
Targeted Plasma Metabolic Profiles and Risk of Recurrence in Stage II and III Colorectal Cancer Patients: Results from an International Cohort Consortium

 , , , , , , , , , , , and add
Show full author list
, , , , , , , , , , , and add
Show full author list
Abstract
:1. Introduction
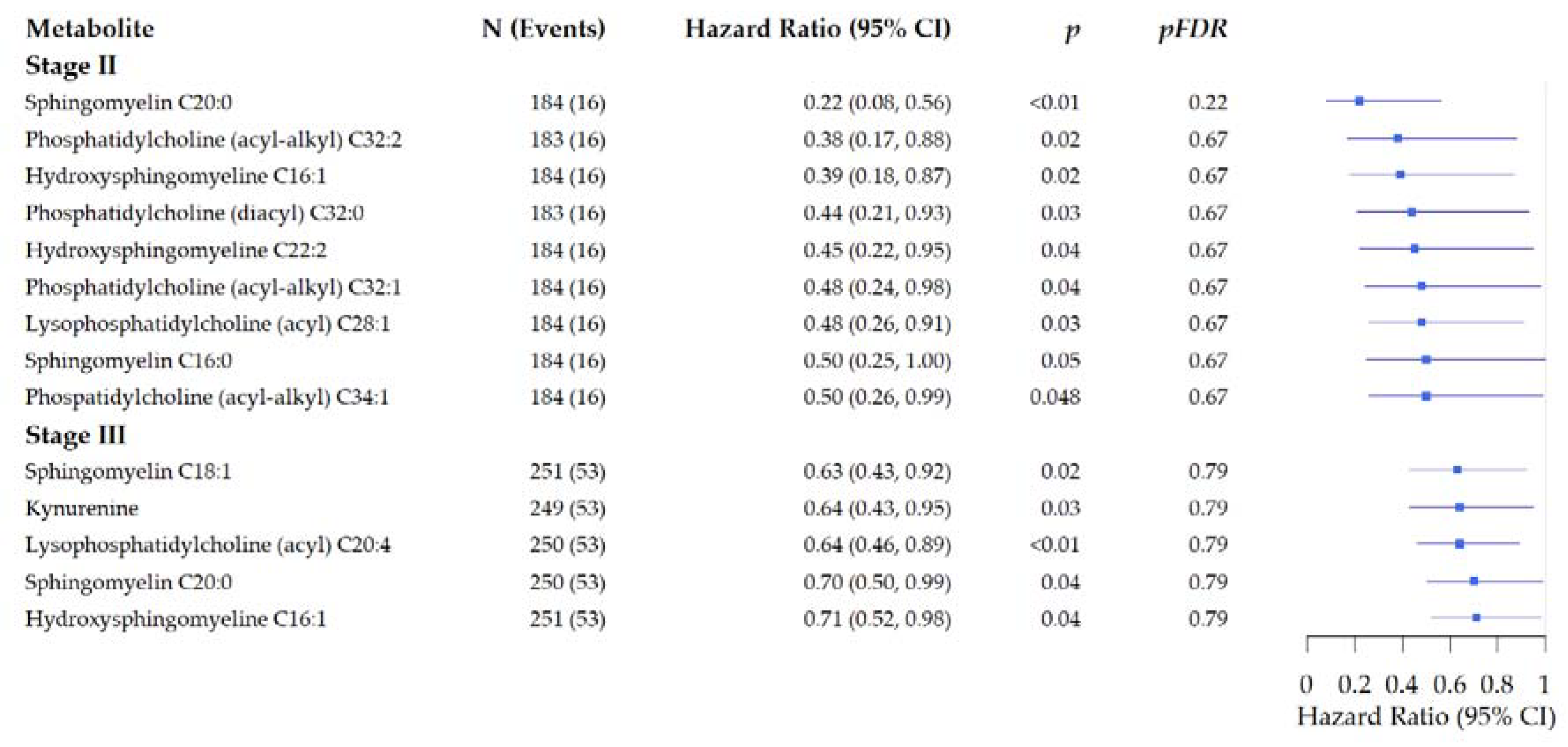
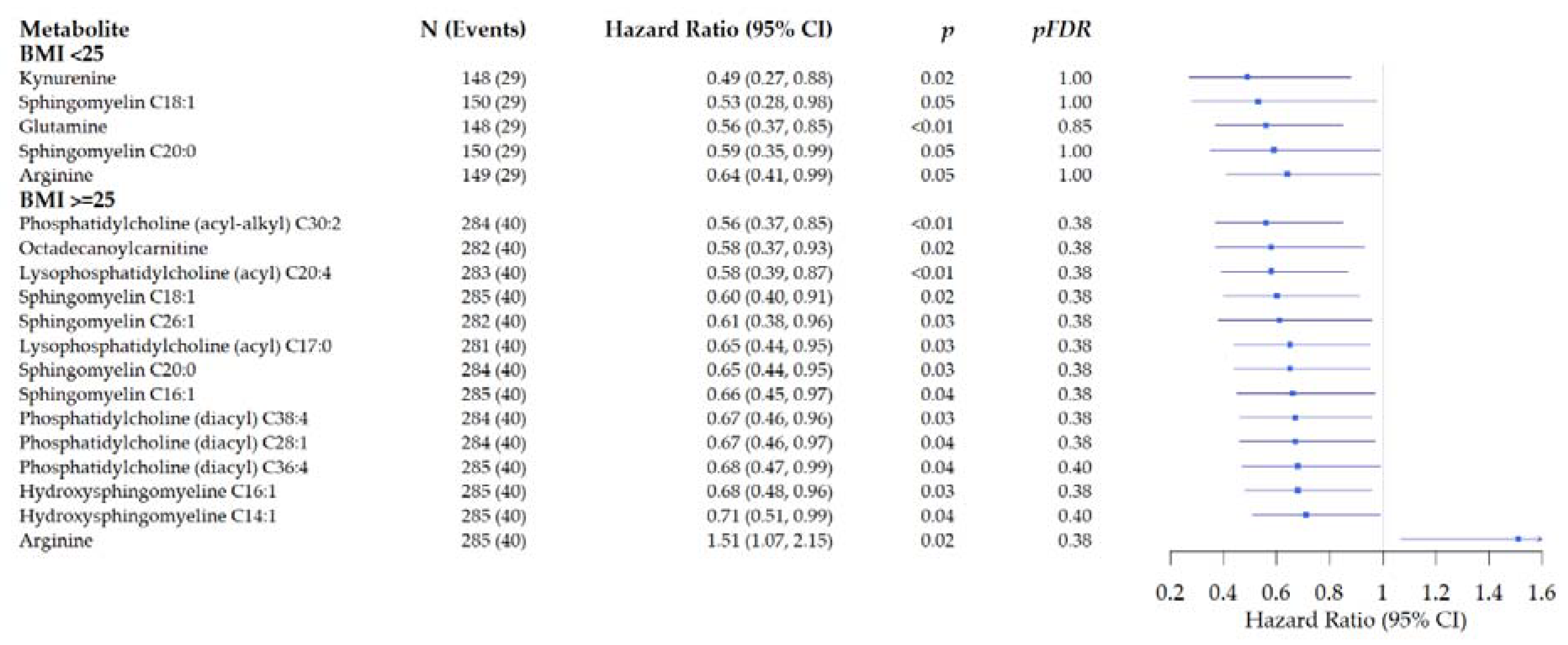
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Design and Populations
4.2. Data Collection
4.3. Biomarker Analysis
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Cancer Society. Cancer Facts & Figures; American Cancer Society: Atlanta, GA, USA, 2005. [Google Scholar]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Rabeneck, L.; Horton, S.; Zauber, A.G.; Earle, C. Colorectal Cancer. In Cancer: Disease Control Priorities, 3rd ed.; Gelband, H., Jha, P., Sankaranarayanan, R., Horton, S., Eds.; The World Bank: Washington, WA, USA, 2015; Volume 3. [Google Scholar] [CrossRef]
- Grothey, A.; Sobrero, A.F.; Shields, A.F.; Yoshino, T.; Paul, J.; Taieb, J.; Souglakos, J.; Shi, Q.; Kerr, R.; Labianca, R.; et al. Duration of Adjuvant Chemotherapy for Stage III Colon Cancer. N. Engl. J. Med. 2018, 378, 1177–1188. [Google Scholar] [CrossRef]
- O’Connell, M.J.; Campbell, M.E.; Goldberg, R.M.; Grothey, A.; Seitz, J.F.; Benedetti, J.K.; Andre, T.; Haller, D.G.; Sargent, D.J. Survival following recurrence in stage II and III colon cancer: Findings from the ACCENT data set. J. Clin. Oncol. 2008, 26, 2336–2341. [Google Scholar] [CrossRef]
- Zafar, S.N.; Hu, C.Y.; Snyder, R.A.; Cuddy, A.; You, Y.N.; Lowenstein, L.M.; Volk, R.J.; Chang, G.J. Predicting Risk of Recurrence After Colorectal Cancer Surgery in the United States: An Analysis of a Special Commission on Cancer National Study. Ann. Surg. Oncol. 2020, 27, 2740–2749. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin 2019, 69, 363–385. [Google Scholar] [CrossRef] [Green Version]
- Chien, C.; Morimoto, L.M.; Tom, J.; Li, C.I. Differences in colorectal carcinoma stage and survival by race and ethnicity. Cancer 2005, 104, 629–639. [Google Scholar] [CrossRef] [PubMed]
