Efficacy and Safety of SGLT-2 Inhibitors for Treatment of Diabetes Mellitus among Kidney Transplant Patients: A Systematic Review and Meta-Analysis

 ,
, 
Abstract
:1. Introduction
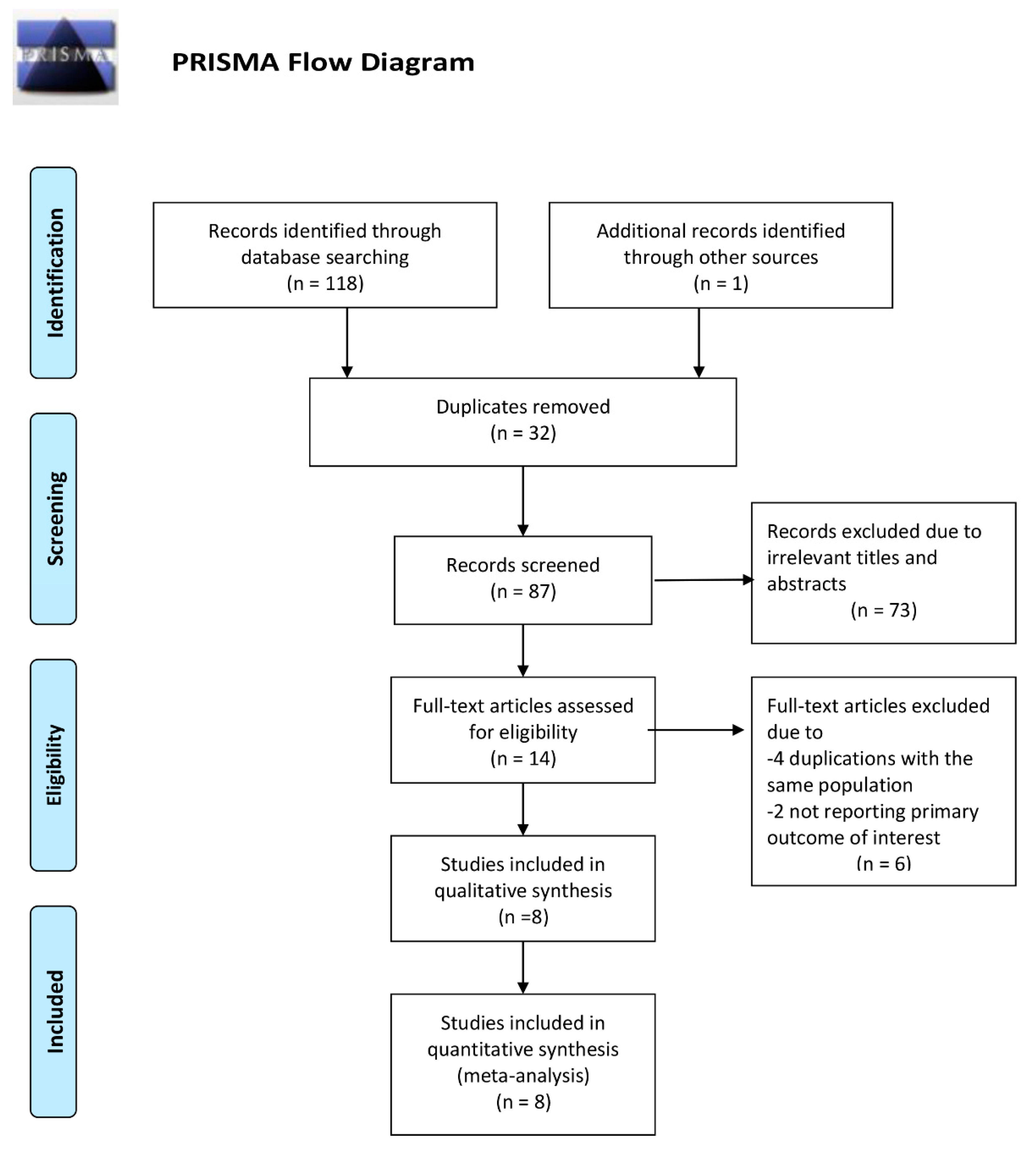
2. Materials and Methods
2.1. Data Sources and Search Strategies
2.2. Study Selection
2.3. Data Extraction
2.4. Data Synthesis and Statistical Analysis
3. Results
3.1. Characteristics and Quality of Studies
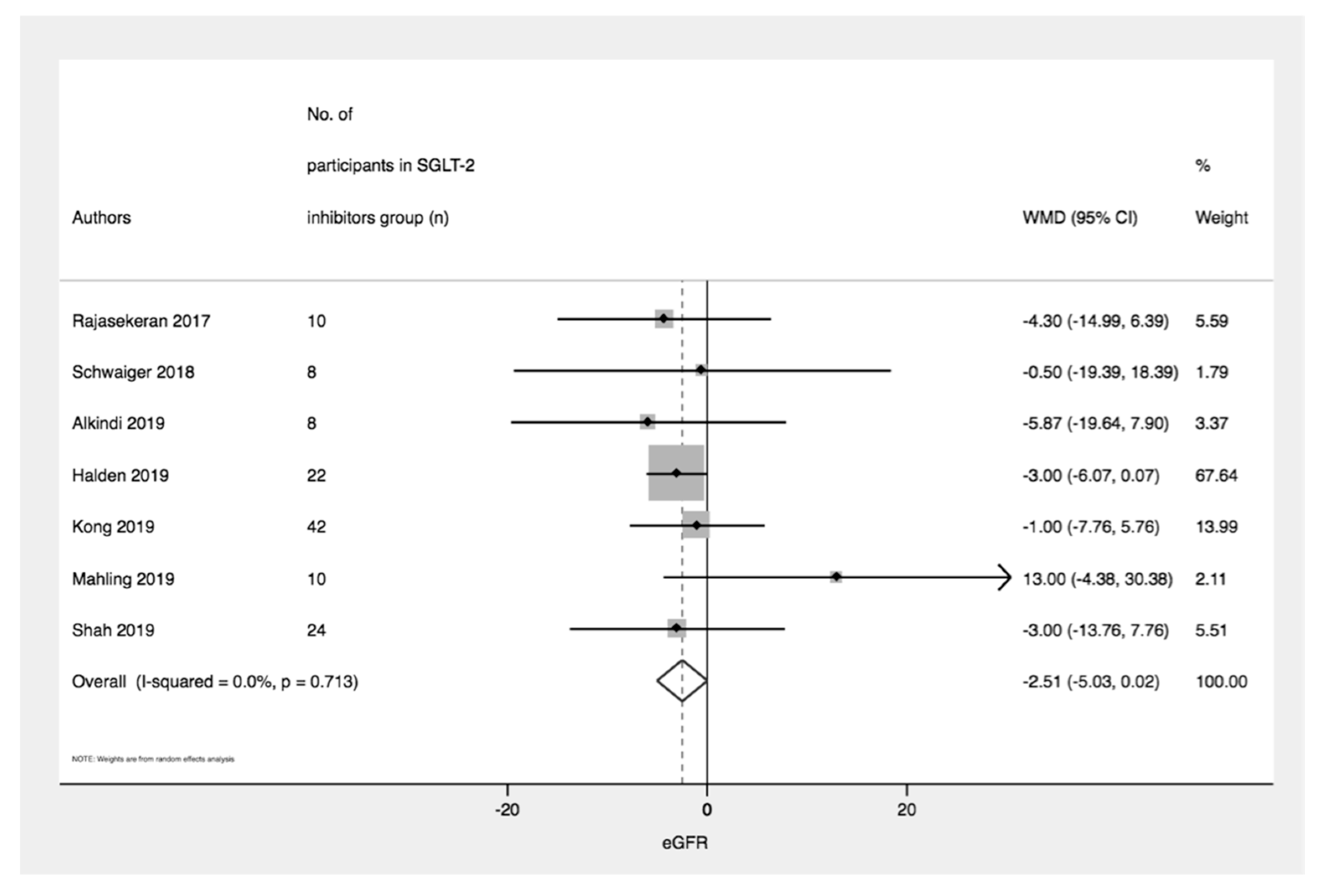
3.2. Efficacy of SGLT-2 Inhibitors on Kidney Function
3.3. Efficacy of SGLT-2 Inhibitors on Glycated Hemoglobin
3.4. Efficacy of SGLT-2 Inhibitors on Blood Pressure and Body Weight
3.5. Safety Profiles of SGLT-2 Inhibitors
3.6. Subgroup Analysis
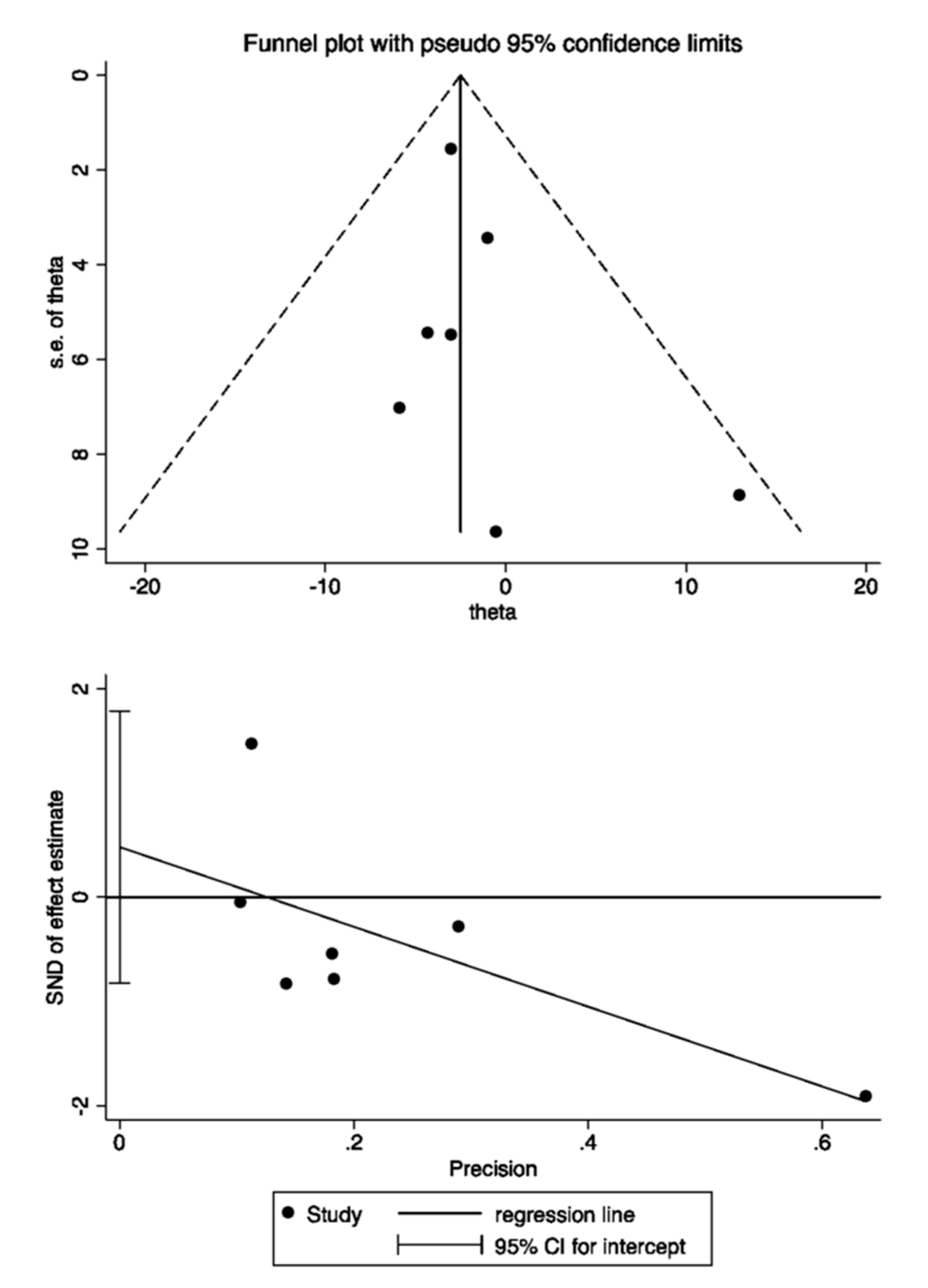
3.7. Assessment of Publication bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Koye, D.N.; Magliano, D.J.; Nelson, R.G.; Pavkov, M.E. The Global Epidemiology of Diabetes and Kidney Disease. Adv. Chronic Kidney Dis. 2018, 25, 121–132. [Google Scholar] [CrossRef]
- Hart, A.; Smith, J.M.; Skeans, M.A.; Gustafson, S.K.; Wilk, A.R.; Robinson, A.; Wainright, J.L.; Haynes, C.R.; Snyder, J.J.; Kasiske, B.L.; et al. OPTN/SRTR 2016 Annual Data Report: Kidney. Arab. Archaeol. Epigr. 2018, 18, 18–113. [Google Scholar] [CrossRef] [PubMed]
- Cosio, F.G.; Pesavento, T.E.; Kim, S.; Osei, K.; Henry, M.; Ferguson, R.M. Patient survival after renal transplantation: IV. Impact of post-transplant diabetes. Kidney Int. 2002, 62, 1440–1446. [Google Scholar] [CrossRef] [PubMed]
- Kasiske, B.L.; Snyder, J.J.; Gilbertson, D.; Matas, A.J. Diabetes Mellitus after Kidney Transplantation in the United States. Arab. Archaeol. Epigr. 2003, 3, 178–185. [Google Scholar] [CrossRef]
- Woodward, R.S.; Schnitzler, M.A.; Baty, J.D.; Lowell, J.A.; Lopez-Rocafort, L.; Haider, S.; Woodworth, T.G.; Brennan, D.C. Incidence and Cost of New Onset Diabetes Mellitus Among U.S. Wait-Listed and Transplanted Renal Allograft Recipients. Arab. Archaeol. Epigr. 2003, 3, 590–598. [Google Scholar] [CrossRef] [Green Version]
- Shivaswamy, V.; Boerner, B.; Larsen, J. Post-Transplant Diabetes Mellitus: Causes, Treatment, and Impact on Outcomes. Endocr. Rev. 2016, 37, 37–61. [Google Scholar] [CrossRef] [Green Version]
- Paek, J.H.; Kang, S.S.; Park, W.Y.; Jin, K.; Park, S.B.; Han, S.; Kim, C.-D.; Ro, H.; Lee, S.; Jung, C.W.; et al. Incidence of Post-transplantation Diabetes Mellitus Within 1 Year After Kidney Transplantation and Related Factors in Korean Cohort Study. Transplant. Proc. 2019, 51, 2714–2717. [Google Scholar] [CrossRef]
