Preventing Surgical Site Infections Using a Natural, Biodegradable, Antibacterial Coating on Surgical Sutures

Abstract
:
1. Introduction
2. Results
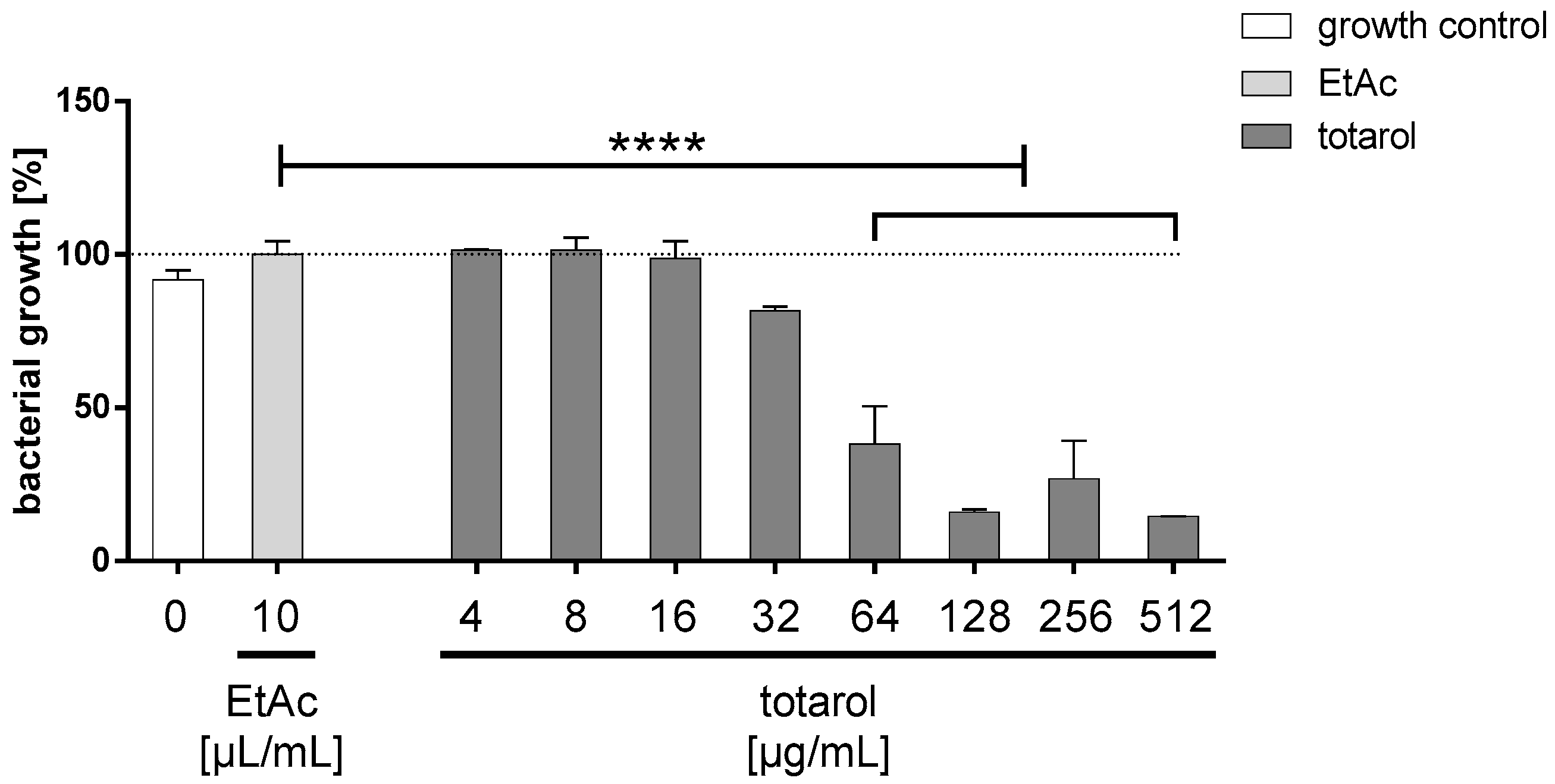
2.1. Antibacterial Activity of Totarol
Minimal Inhibitory Concentration (MIC)
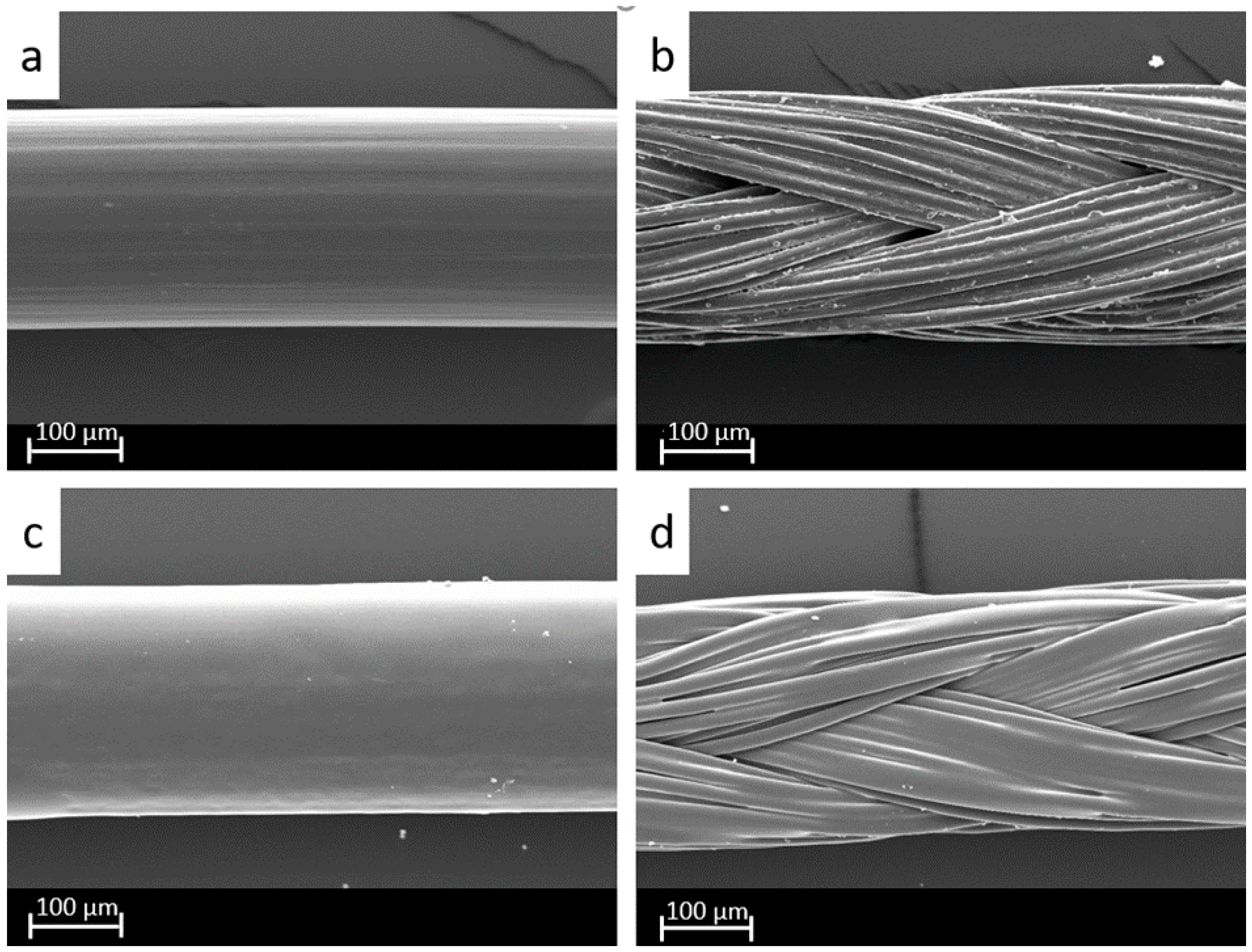
2.2. Coating Analysis
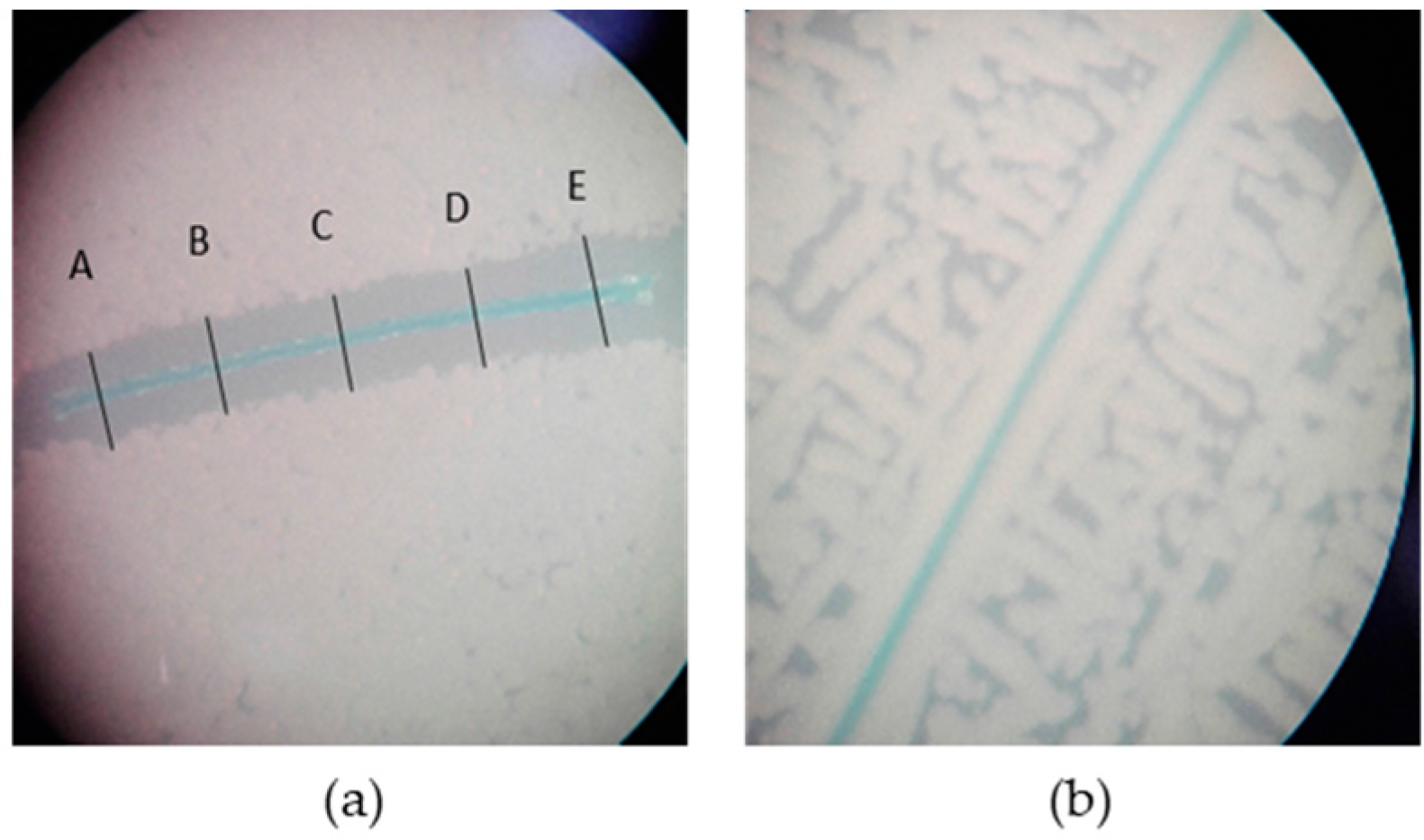
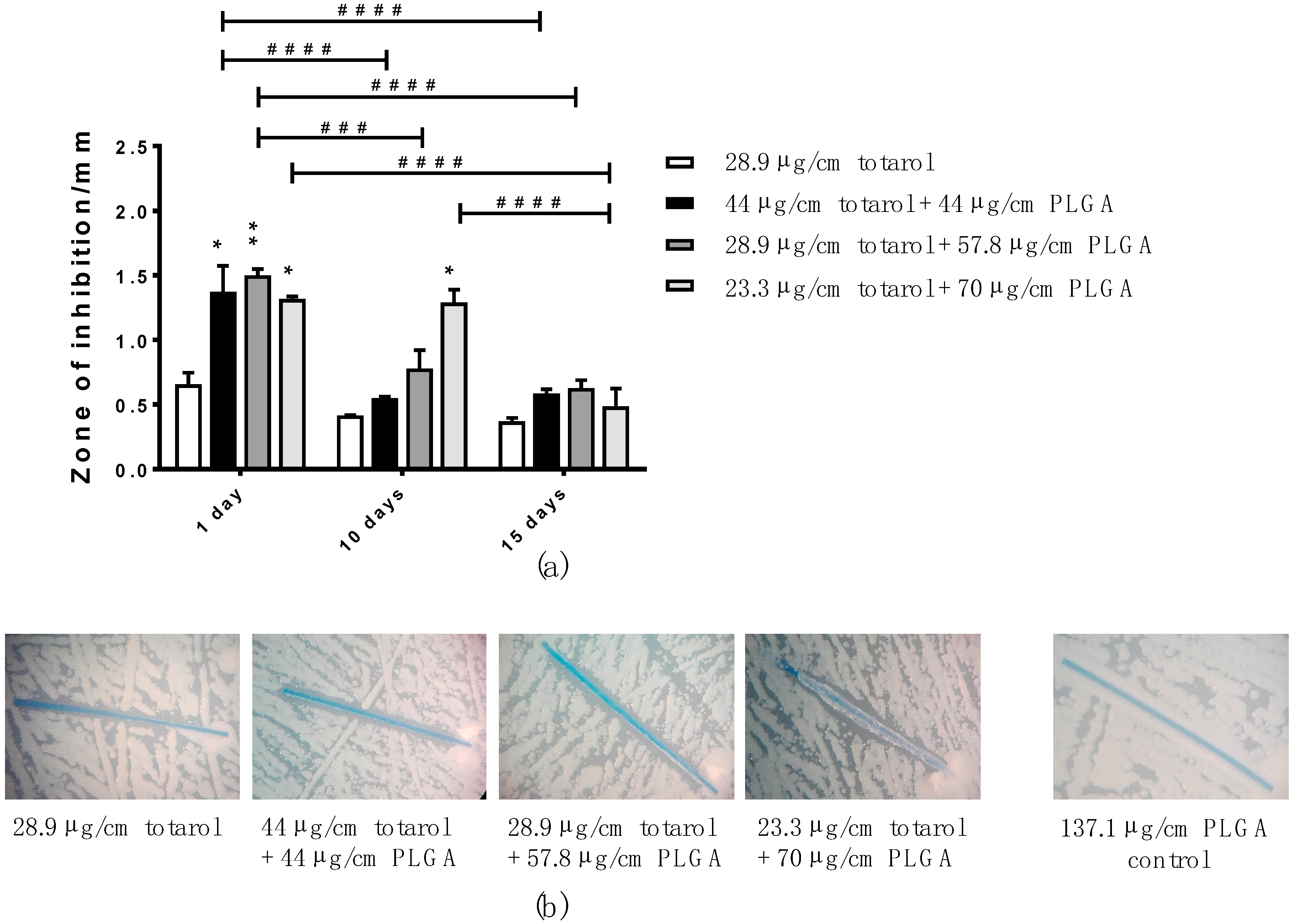
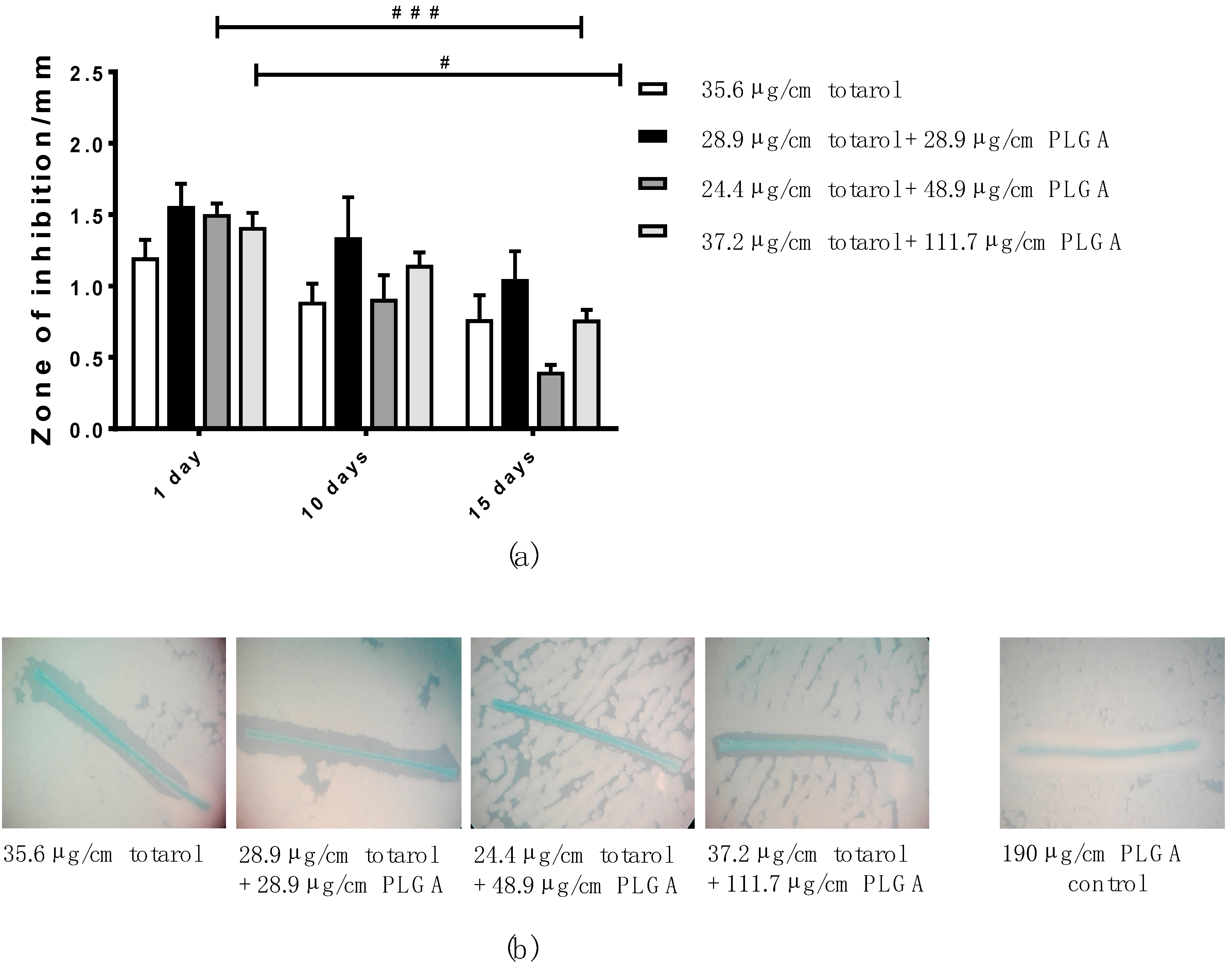
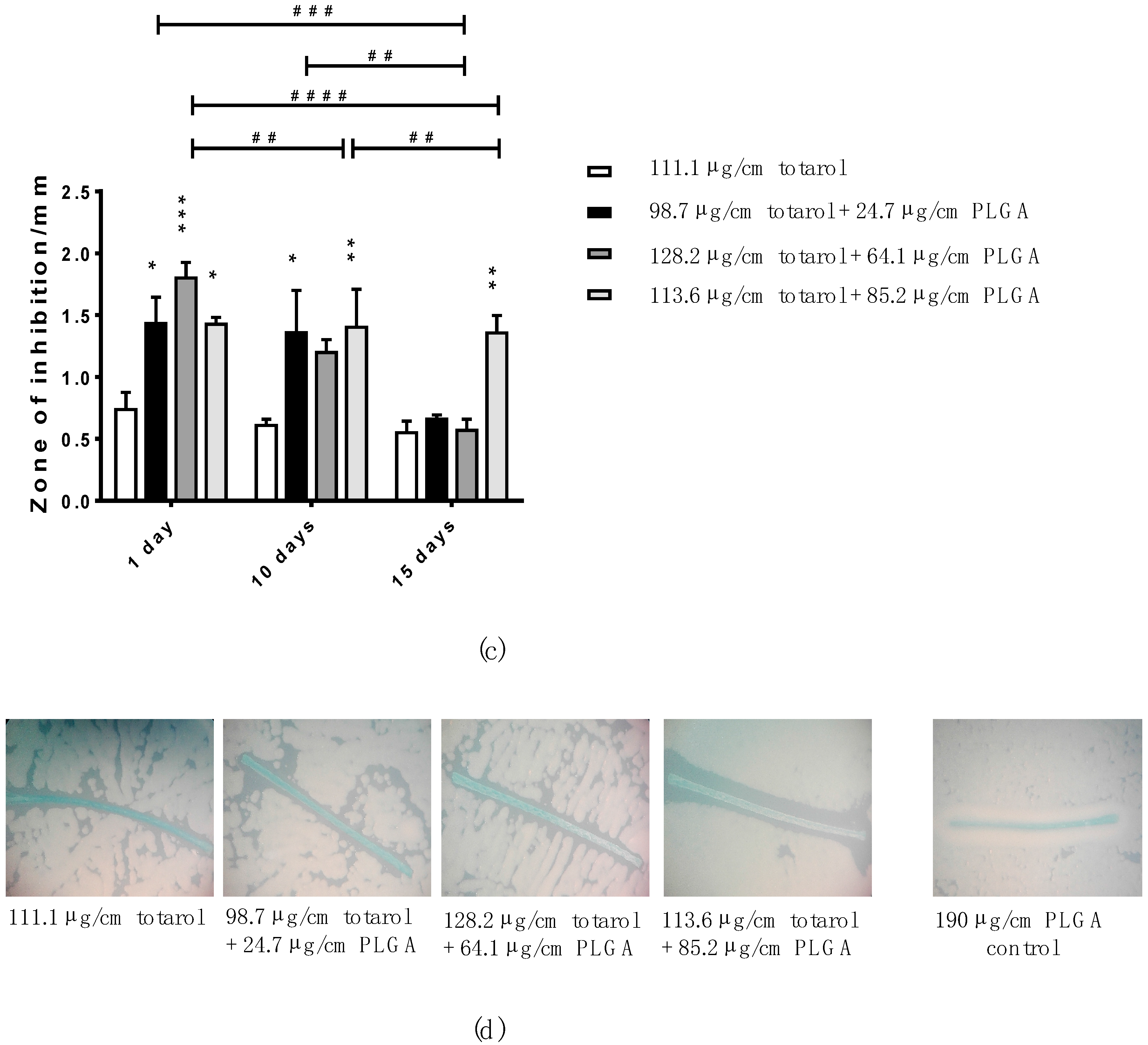
2.3. Long-Term Efficacy of Totarol
Agar Diffusion Test (ADT)
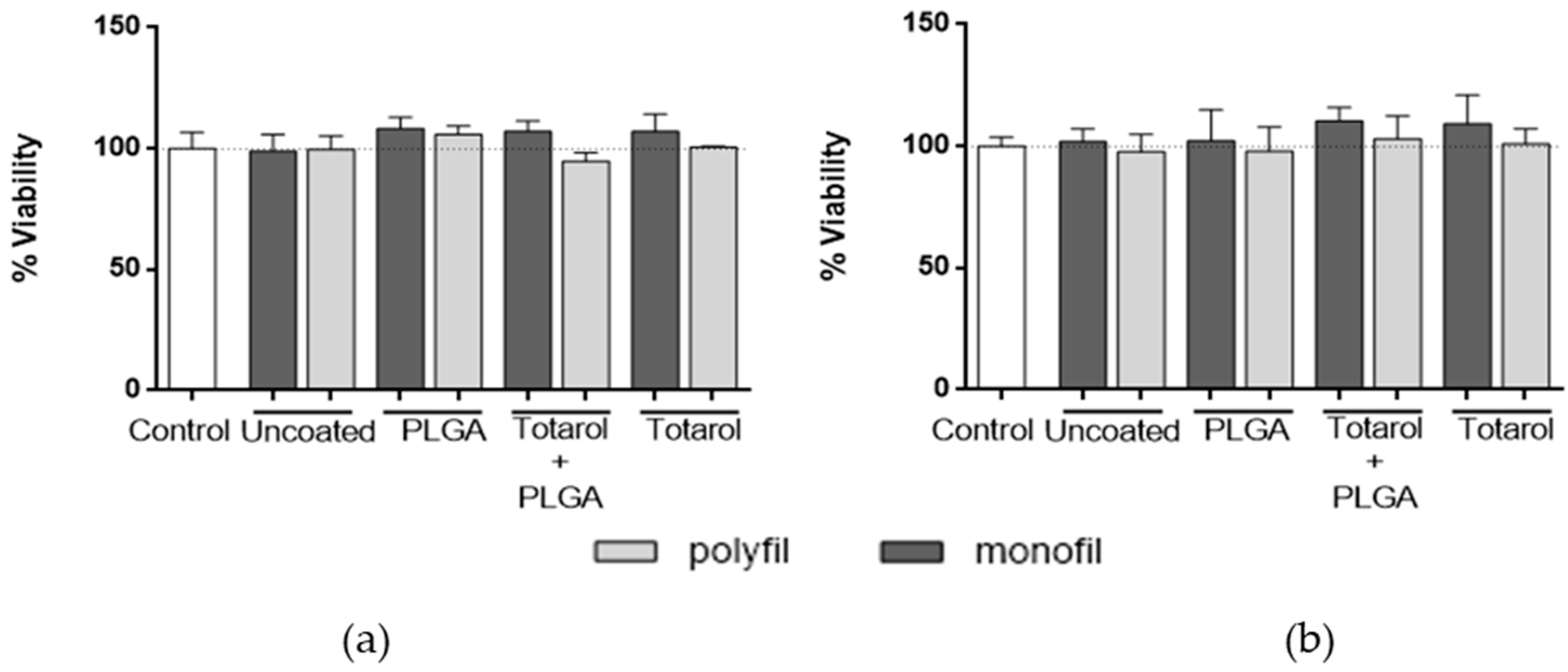
2.4. Cytotoxicity of Coated and Uncoated Sutures
MTT (3-(4,5-Dimethylthiazol-2-yl)-2,5-Diphenyltetrazolium Bromide) Assay
3. Discussion
4. Materials and Methods
4.1. Materials
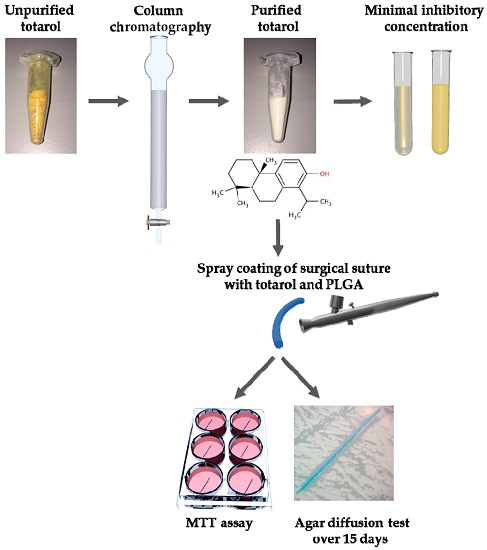
4.2. Totarol Purification
4.3. Coating Process
4.4. In Vitro Antibacterial Activity
4.4.1. Minimal Inhibitory Concentration (MIC)
4.4.2. Agar Diffusion Test
4.5. Cytotoxicity of Coated and Uncoated Sutures
4.6. Statistics
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| SSI | Surgery site infection |
| PLGA | Poly(lactide- co-glycolide acid) |
| ADT | Agar diffusion test |
| MTT | 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide |
| FDA | Food and Drug Administration |
| S. aureus | Staphylococcus aureus |
| MRSA | Methicillin-resistant Staphylococcus aureus |