- Playdon, M.C.; Ziegler, R.G.; Sampson, J.N.; Stolzenberg-Solomon, R.; Thompson, H.J.; Irwin, M.L.; Mayne, S.T.; Hoover, R.N.; Moore, S.C. Nutritional metabolomics and breast cancer risk in a prospective study. Am. J. Clin. Nutr. 2017, 106, 637–649. [Google Scholar] [CrossRef] [PubMed]
- Playdon, M.C.; Moore, S.C.; Derkach, A.; Reedy, J.; Subar, A.F.; Sampson, J.N.; Albanes, D.; Gu, F.; Kontto, J.; Lassale, C.; et al. Identifying biomarkers of dietary patterns by using metabolomics. Am. J. Clin. Nutr. 2017, 105, 450–465. [Google Scholar] [CrossRef] [Green Version]
- Geijsen, A.; Brezina, S.; Keski-Rahkonen, P.; Baierl, A.; Bachleitner-Hofmann, T.; Bergmann, M.M.; Boehm, J.; Brenner, H.; Chang-Claude, J.; van Duijnhoven, F.J.B.; et al. Plasma metabolites associated with colorectal cancer: A discovery-replication strategy. Int. J. Cancer 2019, 145, 1221–1231. [Google Scholar] [CrossRef] [Green Version]
- Delphan, M.; Lin, T.; Liesenfeld, D.B.; Nattenmuller, J.; Bohm, J.T.; Gigic, B.; Habermann, N.; Zielske, L.; Schrotz-King, P.; Schneider, M.; et al. Associations of branched-chain amino acids with parameters of energy balance and survival in colorectal cancer patients: Results from the ColoCare Study. Metab. Off. J. Metab. Soc. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Erben, V.; Bhardwaj, M.; Schrotz-King, P.; Brenner, H. Metabolomics Biomarkers for Detection of Colorectal Neoplasms: A Systematic Review. Cancers 2018, 10, 246. [Google Scholar] [CrossRef] [Green Version]
- Adamski, J. Metabolomics for Biomedical Research; Elsevier: Walthum, MA, USA, 2020. [Google Scholar]
- Geijsen, A.; van Roekel, E.H.; van Duijnhoven, F.J.B.; Achaintre, D.; Bachleitner-Hofmann, T.; Baierl, A.; Bergmann, M.M.; Boehm, J.; Bours, M.J.L.; Brenner, H.; et al. Plasma metabolites associated with colorectal cancer stage: Findings from an international consortium. Int. J. Cancer 2020, 146, 3256–3266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolce, V.; Cappello, A.R.; Lappano, R.; Maggiolini, M. Glycerophospholipid synthesis as a novel drug target against cancer. Curr. Mol. Pharm. 2011, 4, 167–175. [Google Scholar] [CrossRef]
- Kurabe, N.; Hayasaka, T.; Ogawa, M.; Masaki, N.; Ide, Y.; Waki, M.; Nakamura, T.; Kurachi, K.; Kahyo, T.; Shinmura, K.; et al. Accumulated phosphatidylcholine (16:0/16:1) in human colorectal cancer; possible involvement of LPCAT4. Cancer Sci. 2013, 104, 1295–1302. [Google Scholar] [CrossRef]
