
Revisiting Therapeutic Strategies for H. pylori Treatment in the Context of Antibiotic Resistance: Focus on Alternative and Complementary Therapies



Abstract
:1. Introduction
2. Prevalence and Risk Factors Relevant for Therapeutical Support
2.1. Prevalence of H. pylori Related to Different Geographic Areas and Global Population
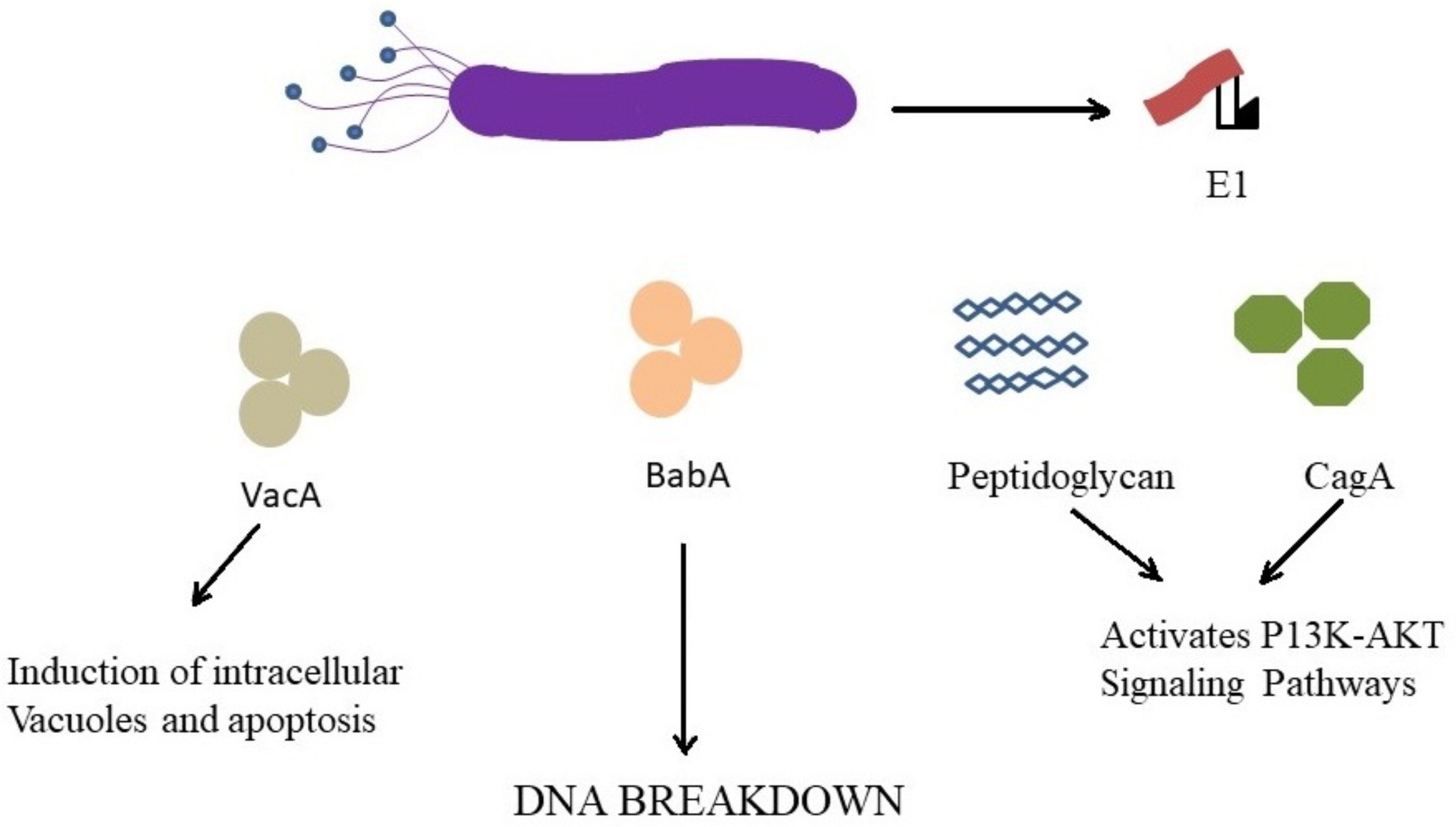
2.2. Risk Factors: Oncogenicity
3. Current Treatment Regimens for H. pylori Infections
3.1. Clarithromycin Triple Therapy
3.2. Bismuth Quadruple Therapy. Non-Bismuth-Based Quadruple Therapy
3.3. Rifabutin-Based Triple Therapy
3.4. Fluoroquinolone Therapy
3.5. Potassium-Competitive Acid Blockers (P-CABs)
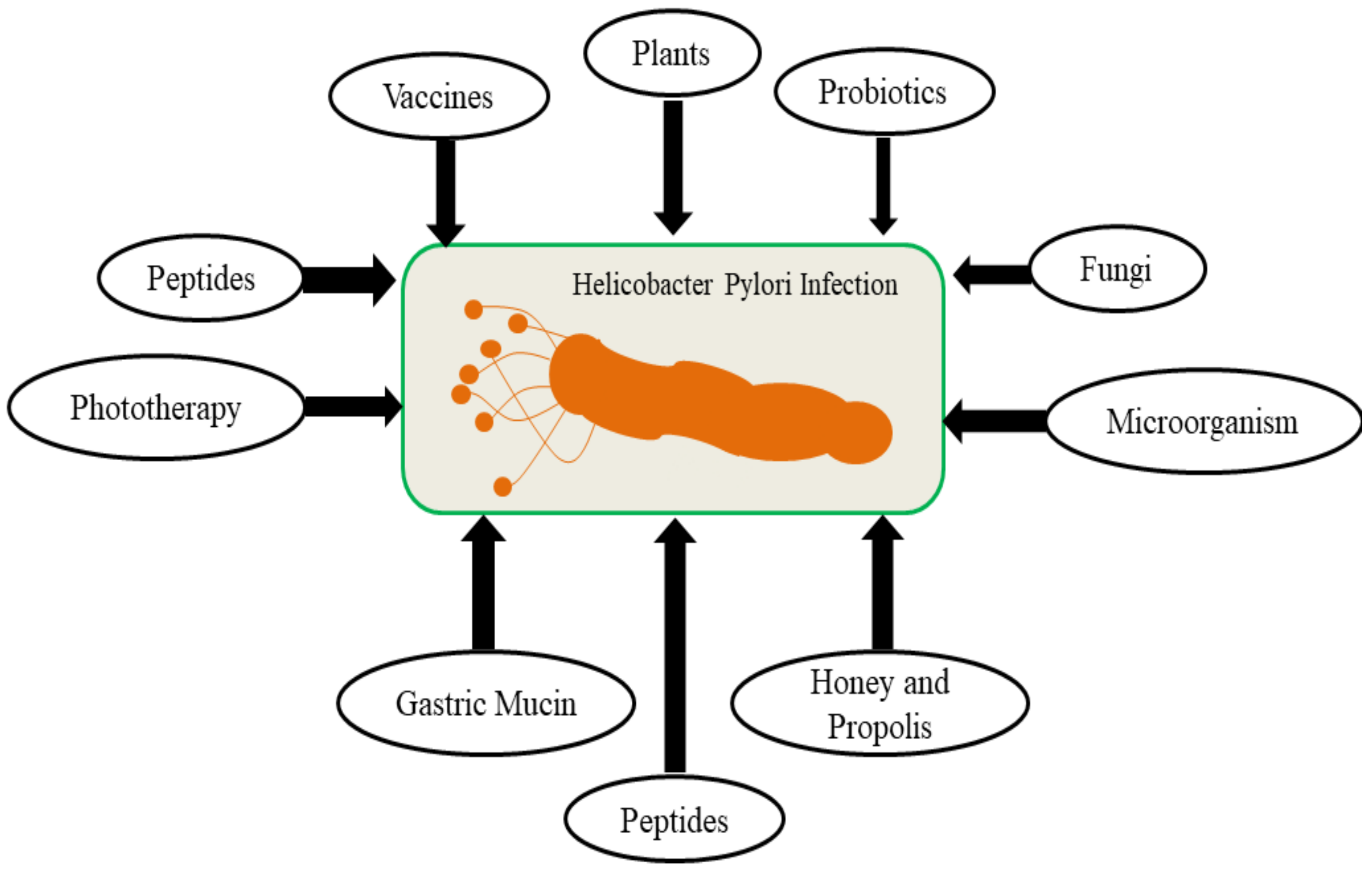
4. Antibiotic Resistance and Alternative Therapy
4.1. Role of Propolis in Treatment of H. pylori Mediated GIT Diseases
4.1.1. Anti-Inflammatory Effect of Propolis
4.1.2. Antioxidant Effect of Propolis
4.2. Role of Curcumin in Treatment of H. pylori Mediated GIT Diseases
4.2.1. Antioxidant Effect of Curcumin
4.2.2. Anti-Inflammatory Effect of Curcumin
4.2.3. Anti-Carcinogenic Effect of Curcumin
4.2.4. Anti-Microbial Effect of Curcumin
4.3. Role of Ginseng in Treatment of H. pylori Mediated GIT Diseases
4.4. Role of Garlic in Treatment of H. pylori Mediated GIT Diseases
5. Nanotechnology-Based Approach against H. pylori Infections
5.1. Role of Biologically Synthesized Silver Nanoparticles
5.2. Other Nanoparticles Formulations for H. pylori Mediated GIT
5.2.1. Polymeric Nanoparticles Encapsulating Drugs and Other Therapeutic Agents
5.2.2. Liposomal Formulations against H. pylori
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kandulski, A.; Selgrad, M.; Malfertheiner, P. Helicobacter pylori infection: A clinical overview. Dig. Liver Dis. 2008, 40, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Chung, J.W. Best Helicobacter pylori Eradication Strategy in the Era of Antibiotic Resistance. Antibiotics 2020, 9, 436. [Google Scholar] [CrossRef] [PubMed]
- De Reuse, H.; Skouloubris, S. Nitrogen Metabolism. In Helicobacter pylori: Physiology and Genetics; Mobley, H.L.T., Mendz, G.L., Hazell, S.L., Eds.; ASM Press: Washington, DC, USA, 2001; Chapter 11. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK2412/ (accessed on 1 August 2021).