| MIC | Minimal inhibitory concentration |
| ATCC | American Type Culture Collection |
| CLSI | Clinical and Laboratory Standard Institute |
| EtAc | Ethyl acetate |
| DMSO | Dimethyl sulfoxide |
| PBS | Phosphate buffer saline |
| DMEM | Dulbecco’s Modified Eagle Medium |
| HEPES | 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid |
| TLC | Thin layer chromatography |
| SEM | Scanning electron microscope |
| MHB | Mueller-Hinton-broth |
| CLSI | Clinical & Laboratory Standards Institute |
| SEM | error of the mean |
| RM | repeated-measures |
References
- De Simone, S.; Gallo, A.L.; Paladini, F.; Sannino, A.; Pollini, M. Development of silver nano-coatings on silk sutures as a novel approach against surgical infections. J. Mater. Sci. Mater. Med. 2014, 25, 2205–2214. [Google Scholar] [CrossRef] [PubMed]
- Gallo, A.L.; Paladini, F.; Romano, A.; Verri, T.; Quattrini, A.; Sannino, A.; Pollini, M. Efficacy of silver coated surgical sutures on bacterial contamination, cellular response and wound healing. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 69, 884–893. [Google Scholar] [CrossRef] [PubMed]
- Lenz, A.M.; Fairweather, M.; Cheadle, W.G. Resistance profiles in surgical-site infection. Future Microbiol. 