
Alterations of Selected Hemorheological and Metabolic Parameters Induced by Physical Activity in Untrained Men and Sportsmen


 and
and
Abstract
:1. Introduction
2. Results
2.1. Hematological Parameters
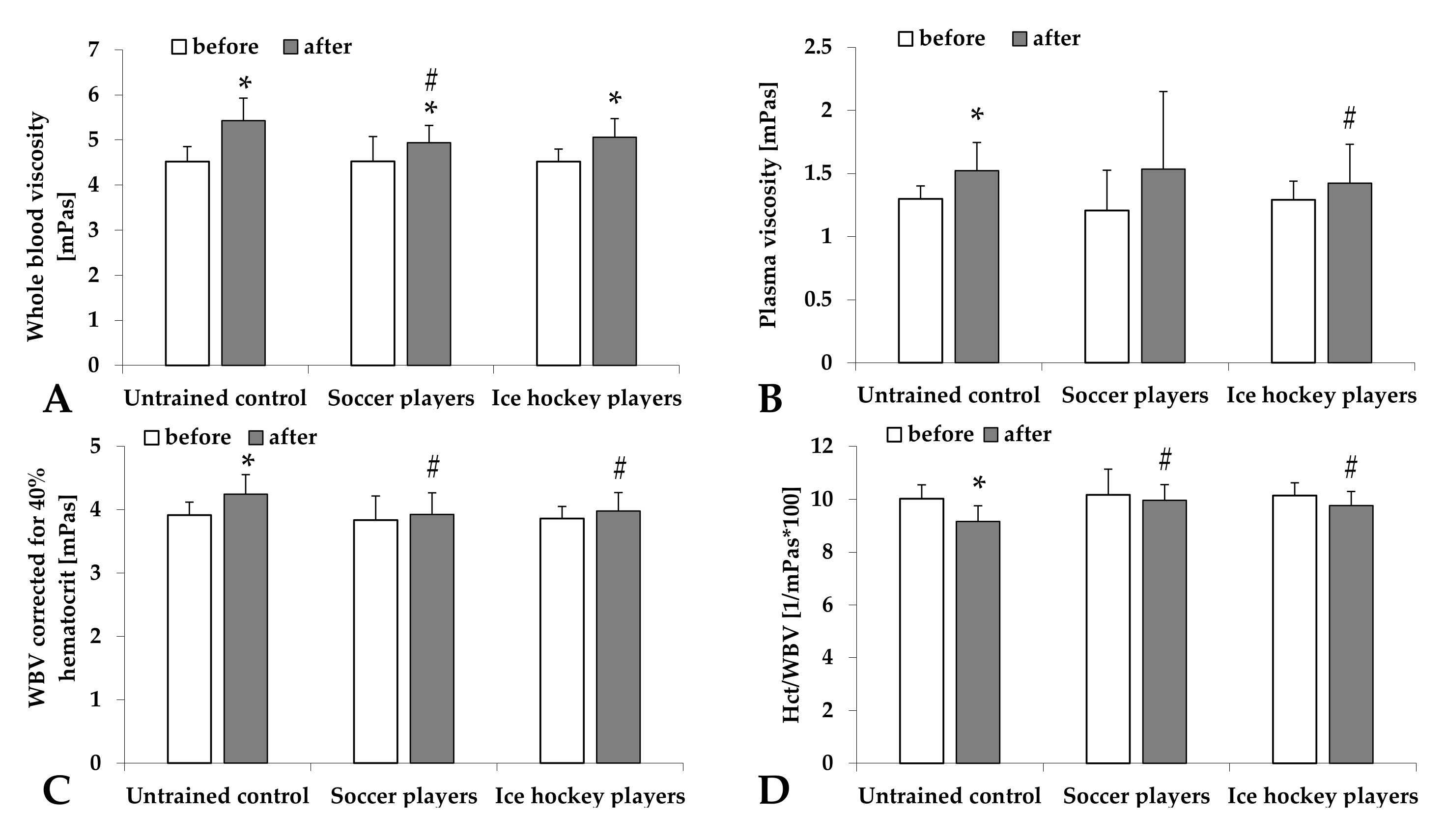
2.2. Blood and Plasma Viscosity
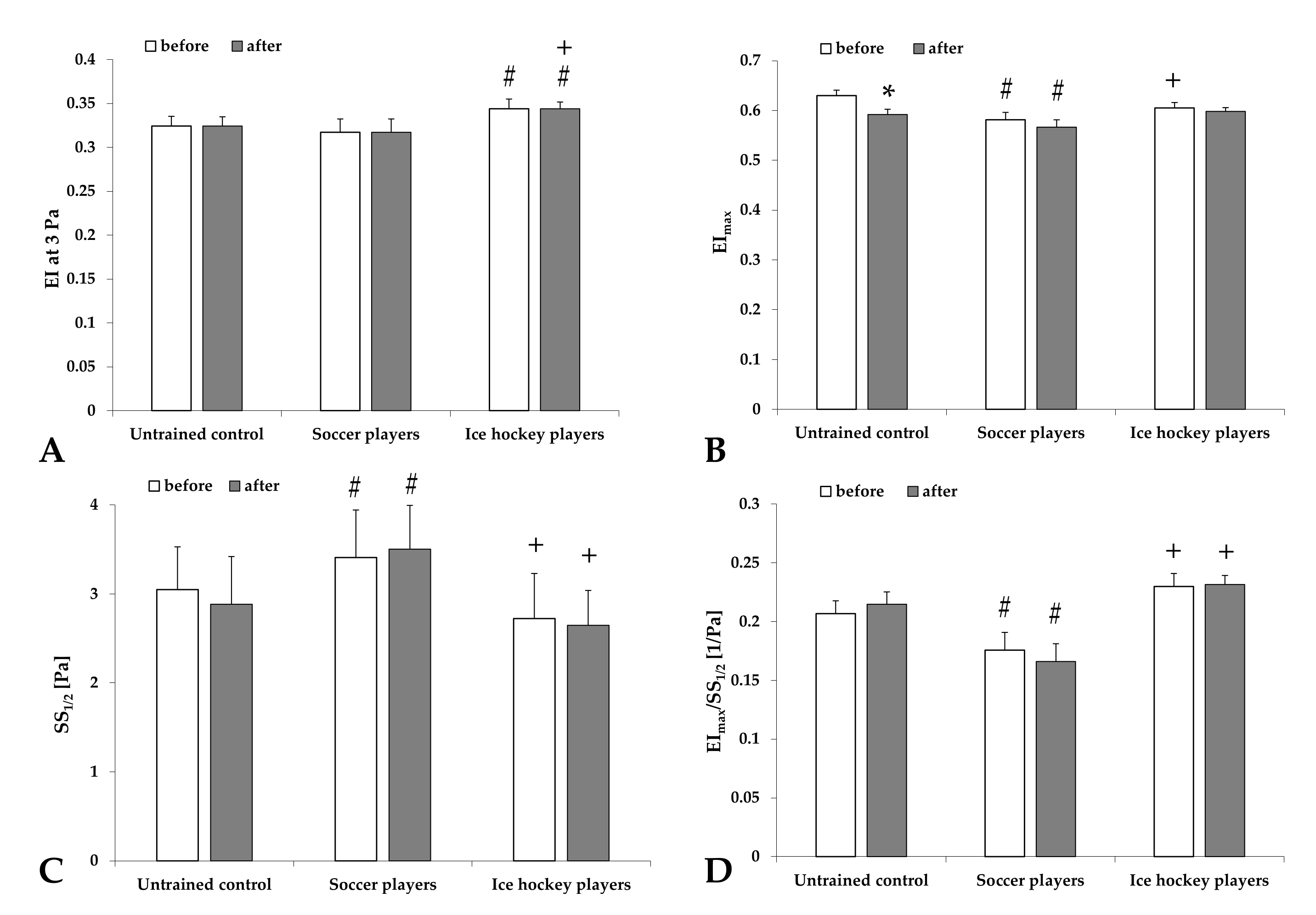
2.3. Red Blood Cell Deformability
2.4. Red Blood Cell Aggregation
2.5. Maximal Oxygen Uptake, Respiratory Exchange Rate, and Lactate Concentration
3. Discussion
4. Materials and Methods
4.1. Volunteers
4.2. Spiroergometry Tests and Collection of Blood Samples
4.3. Laboratory Methods
4.3.1. Hematological Parameters
4.3.2. Hemorheological Parameters
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baskurt, O.K.; Meiselman, H.J. Blood rheology and hemodynamics. Semin. Thromb. Hemost. 2003, 29, 435–450. [Google Scholar]
- Cokelet, G.R.; Meiselman, H.J. Basic aspects of hemorheology. In Handbook of Hemorheology and Hemodynamics; Baskurt, O.K., Hardeman, M.R., Rampling, M.W., Meiselman, H.J., Eds.; IOS Press: Amsterdam, The Netherlands, 2007; pp. 21–33. [Google Scholar]
- Cokelet, G.R.; Meiselman, H.J. Macro- and micro-rheological properties of blood. In Handbook of Hemorheology and Hemodynamics; Baskurt, O.K., Hardeman, M.R., Rampling, M.W., Meiselman, H.J., Eds.; IOS Press: Amsterdam, The Netherlands, 2007; pp. 45–71. [Google Scholar]
- Baskurt, O.K.; Neu, B.; Meiselman, H.J. Determinants of red blood cell aggregation. In Red Blood Cell Aggregation; Baskurt, O.K., Neu, B., Meiselman, H.J., Eds.; CRC Press: Boca Raton, FL, USA, 2012; pp. 9–29. [Google Scholar]
- Baskurt, O.K. Mechanisms of blood rheology alterations. In Handbook of Hemorheology and Hemodynamics; Baskurt, O.K., Hardeman, M.R., Rampling, M.W., Meiselman, H.J., Eds.; IOS Press: Amsterdam, The Netherlands, 2007; pp. 170–190. [Google Scholar]
- Nemeth, N.; Peto, K.; Magyar, Z.; Klarik, Z.; Varga, G.; Oltean, M.; Mantas, A.; Czigany, Z.; Tolba, R.H. Hemorheological and microcirculatory factors in liver ischemia-reperfusion injury—An update on pathophysiology, molecular mechanisms and protective strategies. Int J. Mol. Sci. 2021, 22, 1864. [Google Scholar] [CrossRef] [PubMed]
- Krüger-Genge, A.; Sternitzky, R.; Pindur, G.; Rampling, M.; Franke, R.P.; Jung, F. Erythrocyte aggregation in relation to plasma proteins and lipids. J. Cell. Biotech. 2019, 5, 65–70. [Google Scholar] [CrossRef]
- Weed, R.I.; La Celle, P.L.; Merrill, E.W. Metabolic dependence of red blood cell deformability. J. Clin. Investig. 1969, 48, 795–809. [Google Scholar] [CrossRef] [Green Version]
