Detection of Increased Relative Expression Units of Bacteroides and Prevotella, and Decreased Clostridium leptum in Stool Samples from Brazilian Rheumatoid Arthritis Patients: A Pilot Study

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. DNA Extraction and Real-Time PCR
2.3. Cytokine Quantification by Flow Cytometer
2.4. Statistical Analysis
3. Results
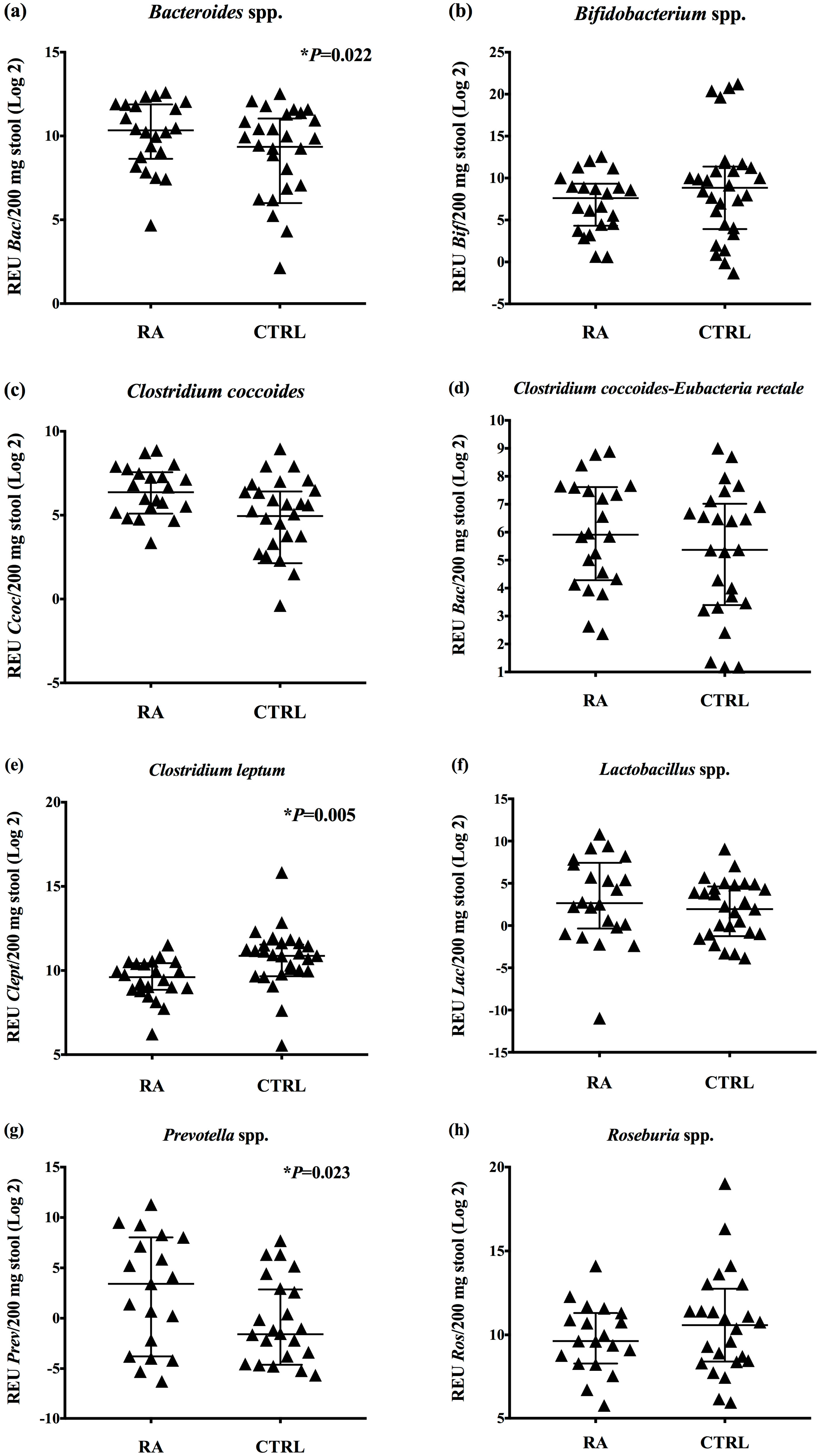
3.1. Increased Relative Expression Units of Bacteroides and Prevotella, and Decreased Clostridium leptum in the Gut Bacteria of RA Patients
3.2. Dietary Habits and Correlations with the Gut Bacteria in RA Patients
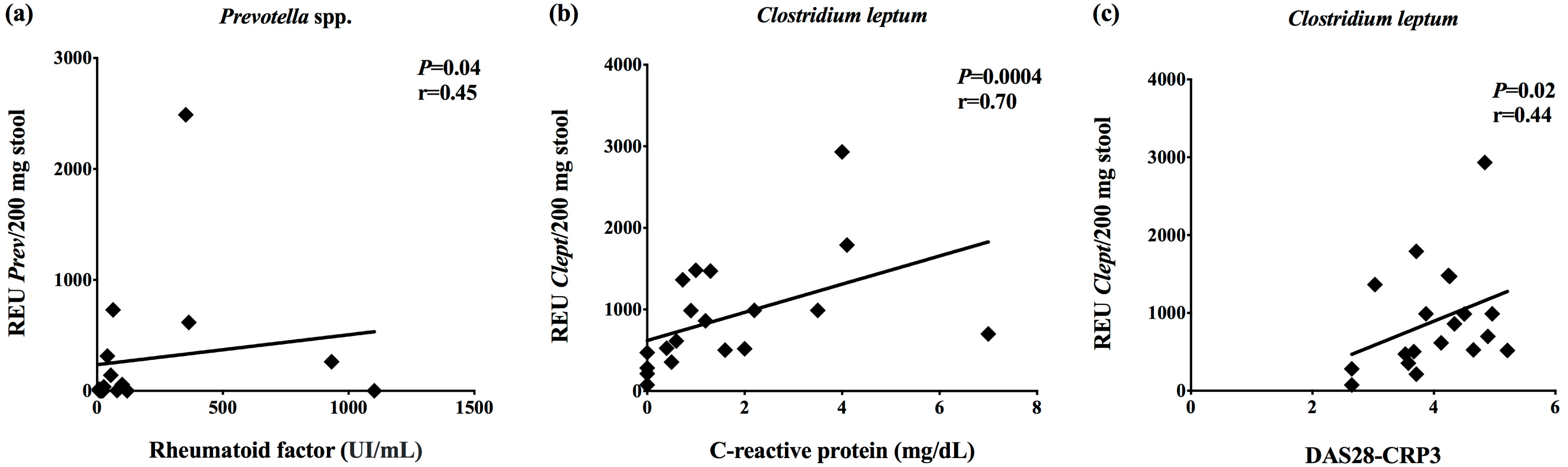
3.3. Correlations between the Gut Bacteria and Clinical Data
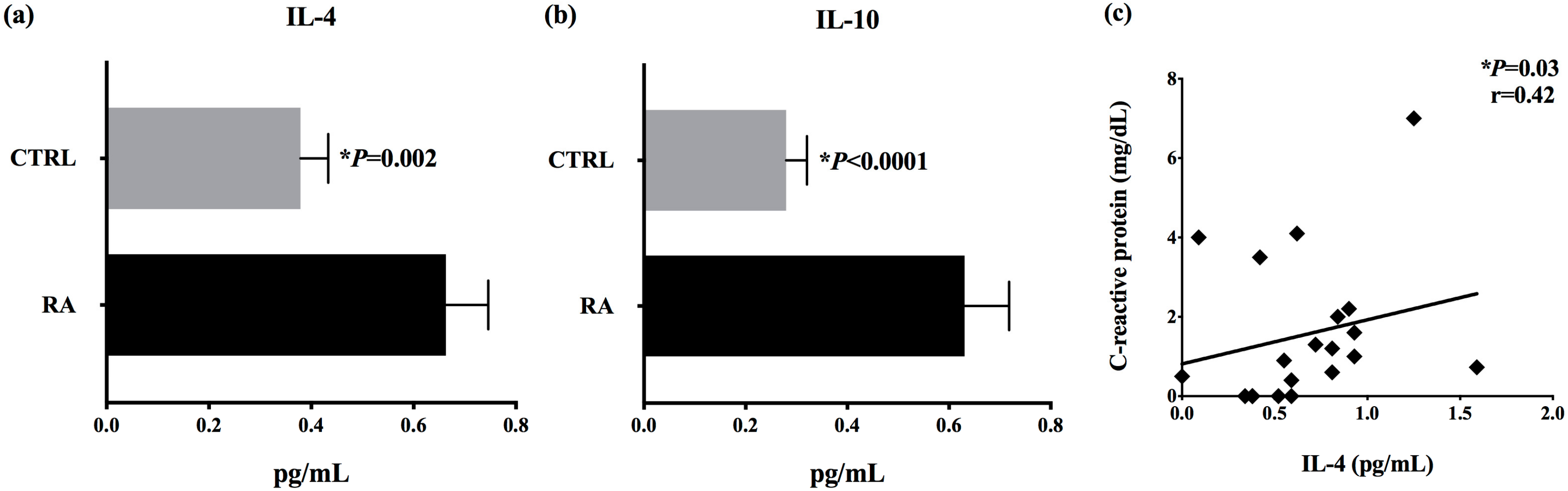
3.4. Increased Serum Concentrations of IL-4 and IL-10 in RA Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| RA | Rheumatoid arthritis |
| PCR | Polymerase chain reaction |
| IL-4 | Interleukin-4 |
| IL-10 | Interleukin-10 |
| DMARDs | Disease modifying antirheumatic drugs |
| RF | Rheumatoid factor |
| CRP | C-reactive protein |
| CIA | Collagen-induced arthritis |
| IL-6 | Interleukin-6 |
| IFN-γ | Interferon-gama |
| IL-17 | Interleukin-17 |
| Th17 | T helper 17 CD4+ lymphocyte |
| NSAIDs | Non-steroidal anti-inflammatories |
| Bac | Bacteroides species |
| Bif | Bifidobacterium species |
| Ccoc | Clostridium coccoides species |
| CIEub | Clostridium coccoides-Eubacteria rectale subgroup |
| Clept | Clostridium leptum species |
| Lac | Lactobacillus |
| Prev | Prevotella |
| Ros | Roseburia |
| DAS28 | Disease activity score |
| TNF | Tumor necrosis factor alpha |
| CTLA-4 | Cytotoxic T-lymphocyte-associated antigen 4 |
References
- Smolen, J.S.; Aletaha, D.; Barton, A.; Burmester, G.R.; Emery, P.; Firestein, G.S.; Kavanaugh, A.; Mclnnes, I.B.; Solomon, D.H.; Strand, V.; et al. Rheumatoid arthritis. Nat. Rev. Dis. Primers 2018, 4, 18001. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Smolen, J.S. Diagnosis and Management of Rheumatoid Arthritis: A Review. JAMA 2018, 320, 1360–1372. [Google Scholar] [CrossRef]