- Eide, I.A.; Halden, T.A.S.; Hartmann, A.; Dahle, D.O.; Åsberg, A.; Jenssen, T. Associations Between Posttransplantation Diabetes Mellitus and Renal Graft Survival. Transplantation 2017, 101, 1282–1289. [Google Scholar] [CrossRef]
- Dienemann, T.; Fujii, N.; Li, Y.; Govani, S.; Kosaraju, N.; Bloom, R.D.; Feldman, H.I. Long-term patient survival and kidney allograft survival in post-transplant diabetes mellitus: A single-center retrospective study. Transpl. Int. 2016, 29, 1017–1028. [Google Scholar] [CrossRef] [Green Version]
- Cooper, L.; Oz, N.; Fishman, G.; Shohat, T.; Rahamimov, R.; Mor, E.; Green, H.; Grossman, A. New onset diabetes after kidney transplantation is associated with increased mortality-A retrospective cohort study. Diabetes/Metab. Res. Rev. 2017, 33, e2920. [Google Scholar] [CrossRef]
- Kuo, H.-T.; Sampaio, M.S.; Vincenti, F.; Bunnapradist, S. Associations of Pretransplant Diabetes Mellitus, New-Onset Diabetes After Transplant, and Acute Rejection with Transplant Outcomes: An Analysis of the Organ Procurement and Transplant Network/United Network for Organ Sharing (OPTN/UNOS) Database. Am. J. Kidney Dis. 2010, 56, 1127–1139. [Google Scholar] [CrossRef] [PubMed]
- Valderhaug, T.G.; Hjelmesæth, J.; Hartmann, A.; Røislien, J.; Bergrem, H.A.; Leivestad, T.; Line, P.D.; Jenssen, T. The association of early post-transplant glucose levels with long-term mortality. Diabetologia 2011, 54, 1341–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galindo, R.J.; Fried, M.; Breen, T.; Tamler, R. HYPERGLYCEMIA MANAGEMENT IN PATIENTS WITH POSTTRANSPLANTATION DIABETES. Endocr. Pract. 2016, 22, 454–465. [Google Scholar] [CrossRef]
- Lo, C.; Jun, M.; Badve, S.V.; Pilmore, H.; White, S.L.; Hawley, C.; Cass, A.; Perkovic, V.; Zoungas, S. Glucose-lowering agents for treating pre-existing and new-onset diabetes in kidney transplant recipients. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef]
- Heerspink, H.J.L. Sodium glucose co-transporter 2 inhibition: A new avenue to protect the kidney. Nephrol. Dial. Transplant. 2019, 34, 2015–2017. [Google Scholar] [CrossRef]
- Musso, G.; Gambino, R.; Cassader, M.; Pagano, G. A novel approach to control hyperglycemia in type 2 diabetes: Sodium glucose co-transport (SGLT) inhibitors. Systematic review and meta-analysis of randomized trials. Ann. Med. 2011, 44, 375–393. [Google Scholar] [CrossRef]
- Clar, C.; Gill, J.A.; Court, R.; Waugh, N. Systematic review of SGLT2 receptor inhibitors in dual or triple therapy in type 2 diabetes. BMJ Open 2012, 2, e001007. [Google Scholar] [CrossRef]