- Brun, J. Hormones, metabolism and body composition as major determinants of blood rheology: Potential pathophysiological meaning. Clin. Hemorheol. Microcirc. 2002, 26, 63–79. [Google Scholar]
- Reinhart, W.H.; Gaudenz, R.; Walter, R. Acidosis induced by lactate, pyruvate, or HCl increases blood viscosity. Crit. Care 2002, 17, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Cicha, I.; Suzuki, Y.; Tateishi, N.; Maeda, N. Changes of RBC aggregation in oxygenation-deoxygenation: pH dependency and cell morphology. Am. J. Physiol. Heart Circ. Physiol. 2003, 284, H2335–H2342. [Google Scholar] [CrossRef] [PubMed]
- Uyuklu, M.; Meiselman, H.J.; Baskurt, O.K. Effect of hemoglobin oxygenation level on red blood cell deformability and aggregation parameters. Clin. Hemorheol. Microcirc. 2009, 41, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Lipowsky, H.H. Microvascular rheology and hemodynamics. Microcirculation 2005, 12, 5–15. [Google Scholar] [CrossRef]
- Adachi, H.; Sakurai, S.; Tanehata, M.; Oshima, S.; Taniguchi, K. Effect of long-term exercise training on blood viscosity during endurance exercise at an anaerobic threshold intensity. Jpn. Circ. J. 2000, 64, 848–850. [Google Scholar] [CrossRef] [Green Version]
- Brun, J.F.; Varlet-Marie, E.; Connes, P.; Aloulou, I. Hemorheological alterations related to training and overtraining. Biorheology 2010, 47, 95–115. [Google Scholar] [CrossRef] [PubMed]
- Brun, J.F.; Varlet-Marie, E.; Romain, A.J.; Guiraudou, M.; Raynaud de Mauverger, E. Exercise hemorheology: Moving from old simplistic paradigms to a more complex picture. Clin. Hemorheol. Microcirc. 2013, 55, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Connes, P.; Simmonds, M.; Brun, J.F.; Baskurt, O.K. Exercise hemorheology: Classical data, recent findings and unresolved issues. Clin. Hemorheol. Microcirc. 2013, 53, 187–199. [Google Scholar] [CrossRef] [Green Version]
- Romain, A.J.; Brun, J.F.; Varlet-Marie, E.; Raynaud de Mauverger, E. Effects of exercise training on blood rheology: A meta-analysis. Clin. Hemorheol. Microcirc. 2011, 49, 199–205. [Google Scholar] [CrossRef]
- Ernst, E. Influence of regular physical activity on blood rheology. Eur. Heart J. 1987, 8, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Varlet-Marie, E.; Maso, F.; Lac, G.; Brun, J.F. Hemorheological disturbances in the overtraining syndrome. Clin. Hemorheol. Microcirc. 2004, 30, 211–218. [Google Scholar]
- El-Sayed, M.S.; Ali, N.; El-Sayed Ali, Z. Haemorheology in exercise and training. Sports Med. 2005, 35, 649–670. [Google Scholar] [CrossRef] [PubMed]