- Weijers, L.; Baerwald, C.; Mennini, F.S.; Rodríguez-Heredia, J.M.; Bergman, M.J.; Choquette, D.; Herrmann, K.H.; Attinà, G.; Nappi, C.; Merino, S.J.; et al. Cost per response for abatacept versus adalimumab in rheumatoid arthritis by ACPA subgroups in Germany, Italy, Spain, US and Canada. Rheumatol. Int. 2017, 37, 1111–1123. [Google Scholar] [CrossRef] [PubMed]
- Senna, E.R.; Barros, A.L.; Silva, E.O.; Costa, I.F.; Pereira, L.V.; Ciconelli, R.M.; Ferraz, M.B. Prevalence of rheumatic diseases in Brazil: A study using the COPCORD approach. J. Rheumatol. 2004, 31, 594–597. [Google Scholar] [PubMed]
- Lundkvist, J.; Kastang, F.; Kobelt, G. The burden of rheumatoid arthritis and access to treatment: Health burden and costs. Eur. J. Health Econ. 2008, 8, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, R.D.C.; Zanini, A.C. Cost analysis of drug therapy in rheumatoid arthritis. Braz. J. Pharm. Sci. 2008, 44, 25–33. [Google Scholar] [CrossRef]
- Malmström, V.; Catrina, A.I.; Klareskog, L. The immunopathogenesis of seropositive rheumatoid arthritis: from triggering to targeting. Nat. Rev. Immunol. 2017, 17, 60–75. [Google Scholar] [CrossRef]
- Van den Hoek, J.; Boshuizen, H.C.; Roorda, L.D.; Roorda, L.D.; Tijhuis, G.J.; Nurmohamed, M.T.; Van den Bos, G.A.; Dekker, J. Mortality in patients with rheumatoid arthritis: A 15-year prospective cohort study. Rheumatol. Int. 2017, 37, 487–493. [Google Scholar] [CrossRef]
- Horta-Baas, G.; Romero-Figueroa, M.D.S.; Montiel-Jarquín, A.J.; Pizano-Zárate, M.L.; García-Mena, J.; Ramírez-Durán, N. Intestinal Dysbiosis and Rheumatoid Arthritis: A Link between Gut Microbiota and the Pathogenesis of Rheumatoid Arthritis. J. Immunol. Res. 2017, 2017, 4835189. [Google Scholar] [CrossRef]
- Wu, X.; He, B.; Liu, J.; Feng, H.; Ma, Y.; Li, D.; Guo, B.; Liang, C.; Dang, L.; Wang, L.; et al. Molecular Insight into Gut Microbiota and Rheumatoid Arthritis. Int. J. Mol. Sci. 2016, 17, 431. [Google Scholar] [CrossRef]
- Brusca, S.B.; Abramson, S.B.; Scher, J.U. Microbiome and mucosal inflammation as extra-articular triggers for rheumatoid arthritis and autoimmunity. Curr. Opin. Rheumatol. 2014, 26, 101–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorożyńska, I.; Majewska-Szczepanik, M.; Marcińka, K.; Szczepanik, M. Partial depletion of natural gut flora by antibiotic aggravates collagen induced arthritis (CIA) in mice. Pharm. Rep. 2014, 66, 250–255. [Google Scholar] [CrossRef]