- Daniele, G.; Solis-Herrera, C.; Dardano, A.; Mari, A.; Tura, A.; Giusti, L.; Kurumthodathu, J.J.; Campi, B.; Saba, A.; Bianchi, A.M.; et al. Increase in endogenous glucose production with SGLT2 inhibition is attenuated in individuals who underwent kidney transplantation and bilateral native nephrectomy. Diabetologia 2020, 63, 2423–2433. [Google Scholar] [CrossRef]
- Chao, E.C.; Henry, R.R. SGLT2 inhibition—A novel strategy for diabetes treatment. Nat. Rev. Drug Discov. 2010, 9, 551–559. [Google Scholar] [CrossRef]
- Nauck, M.A. Update on developments with SGLT2 inhibitors in the management of type 2 diabetes. Drug Des. Dev. Ther. 2014, 8, 1335–1380. [Google Scholar] [CrossRef] [Green Version]
- Anderson, S.; Cotiguala, L.; Tischer, S.; Park, J.M.; McMurry, K. Review of Newer Antidiabetic Agents for Diabetes Management in Kidney Transplant Recipients. Ann. Pharmacother. 2020, 1060028020951955. [Google Scholar] [CrossRef] [PubMed]
- Kanduri, S.R.; Kovvuru, K.; Hansrivijit, P.; Thongprayoon, C.; Vallabhajosyula, S.; Pivovarova, A.I.; Chewcharat, A.; Garla, V.V.; Medaura, J.; Cheungpasitporn, W. SGLT2 Inhibitors and Kidney Outcomes in Patients with Chronic Kidney Disease. J. Clin. Med. 2020, 9, 2723. [Google Scholar] [CrossRef] [PubMed]
- Song, C.C.; Brown, A.; Winstead, R.; Yakubu, I.; Demehin, M.; Kumar, D.; Gupta, G. Early initiation of sodium-glucose linked transporter inhibitors (SGLT-2i) and associated metabolic and electrolyte outcomes in diabetic kidney transplant recipients. Endocrinol. Diabetes Metab. 2020, e00185. [Google Scholar] [CrossRef]
- Zelniker, T.A.; Wiviott, S.D.; Raz, I.; Im, K.; Goodrich, E.L.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Furtado, R.H.M.; et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: A systematic review and meta-analysis of cardiovascular outcome trials. Lancet 2019, 393, 31–39. [Google Scholar] [CrossRef]
- Liu, X.-Y.; Zhang, N.; Chen, R.; Zhao, J.-G.; Yu, P. Efficacy and safety of sodium–glucose cotransporter 2 inhibitors in type 2 diabetes: A meta-analysis of randomized controlled trials for 1 to 2 years. J. Diabetes Complicat. 2015, 29, 1295–1303. [Google Scholar] [CrossRef] [PubMed]
- Vergara, A.; Jacobs-Cachá, C.; Soler, M.J. Sodium-glucose cotransporter inhibitors: Beyond glycaemic control. Clin. Kidney J. 2019, 12, 322–325. [Google Scholar] [CrossRef] [Green Version]
- Nadkarni, G.N.; Ferrandino, R.; Chang, A.; Surapaneni, A.; Chauhan, K.; Poojary, P.; Saha, A.; Ferket, B.; Grams, M.E.; Coca, S.G. Acute Kidney Injury in Patients on SGLT2 Inhibitors: A Propensity-Matched Analysis. Diabetes Care 2017, 40, 1479–1485. [Google Scholar] [CrossRef] [Green Version]