2008, 3, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Izhar, M.; Mirelman, D. Bacterial adherence to surgical sutures. A possible factor in suture induced infection. Ann. Surg. 1981, 194, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Shunmugaperumal, T. Microbial colonization of medical devices and novel preventive strategies. Recent Pat. Drug Deliv. Formul. 2010, 4, 153–173. [Google Scholar] [CrossRef] [PubMed]
- Klose, D.; Siepmann, F.; Willart, J.F.; Descamps, M.; Siepmann, J. Drug release from PLGA-based microparticles: Effects of the ‘microparticle:bulk fluid’ ratio. Int. J. Pharm. 2010, 383, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Ignatius, A.A.; Claes, L.E. In vitro biocompatibility of bioresorbable polymers: Poly(l, dl-lactide) and poly(l-lactide-co-glycolide). Biomaterials 1996, 17, 831–839. [Google Scholar] [CrossRef]
- Shive, M.S.; Anderson, J.M. Biodegradation and biocompatibility of PLA and PLGA microspheres. Adv. Drug Deliv. Rev. 1997, 28, 5–24. [Google Scholar] [PubMed]
- Hu, C.; Feng, H.; Zhu, C. Preparation and characterization of rifampicin-PLGA microspheres/sodium alginate in situ gel combination delivery system. Colloids Surf. B Biointerfaces 2012, 95, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Marquette, S.; Peerboom, C.; Yates, A.; Denis, L.; Langer, I.; Amighi, K.; Goole, J. Stability study of full-length antibody (anti-TNF alpha) loaded PLGA microspheres. Int. J. Pharm. 