- Gomez, A.; Luckey, D.; Yeoman, C.J.; Marietta, E.V.; Berg Miller, M.E.; Murray, J.A.; White, B.A.; Taneja, V. Loss of sex and age driven differences in the gut microbiome characterize arthritis-susceptible 0401 mice but not arthritis-resistant 0402 mice. PLoS ONE 2012, 7, e36095. [Google Scholar] [CrossRef] [PubMed]
- Maeda, Y.; Kurakawa, T.; Umemoto, E.; Motooka, D.; Ito, Y.; Gotoh, K.; Hirota, K.; Matsushita, M.; Furuta, Y.; Narazaki, M.; et al. Dysbiosis Contributes to Arthritis Development via Activation of Autoreactive T Cells in the Intestine. Arthritis Rheumatol. 2016, 68, 2646–2661. [Google Scholar] [CrossRef] [PubMed]
- Nardini, C.; Devescovi, V.; Liu, Y.; Zhou, X.; Lu, Y.; Dent, J.E. Systemic Wound Healing Associated with local sub-Cutaneous Mechanical Stimulation. Sci. Rep. 2016, 6, 39043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, X.; Devescovi, V.; Liu, Y.; Dent, J.E.; Nardini, C. Host-Microbiome Synergistic Control on Sphingolipid Metabolism by Mechanotransduction in Model Arthritis. Biomolecules 2019, 9, 144. [Google Scholar] [CrossRef] [PubMed]
- Scher, J.U.; Sczesnak, A.; Longman, R.S.; Segata, N.; Ubeda, C.; Bielski, C.; Rostron, T.; Cerundolo, V.; Pamer, E.G.; Abramson, S.B.; et al. Expansion of intestinal Prevotella copri correlates with enhanced susceptibility to arthritis. Elife 2013, 5, e01202. [Google Scholar] [CrossRef]
- Chen, J.; Wright, K.; Davis, J.M.; Jeraldo, P.; Marietta, E.V.; Murray, J.; Nelson, H.; Matteson, E.L.; Taneja, V. An expansion of rare lineage intestinal microbes characterizes rheumatoid arthritis. Genome Med. 2016, 8, 43. [Google Scholar] [CrossRef]
- Picchianti-Diamanti, A.; Panebianco, C.; Salemi, S.; Sorgi, M.L.; Di Rosa, R.; Tropea, A.; Sgrulletti, M.; Salerno, G.; Terracciano, F.; D’Amelio, R.; et al. Analysis of Gut Microbiota in Rheumatoid Arthritis Patients: Disease-Related Dysbiosis and Modifications Induced by Etanercept. Int. J. Mol. Sci. 2018, 19, 2938. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, D.; Jia, H.; Feng, Q.; Wang, D.; Liang, D.; Wu, X.; Li, J.; Tang, L.; Li, Y.; et al. The oral and gut microbiomes are perturbed in rheumatoid arthritis and partly normalizedafter treatment. Nat. Med. 2015, 21, 895–905. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- Larsen, N.; Vogensen, F.K.; Van den Berg, F.W.J.; Nielsen, D.S.; Andreasen, A.S.; Pedersen, B.K.; Al-Soud, W.A.; Sørensen, S.J.; Hansen, L.H.; Jakobsen, M. Gut microbiota in human adults with type 2 diabetes differs from non-diabetic adults. PLoS ONE 2010, 5, e9085. [Google Scholar] [CrossRef] [PubMed]
- Albesiano, E.; Messmer, B.T.; Damle, R.N.; Allen, S.L.; Rai, K.R.; Chiorazzi, N. Activation-induced cytidine deaminase in chronic lymphocytic leukemia B cells: Expression as multiple forms in a dynamic, variably sized fraction of the clone. Blood 2003, 102, 3333–3339. [Google Scholar] [CrossRef] [PubMed]
- Bernard, N.J. Rheumatoid arthritis: Prevotella copri associated with new-onset untreated RA. Nat. Rev. Rheumatol. 2014, 10, 2. [Google Scholar] [CrossRef] [PubMed]
- Shinebaum, R.; Neumann, V.C.; Cooke, E.M.; Wright, V. Comparison of faecal florae in patients with rheumatoid arthritis and controls. Br. J. Rheumatol. 1987, 26, 329–333. [Google Scholar] [CrossRef]
- Eerola, E.; Möttönen, T.; Hannonen, P.; Luukkainen, R.; Kantola, I.; Vuori, K.; Tuominen, J.; Toivanen, P. Intestinal flora in early rheumatoid arthritis. Br. J. Rheumatol. 1994, 33, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Vaahtovuo, J.; Munukka, E.; Korkeamäki, M.; Luukkainen, R.; Toivanen, P. Fecal microbiota in early rheumatoid arthritis. J. Rheumatol. 2008, 35, 1500–1505. [Google Scholar] [PubMed]
- Toivanen, P.; Vartiainen, S.; Jalava, J.; Luukkainen, R.; Möttönen, T.; Eerola, E.; Manninen, R. Intestinal anaerobic bacteria in early rheumatoid arthritis (RA). Arthritis Res. 2002, 4, 5. [Google Scholar] [CrossRef]
- Liu, X.; Zou, Q.; Zeng, B.; Fang, Y.; Wei, H. Analysis of fecal Lactobacillus community structure in patients with early rheumatoid arthritis. Curr. Microbiol. 2013, 67, 170–176. [Google Scholar] [CrossRef]
- Holers, V.M. Autoimmunity to citrullinated proteins and the initiation of rheumatoid arthritis. Curr. Opin. Immunol. 2013, 25, 728–735. [Google Scholar] [CrossRef] [Green Version]