- Watts, N.B.; Bilezikian, J.P.; Usiskin, K.; Edwards, R.; Desai, M.; Law, G.; Meininger, G. Effects of Canagliflozin on Fracture Risk in Patients with Type 2 Diabetes Mellitus. J. Clin. Endocrinol. Metab. 2016, 101, 157–166. [Google Scholar] [CrossRef] [Green Version]
- Peters, A.; Buschur, E.O.; Buse, J.B.; Cohan, P.; Diner, J.C.; Hirsch, I.B. Euglycemic Diabetic Ketoacidosis: A Potential Complication of Treatment with Sodium–Glucose Cotransporter 2 Inhibition. Diabetes Care 2015, 38, 1687–1693. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.-Y.; Singh, S.; Mansour, O.; Baksh, S.; Alexander, G.C. Association Between Sodium-Glucose Cotransporter 2 Inhibitors and Lower Extremity Amputation Among Patients with Type 2 Diabetes. JAMA Intern. Med. 2018, 178, 1190–1198. [Google Scholar] [CrossRef] [Green Version]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; De Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Perkovic, V.; De Zeeuw, D.; Mahaffey, K.W.; Fulcher, G.; Erondu, N.; Shaw, W.; Barrett, T.D.; Weidner-Wells, M.; Deng, H.; Matthews, D.R.; et al. Canagliflozin and renal outcomes in type 2 diabetes: Results from the CANVAS Program randomised clinical trials. Lancet Diabetes Endocrinol. 2018, 6, 691–704. [Google Scholar] [CrossRef]
- Yale, J.; Bakris, G.; Cariou, B.; Nieto, J.; David-Neto, E.; Yue, D.; Wajs, E.; Figueroa, K.; Jiang, J.; Law, G.; et al. Efficacy and safety of canagliflozin over 52 weeks in patients with type 2 diabetes mellitus and chronic kidney disease. Diabetes Obes. Metab. 2014, 16, 1016–1027. [Google Scholar] [CrossRef] [PubMed]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohan, D.E.; Fioretto, P.; Tang, W.; List, J.F. Long-term study of patients with type 2 diabetes and moderate renal impairment shows that dapagliflozin reduces weight and blood pressure but does not improve glycemic control. Kidney Int. 2014, 85, 962–971. [Google Scholar] [CrossRef] [Green Version]
- Fioretto, P.; Del Prato, S.; Buse, J.B.; Goldenberg, R.; Giorgino, F.; Reyner, D.; Langkilde, A.M.; Sjöström, C.D.; Sartipy, P.; on behalf of the DERIVE Study Investigators. Efficacy and safety of dapagliflozin in patients with type 2 diabetes and moderate renal impairment (chronic kidney disease stage 3A): The DERIVE Study. Diabetes Obes. Metab. 2018, 20, 2532–2540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- Martinez, F.A.; Serenelli, M.; Nicolau, J.C.; Petrie, M.C.; Chiang, C.-E.; Tereshchenko, S.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; et al. Efficacy and Safety of Dapagliflozin in Heart Failure with Reduced Ejection Fraction According to Age. Circulation 2020, 141, 100–111. [Google Scholar] [CrossRef]