- Sandor, B.; Nagy, A.; Toth, A.; Rabai, M.; Mezey, B.; Csatho, A.; Czuriga, I.; Toth, K.; Szabados, E. Effects of moderate aerobic exercise training on hemorheological and laboratory parameters in ischemic heart disease patients. PLoS ONE 2014, 9, e110751. [Google Scholar]
- Nader, E.; Skinner, S.; Romana, M.; Fort, R.; Lemonne, N.; Guillot, N.; Gauthier, A.; Antoine-Jonville, S.; Renoux, C.; Hardy-Dessources, M.D.; et al. Blood rheology: Key parameters, impact on blood flow, role in sickle cell disease and effects of exercise. Front. Physiol. 2019, 10, 1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broich, H.; Sperlich, B.; Buitrago, S.; Mathes, S.; Mester, J. Performance assessment in elite football players: Field level test versus spiroergometry. J. Hum. Sport Exerc. 2012, 7, 287–295. [Google Scholar] [CrossRef] [Green Version]
- Löllgen, H.; Leyk, D. Exercise testing in sports medicine. Dtsch. Arztebl. Int. 2018, 115, 409–416. [Google Scholar] [CrossRef]
- Johnson, R.M. pH effects on red blood cell deformability. Blood Cells 1985, 11, 317–321. [Google Scholar] [PubMed]
- Senturk, U.K.; Gunduz, F.; Kuru, O.; Kocer, G.; Ozkaya, Y.G.; Yesilkaya, A.; Bor-Kucukatay, M.; Uyuklu, M.; Yalcin, O.; Baskurt, O.K. Exercise-Induced oxidative stress leads hemolysis in sedentary but not trained humans. J. Appl. Physiol. 2005, 99, 1434–1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinhart, W.H. The optimum hematocrit. Clin. Hemorheol. Microcirc. 2016, 64, 575–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krüger-Genge, A.; Blocki, A.; Franke, R.P.; Jung, F. Vascular endothelial cell biology: An update. Int. J. Mol. Sci. 2019, 20, 4411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.A.; Telford, R.D.; Kolbuch-Braddon, M.; Weidemann, M.J. Lactate/H+ uptake by red blood cells during exercise alters their physical properties. Eur. J. Appl. Physiol. Occup. Physiol. 1997, 75, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Skelton, M.S.; Kremer, D.E.; Smith, E.W.; Gladden, L.B. Lactate influx into red blood cells from trained and untrained human subject. Med. Sci. Sports Exerc. 1998, 30, 536–542. [Google Scholar] [CrossRef]
- Connes, P.; Bouix, D.; Py, G.; Prefaut, C.; Mercier, J.; Brun, J.F.; Caillaud, C. Opposite effects of In Vitro lactate on erythrocyte deformability in athletes and untrained subjects. Clin. Hemorheol. Microcirc. 2004, 31, 311–318. [Google Scholar]
- Messonnier, L.; Freund, H.; Denis, C.; Féasson, L.; Lacour, J.R. Effects of training on lactate kinetics parameters and their influence on short high-intensity exercise performance. Int. J. Sports Med. 2006, 27, 60–66. [Google Scholar] [CrossRef]