- Halama, A.; Guerrouahen, B.S.; Pasquier, J.; Satheesh, N.J.; Suhre, K.; Rafii, A. Nesting of colon and ovarian cancer cells in the endothelial niche is associated with alterations in glycan and lipid metabolism. Sci. Rep. 2017, 7, 39999. [Google Scholar] [CrossRef] [Green Version]
- Ose, J.; Holowatyj, A.N.; Nattenmüller, J.; Gigic, B.; Lin, T.; Himbert, C.; Habermann, N.; Achaintre, D.; Scalbert, A.; Keski-Rahkonen, P.; et al. Metabolomics profiling of visceral and abdominal subcutaneous adipose tissue in colorectal cancer patients: Results from the ColoCare study. Cancer Causes Control 2020, 31, 723–735. [Google Scholar] [CrossRef]
- Siskos, A.P.; Jain, P.; Romisch-Margl, W.; Bennett, M.; Achaintre, D.; Asad, Y.; Marney, L.; Richardson, L.; Koulman, A.; Griffin, J.L.; et al. Interlaboratory Reproducibility of a Targeted Metabolomics Platform for Analysis of Human Serum and Plasma. Anal. Chem. 2017, 89, 656–665. [Google Scholar] [CrossRef]
- Carayol, M.; Licaj, I.; Achaintre, D.; Sacerdote, C.; Vineis, P.; Key, T.J.; Onland Moret, N.C.; Scalbert, A.; Rinaldi, S.; Ferrari, P. Reliability of Serum Metabolites over a Two-Year Period: A Targeted Metabolomic Approach in Fasting and Non-Fasting Samples from EPIC. PLoS ONE 2015, 10, e0135437. [Google Scholar] [CrossRef] [Green Version]
- Breier, M.; Wahl, S.; Prehn, C.; Fugmann, M.; Ferrari, U.; Weise, M.; Banning, F.; Seissler, J.; Grallert, H.; Adamski, J.; et al. Targeted metabolomics identifies reliable and stable metabolites in human serum and plasma samples. PLoS ONE 2014, 9, e89728. [Google Scholar] [CrossRef]
- Sampson, J.N.; Boca, S.M.; Shu, X.O.; Stolzenberg-Solomon, R.Z.; Matthews, C.E.; Hsing, A.W.; Tan, Y.T.; Ji, B.T.; Chow, W.H.; Cai, Q.; et al. Metabolomics in epidemiology: Sources of variability in metabolite measurements and implications. Cancer Epidemiol. Biomark. Prev. 2013, 22, 631–640. [Google Scholar] [CrossRef] [Green Version]