- Cherney, D.Z.I.; Dekkers, C.C.J.; Barbour, S.J.; Cattran, D.; Gafor, A.H.A.; Greasley, P.J.; Laverman, G.D.; Lim, S.K.; Di Tanna, G.L.; Reich, H.N.; et al. Effects of the SGLT2 inhibitor dapagliflozin on proteinuria in non-diabetic patients with chronic kidney disease (DIAMOND): A randomised, double-blind, crossover trial. Lancet Diabetes Endocrinol. 2020, 8, 582–593. [Google Scholar] [CrossRef]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.H.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [PubMed]
- Häring, H.-U.; Merker, L.; Seewaldt-Becker, E.; Weimer, M.; Meinicke, T.; Woerle, H.J.; Broedl, U.C.; on behalf of the EMPA-REG METSU Trial Investigators. Empagliflozin as Add-on to Metformin Plus Sulfonylurea in Patients with Type 2 Diabetes: A 24-week, randomized, double-blind, placebo-controlled trial. Diabetes Care 2013, 36, 3396–3404. [Google Scholar] [CrossRef] [Green Version]
- Barnett, A.H.; Mithal, A.; Manassie, J.; Jones, R.; Rattunde, H.; Woerle, H.J.; Broedl, U.C. Efficacy and safety of empagliflozin added to existing antidiabetes treatment in patients with type 2 diabetes and chronic kidney disease: A randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 2014, 2, 369–384. [Google Scholar] [CrossRef]
- Halden, T.A.S.; Kvitne, K.E.; Midtvedt, K.; Rajakumar, L.; Robertsen, I.; Brox, J.; Bollerslev, J.; Hartmann, A.; Åsberg, A.; Jenssen, T. Efficacy and Safety of Empagliflozin in Renal Transplant Recipients with Posttransplant Diabetes Mellitus. Diabetes Care 2019, 42, 1067–1074. [Google Scholar] [CrossRef]
- Allegretti, A.S.; Zhang, W.; Zhou, W.; Thurber, T.K.; Rigby, S.P.; Bowman-Stroud, C.; Trescoli, C.; Serusclat, P.; Freeman, M.W.; Halvorsen, Y.-D.C. Safety and Effectiveness of Bexagliflozin in Patients with Type 2 Diabetes Mellitus and Stage 3a/3b CKD. Am. J. Kidney Dis. 2019, 74, 328–337. [Google Scholar] [CrossRef]
- Wheeler, D.C.; Stefansson, B.V.; Batiushin, M.; Bilchenko, O.; Cherney, D.Z.I.; Chertow, G.M.; Douthat, W.; Dwyer, J.P.; Escudero, E.; Pecoits-Filho, R.; et al. The dapagliflozin and prevention of adverse outcomes in chronic kidney disease (DAPA-CKD) trial: Baseline characteristics. Nephrol. Dial. Transplant. 2020, 35, 1700–1711. [Google Scholar] [CrossRef]
- Lo, C.; Toyama, T.; Oshima, M.; Jun, M.; Chin, K.L.; Hawley, C.M.; Zoungas, S. Glucose-lowering agents for treating pre-existing and new-onset diabetes in kidney transplant recipients. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- National Heart Lung and Blood Institute. Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 14 December).