2014, 470, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Muroi, H.; Kubo, I. Antibacterial activity of anacardic acid and totarol, alone and in combination with methicillin, against methicillin-resistant Staphylococcus aureus. J. Appl. Bacteriol. 1996, 80, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Kubo, I.; Muroi, H.; Himejima, M. Antibacterial activity of totarol and its potentiation. J. Nat. Prod. 1992, 55, 1436–1440. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, K.; Evans, G.; O’Toole, P.W. Potentiation of methicillin activity against methicillin-resistant Staphylococcus aureus by diterpenes. FEMS Microbiol. Lett. 1999, 179, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Haraguchi, H.; Oike, S.; Muroi, H.; Kubo, I. Mode of antibacterial action of totarol, a diterpene from Podocarpus nagi. Planta Med. 1996, 62, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.C.; Kaatz, G.W.; Seo, S.M.; Wareham, N.; Williamson, E.M.; Gibbons, S. The phenolic diterpene totarol inhibits multidrug efflux pump activity in Staphylococcus aureus. Antimicrob. Agents Chemother. 2007, 51, 4480–4483. [Google Scholar] [CrossRef] [PubMed]
- Micol, V.; Mateo, C.R.; Shapiro, S.; Aranda, F.J.; Villalain, J. Effects of (+)-totarol, a diterpenoid antibacterial agent, on phospholipid model membranes. Biochim. Biophys. Acta 2001, 1511, 281–290. [Google Scholar] [CrossRef]
- Jaiswal, R.; Beuria, T.K.; Mohan, R.; Mahajan, S.K.; Panda, D. Totarol Inhibits Bacterial Cytokinesis by Perturbing the Assembly Dynamics of FtsZ. Biochemistry 2007, 46, 4211–4220. [Google Scholar] [CrossRef] [PubMed]