- Klareskog, L.; Amara, K.; Malmström, V. Adaptive immunity in rheumatoid arthritis: anticitrulline and other antibodies in the pathogenesis of rheumatoid arthritis. Curr. Opin. Rheumatol. 2014, 26, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Skoldstam, L.; Hagfors, L.; Johansson, G. An experimental study of a Mediterranean diet intervention for patients with rheumatoid arthritis. Ann. Rheum. Dis. 2003, 62, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Glick-Bauer, M.; Yeh, M.-C. The health advantage of a vegan diet: Exploring the gut microbiota connection. Nutrients 2014, 6, 4822–4838. [Google Scholar] [CrossRef] [PubMed]
- Peltonen, R.; Nenonen, M.; Helve, T.; Hänninen, O.; Toivanen, P.; Eerola, E. Faecal microbial flora and disease activity in rheumatoid arthritis during a vegan diet. Br. J. Rheumatol. 1997, 36, 64–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, G.D.; Chen, J.; Hoffmann, C.; Bittinger, K.; Chen, Y.-Y.; Keilbaugh, S.A.; Bewtra, M.; Knights, D.; Walters, W.A.; Knight, R.; et al. Linking long-term dietary patterns with gut microbial enterotypes. Science 2011, 334, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Zhou, X.; Nardini, C. Dissection of the module network implementation “LemonTree”: enhancements towards applications in metagenomics and translation in autoimmune maladies. Mol. Biosyst. 2017, 13, 2083–2091. [Google Scholar] [CrossRef] [PubMed]
- Kolli, V.K.; Abraham, P.; Rabi, S. Methotrexate-induced nitrosative stress may play a critical role in small intestinal damage in the rat. Arch. Toxicol. 2008, 82, 763–770. [Google Scholar] [CrossRef] [PubMed]
- Fijlstra, M.; Ferdous, M.; Koning, A.M.; Rings, E.H.; Harmsen, H.J.; Tissing, W.J. Substantial decreases in the number and diversity of microbiota during chemotherapy-induced gastrointestinal mucositis in a rat model. Support Care Cancer 2015, 23, 1513–1522. [Google Scholar] [CrossRef]
- Alexander, J.L.; Wilson, I.D.; Teare, J.; Marchesi, J.R.; Nicholson, J.K.; Kinross, J.M. Gut microbiota modulation of chemotherapy efficacy and toxicity. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 356–365. [Google Scholar] [CrossRef]