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Rajasekeran, H.; Kim, J.S.; Cardella, C.J.; Schiff, J.; Cattral, M.; Cherney, D.Z.; Singh, S.K. Use of Canagliflozin in Kidney Transplant Recipients for the Treatment of Type 2 Diabetes: A Case Series. Diabetes Care 2017, 40, e75–e76. [Google Scholar] [CrossRef] [Green Version]
- Schwaiger, E.; Burghart, L.; Signorini, L.; Ristl, R.; Kopecky, C.; Tura, A.; Pacini, G.; Wrba, T.; Antlanger, M.; Schmaldienst, S.; et al. Empagliflozin in posttransplantation diabetes mellitus: A prospective, interventional pilot study on glucose metabolism, fluid volume, and patient safety. Arab. Archaeol. Epigr. 2019, 19, 907–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkindi, F.; Al-Omary, H.L.; Hussain, Q.; Al Hakim, M.; Chaaban, A.; Boobes, Y. Outcomes of SGLT2 Inhibitors Use in Diabetic Renal Transplant Patients. Transplant. Proc. 2020, 52, 175–178. [Google Scholar] [CrossRef]
- Attallah, N.; Yassine, L. Use of Empagliflozin in Recipients of Kidney Transplant: A Report of 8 Cases. Transplant. Proc. 2019, 51, 3275–3280. [Google Scholar] [CrossRef] [PubMed]
- Mahling, M.; Schork, A.; Nadalin, S.; Fritsche, A.; Heyne, N.; Guthoff, M. Sodium-Glucose Cotransporter 2 (SGLT2) Inhibition in Kidney Transplant Recipients with Diabetes Mellitus. Kidney Blood Press. Res. 2019, 44, 984–992. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.; Virani, Z.; Rajput, P.; Shah, B. Efficacy and Safety of Canagliflozin in Kidney Transplant Patients. Indian J. Nephrol. 2019, 29, 278–281. [Google Scholar] [CrossRef] [PubMed]
- Kong, J.; Joon, J.; Chul, Y.; Eun, W.; Hyuk, K.; Hyun, S.S. SP770SODIUM/GLUCOSE COTRANSPORTER 2 INHIBOTOR FOR THE TREATMENT OF DIABETES IN KIDNEY TRANSPLANT PATIENTS. Nephrol. Dial. Transplant. 2019, 34. [Google Scholar] [CrossRef]
- Toyama, T.; Neuen, B.L.; Jun, M.; Ohkuma, T.; Neal, B.; Jardine, M.J.; Heerspink, H.L.; Wong, M.G.; Ninomiya, T.; Wada, T.; et al. Effect of SGLT2 inhibitors on cardiovascular, renal and safety outcomes in patients with type 2 diabetes mellitus and chronic kidney disease: A systematic review and meta-analysis. Diabetes Obes. Metab. 2019, 21, 1237–1250. [Google Scholar] [CrossRef] [Green Version]
- Foote, C.; Perkovic, V.; Neal, B. Effects of SGLT2 inhibitors on cardiovascular outcomes. Diabetes Vasc. Dis. Res. 2012, 9, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Ceriello, A.; Ofstad, A.P.; Zwiener, I.; Kaspers, S.; George, J.; Nicolucci, A. Empagliflozin reduced long-term HbA1c variability and cardiovascular death: Insights from the EMPA-REG OUTCOME trial. Cardiovasc. Diabetol. 2020, 19, 176. [Google Scholar] [CrossRef]
- Sahebkar, A.; Atkin, S.L.; Sahebkar, A. Mechanistic effects of SGLT2 inhibition on blood pressure in diabetes. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 1679–1683. [Google Scholar] [CrossRef]
- Weir, M.R.; Burgess, E.D.; Cooper, J.E.; Fenves, A.Z.; Goldsmith, D.; McKay, D.; Mehrotra, A.; Mitsnefes, M.M.; Sica, D.A.; Taler, S.J. Assessment and Management of Hypertension in Transplant Patients. J. Am. Soc. Nephrol. 2015, 26, 1248–1260. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Perco, P.; Mulder, S.; Leierer, J.; Hansen, M.K.; Heinzel, A.; Mayer, G. Canagliflozin reduces inflammation and fibrosis biomarkers: A potential mechanism of action for beneficial effects of SGLT2 inhibitors in diabetic kidney disease. Diabetologia 2019, 62, 1154–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hattori, S. Anti-inflammatory effects of empagliflozin in patients with type 2 diabetes and insulin resistance. Diabetol. Metab. Syndr. 2018, 10, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahebkar, A.; Simental-Mendía, L.E.; Banach, M.; Bo, S.; Sahebkar, A. The major molecular mechanisms mediating the renoprotective effects of SGLT2 inhibitors: An update. Biomed. Pharmacother. 2019, 120, 109526. [Google Scholar] [CrossRef]