- Connes, P.; Caillaud, C.; Py, G.; Mercier, J.; Hue, O.; Brun, J.F. Maximal exercise and lactate do not change red blood cell aggregation in well trained athletes. Clin. Hemorheol. Microcirc. 2007, 36, 319–326. [Google Scholar] [PubMed]
- Connes, P.; Tripette, J.; Mukisi-Mukaza, M.; Baskurt, O.K.; Toth, K.; Meiselman, H.J.; Hue, O.; Antoine-Jonville, S. Relationships between hemodynamic, hemorheological and metabolic responses during exercise. Biorheology 2009, 46, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Nemkov, T.; Skinner, S.C.; Nader, E.; Stefanoni, D.; Robert, M.; Cendali, F.; Stauffer, E.; Cibiel, A.; Boisson, C.; Connes, P.; et al. Acute cycling exercise induces changes in red blood cell deformability and membrane lipid remodeling. Int. J. Mol. Sci. 2021, 22, 896. [Google Scholar] [CrossRef] [PubMed]
- Quittmann, O.J.; Abel, T.; Zeller, S.; Foitschik, T.; Strüder, H.K. Lactate kinetics in handcycling under various exercise modalities and their relationship to performance measures in able-bodied participants. Eur. J. Appl. Physiol. 2018, 118, 1493–1505. [Google Scholar] [CrossRef] [PubMed]
- Quittmann, O.J.; Abel, T.; Vafa, R.; Mester, J.; Schwarz, Y.M.; Strüder, H.K. Maximal lactate accumulation rate and post-exercise lactate kinetics in handcycling and cycling. Eur. J. Sport Sci. 2021, 21, 539–551. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, E.A.; Martin, N.R.W.; Bailey, S.J.; Ferguson, R.A. Critical power is positively related to skeletal muscle capillarity and type I muscle fibers in endurance-trained individuals. J. Appl. Physiol. 2018, 125, 737–745. [Google Scholar] [CrossRef]
- Hendrickse, P.; Degens, H. The role of the microcirculation in muscle function and plasticity. J. Muscle Res. Cell. Motil. 2019, 40, 127–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tesch, P.A.; Thorsson, A.; Kaiser, P. Muscle capillary supply and fiber type characteristics in weight and power lifters. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1984, 56, 35–38. [Google Scholar] [CrossRef]
- Alis, R.; Ibañez-Sania, S.; Basterra, J.; Sanchis-Gomar, F.; Romagnoli, M. Effects of an acute high-intensity interval training protocol on plasma viscosity. J. Sports Med. Phys. Fitness. 2015, 55, 647–653. [Google Scholar] [PubMed]