- Winkels, R.M.; Heine-Broring, R.C.; van Zutphen, M.; van Harten-Gerritsen, S.; Kok, D.E.; van Duijnhoven, F.J.; Kampman, E. The COLON study: Colorectal cancer: Longitudinal, Observational study on Nutritional and lifestyle factors that may influence colorectal tumour recurrence, survival and quality of life. BMC Cancer 2014, 14, 374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Roekel, E.H.; Bours, M.J.; de Brouwer, C.P.; Ten Napel, H.; Sanduleanu, S.; Beets, G.L.; Kant, I.J.; Weijenberg, M.P. The applicability of the international classification of functioning, disability, and health to study lifestyle and quality of life of colorectal cancer survivors. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1394–1405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulrich, C.M.; Gigic, B.; Böhm, J.; Ose, J.; Viskochil, R.; Schneider, M.; Colditz, G.A.; Figueiredo, J.C.; Grady, W.M.; Li, C.I.; et al. The ColoCare Study: A Paradigm of Transdisciplinary Science in Colorectal Cancer Outcomes. Cancer Epidemiol. Biomark. Prev. 2019, 28, 591–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours; John Wiley & Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Van Roekel, E.H.; Trijsburg, L.; Assi, N.; Carayol, M.; Achaintre, D.; Murphy, N.; Rinaldi, S.; Schmidt, J.A.; Stepien, M.; Kaaks, R. Circulating metabolites associated with alcohol intake in the european prospective investigation into cancer and nutrition cohort. Nutrients 2018, 10, 654. [Google Scholar] [CrossRef] [Green Version]
- Di Guida, R.; Engel, J.; Allwood, J.W.; Weber, R.J.; Jones, M.R.; Sommer, U.; Viant, M.R.; Dunn, W.B. Non-targeted UHPLC-MS metabolomic data processing methods: A comparative investigation of normalisation, missing value imputation, transformation and scaling. Metab. Off. J. Metab. Soc. 2016, 12, 93. [Google Scholar] [CrossRef] [Green Version]
- Rosner, B. Percentage points for a generalized esd many-outlier procedure. Technometrics 1983, 25, 165–172. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Chong, J.; Wishart, D.S.; Xia, J. Using MetaboAnalyst 4.0 for Comprehensive and Integrative Metabolomics Data Analysis. Curr. Protoc. Bioinform. 2019, 68, e86. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| COHORTS | |||||
|---|---|---|---|---|---|
| Participant Characteristics- | Total Population | COLON | EnCoRe | CORSA | ColoCare |
| Number of participants | 440 | 135 | 137 | 26 | 142 |
| Sex, n (%) | |||||
| Male | 282 (64%) | 76 (56%) | 86 (63%) | 22 (84%) | 98 (69%) |