- Haraguchi, H.; Ishikawa, H.; Kubo, I. Antioxidative action of diterpenoids from Podocarpus nagi. Planta Med. 1997, 63, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Reinbold, J.; Hierlemann, T.; Hinkel, H.; Muller, I.; Maier, M.E.; Weindl, T.; Schlensak, C.; Wendel, H.P.; Krajewski, S. Development and in vitro characterization of poly(lactide-co-glycolide) microspheres loaded with an antibacterial natural drug for the treatment of long-term bacterial infections. Drug Des. Dev. Ther. 2016, 10, 2823–2832. [Google Scholar] [PubMed]
- Watanabe, A.; Kohnoe, S.; Shimabukuro, R.; Yamanaka, T.; Iso, Y.; Baba, H.; Higashi, H.; Orita, H.; Emi, Y.; Takahashi, I.; et al. Risk factors associated with surgical site infection in upper and lower gastrointestinal surgery. Surg. Today 2008, 38, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Engelsman, A.F.; van der Mei, H.C.; Ploeg, R.J.; Busscher, H.J. The phenomenon of infection with abdominal wall reconstruction. Biomaterials 2007, 28, 2314–2327. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.; Sethu, S.; Nayak, S.; Mohan, L.; Morsi, Y.Y.; Manivasagam, G. Suture materials—Current and emerging trends. J. Biomed. Mater. Res. Part A 2016, 104, 1544–1559. [Google Scholar] [CrossRef] [PubMed]
