs/ADRs | 5 (0.5) {12} | 1 (0.1) {3} |
| Serious AEs/ADRs | 2 (0.2) {2} | - |
| Life-threatening AEs/ADRs | 2 (0.2) {2} | - |
| Severity | ||
| Mild | 19 (1.8) {25} | 3 (0.3) {5} |
| Moderate | 1 (0.1) {1} | 1 (0.1) {1} |
| Severe | 3 (0.3) {4} | 1 (0.1) {1} |
| Outcome of AEs | ||
| Recovered/Resolved | 16 (1.6) {19} | 3 (0.3) {3} |
| Not recovered/Not resolved | 5 (0.5) {8} | 1 (0.1) {3} |
| Recovering/Resolving | - | - |
| Fatal | 2 (0.2) {2} | - |
| Recovered/Resolved with sequelae | - | - |
| Unknown | 1 (0.1) {1} | 1 (0.1) {1} |
| Causality | ||
| Probable | 3 (0.3) {5} | - |
| Possible | 2 (0.2) {2} | - |
| Unlikely | 20 (1.9) {23} | - |
| Actions taken to study product(s) due to adverse event/adverse drug reaction | ||
| Drug interrupted | - | - |
| Drug withdrawn | 2 (0.2) {3} | 2 (0.2) {2} |
| Dose reduced | 2 (0.2) {2} | 1 (0.1) {1} |
| Dose increased | - | - |
| Dose not changed | 7 (0.7) {12} | 1 (0.1) {3} |
| Unknown | - | - |
| Not applicable | 12 (1.2) {13} | 1 (0.1) {1} |
| AEs reported in ≥2 patients or number of ADRs reported | ||
| Fatigue | 2 (0.2) {2} | 1 (1.0) {1} |
| Pyrexia | 5 (0.5) {5} | - |
| Upper respiratory tract infection | 2 (0.2) {2} | - |
| Dizziness | 2 (0.2) {2} | 1 (0.1) {1} |
| Muscle spasms | 2 (0.2) {2} | - |
| Weight gain | - | 1 (0.1) {1} |
| Hyperglycemia | - | 1 (0.1) {1} |
| Increased appetite | - | 1 (0.1) {2} |
| Injury, poisoning, and procedural complications | - | 1 (1.0) {1} |
| Parameters | Visit 1 (Baseline) | Visit 2 (3 Months ±2 Weeks) | Visit 3 (6 Months ±2 Weeks) | Visit 4 (12 Months ±2 Weeks) |
|---|---|---|---|---|
| Confirmed hypoglycemia | 67 (6.7%) {176} | 12 (1.2%) {28} | 15 (1.5%) {17} | 11 (1.1%) {11} |
| Severe hypoglycemia | 17 (1.7%) {24} | Nil | Nil | Nil |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kesavadev, J.; Gowda, A.; Kumar, H.; Yalamanchi, S.R.; Lodha, S.; Singh, K.P.; Basu, D.; Asirvatham, A.; Shah, N.; Pathan, M.K.; et al. Safety of Insulin Degludec/Insulin Aspart in Patients with Diabetes Mellitus over a Period of 1 Year during Routine Clinical Care in India: SMART (Study of Management of Diabetes with Ryzodeg™ Treatment). Med. Sci. 2022, 10, 1. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010001
Kesavadev J, Gowda A, Kumar H, Yalamanchi SR, Lodha S, Singh KP, Basu D, Asirvatham A, Shah N, Pathan MK, et al. Safety of Insulin Degludec/Insulin Aspart in Patients with Diabetes Mellitus over a Period of 1 Year during Routine Clinical Care in India: SMART (Study of Management of Diabetes with Ryzodeg™ Treatment). Medical Sciences. 2022; 10(1):1. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010001
Chicago/Turabian StyleKesavadev, Jothydev, Ambanna Gowda, Harish Kumar, Sadasiva Rao Yalamanchi, Sailesh Lodha, Kiran Pal Singh, Debasis Basu, Arthur Asirvatham, Navneet Shah, Muzammil Khan Pathan, and et al. 2022. "Safety of Insulin Degludec/Insulin Aspart in Patients with Diabetes Mellitus over a Period of 1 Year during Routine Clinical Care in India: SMART (Study of Management of Diabetes with Ryzodeg™ Treatment)" Medical Sciences 10, no. 1: 1. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010001