- Weeks, D.L.; Eskandari, S.; Scott, D.R.; Sachs, G. A H+-gated urea channel: The link between Helicobacter pylori urease and gastric colonization. Science 2000, 287, 482–485. [Google Scholar] [CrossRef] [Green Version]
- Quintero, M.J.; Muro-Pastor, A.M.; Herrero, A.; Flores, E. Arginine catabolism in the cyanobacterium Synechocystis sp. strain PCC6803 involves the urea cycle and arginase pathway. J. Bacteriol. 2000, 182, 1008–1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreiber, S.; Konradt, M.; Groll, C.; Scheid, P.; Hanauer, G.; Werling, H.O.; Josenhans, C.; Suerbaum, S. The spatial orientation of Helicobacter pylori in the gastric mucus. Proc. Natl. Acad. Sci. USA 2004, 101, 5024–5029. [Google Scholar] [CrossRef] [Green Version]
- Eaton, K.A.; Morgan, D.R.; Krakowka, S. Campylobacter pylori virulence factors in gnotobiotic piglets. Infect. Immun. 1989, 57, 1119–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomb, J.F.; White, O.; Kerlavage, A.R.; Clayton, R.A.; Sutton, G.G.; Fleischmann, R.D.; Ketchum, K.A.; Klenk, H.P.; Gill, S.; Dougherty, B.A.; et al. The complete genome sequence of the gastric pathogen Helicobacter pylori. Nature 1997, 388, 539–547, Erratum in Nature 1997, 389, 412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labigne, A.; De Reuse, H. Determinants of Helicobacter pylori pathogenicity. Infect. Agents Dis. 1996, 191–202. [Google Scholar] [CrossRef] [Green Version]
- Hatakeyama, M.; Higashi, H. Helicobacter pylori CagA: A new paradigm for bacterial carcinogenesis. Cancer Sci. 2005, 96, 835–843. [Google Scholar] [CrossRef]
- Roszczenko-Jasińska, P.; Wojtyś, M.I.; Jagusztyn-Krynicka, E.K. Helicobacter pylori treatment in the post-antibiotics era-searching for new drug targets. Appl. Microbiol. Biotechnol. 2020, 104, 9891–9905. [Google Scholar] [CrossRef]
- Tshibangu-Kabamba, E.; Yamaoka, Y. Helicobacter pylori infection and antibiotic resistance from biology to clinical implications. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 613–629. [Google Scholar] [CrossRef]
- WHO. Global Priority List of Antibiotic-Resistant Bacteria to Guide Research, Discovery, and Development of New Antibiotics. 2017. Available online: https://www.who.int/medicines/publications/WHO-PPL-Short_Summary_25Feb-ET_NM_WHO.pdf (accessed on 1 August 2021).