- Zhou, B.; Xia, X.; Wang, P.; Chen, S.; Yu, C.; Huang, R.; Zhang, R.; Wang, Y.; Lu, L.; Yuan, F.; et al. Induction and Amelioration of Methotrexate-Induced Gastrointestinal Toxicity are Related to Immune Response and Gut Microbiota. EBioMedicine 2018, 33, 122–133. [Google Scholar] [CrossRef] [Green Version]
- Atarashi, K.; Tanoue, T.; Shima, T.; Imaoka, A.; Kuwahara, T.; Momose, Y.; Cheng, G.; Yamasaki, S.; Saito, T.; Ohba, Y.; et al. Induction of colonic regulatory T cells by indigenous Clostridium species. Science 2011, 331, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Round, J.L.; Mazmanian, S.K. Inducible Foxp3+ regulatory T-cell development by a commensal bacterium of the intestinal microbiota. Proc. Natl. Acad. Sci. USA 2010, 107, 12204–12209. [Google Scholar] [CrossRef] [PubMed]
- Nakachi, S.; Sumitomo, S.; Tsuchida, Y.; Tsuchiya, H.; Kono, M.; Kato, R.; Sakurai, K.; Hanata, N.; Nagafuchi, Y.; Tateishi, S.; et al. Interleukin-10-producing LAG3+ regulatory T cells are associated with disease activity and abatacept treatment in rheumatoid arthritis. Arthritis Res. 2017, 19, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobl, E.-L.; Mader, R.M.; Erlacher, L.; Duhm, B.; Mustak, M.; Bröll, H.; Högger, P.; Kalipciyan, M.; Jilma, B. The influence of methotrexate on the gene expression of the pro-inflammatory cytokine IL-12A in the therapy of rheumatoid arthritis. Clin. Exp. Rheumatol. 2011, 29, 963–969. [Google Scholar] [PubMed]
- Bankó, Z.; Pozsgay, J.; Gáti, T.; Rojkovich, B.; Ujfalussy, I.; Sármay, G. Regulatory B cells in rheumatoid arthritis: Alterations in patients receiving anti-TNF therapy. Clin. Immunol. 2017, 184, 63–69. [Google Scholar] [CrossRef]
- Stahn, C.; Buttgereit, F. Genomic and nongenomic effects of glucocorticoids. Nat. Clin. Pr. Rheumatol. 2008, 4, 525–533. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients | Sex/Age | Ethnicity | DAS28-CRP3 | RF (UI/mL) | ESR (mm/h) | CRP (mg/dL) | Disease Duration (years) | Current Treatment |
|---|---|---|---|---|---|---|---|---|
| RA01 | F/64 | Caucasian | 3.53 | ND | 46 | 0 | 12 | PRED, NAP/ESO, SSZ |
| RA02 | F/66 | Caucasian | 4.26 | ND | 10 | 1.3 | 20 | MTX |