- Zimmerli, W.; Waldvogel, F.A.; Vaudaux, P.; Nydegger, U.E. Pathogenesis of foreign body infection: Description and characteristics of an animal model. J. Infect. Dis. 1982, 146, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Justinger, C.; Moussavian, M.R.; Schlueter, C.; Kopp, B.; Kollmar, O.; Schilling, M.K. Antibacterial [corrected] coating of abdominal closure sutures and wound infection. Surgery 2009, 145, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Yueh, M.F.; Tukey, R.H. Triclosan: A Widespread Environmental Toxicant with Many Biological Effects. Annu. Rev. Pharmacol. Toxicol. 2016, 56, 251–272. [Google Scholar] [CrossRef] [PubMed]
- Calafat, A.M.; Ye, X.; Wong, L.Y.; Reidy, J.A.; Needham, L.L. Urinary concentrations of triclosan in the U.S. population: 2003–2004. Environ. Health Perspect. 2008, 116, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Zhao, X.; Li, W.; Meng, R.; Liu, Z.; Liu, M.; Guo, N.; Yu, L. Inhibitory effect of totarol on exotoxin proteins hemolysin and enterotoxins secreted by Staphylococcus aureus. World J. Microbiol. Biotechnol. 2015, 31, 1565–1573. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Kumar, K.N.; Dabkowski, J.M.; Corrigan, M.; Scott, R.W.; Nusslein, K.; Tew, G.N. New bactericidal surgical suture coating. Langmuir 2012, 28, 12134–12139. [Google Scholar] [CrossRef] [PubMed]