- Kilic-Toprak, E.; Yapici, A.; Kilic-Erkek, O.; Koklu, Y.; Tekin, V.; Alemdaroglu, U.; Bor-Kucukatay, M. Acute effects of Yo-Yo intermittent recovery test level 1 (Yo-YoIR1) on hemorheological parameters in female volleyball players. Clin. Hemorheol. Microcirc. 2015, 60, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Bizjak, D.A.; Tomschi, F.; Bales, G.; Nader, E.; Romana, M.; Connes, P.; Bloch, W.; Grau, M. Does endurance training improve red blood cell aging and hemorheology in moderate-trained healthy individuals? J. Sport Health Sci. 2020, 9, 595–603. [Google Scholar] [CrossRef]
- Harper, D.J.; Carling, C.; Kiely, J. High-Intensity acceleration and deceleration demands in elite team sports competitive match play: A systematic review and meta-analysis of observational studies. Sports Med. 2019, 49, 1923–1947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeder, M.; Wolber, T.; Atefy, R.; Gadza, M.; Ammann, P.; Myers, J.; Rickli, H. A nomogram to select the optimal treadmill ramp protocol in subjects with high exercise capacity: Validation and comparison with the Bruce protocol. J. Cardiopulm. Rehabil. 2006, 26, 16–23. [Google Scholar] [CrossRef]
- Arena, R.; Myers, J.; Williams, M.A.; Gulati, M.; Kligfield, P.; Balady, G.J.; Collins, E.; Fletcher, G.; American Heart Association Committee on Exercise, Rehabilitation, and Prevention of the Council on Clinical Cardiology; American Heart Association Council on Cardiovascular Nursing. Assessment of functional capacity in clinical and research settings: A scientific statement from the American Heart Association Committee on Exercise, Rehabilitation, and Prevention of the Council on Clinical Cardiology and the Council on Cardiovascular Nursing. Circulation 2007, 116, 329–343. [Google Scholar] [PubMed]
- Matrai, A.; Whittington, R.B.; Ernst, E. A simple method of estimating whole blood viscosity at standardized hematocrit. Clin. Hemorheol. 1987, 7, 261–265. [Google Scholar] [CrossRef]
- Hardeman, M.; Goedhart, P.; Shin, S. Methods in hemorheology. In Handbook of Hemorheology and Hemodynamics; Baskurt, O.K., Hardeman, M.R., Rampling, M.W., Meiselman, H.J., Eds.; IOS Press: Amsterdam, The Netherlands, 2007; pp. 242–266. [Google Scholar]
- Baskurt, O.K.; Boynard, M.; Cokelet, G.C.; Connes, P.; Cooke, B.M.; Forconi, S.; Liao, F.; Hardeman, M.R.; Jung, F.; Meiselman, H.J.; et al. New guidelines for hemorheological laboratory techniques. Clin. Hemorheol. Microcirc. 2009, 42, 75–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baskurt, O.K.; Hardeman, M.R.; Uyuklu, M.; Ulker, P.; Cengiz, M.; Nemeth, N.; Shin, S.; Alexy, T.; Meiselman, H.J. Parameterization of red blood cell elongation index--shear stress curves obtained by ektacytometry. Scand. J. Clin. Lab. Investig. 