- Gerrits, M.; H M van Vliet, A.; Kuipers, E.; Kusters, J.G. Helicobacter pylori and antimicrobial resistance: Molecular mechanisms and clinical implications. Lancet Infect. Dis. 2006, 6, 699–709. [Google Scholar] [CrossRef]
- Thung, I.; Aramin, H.; Vavinskaya, V.; Gupta, S.; Park, J.Y.; Crowe, S.E.; Valasek, M.A. Review article: The global emergence of Helicobacter pylori antibiotic resistance. Aliment. Pharmacol. Ther. 2016, 43, 514–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyssen, O.P.; Bordin, D.; Tepes, B.; Pérez-Aisa, Á.; Vaira, D.; Caldas, M.; Bujanda, L.; Castro-Fernandez, M.; Lerang, F.; Leja, M.; et al. European Registry on Helicobacter pylori management (Hp-EuReg): Patterns and trends in first-line empirical eradication prescription and outcomes of 5 years and 21 533 patients. Gut 2021, 70, 40–54. [Google Scholar] [CrossRef]
- Zamani, M.; Ebrahimtabar, F.; Zamani, V.; Miller, W.H.; Alizadeh-Navaei, R.; Shokri-Shirvani, J.; Derakhshan, M.H. Systematic review with meta-analysis: The worldwide prevalence of Helicobacter pylori infection. Aliment. Pharmacol. Ther. 2018, 47, 868–876. [Google Scholar] [CrossRef] [Green Version]
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.; Wu, J.C.Y.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef] [Green Version]
- Sjomina, O.; Pavlova, J.; Niv, Y.; Leja, M. Epidemiology of Helicobacter pylori infection. Helicobacter 2018, 23, e12514. [Google Scholar] [CrossRef] [Green Version]
- Rowland, M.; Daly, L.; Vaughan, M.; Higgins, A.; Bourke, B.; Drumm, B. Age-specific incidence of Helicobacter pylori. Gastroenterology 2006, 130, 65–72; quiz 211. [Google Scholar] [CrossRef] [PubMed]
- Aguilera Matos, I.; Diaz Oliva, S.E.; Escobedo, A.A.; Villa Jiménez, O.M.; Velazco Villaurrutia, Y.D.C. Helicobacter pylori infection in children. BMJ Paediatr. Open 2020, 4, e000679. [Google Scholar] [CrossRef] [PubMed]
- Hoda, M.M.; Nancy, D.L.; David, Y.G.; Ramchatesingh, J.E. Helicobacter pylori Infection in Preschool and School-Aged Minority Children: Effect of Socioeconomic Indicators and Breast-Feeding Practices. Clin. Infect. Dis. 2001, 32, 1387–1392. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.E.; Austin, S.; Dale, A.; McClean, P.; Harding, M.; Coward, W.A.; Weaver, L.T. Protection by human milk IgA against Helicobacter pylori infection in infancy. Lancet 1993, 342, 121. [Google Scholar] [CrossRef]
- Sasaki, K.; Tajiri, Y.; Sata, M.; Fujii, Y.; Matsubara, F.; Zhao, M.G.; Shimizu, S.; Toyonaga, A.; Tanikawa, K. Helicobacter pylori in the natural environment. Scand. J. Infect. Dis. 1999, 31, 275–280. [Google Scholar]
- Velazquez, M.; Feirtag, J.M. Helicobacter pylori: Characteristics, pathogenicity, detection methods and mode of transmission implicating foods and water. Int. J. Food Microbiol. 1999, 53, 95–104. [Google Scholar] [CrossRef]
- Ansorg, R.; Vonheinegg, E.H.; Vonrecklinghausen, G. Cat owner’s risk of acquiring a Helicobacter pylori infection. Zentralbl. Bakteriol. Int. J. Med. Microbiol. Vir. Parasitol. Infect. Dis. 1995, 283, 122–126. [Google Scholar]
- Fox, J.G. Non-human reservoirs of Helicobacter pylori. Aliment. Pharmacol. Ther. 1995, 9, 93–103. [Google Scholar] [PubMed]
- Dore, M.P.; Bilotta, M.; Vaira, D.; Mancal, A.; Massarelli, G.; Leandro, G.; Atzei, A.; Pisanu, G.; Graham, D.Y.; Realdi, G. High prevalence of Helicobacter pylori infection in shepherds. Dig. Dis. Sci. 1999, 44, 1161–1164. [Google Scholar] [CrossRef] [PubMed]
- Goodman, K.J.; Correa, P. Transmission of Helicobacter pylori among siblings. Lancet 2000, 355, 358–362. [Google Scholar] [CrossRef]
- O’Connor, A.; O′Morain, C. Helicobacter pylori infection in Europe: Current perspectives. Expert Rev. Gastroenterol. Hepatol. 2013, 7, 541–548. [Google Scholar] [CrossRef]
- Kouitcheu Mabeku, L.B.; Noundjeu Ngamga, M.L.; Leundji, H. Potential risk factors and prevalence of Helicobacter pylori infection among adult patients with dyspepsia symptoms in Cameroon. BMC Infect. Dis. 2018, 18, 278. [Google Scholar] [CrossRef]
- Ogihara, A.; Kikuchi, S.; Hasegawa, A.; Kurosawa, M.; Miki, K.; Kaneko, E.; Mizukoshi, H. Relationship between Helicobacter pylori infection, smoking and drinking habits. J. Gastroenterol. Hepatol. 2000, 15, 271–276. [Google Scholar]
- Tonkic, A.; Tonkic, M.; Lehours, P.; Mégraud, F. Epidemiology and diagnosis of Helicobacter pylori infection. Helicobacter 2012, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Haley, K.P.; Gaddy, J.A. Nutrition and Helicobacter pylori: Host Diet and Nutritional Immunity Influence Bacterial Virulence and Disease Outcome. Gastroenterol. Res. Pract. 2016, 2016, 3019362. [Google Scholar] [CrossRef] [Green Version]