- Makadia, H.K.; Siegel, S.J. Poly Lactic-co-Glycolic Acid (PLGA) as Biodegradable Controlled Drug Delivery Carrier. Polymers 2011, 3, 1377–1397. [Google Scholar] [CrossRef] [PubMed]
- Dhas, S.P.; Anbarasan, S.; Mukherjee, A.; Chandrasekaran, N. Biobased silver nanocolloid coating on silk fibers for prevention of post-surgical wound infections. Int. J. Nanomed. 2015, 10 (Suppl. 1), 159–170. [Google Scholar]
- Meghil, M.M.; Rueggeberg, F.; El-Awady, A.; Miles, B.; Tay, F.; Pashley, D.; Cutler, C.W. Novel Coating of Surgical Suture Confers Antimicrobial Activity Against Porphyromonas gingivalis and Enterococcus faecalis. J. Periodontol. 2015, 86, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Obermeier, A.; Schneider, J.; Fohr, P.; Wehner, S.; Kuhn, K.D.; Stemberger, A.; Schieker, M.; Burgkart, R. In vitro evaluation of novel antimicrobial coatings for surgical sutures using octenidine. BMC Microbiol. 2015, 15. [Google Scholar] [CrossRef] [PubMed]
Sample Availability: Not available. |









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Monofilament Sutures | m (Totarol) in Solution (mg/mL) | m (PLGA) in Solution (mg/mL) | Calculated Value Totarol Applied (µg/cm) | Calculated Value PLGA Applied (µg/cm) |
|---|---|---|---|---|
| 1 | 25 | --- | 28.9 | --- |
| 2 | 25 | 25 | 44 | 44 |
| 3 | 25 | 50 | 28.9 | 57.8 |
| 4 | 25 | 75 | 23.3 | 70 |
| 5 | 100 | --- | 156.7 | --- |
| 6 | 100 | 25 | 107.6 | 26.9 |
| 7 | 100 | 50 | 106 | 53 |
| 8 | 100 | 75 | 117.5 | 88.1 |