2009, 69, 777–788. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, N.; Kiss, F.; Miszti-Blasius, K. Interpretation of osmotic gradient ektacytometry (osmoscan) data: A comparative study for methodological standards. Scand. J. Clin. Lab. Investig. 2015, 75, 213–222. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | UnTrained Control Group | Professional Soccer Players | Professional Ice Hockey Players | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | Before/After Ratio | Before | After | Before/After Ratio | Before | After | Before/After Ratio | |
| WBC [×109/L] | 6.53 ± 0.99 | 11.86 ± 2.34 * | 1.81 ± 0.22 | 5.22 ± 1.21 # | 9.28 ± 2.39 *,# | 1.78 ± 0.37 | 5.48 ± 0.84 # | 11.01 ± 2.08 *,+ | 2.05 ± 0.52 |
| Lymph [%] | 37.36 ± 10.77 | 46.24 ± 8.16 * | 1.28 ± 0.21 | 32.39 ± 5.52 | 43.47 ± 8.34 * | 1.31 ± 0.21 | 34.12 ± 7.99 + | 35.01 ± 11.77 #,+ | 1.04 ± 0.27 #,+ |
| Gr+Mo [%] | 10.54 ± 2.23 | 10.21 ± 2.78 | 0.97 ± 0.16 | 9.08 ± 2.54 # | 8.43 ± 2.43 # | 1.06 ± 0.47 | 13.79 ± 3.85 #,+ | 11.44 ± 4.45 + | 0.82 ± 0.18 #,+ |
| RBC [×1012/L] | 5.06 ± 0.25 | 5.45 ± 0.25 * | 1.08 ± 0.03 | 5.24 ± 0.19 # | 5.53 ± 0.22 * | 1.06 ± 0.03 # | 5.14 ± 0.33 | 5.41 ± 0.41 * | 1.05 ± 0.03 # |
| Hct [%] | 45.14 ± 2.11 | 49.45 ± 2.29 * | 1.10 ± 0.03 | 45.52 ± 1.56 | 49.02 ± 1.42 * | 1.08 ± 0.03 # | 45.71 ± 1.74 | 49.27 ± 2.78 * | 1.08 ± 0.03 |
| Hgb [g/L] | 15.46 ± 0.84 | 16.77 ± 0.97 * | 1.08 ± 0.03 | 15.68 ± 0.73 | 16.53 ± 1.07 * | 1.06 ± 0.06 # | 15.65 ± 0.68 | 17.86 ± 6.21 * | 1.14 ± 0.41 # |
| MCV [fL] | 89.24 ± 3.05 | 90.74 ± 2.87 * | 1.02 ± 0.01 | 86.95 ± 3.07 # | 88.62 ± 3.06 *,# | 1.02 ± 0.01 | 89.09 ± 3.25 + | 91.21 ± 3.90 *,+ | 1.02 ± 0.01 #,+ |
| MCH [pg] | 30.57 ± 1.34 | 30.76 ± 1.49 | 1.01 ± 0.01 | 29.95 ± 1.47 | 29.91 ± 2.33 | 1.00 ± 0.06 | 30.51 ± 1.12 | 31.98 ± 1.15 | 1.05 ± 0.21 |
| MCHC [g/L] | 34.24 ± 0.72 | 33.90 ± 0.85 | 0.99 ± 0.02 | 34.44 ± 0.89 | 33.75 ± 2.19 | 0.98 ± 0.06 | 34.24 ± 0.54 | 33.71 ± 0.64 *,+ | 0.98 ± 0.02 |
| Plt [×109/L] | 231.45 ± 49.71 | 301.59 ± 66.13 * | 1.31 ± 0.08 | 215.46 ± 22.61 | 287.25 ± 41.43 * | 1.31 ± 0.14 | 224.75 ± 38.89 | 288.67 ± 45.53 * | 1.29 ± 0.10 |
| MPV [fL] | 10.77 ± 0.77 | 11.09 ± 0.91 | 1.03 ± 0.03 | 10.35 ± 1.23 | 10.46 ± 1.19 | 1.03 ± 0.03 | 10.40 ± 0.92 | 10.88 ± 1.00 | 1.05 ± 0.04 |
| Before/After Ratio of | Untrained Control Group | Professional Soccer Players | Professional Ice Hockey Players |
|---|---|---|---|
| WBV [mPas] | 1.20 ± 0.08 | 1.10 ± 0.10 # | 1.12 ± 0.05 # |
| PV [mPas] | 1.18 ± 0.19 | 1.41 ± 0.77 | 1.09 ± 0.11 |
| Hct40% [%] | 1.08 ± 0.06 | 1.03 ± 0.13 | 1.03 ± 0.06 # |