- Packer, M. SGLT2 Inhibitors Produce Cardiorenal Benefits by Promoting Adaptive Cellular Reprogramming to Induce a State of Fasting Mimicry: A Paradigm Shift in Understanding Their Mechanism of Action. Diabetes Care 2020, 43, 508–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iannantuoni, F.; De Marañon, A.M.; Diaz-Morales, N.; Falcon, R.; Bañuls, C.; Abad-Jiménez, Z.; Victor, V.M.; Hernández-Mijares, A.; Rovira-Llopis, S. The SGLT2 Inhibitor Empagliflozin Ameliorates the Inflammatory Profile in Type 2 Diabetic Patients and Promotes an Antioxidant Response in Leukocytes. J. Clin. Med. 2019, 8, 1814. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.; Dong, Y.; Liu, Y.; Li, Y.; Sun, Y.; Wang, J.; Wang, S. The prevalence and predictive factors of urinary tract infection in patients undergoing renal transplantation: A meta-analysis. Am. J. Infect. Control. 2016, 44, 1261–1268. [Google Scholar] [CrossRef]
- Liu, J.; Li, L.; Li, S.; Jia, P.; Deng, K.; Chen, W.; Sun, X. Effects of SGLT2 inhibitors on UTIs and genital infections in type 2 diabetes mellitus: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 1–11. [Google Scholar] [CrossRef]
- Lee, P.C.; Ganguly, S.; Goh, S.-Y. Weight loss associated with sodium-glucose cotransporter-2 inhibition: A review of evidence and underlying mechanisms. Obes. Rev. 2018, 19, 1630–1641. [Google Scholar] [CrossRef]
- Nespoux, J.; Vallon, V. SGLT2 inhibition and kidney protection. Clin. Sci. 2018, 132, 1329–1339. [Google Scholar] [CrossRef]
- Phadke, G.; Kaushal, A.; Tolan, D.R.; Hahn, K.; Jensen, T.; Bjornstad, P.; Roncal-Jimenez, C.; Hernando, A.A.; Lanaspa, M.A.; Alexander, M.P.; et al. Osmotic Nephrosis and Acute Kidney Injury Associated with SGLT2 Inhibitor Use: A Case Report. Am. J. Kidney Dis. 2020, 76, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Menne, J.; Dumann, E.; Haller, H.; Schmidt, B.M.W. Acute kidney injury and adverse renal events in patients receiving SGLT2-inhibitors: A systematic review and meta-analysis. PLoS Med. 2019, 16, e1002983. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Country | Treatment Medication | Number of Participants Treated with SGLT-2 Inhibitors | Mean Age (Years) | %Male | %DM Prior to KT | F/U (Months) | GFR Baseline (mL/min/1.73 m2) | HbA1C | Transplant Duration (Years) | Quality Assessment |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Rajasekeran 2017 [50] | Canada | Canagliflozin | 10 | 56.7 ± 12.4 | 70% | 80% | 8 | 70.8 ± 18.3 | 8.1 ± 1.4 | 4.0 ± 3.4 | good |
| Schwaiger 2018 [51] | Austria | Empagliflozin | 8 | 56.5 ± 7.9 | 50% | 0% | 12 | 54.0 ± 23.8 | 6.7 ± 0.7 | 5.8 ± 4.8 | good |
| Alkindi 2019 [52] | UAE | Empagliflozin or Dapagliflozin | 8 | 56.8 ± 13.7 | 75% | 25% | 24 | 75.8 ± 13.4 | 9.3 ± 1.4 | 9.6 ± 6.4 | good |
| Attallah 2019 [53] | UAE | Empagliflozin | 8 | 45.9 ± 6.6 | 50% | 50% | 12 | NR | 8.1 ± 0.2 | 19.9 ± 6.0 | good |
| Halden 2019 [43] | Norway | Empagliflozin | 22 | 63 | 77% | 0% | 6 | 66 ± 10.5 | 6.9 ± 0.4 | 3 | good |
| Placebo | 22 (control) | 59 | 77% | 0% | 6 | 59 ± 9.5 | 6.8 ± 0.3 | 3 | |||
| Kong 2019 [56] | South Korea | Dapagliflozin | 42 | NR | NR | NR | 12 | 60.3 ± 17 | 7.5 ± 1.1 | NR | fair |
| Mahling 2019 [54] | Germany | Empagliflozin | 10 | 66.0 ± 12.6 | 80% | 30% | 12 | 57 ± 19.3 | 7.3 ± 1.0 | 5.9 ± 3.3 | good |
| Shah 2019 [55] | India | Canagliflozin | 24 | 53.8 ± 7.1 | 96% | 83% | 6 | 86 ± 20 | 8.5 ± 1.5 | 2.7 | good |
| Parameters | Number of Study | Sample Size | WMD | 95% CI | p-Value | I2 |
|---|---|---|---|---|---|---|
| eGFR | 7 | 124 | −2.51 mL/min/1.73 m2 | (−5.03, 0.02) | 0.06 | 0 |
| Serum creatinine | 5 | 58 | −0.05 mg/dL | (−0.13, 0.03) | 0.21 | 0 |
| Urine protein-creatinine ratio | 3 | 38 | −211 mg/g | (−655, 232) | 0.35 | 93.2 |
| HbA1C | 8 | 132 | −0.57% | (−0.97, −0.16) | 0.006 | 85.2 |
| SBP | 6 | 82 | −3.24 mmHg | (−7.92, 1.45) | 0.18 | 21.3 |
| DBP | 6 | 82 | −1.49 mmHg | (−3.81, 0.83) | 0.21 | 0 |
| BMI | 3 | 38 | −1.20 kg/m2 | (−2.67, 0.27) | 0.11 | 21.4 |