- Setiawan, V.W.; Zhang, Z.-F.; Yu, G.-P.; Lu, Q.Y.; Li, Y.L.; Lu, M.L.; Wang, M.R.; Guo, C.H.; Yu, S.Z.; Kurtz, R.C.; et al. Protective effect of green tea on the risks of chronic gastritis and stomach cancer. Int. J. Cancer 2001, 92, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Lunet, N.; Lacerda-Vieira, A.; Barros, H. Fruit and vegetables consumption and gastric cancer: A systematic review and meta-analysis of cohort studies. Nutr. Cancer 2005, 53, 1–10. [Google Scholar] [CrossRef]
- Jarosz, M.; Dzieniszewski, J.; Dabrowska-Ufniarz, E.; Wartanowicz, M.; Ziemlanski, S.; Reed, P.I. Effects of high dose vitamin C treatment on Helicobacter pylori infection and total vitamin C concentration in gastric juice. Eur. J. Cancer Prev. 1998, 7, 449–454. [Google Scholar] [CrossRef]
- Venneman, K.; Huybrechts, I.; Gunter, M.J.; Vandendaele, L.; Herrero, R.; Van Herck, K. The epidemiology of Helicobacter pylori infection in Europe and the impact of lifestyle on its natural evolution toward stomach cancer after infection: A systematic review. Helicobacter 2018, 23, e12483. [Google Scholar] [CrossRef]
- Noto, J.M.; Gaddy, J.A.; Lee, J.Y. Iron deficiency accelerates Helicobacter pylori-induced carcinogenesis in rodents and humans. J. Clin. Investig. 2013, 123, 479–492. [Google Scholar] [CrossRef] [Green Version]
- Ghoshal, U.C.; Tiwari, S.; Dhingra, S. Frequency of Helicobacter pylori and CagA antibody in patients with gastric neoplasms and controls: The Indian enigma. Dig. Dis. Sci. 2008, 53, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- Khoder, G.; Muhammad, J.S.; Mahmoud, I.; Soliman, S.S.M.; Burucoa, C. Prevalence of Helicobacter pylori and Its Associated Factors among Healthy Asymptomatic Residents in the United Arab Emirates. Pathogens 2019, 8, 44. [Google Scholar] [CrossRef] [Green Version]
- World Cancer Research Fund; American Institute for Cancer Research (WCRF/AICR). Continuous Update Project Report: Diet, Nutrition, Physical Activity and Stomach Cancer. World Cancer Research Fund International: London, UK, 2016. Revised 2018. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/stomach-cancer-report.pdf (accessed on 1 August 2021).
- Ibrahim, A.; Morais, S.; Ferro, A.; Lunet, N.; Peleteiro, B. Sex-differences in the prevalence of Helicobacter pylori infection in pediatric and adult populations: Systematic review and meta-analysis of 244 studies. Dig. Liver Dis. 2017, 49, 742–749. [Google Scholar] [CrossRef]
- Kim, H.J.; Choi, B.Y.; Byun, T.J.; Eun, C.S.; Song, K.S.; Kim, Y.S.; Han, D.S. The prevalence of atrophic gastritis and intestinal metaplasia according to gender, age and Helicobacter pylori infection in a rural population. J. Prev. Med. Public Health 2008, 41, 373–379. [Google Scholar] [CrossRef]
- Prashanth, R.; Barsouk, A. Epidemiology of gastric cancer: Global trends, risk factors and prevention. Prz. Gastroenterol. 2019, 14, 26–38. [Google Scholar]
- Muzaheed. Helicobacter pylori Oncogenicity: Mechanism, Prevention, and Risk Factors. Sci. World J. 2020, 10. [Google Scholar] [CrossRef]
- Saka, K.Y.; Nimura, S. Endoscopic and histological features of gastric cancers after successful Helicobacter pylori eradication therapy. Gastric Cancer 2016, 19, 524–530. [Google Scholar] [CrossRef]
- Setia, N.; Clark, J.W.; Duda, D.G.; Hong, T.S.; Kwak, E.L.; Mullen, J.T.; Lauwers, G.Y. Familial gastric cancers. Oncologist 2015, 20, 1365–1377. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.J.; Kim, N. Gastric cancer and family history. Korean J. Intern. Med. 2016, 31, 1042–1053. [Google Scholar] [CrossRef]
- Sasazuki, S.; Sasaki, S.; Tsugane, S. Cigarette smoking, alcohol consumption and subsequent gastric cancer risk by subsite and histologic type. Inter. J. Cancer 2002, 101, 560–566. [Google Scholar] [CrossRef]
- Wroblewski, L.E.; Peek, R.M.; Wilson, K.T. Helicobacter pylori and gastric cancer: Factors that modulate disease risk. Clin. Microbiol. Rev. 2010, 3, 713–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watari, J.; Chen, N.; Amenta, P.S.; Fukui, H.; Oshima, T.; Tomita, T.; Miwa, H.; Lim, K.J.; Das, K.M. Helicobacter pylori associated chronic gastritis, clinical syndromes, precancerous lesions, and pathogenesis of gastric cancer development. World J. Gastroenterol. 2014, 20, 5461–5473. [Google Scholar] [CrossRef] [PubMed]
- Stolte, M.; Bayerdörffer, E.; Morgner, A.; Alpen, B.; Wündisch, T.; Thiede, C.; Neubauer, A. Helicobacter and gastric MALT lymphoma. Gut 2002, 50, 3. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Shiotani, A.; Graham, D.Y. Current and Future Treatment of Helicobacter pylori Infections. Adv. Exp. Med. Biol. 2019, 1149, 211–225. [Google Scholar]
- Yang, J.C.; Lin, C.J. CYP2C19 genotypes in the pharmacokinetics/pharmacodynamics of proton pump inhibitor-based therapy of Helicobacter pylori infection. Expert Opin. Drug Metab. Toxicol. 2010, 6, 29–41. [Google Scholar] [CrossRef]