| Hct/WBV [mPas−1] | 0.91 ± 0.046 | 0.99 ± 0.11 # | 0.96 ± 0.04 # |
| EI at 3 Pa | 1.02 ± 0.11 | 1.02 ± 0.05 | 1.02 ± 0.04 |
| EImax | 1.13 ± 0.55 | 0.98 ± 0.04 # | 0.1 ± 0.04 |
| SS1/2 [Pa] | 1.02 ± 0.37 | 0.96 ± 0.14 | 0.96 ± 0.17 |
| EImax/SS1/2 [Pa−1] | 1.34 ± 1.32 | 1.04 ± 0.11 | 1.06 ± 0.15 |
| Variable | Untrained Control Group | Professional Soccer Players | Professional Ice Hockey Players | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | Before/ After Ratio | Before | After | Before/ After Ratio | Before | After | Before/ After Ratio | |
| EI min | 0.117 ± 0.007 | 0.12 ± 0.01 | 1.029 ± 0.069 | 0.13 ± 0.013 # | 0.128 ± 0.009 # | 0.992 ± 0.079 | 0.122 ± 0.01 | 0.119 ± 0.008 + | 0.979 ± 0.074 |
| EImax | 0.548 ± 0.011 | 0.547 ± 0.011 | 0.999 ± 0.034 | 0.569 ± 0.015# | 0.558 ± 0.007 *,# | 0.978 ± 0.022 | 0.554 ± 0.011 + | 0.566 ± 0.008 *,#,+ | 1.022 ± 0.027 + |
| EI hyper | 0.2742 ± 0.005 | 0.2738 ± 0.005 | 0.999 ± 0.033 | 0.284 ± 0.007 # | 0.279 ± 0.004 *# | 0.978 ± 0.021 | 0.277 ± 0.005 + | 0.283 ± 0.004 *,#,+ | 1.021 ± 0.027 + |
| O min [mOsm/L] | 139.09 ± 3.96 | 145.45 ± 4.69 * | 1.04 ± 0.02 | 137.5 ± 4.381 | 141.08 ± 4.72 # | 1.021 ± 0.03 # | 138.66 ± 4.81 | 140.75 ± 4.22 # | 1.015 ± 0.016 # |
| O (EImax) [mOsm/L] | 281.54 ± 16.38 | 278.64 ± 29.33 | 0.992 ± 0.115 | 288.64 ± 9.45 | 291.33 ± 11.63 | 1.007 ± 0.03 | 282.5 ± 9.01 | 289.5 ± 9.67 | 1.025 ± 0.022 |
| O hyper [mOsm/L] | 413.55 ± 14.14 | 418.82 ± 15.09 | 1.012 ± 0.016 | 418.21 ± 15 | 422.91 ± 16.26 | 1.008 ± 0.019 | 424.83 ± 9.97 # | 425.5 ± 11.21 | 1.002 ± 0.015 |
| Area | 143.98 ± 5.94 | 142.97 ± 5.11 | 0.994 ± 0.034 | 150.2 ± 6.63 # | 147.91 ± 5.91 # | 0.98 ± 0.024 # | 150.51 ± 4.71 # | 153.95 ± 3.54 #,+ | 1.024 ± 0.038 + |
| Variable | UnTrained Control Group | Professional Soccer Players | Professional Ice Hockey Players | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | Before/ After Ratio | Before | After | Before/ After Ratio | Before | After | Before/ After Ratio | |
| M 5 s | 3.38 ± 1.13 | 2.81 ± 1.07 * | 0.89 ± 0.36 | 2.97 ± 1.07 | 2.65 ± 0.96 | 0.99 ± 0.64 | 3.39 ± 0.88 | 3.00 ± 1.41 * | 0.88 ± 0.32 |
| M1 5 s | 2.75 ± 1.23 | 4.07 ± 1.15 * | 1.80 ± 1.02 | 2.78 ± 1.03 | 3.61 ± 1.01 *,# | 1.53 ± 0.94 | 3.14 ± 1.30 | 4.02 ± 1.14 * | 1.34 ± 0.44 |
| M 10 s | 9.43 ± 3.97 | 9.00 ± 3.08 | 1.07 ± 0.41 | 7.62 ± 3.34 # | 8.00 ± 2.55 | 1.27 ± 0.69 | 8.89 ± 3.36 | 8.36 ± 3.12 | 1.03 ± 0.50 |
| M1 10 s | 7.27 ± 2.57 | 10.53 ± 3.41 * | 1.61 ± 0.68 | 6.20 ± 3.07 | 8.94 ± 2.86 *,# | 1.74 ± 0.99 | 7.98 ± 3.80 + | 9.81 ± 3.89 * | 1.49 ± 0.97 # |