| Female | 158 (36%) | 59 (44%) | 51 (37%) | 4 (16%) | 44 (31%) |
| Age at diagnosis, years (median, range) | 66.0 (27.0–88.0) | 66.0 (31.0–84.0) | 67.0 (36.0–87.0) | 69.5 (39.0–88.0) | 64.0 (27.0–86.0) |
| Body mass index * | |||||
| Continuous, kg/m2 (median, range) | 26.3 (17.2–46.0) | 25.4 (17.2–40.2) | 27.2 (19.0–46.0) | 26.4 (21.0–35.9) | 26.2 (17.8–39.7) |
| Underweight, <18.5, n (%) | 5 (1%) | 3 (2%) | 2 (1%) | ||
| Normal weight, 18.5–24.9, n (%) | 143 (33%) | 57 (44%) | 36(26%) | 6 (26%) | 44 (31%) |
| Overweight, 25–29.9, n (%) | 192 (45%) | 52 (40%) | 58 (43%) | 13 (57%) | 69 (49%) |
| Obese, ≥30, n (%) | 92 (21%) | 19 (14%) | 42 (31%) | 5 (17%) | 26 (19%) |
| Tumor stage, n (%) | |||||
| II | 187 (43%) | 66 (49%) | 45 (33%) | 13 (50%) | 63 (44%) |
| III | 253 (57%) | 69 (51%) | 92 (67%) | 13 (50%) | 79 (56%) |
| Tumor location 1, n (%) | |||||
| Colon cancer | 248 (57%) | 86 (64%) | 81 (59%) | 17 (71%) | 64 (45%) |
| Distal colon | 129 (30%) | 44 (33%) | 39 (28%) | 10 (42%) | 36 (25%) |
| Proximal colon | 119 (27%) | 42 (31%) | 42 (31%) | 7 (29%) | 28 (20%) |
| Rectal cancer | 190 (43%) | 49 (36%) | 56 (41%) | 7 (29%) | 78 (55%) |
| Neo-adjuvant treatment, n (%) | |||||
| Yes | 306 (70%) | 91 (67%) | 90 (66%) | 25 (96%) | 100 (70%) |
| No | 134 (30%) | 44 (33%) | 47 (34%) | 1 (4%) | 42 (30%) |
| Adjuvant treatment, n (%) | |||||
| Yes | 183 (42%) | 42 (32%) | 64 (47%) | 12 (46%) | 65 (47%) |
| No | 249 (58%) | 90 (68%) | 73 (53%) | 14 (54%) | 72 (53%) |
| Follow-up time (months), median, range) | |||||
| Patients with recurrence | 19.9 (3.6–81.0) | 27.1 (7.0–81.0) | 15.0 (3.7–45.1) | 46.7 (39.0–65.8) | 15.7 (3.6–45.6) |
| Patients without recurrence | 42.2 (3.6–88.8) | 71.2 (9.3–88.8) | 41.9 (4.1–69.1) | 44.9 (3.6–70.1) | 31.5 (3.6–65.8) |
| Recurrence 2, n (%) | |||||
| Yes | 69 (15%) | 20 (15%) | 23 (17%) | 6 (23%) | 20 (14%) |
| Early Recurrence 3 | 44 (64%) | 8 (40%) | 18 (78%) | 18 (90%) | |
| Late Recurrence 4 | 25 (36%) | 12 (60%) | 5 (22%) | 6 (100%) | 2 (10%) |
| No | 371 (85%) | 115 (85%) | 114 (83%) | 20 (77%) | 122 (86%) |
| Participant Characteristics- | Patients without Recurrence | Patients with Recurrence |
|---|---|---|
| Number of participants | 371 | 69 |
| Sex, n (%) | ||