- Han, H.S.; Lee, S.Y. Correlations of the Gastric and Duodenal Microbiota with Histological, Endoscopic, and Symptomatic Gastritis. J. Clin. Med. 2019, 8, 312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nezami, B.G.; Jani, M.; Alouani, D.; Rhoads, D.D.; Sadri, N. Helicobacter pylori Mutations Detected by Next-Generation Sequencing in Formalin-Fixed, Paraffin-Embedded Gastric Biopsy Specimens Are Associated with Treatment Failure. J. Clin. Microbiol. 2019, 57, e01834-18. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, R.M.; Pereira-Marques, J.; Pinto-Ribeiro, I.; Costa, J.L.; Carneiro, F.; Machado, J.C.; Figueiredo, C. Gastric microbial community profiling reveals a dysbiotic cancer-associated microbiota. Gut 2018, 67, 226–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. European Helicobacter and Microbiota Study Group and Consensus panel. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chey, W.D.; Wong, B.C. American College of Gastroenterology guideline on the management of Helicobacter pylori infection. Am. J. Gastroenterol. 2007, 102, 1808–1825. [Google Scholar] [CrossRef]
- Miftahussurur, M.; Cruz, M.; Subsomwong, P.; Jiménez Abreu, J.A.; Hosking, C.; Nagashima, H.; Akada, J.; Yamaoka, Y. Clarithromycin-Based Triple Therapy is Still Useful as an Initial Treatment for Helicobacter pylori Infection in the Dominican Republic. Am. J. Trop. Med. Hyg. 2017, 96, 1050–1059. [Google Scholar] [CrossRef] [Green Version]
- Gebeyehu, E.; Nigatu, D.; Engidawork, E. Helicobacter pylori eradication rate of standard triple therapy and factors affecting eradication rate at Bahir Dar city administration, Northwest Ethiopia: A prospective follow up study. PLoS ONE 2019, 14, e0217645. [Google Scholar] [CrossRef] [Green Version]
- Graham, D.Y.; Fischbach, L. Helicobacter pylori treatment in the era of increasing antibiotic resistance. Gut 2010, 59, 1143–1153. [Google Scholar] [CrossRef]
- Chung, J.W.; Han, J.P.; Kim, K.O.; Kim, S.Y.; Hong, S.J.; Kim, T.H.; Kim, C.W.; Kim, J.S.; Kim, B.W.; Bang, B.W.; et al. Ten-day empirical sequential or concomitant therapy is more effective than triple therapy for Helicobacter pylori eradication: A multicenter, prospective study. Dig. Liver. Dis. 2016, 48, 888–892. [Google Scholar] [CrossRef]
- Park, S.M.; Kim, J.S.; Kim, B.W.; Ji, J.S.; Choi, H. Randomized clinical trial comparing 10- or 14-day sequential therapy and 10- or 14-day concomitant therapy for the first line empirical treatment of Helicobacter pylori infection. J. Gastroenterol. Hepatol. 2017, 32, 589–594. [Google Scholar] [CrossRef]
- Ang, T.L.; Fock, K.M.; Song, M.; Ang, D.; Kwek, A.B.; Ong, J.; Tan, J.; Teo, E.K.; Dhamodaran, S. Ten-day triple therapy versus sequential therapy versus concomitant therapy as first-line treatment for Helicobacter pylori infection. J. Gastroenterol. Hepatol. 2015, 30, 1134–1139. [Google Scholar] [CrossRef]
- McNicholl, A.G.; Marin, A.C.; Molina-Infante, J.; Castro, M.; Barrio, J.; Ducons, J.; Calvet, X.; de la Coba, C.; Montoro, M.; Bory, F.; et al. Randomised clinical trial comparing sequential and concomitant therapies for Helicobacter pylori eradication in routine clinical practice. Gut 2014, 63, 244–249. [Google Scholar] [CrossRef]
- Gatta, L.; Vakil, N.; Vaira, D.; Scarpignato, C. Global eradication rates for Helicobacter pylori infection: Systematic review and meta-analysis of sequential therapy. BMJ 2013, 347, f4587. [Google Scholar] [CrossRef] [Green Version]
- He, L.; Deng, T.; Luo, H. Meta-analysis of sequential, concomitant and hybrid therapy for Helicobacter pylori eradication. Intern. Med. 2015, 54, 703–710. [Google Scholar] [CrossRef] [Green Version]
- Malfertheiner, P.; Selgrad, M. Helicobacter pylori infection and current clinical areas of contention. Curr. Opin. Gastroenterol. 2010, 26, 618–623. [Google Scholar] [CrossRef] [PubMed]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Y.; Zhu, Y.; Lu, N.H. Novel and Effective Therapeutic Regimens for Helicobacter pylori in an Era of Increasing Antibiotic Resistance. Front. Cell Infect. Microbiol. 2017, 5, 168. [Google Scholar] [CrossRef]
- Fallone, C.A.; Moss, S.F.; Malfertheiner, P. Reconciliation of Recent Helicobacter pylori Treatment Guidelines in a Time of Increasing Resistance to Antibiotics. Gastroenterology 2019, 157, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.I.; Tsai, F.W.; Kao, S.S.; Hsu, W.H.; Cheng, J.S.; Peng, N.J.; Tsai, K.W.; Hu, H.M.; Wang, Y.K.; Chuah, S.K.; et al. Ten-day quadruple therapy comprising proton pump inhibitor, bismuth, tetracycline, and levofloxacin is more effective than standard levofloxacin triple therapy in the second-line treatment of Helicobacter pylori infection: A randomized controlled trial. Am. J. Gastroenterol. 2017, 112, 1374–1381. [Google Scholar] [CrossRef] [PubMed]