| AI [%] | 74.83 ± 18.44 | 86.45 ± 10.12 * | 1.24 ± 0.44 | 63.41 ± 4.90 # | 68.31 ± 3.59 *,# | 1.09 ± 0.06 | 78.43 ± 15.65 + | 79.19 ± 9.59 #,+ | 1.03 ± 0.15 #,+ |
| Amp [au] | 7.05 ± 4.80 | 4.55 ± 4.20 | 0.79 ± 0.29 | 16.80 ± 2.66 # | 15.54 ± 2.26 # | 0.96 ± 0.18 | 1.39 ± 2.95 #,+ | 0.20 ± 0.27 #,+ | 0.85 ± 0.90 |
| t1/2 [s] | 1.91 ± 2.04 | 0.97 ± 1.01 | 2.01 ± 3.26 | 2.25 ± 0.49 | 1.70 ± 0.29 *,# | 0.75 ± 0.15 | 1.48 ± 1.29 + | 1.36 ± 0.68 #,+ | 1.89 ± 1.96 + |
| Group | RER | Lactatemax [mmol/L] | Lactate5′ [mmol/L] | Lactatemax/Lactate5′ | R2 of RER and Lactatemax | R2 of RER and Lactate5′ |
|---|---|---|---|---|---|---|
| Untrained control group | 1.22 ± 0.08 | 12.71 ± 1.91 | 12.29 ± 2 | 1.04 ± 0.13 | 0.4176 | 0.1319 |
| Professional soccer players | 1.18 ± 0.05 | 14.94 ± 3.01 # | 14.58 ± 2.96 # | 1.03 ± 0.16 | 0.0029 | 0.0287 |
| Professional ice hockey players | 1.13 ± 0.04 #,+ | 13.26 ± 1.96 | 12.53 ± 2.16 | 1.07 ± 0.14 | 0.2027 | 0.1439 |
| Group | Age [year] | Height [cm] | Weight [kg] | BMI [kg/m2] | Percent Body Fat [%] | Skeletal Muscle Mass [kg] |
|---|---|---|---|---|---|---|
| Untrained control group | 25.09 ± 2.55 | 184.09 ± 5.82 | 89.55 ± 13.02 | 26.36 ± 3.41 | 20.41 ± 3.91 | 38.87 ± 1.94 |
| Professional soccer players | 22.71 ± 3.43 | 182.21 ± 5.63 | 77.79 ± 6.55 # | 23.64 ± 1.08 | 10.03 ± 4.55 # | 39.69 ± 3.54 |
| Professional ice hockey players | 24.25 ± 4.29 | 183.92 ± 5.6 | 86.17 ± 8.72 + | 25.42 ± 1.68 + | 16.46 ± 3.94 #,+ | 43.35 ± 8.83 # |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szanto, S.; Mody, T.; Gyurcsik, Z.; Babjak, L.B.; Somogyi, V.; Barath, B.; Varga, A.; Matrai, A.A.; Nemeth, N. Alterations of Selected Hemorheological and Metabolic Parameters Induced by Physical Activity in Untrained Men and Sportsmen. Metabolites 2021, 11, 870. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11120870
Szanto S, Mody T, Gyurcsik Z, Babjak LB, Somogyi V, Barath B, Varga A, Matrai AA, Nemeth N. Alterations of Selected Hemorheological and Metabolic Parameters Induced by Physical Activity in Untrained Men and Sportsmen. Metabolites. 2021; 11(12):870. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11120870
Chicago/Turabian StyleSzanto, Sandor, Tobias Mody, Zsuzsanna Gyurcsik, Laszlo Balint Babjak, Viktoria Somogyi, Barbara Barath, Adam Varga, Adam Attila Matrai, and Norbert Nemeth. 2021. "Alterations of Selected Hemorheological and Metabolic Parameters Induced by Physical Activity in Untrained Men and Sportsmen" Metabolites 11, no. 12: 870. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11120870