| RA03 | F/37 | Caucasian | 3.67 | 8.70 | 30 | 1.6 | 4 | NAP/ESO, PRED |
| RA04 | F/49 | Caucasian | 3.03 | ND | 5 | 0.73 | 5 | PRED, MTX, LEF |
| RA05 | F/53 | Hispanic | 4.24 | 9.20 | 24 | 1.0 | 15 | DFZ |
| RA06 | F/66 | Caucasian | 4.12 | 64.0 | 68 | 0.6 | 8 | PRED, MTX, ADA |
| RA07 | F/55 | Hispanic | 4.50 | 41.0 | 6 | 0.9 | 25 | MTX, ADA |
| RA08 | F/50 | Hispanic | 3.87 | 22.7 | 69 | 2.2 | 25 | MTX, PRED |
| RA09 | F/71 | Caucasian | 4.65 | 15.8 | 9 | 0.4 | 15 | MTX, PRED |
| RA10 | F/59 | Caucasian | 5.21 | 932.5 | 51 | 2.0 | 7 | ABA, MTX |
| RA11 | F/63 | Caucasian | 4.96 | 1102.5 | 99 | 3.5 | 10 | PRED |
| RA12 | F/51 | Caucasian | 2.65 | 100.0 | 63 | 0 | 3 | MTX |
| RA13 | F/64 | Afro-descendent | 3.71 | 79.9 | 68 | 4.1 | 12 | Meloxicam |
| RA14 | F/36 | Caucasian | 4.34 | 365.0 | 31 | 1.2 | 14 | MTX, PRED, ADA |
| RA15 | F/61 | Caucasian | 2.65 | 353.2 | 50 | 0 | 12 | MTX |
| RA16 | F/57 | Caucasian | 4.89 | 27.0 | 72 | 7.0 | 2 | MTX |
| RA17 | F/46 | Hispanic | 3.58 | 16.8 | 34 | 0.5 | 12 | ADA, LEF |
| RA18 | F/62 | Hispanic | 3.71 | 55.0 | 7 | 0 | 10 | PRED, NAP/ESO, HCQ |
| RA19 | F/61 | Caucasian | 4.84 | ND | 35 | 4.0 | 4 | ABA, LEF |
| RA20 | F/64 | Caucasian | 3.95 | 120.0 | 48 | 0 | 15 | PRED |
| Consumption Frequency | Number of Individuals (N) | RA Patients (%) | Number of Individuals (N) | Healthy Controls (%) | Chi-Squared p-Value | Adjusted p-Value |
|---|---|---|---|---|---|---|
| Vegetables | ||||||
| Never | - | - | - | - | p = 0.676 | p = 1.000 |
| * Rarely | 5 | 25 | 6 | 20 | ||
| # Frequently | 15 | 75 | 24 | 80 | ||
| Fresh fruits | ||||||
| Never | - | - | - | - | p = 0.273 | p = 0.910 |
| * Rarely | 5 | 25 | 12 | 40 | ||
| # Frequently | 15 | 75 | 18 | 60 | ||
| Carbohydrates | ||||||
| Never | 1 | 5 | 1 | 3.3 | p = 0.953 | p = 1.000 |
| * Rarely | 5 | 25 | 8 | 26.7 | ||
| # Frequently | 14 | 70 | 21 | 70 | ||
| Animal-derived proteins | ||||||
| Never | - | - | - | - | p = 1.000 | p = 1.000 |
| * Rarely | 8 | 40 | 12 | 40 | ||
| # Frequently | 12 | 60 | 18 | 60 | ||
| Trans fats | ||||||
| Never | 3 | 15 | 6 | 20 | p = 0.859 | p = 1.000 |
| * Rarely | 12 | 60 | 18 | 60 | ||
| # Frequently | 5 | 25 | 6 | 20 | ||