- Macias-Garcia, F.; Baston-Rey, I.; de la Iglesia-Garcia, D.; Calvino-Suarez, C.; Nieto-Garcia, L.; Dominguez-Munoz, J.E. Bismuth-containing quadruple therapy versus concomitant quadruple therapy as first-line treatment for Helicobacter pylori infection in an area of high resistance to clarithromycin: A prospective, cross-sectional, comparative, open trial. Helicobacter 2019, 24, e12546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, D.Y.; Lee, S.Y. How to Effectively Use Bismuth Quadruple Therapy: The Good, the Bad, and the Ugly. Gastroenterol. Clin. N. Am. 2015, 44, 537–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borsch, G.M.; Graham, D.Y. Helicobacter pylori. In Pharmacology of Peptic Ulcer Disease; Collen, M.J., Benjamin, S.B., Eds.; Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 1991; pp. 107–148. [Google Scholar]
- Xie, Y.; Pan, X.; Li, Y.; Wang, H.; Du, Y.; Xu, J.; Wang, J.; Zeng, Z.; Chen, Y.; Zhang, G. New single capsule of bismuth, metronidazole and tetracycline given with omeprazole versus quadruple therapy consisting of bismuth, omeprazole, amoxicillin and clarithromycin for eradication of Helicobacter pylori in duodenal ulcer patients: A Chinese prospective, randomized, multicentre trial. J. Antimicrob. Chemother. 2018, 73, 1681–1687. [Google Scholar] [PubMed]
- Fiorini, G.; Zullo, A.; Saracino, I.M.; Gatta, L.; Pavoni, M.; Vaira, D. Pylera and sequential therapy for first-line Helicobacter pylori eradication: A culture-based study in real clinical practice. Eur. J. Gastroenterol. Hepatol. 2018, 30, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Andreev, D. Helicobacter pylori Eradication Therapy: Current Regimens. Adv. Res. Gastroenterol. Hepatol. 2017, 7, 555710. [Google Scholar] [CrossRef]
- Gisbert, J.P.; Calvet, X. Update on non-bismuth quadruple (concomitant) therapy for eradication of Helicobacter pylori. Clin. Exp. Gastroenterol. 2012, 5, 23–34. [Google Scholar] [CrossRef] [Green Version]
- Gisbert, J.P.; Calvet, X. Review article: Rifabutin in the treatment of refractory Helicobacter pylori infection. Aliment. Pharmacol. Ther. 2012, 35, 209–221. [Google Scholar] [CrossRef]
- Bock, H.M.D.; Koop, H.M.D.; Lehn, N.M.D.; Heep, M.M.D. Rifabutin-based Triple Therapy After Failure of Helicobacter pylori Eradication Treatment: Preliminary Experience. J. Clin. Gastroenterol. 2000, 31, 222–225. [Google Scholar] [CrossRef]
- Ribaldone, D.G.; Fagoonee, S.; Astegiano, M. Rifabutin-Based Rescue Therapy for Helicobacter pylori Eradication: A Long-Term Prospective Study in a Large Cohort of Difficult-to-Treat Patients. J. Clin. Med. 2019, 8, 199. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Chen, C.Y.; Wang, X.T.; Lyu, B. Levofloxacin-based triple therapy versus bismuth-based quadruple therapy in the treatment of Helicobacter pylori as the rescue therapy: A meta analysis. Zhonghua Nei Ke Za Zhi 2017, 56, 368–374. [Google Scholar]
- Glocker, E.; Stueger, H.P.; Kist, M. Quinolone resistance in Helicobacter pylori isolates in Germany. Antimicrob. Agents Chemother. 2007, 51, 346–349. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.M.; Kim, N.; Lee, D.H.; Park, Y.S.; Kim, Y.R.; Kim, J.S. Second-line treatment for Helicobacter pylori infection: 10-day moxifloxacin-based triple therapy versus 2-week quadruple therapy. Helicobacter 2007, 12, 623–628. [Google Scholar] [CrossRef]
- Nista, E.C.; Candelli, M.; Zocco, M.A.; Cazzato, I.A.; Cremonini, F.; Ojetti, V. Moxifloxacin-based strategies for first-line treatment of Helicobacter pylori infection. Aliment. Pharmacol. 2005, 21, 1241–1247. [Google Scholar] [CrossRef] [PubMed]
- Berning, M.; Krasz, S.; Miehlke, S. Should quinolones come first in Helicobacter pylori therapy? Therap. Adv. Gastroenterol. 2011, 4, 103–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, V.K.; Dhar, A.; Srinivasan, S.; Rattan, A.; Sharma, M.P. Eradication of H. pylori in a developing country: Comparison of lansoprazole versus omeprazole with norfloxacin, in a dual-therapy study. Am. J. Gastroenterol. 1997, 92, 1140–1142. [Google Scholar] [PubMed]
- Zaidi, S.F.; Muhammad, J.S.; Usmanghani, K.; Sugiyama, T. Pharmacological ins and outs of medicinal plants against Helicobacter pylori: A review. Pak. J. Pharm. Sci. 2015, 2, 28. [Google Scholar]
- Hunt, R.H.; Scarpignato, C. Potassium-Competitive Acid Blockers (P-CABs): Are They Finally Ready for Prime Time in Acid-Related Disease? Clin. Transl. Gastroenterol. 2015, 6, e119. [Google Scholar] [CrossRef]
- Tanabe, H.; Ando, K.; Sato, K.; Ito, T.; Goto, M.; Sato, T.; Fujinaga, A.; Kawamoto, T.; Utsumi, T.; Yanagawa, N. Efficacy of Vonoprazan-Based Triple Therapy for Helicobacter pylori Eradication: A Multicenter Study and a Review of the Literature. Dig. Dis. Sci. 2017, 62, 3069–3076. [Google Scholar] [CrossRef]