| Female | 137 (37%) | 21 (30%) |
| Male | 234 (63%) | 48 (70%) |
| Age at diagnosis, years (median, range) | 67.0 (27–88) | 63.0 (38–87) |
| Tumor stage, n (%) | ||
| II | 171 (46%) | 16 (23%) |
| III | 200 (54%) | 53 (77%) |
| Tumor location, n (%) | ||
| Colon | 213 (58%) | 45 (51%) |
| Distal colon | 104 (28%) | 15 (21%) |
| Proximal colon | 109 (30%) | 30 (29%) |
| Rectal | 156 (42%) | 34 (49%) |
| Neo-adjuvant treatment, n (%) | ||
| Yes | 110 (30%) | 24 (35%) |
| No | 261 (70%) | 45 (65%) |
| Adjuvant treatment, n (%) | ||
| Yes | 147 (40%) | 36 (54%) |
| No | 218 (60%) | 31 (46%) |
| Metabolite | N Patients 1 (N Events 2) | HR (95% Confidence Interval) | p | pFDR |
|---|---|---|---|---|
| Lysophosphatidylcholine (acyl) C20:4 | 438 (44) | 0.67 (0.47, 0.96) | 0.03 | 0.76 |
| Hydroxysphingomyeline C16:1 | 438 (44) | 0.69 (0.48, 0.99) | <0.01 | 0.76 |
| Sphingomyeline C18:1 | 438 (44) | 0.56 (0.36, 0.85) | <0.01 | 0.76 |
| Sphingomyeline C20:2 | 438 (44) | 0.67 (0.46, 0.97) | 0.03 | 0.76 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ose, J.; Gigic, B.; Brezina, S.; Lin, T.; Baierl, A.; Geijsen, A.J.M.R.; van Roekel, E.; Robinot, N.; Gicquiau, A.; Achaintre, D.; et al. Targeted Plasma Metabolic Profiles and Risk of Recurrence in Stage II and III Colorectal Cancer Patients: Results from an International Cohort Consortium. Metabolites 2021, 11, 129. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11030129
Ose J, Gigic B, Brezina S, Lin T, Baierl A, Geijsen AJMR, van Roekel E, Robinot N, Gicquiau A, Achaintre D, et al. Targeted Plasma Metabolic Profiles and Risk of Recurrence in Stage II and III Colorectal Cancer Patients: Results from an International Cohort Consortium. Metabolites. 2021; 11(3):129. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11030129
Chicago/Turabian StyleOse, Jennifer, Biljana Gigic, Stefanie Brezina, Tengda Lin, Andreas Baierl, Anne J. M. R. Geijsen, Eline van Roekel, Nivonirina Robinot, Audrey Gicquiau, David Achaintre, and et al. 2021. "Targeted Plasma Metabolic Profiles and Risk of Recurrence in Stage II and III Colorectal Cancer Patients: Results from an International Cohort Consortium" Metabolites 11, no. 3: 129. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11030129