| Weight | 8 | 132 | −2.15 kg | (−3.07, −1.23) | <0.001 | 0 |
| Parameters | Number of Study | Sample Size | WMD | 95% CI | p-Value | I2 |
|---|---|---|---|---|---|---|
| At 6 months | ||||||
| eGFR | 5 | 72 | −2.38 mL/min/1.73 m2 | (−5.13, 0.37) | 0.09 | 0 |
| Serum creatinine | NA | |||||
| Urine protein-creatinine ratio | 3 | 38 | −211 mg/g | (−655, 232) | 0.35 | 93.2 |
| HbA1C | 5 | 72 | −0.22% | (−0.62, 0.18) | 0.28 | 41.6 |
| SBP | 4 | 62 | −6.38 mmHg | (−15.54, 2.80) | 0.17 | 64.3 |
| DBP | 4 | 62 | −2.54 mmHg | (−6.67, 1.59) | 0.23 | 47.2 |
| BMI | 3 | 38 | −0.80 kg/m2 | (−1.38, −0.22) | 0.007 | 0 |
| Weight | 2 | 46 | −2.49 kg | (−4.15, −0.84) | 0.003 | 0 |
| At 12 months | ||||||
| eGFR | 4 | 68 | −0.35 mL/min/1.73 m2 | (−5.66, 4.97) | 0.90 | 0 |
| Serum creatinine | 3 | 24 | −0.05 | (−0.15, 0.05) | 0.32 | 0 |
| Urine protein-creatinine ratio | NA | |||||
| HbA1C | 5 | 76 | −0.58% | (−1.12, −0.05) | 0.03 | 79.8 |
| SBP | 3 | 26 | −7.25 mmHg | (−16.04, 1.54) | 0.11 | 0 |
| DBP | 3 | 26 | −5.24 mmHg | (−11.19, 0.72) | 0.09 | 0 |
| BMI | 2 | 16 | −2.70 kg/m2 | (−6.03, 0.61) | 0.11 | 16.1 |
| Weight | 5 | 76 | −1.97 kg | (−3.21, −0.73) | 0.002 | 0 |
| Empagliflozin | ||||||
| eGFR | 3 | 40 | 0.31 mL/min/1.73 m2 | (−8.27, 8.88) | 0.94 | 37.5 |
| Serum creatinine | 2 | 16 | 0.02 | (−0.13, 0.16) | 0.84 | 0 |
| Urine protein-creatinine ratio | 3 | 38 | −211 mg/g | (−655, 232) | 0.35 | 93.2 |
| HbA1C | 4 | 48 | −0.31% | (−0.91, 0.28) | 0.30 | 92.9 |
| SBP | 3 | 40 | 1.55 mmHg | (−3.05, 6.15) | 0.51 | 0 |
| DBP | 3 | 40 | −1.14 mmHg | (−5.37, 3.09) | 0.60 | 15.8 |
| BMI | 2 | 30 | −0.82 kg/m2 | (−1.41, −0.24) | 0.006 | 0 |
| Weight | 4 | 48 | −2.17 kg | (−3.20, −1.15) | <0.001 | 0 |
| Canagliflozin | ||||||
| eGFR | 2 | 34 | −3.65 mL/min/1.73 m2 | (−11.24, 3.93) | 0.35 | 0 |
| Serum creatinine | 2 | 34 | −0.04 | (−0.16, 0.07) | 0.48 | 0 |
| Urine protein-creatinine ratio | NA | |||||
| HbA1C | 2 | 34 | −0.87% | (−1.46, −0.27) | 0.004 | 0 |
| SBP | 2 | 34 | −7.15 mmHg | (−14.27, −0.03) | 0.04 | 0 |
| DBP | 2 | 34 | −2.49 mmHg | (−6.87, 1.89) | 0.27 | 0 |
| BMI | NA | |||||
| Weight | 2 | 34 | −2.14 kg | (−4.43, 0.16) | 0.07 | 0 |
| Authors | Urinary Infection | Genital Mycosis | Euglycemic Ketoacidosis | Acute Kidney Injury | Acute Rejection | Ulcer | Cellulitis |
|---|---|---|---|---|---|---|---|
| Rajasekeran 2017 | 0 | 0 | NR | 0 | 0 | NR | 1 |
| Schwaiger 2018 | 3 | 0 | 0 | NR | 0 | NR | NR |
| Alkindi 2019 | 1 | 0 | 0 | 0 | 0 | NR | NR |
| Attallah 2019 | 2 | NR | 0 | 0 | 0 | NR | NR |
| Halden 2019 | 3 | 1 | NR | NR | 0 | NR | NR |
| Kong 2019 | 3 | NR | NR | NR | NR | NR | NR |
| Mahling 2019 | 2 | NR | 0 | 1 | NR | 1 | NR |
| Shah 2019 | 0 | 0 | NR | NR | NR | NR | NR |
| %incidence proportion | 43.8% | 1.4% | 0% | 3.6% | 0% | 10% | 10% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chewcharat, A.; Prasitlumkum, N.; Thongprayoon, C.; Bathini, T.; Medaura, J.; Vallabhajosyula, S.; Cheungpasitporn, W. Efficacy and Safety of SGLT-2 Inhibitors for Treatment of Diabetes Mellitus among Kidney Transplant Patients: A Systematic Review and Meta-Analysis. Med. Sci. 2020, 8, 47. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci8040047
Chewcharat A, Prasitlumkum N, Thongprayoon C, Bathini T, Medaura J, Vallabhajosyula S, Cheungpasitporn W. Efficacy and Safety of SGLT-2 Inhibitors for Treatment of Diabetes Mellitus among Kidney Transplant Patients: A Systematic Review and Meta-Analysis. Medical Sciences. 2020; 8(4):47. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci8040047
Chicago/Turabian StyleChewcharat, Api, Narut Prasitlumkum, Charat Thongprayoon, Tarun Bathini, Juan Medaura, Saraschandra Vallabhajosyula, and Wisit Cheungpasitporn. 2020. "Efficacy and Safety of SGLT-2 Inhibitors for Treatment of Diabetes Mellitus among Kidney Transplant Patients: A Systematic Review and Meta-Analysis" Medical Sciences 8, no. 4: 47. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci8040047