- Njume, C.; Afolayan, A.J.; Ndip, R.N. An overview of antimicrobial resistance and the future of medicinal plants in the treatment of Helicobacter pylori infections. Afr. J. Pharm. Pharmacol. 2009, 3, 685–699. [Google Scholar]
- Safavi, M.; Shams-Ardakani, M.; Foroumadi, A. Medicinal plants in the treatment of Helicobacter pylori infections. Pharm. Biol. 2015, 53, 939–960. [Google Scholar] [CrossRef]
- O’Gara, E.A.; Hill, D.J.; Maslin, D.J. Activities of garlic oil, garlic powder, and their diallyl constituents against Helicobacter pylori. Appl. Environ. Microbiol. 2000, 66, 2269–2273. [Google Scholar] [CrossRef] [Green Version]
- O’Gara, E.A.; Maslin, D.J.; Nevill, A.M.; Hill, D.J. The effect of simulated gastric environments on the anti-Helicobacter activity of garlic oil. J. Appl. Microbiol. 2007, 104, 1324–1331. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.; Zhang, X.-M. Allicin as add-on therapy for Helicobacter pylori infection: A systematic review and meta-analysis. World J. Gastroenterol. 2019, 25, 6025–6040. [Google Scholar] [CrossRef]
- Okeleye, B.I.; Bessong, P.O.; Ndip, R.N. Preliminary phytochemical screening and in vitro anti-Helicobacter pylori activity of extracts of the stem bark of Bridelia micrantha (Hochst., Baill., Euphorbiaceae). Molecules 2011, 16, 6193–6205. [Google Scholar] [CrossRef] [PubMed]
- Adefuye, A.O.; Ndip, R.N. Phytochemical analysis and antibacterial evaluation of the ethyl acetate extract of the stem bark of Bridelia micrantha. Pharmacogn. Mag. 2013, 9, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Baker, D.A. Plants against Helicobacter pylori to combat resistance: An ethnopharmacological review. Biotechnol. Rep. 2020, 26, e00470. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, P.; Rossi, G.; Tombola, F. Red wine and green tea reduce H pylori- or VacA-induced gastritis in a mouse model. World J. Gastroenterol. 2007, 13, 349–354. [Google Scholar] [CrossRef] [Green Version]
- Shoae Hassani, A.; Ordouzadeh, N.; Ghaemi, A.; Amirmozafari, N.; Hamdi, K.; Nazari, R. In vitro inhibition of Helicobacter pylori urease with non and semi fermented Camellia sinensis. Indian J. Med. Microbiol. 2009, 27, 30–34. [Google Scholar] [CrossRef]
- Boyanova, L.; Ilieva, J.; Gergova, G.; Vladimirov, B.; Nikolov, R.; Mitova, I. Honey and green/black tea consumption may reduce the risk of Helicobacter pylori infection. Diagn. Microbiol. Infect. Dis. 2015, 82, 85–86. [Google Scholar] [CrossRef] [PubMed]
- Bergonzelli, G.E.; Donnicola, D.; Porta, N.; Corthésy-Theulaz, I.E. Essential oils as components of a diet-based approach to management of Helicobacter infection. Antimicrob. Agents Chemother. 2003, 47, 3240–3246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asdaq, S.M.B.; Swathi, E.; Dhamanigi, S.S. Role of Daucus carota in Enhancing Antiulcer Profile of Pantoprazole in Experimental Animals. Molecules 2020, 25, 5287. [Google Scholar] [CrossRef] [PubMed]
- Shaik, M.A.; Aleem, A.K.; Irshad, A.; Musaddiq, M.; Khaja, S.A.; Polasa, H.; L Venkateswar, R.; Chittoor, M.H.; Leonardo, A.S.; Niyaz, A. Antimicrobial activities of Eugenol and Cinnamaldehyde against the human gastric pathogen Helicobacter pylori. Ann. Clin. Microbiol. Antimicrob. 2005, 4, 20. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.C. Medicinal plant activity on Helicobacter pylori related diseases. World J. Gastroenterol. 2014, 20, 10368–10382. [Google Scholar] [CrossRef] [PubMed]
- Shahani, S.; Monsef-Esfahani, H.R.; Saeidnia, S.; Sanie, P.; Siavoshi, F.; Foroumadi, A.; Samadi, N.; Gohari, A.R. Anti-Helicobacter pylori activity of the methanolic extract of Geum iranicum and its main compounds. Z. Naturforsch. C 2012, 67, 172–180. [Google Scholar] [CrossRef]
- De Mello Moraes, T.; Rodrigues, C.M.; Kushima, H.; Bauab, T.M.; Villegas, W.; Pellizzon, C.H.; Brito, A.R.; Hiruma-Lima, C.A. Hancornia speciosa: Indications of gastroprotective, healing and anti-Helicobacter pylori actions. J. Ethnopharmacol. 2008, 120, 161–168. [Google Scholar] [CrossRef]
- Xavier Bastos, K.; Noleto Dias, C.; Mangueira Nascimento, Y.; Sobral da Silva, M.; Zucolotto Langassner, S.M.; Wessjohann, L.A.; Fechine Tavares, J. Identification of Phenolic Compounds from Hancornia speciosa (Apocynaceae) Leaves by UHPLC Orbitrap-HRMS. Molecules 2017, 22, 143. [Google Scholar] [CrossRef] [Green Version]
- Deriu, A.; Branca, G.; Molicotti, P.; Pintore, G.; Chessa, M.; Tirillini, B.; Paglietti, B.; Mura, A.; Sechi, L.A.; Fadda, G.; et al. In vitro activity of essential oil of Myrtus communis L. against Helicobacter pylori. Inter. J. Antimicrob. Agents 2007, 30, 562–563. [Google Scholar] [CrossRef]