| 9 | --- | 75 | --- | 137.1 |
| Multifilament Sutures | ||||
| 1 | 25 | --- | 35.6 | --- |
| 2 | 25 | 25 | 28.9 | 28.9 |
| 3 | 25 | 50 | 24.4 | 48.9 |
| 4 | 25 | 75 | 37.2 | 111.7 |
| 5 | 100 | --- | 111.1 | --- |
| 6 | 100 | 25 | 98.7 | 24.7 |
| 7 | 100 | 50 | 128.2 | 64.1 |
| 8 | 100 | 75 | 113.6 | 85.2 |
| 9 | --- | 75 | --- | 190 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reinbold, J.; Uhde, A.-K.; Müller, I.; Weindl, T.; Geis-Gerstorfer, J.; Schlensak, C.; Wendel, H.-P.; Krajewski, S. Preventing Surgical Site Infections Using a Natural, Biodegradable, Antibacterial Coating on Surgical Sutures. Molecules 2017, 22, 1570. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules22091570
Reinbold J, Uhde A-K, Müller I, Weindl T, Geis-Gerstorfer J, Schlensak C, Wendel H-P, Krajewski S. Preventing Surgical Site Infections Using a Natural, Biodegradable, Antibacterial Coating on Surgical Sutures. Molecules. 2017; 22(9):1570. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules22091570
Chicago/Turabian StyleReinbold, Jochen, Ann-Kristin Uhde, Ingrid Müller, Tobias Weindl, Jürgen Geis-Gerstorfer, Christian Schlensak, Hans-Peter Wendel, and Stefanie Krajewski. 2017. "Preventing Surgical Site Infections Using a Natural, Biodegradable, Antibacterial Coating on Surgical Sutures" Molecules 22, no. 9: 1570. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules22091570