| Milk and derivatives | ||||||
| Never | 1 | 5 | 1 | 3.3 | p = 0.957 | p = 1.000 |
| * Rarely | 6 | 30 | 9 | 30 | ||
| # Frequently | 13 | 65 | 20 | 66.7 | ||
| Hot drinks (coffee/tea) | ||||||
| Never | 1 | 5 | 1 | 3.3 | p = 0.102 | p = 0.51 |
| * Rarely | - | - | 6 | 20 | ||
| # Frequently | 19 | 95 | 23 | 76.7 | ||
| Canned food | ||||||
| Never | 7 | 35 | 8 | 26.7 | p = 0.812 | p = 1.000 |
| * Rarely | 11 | 55 | 19 | 63.3 | ||
| # Frequently | 2 | 10 | 3 | 10 | ||
| Condiments (ketchup/mayo) | ||||||
| Never | 8 | 40 | 12 | 40 | p = 0.46 | p = 1.000 |
| * Rarely | 11 | 55 | 18 | 60 | ||
| # Frequently | 1 | 5 | - | - | ||
| Spicy food | ||||||
| Never | 7 | 35 | 15 | 50 | p = 0.005 | p = 0.05 |
| * Rarely | 3 | 15 | 12 | 40 | ||
| # Frequently | 10 | 50 | 3 | 10 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, G.S.P.; Cayres, L.C.F.; Gonçalves, F.P.; Takaoka, N.N.C.; Lengert, A.H.; Tansini, A.; Brisotti, J.L.; Sasdelli, C.B.G.; de Oliveira, G.L.V. Detection of Increased Relative Expression Units of Bacteroides and Prevotella, and Decreased Clostridium leptum in Stool Samples from Brazilian Rheumatoid Arthritis Patients: A Pilot Study. Microorganisms 2019, 7, 413. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms7100413
Rodrigues GSP, Cayres LCF, Gonçalves FP, Takaoka NNC, Lengert AH, Tansini A, Brisotti JL, Sasdelli CBG, de Oliveira GLV. Detection of Increased Relative Expression Units of Bacteroides and Prevotella, and Decreased Clostridium leptum in Stool Samples from Brazilian Rheumatoid Arthritis Patients: A Pilot Study. Microorganisms. 2019; 7(10):413. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms7100413
Chicago/Turabian StyleRodrigues, Guilherme S. P., Leonardo C. F. Cayres, Fernanda P. Gonçalves, Nauyta N. C. Takaoka, André H. Lengert, Aline Tansini, João L. Brisotti, Carolina B. G. Sasdelli, and Gislane L. V. de Oliveira. 2019. "Detection of Increased Relative Expression Units of Bacteroides and Prevotella, and Decreased Clostridium leptum in Stool Samples from Brazilian Rheumatoid Arthritis Patients: A Pilot Study" Microorganisms 7, no. 10: 413. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms7100413