- Sisay, M.; Gashaw, T. Ethnobotanical, Ethnopharmacological, and Phytochemical Studies of Myrtus communis Linn: A Popular Herb in Unani System of Medicine. J. Evid.-Based Compl. Altern. Med. 2017, 22, 1035–1043. [Google Scholar] [CrossRef] [Green Version]
- Pastene, E.; Speisky, H.; García, A.; Moreno, J.; Troncoso, M.; Figueroa, G. In vitro and in vivo effects of apple peel polyphenols against Helicobacter pylori. J. Agricul. Food Chem. 2010, 58, 7172–7179. [Google Scholar] [CrossRef]
- Salehi, B.; Sharopov, F.; Martorell, M.; Rajkovic, J.; Ademiluyi, A.O.; Sharifi-Rad, M.; Fokou, P.V.T.; Martins, N.; Iriti, M.; Sharifi-Rad, J. Phytochemicals in Helicobacter pylori Infections: What Are We Doing Now? Int. J. Mol. Sci. 2018, 19, 2361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudjana, A.N.; D’Orazio, C.; Ryan, V.; Rasool, N.; Ng, J.; Islam, N.; Riley, T.V.; Hammer, K.A. Antimicrobial activity of commercial Olea europaea (olive) leaf extract. Int. J. Antimicrob. Agents 2009, 33, 461–463. [Google Scholar] [CrossRef] [PubMed]
- Lee, O.-H.; Lee, B.-Y. Antioxidant and antimicrobial activities of individual and combined phenolics in Olea europaea leaf extract. Bioresour. Technol. 2010, 101, 3751–3754. [Google Scholar] [CrossRef] [PubMed]
- Bisignano, C.; Filocamo, A.; La Camera, E.; Zummo, S.; Fera, M.T.; Mandalari, G. Antibacterial activities of almond skins on cagA-positive and-negative clinical isolates of Helicobacter pylori. BMC Microbiol. 2013, 13, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Musarra-Pizzo, M.; Ginestra, G.; Smeriglio, A.; Pennisi, R.; Sciortino, M.T.; Mandalari, G. The Antimicrobial and Antiviral Activity of Polyphenols from Almond (Prunus dulcis L.) Skin. Nutrients 2019, 11, 2355. [Google Scholar] [CrossRef] [Green Version]
- Han, J.H.; Khin, P.P.; Sohn, U.D. Effect of Rumex aquaticus herba extract against Helicobacter pylori-induced inflammation in gastric epithelial cells. J. Medic. Food 2016, 19, 31–37. [Google Scholar] [CrossRef]
- Kwak, H.; Park, S.; Nguyen, Y.T.T.; Kim, C.H.; Lee, J.M.; Suh, J.S.; Whang, W.K.; Sohn, U.D. Protective Effect of Extract from Rumex Aquaticus Herba on Ethanol-induced Gastric Damage in Rats. Pharmacology 2012, 90, 288–297. [Google Scholar] [CrossRef]
- Khanavi, M.; Safavi, M.; Siavoshi, F.; Fallah Tafti, A.; Hajimahmoodi, M.; Hadjiakhoondi, A.; Rezazadeh, S.; Foroumadi, A. Evaluation of anti-Helicobacter pylori activity of methanol extracts of some species of Stachys and Melia. J. Med. Plants 2008, 4, 74–80. [Google Scholar]
- Nostro, A.; Cellini, L.; Bartolomeo, S.D.; Cannatelli, M.A.; Campli, E.D.; Procopio, F.; Grande, R.; Marzio, L.; Alonzo, V. Effects of combining extracts (from propolis or Zingiber officinale) with clarithromycin on Helicobacter pylori. Phytother. Res. Int. J. Devoted Pharmacol. Toxicol. Eval. Nat. Prod. Deriv. 2006, 20, 187–190. [Google Scholar]
- Siddaraju, M.N.; Shylaja, M.D. Inhibition of gastric H+,K+-ATPase and Helicobacter pylori growth by phenolic antioxidants of Zingiber officinale. Mol. Nutr. Food Res. 2007, 51, 324–332. [Google Scholar] [CrossRef]
- Ebrahimzadeh Attari, V.; Somi, M.H.; Asghari Jafarabadi, M.; Ostadrahim, A.; Moaddab, S.Y.; Lotfi, N. The Gastro-protective Effect of Ginger (Zingiber officinale Roscoe) in Helicobacter pylori Positive Functional Dyspepsia. Adv. Pharm. Bull. 2019, 9, 321–324. [Google Scholar] [CrossRef]
- Sforcin, J.M.; Bankova, V. Propolis: Is there a potential for the development of new drugs? J. Ethnopharmacol. 2011, 133, 253–260. [Google Scholar] [CrossRef]
- Salatino, A.; Teixeira, E.W.; Negri, G.; Message, D. Origin and chemical variation of Brazilian propolis. Evid.-Based Complementary Altern. Med. 2005, 2, 33–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapla, U.M.; Raihan, J.I.A.; Alam, F.; Solayman, N.; Gan, S.H.; Hossen, S.; Khalil, I. Propolis: The future therapy against Helicobacter pylori-mediated gastrointestinal diseases. J. Appl. Biomed. 2018, 16, 81–99. [Google Scholar] [CrossRef] [Green Version]
- Baltas, N.; Karaoglu, S.A.; Tarakci, C.; Kolayli, S. Effect of propolis in gastric disorders: Inhibition studies on the growth of Helicobacter pylori and production of its urease. J. Enzym. Inhib. Med. Chem. 2016, 31, 46–50. [Google Scholar] [CrossRef] [Green Version]
- Boyanova, L.; Gergova, G.; Nikolov, R.; Derejian, S.; Lazarova, E.; Katsarov, N. Activity of Bulgarian propolis against 94 Helicobacter pylori strains in vitro by agar-well diffusion, agar dilution and disc diffusion methods. J. Med. Microbiol. 2005, 54, 481–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho, L.; Bastos, E.; Resende, C.; Paula e Silva, C.; Sanches, B.; de Castro, F.; Moretzsohn, L.D.; Dos Santos Vieira, W.L.; Trindade, O.R. Brazilian green propolis on Helicobacter pylori infection. A pilot clinical study. Helicobacter 2007, 12, 572–574. [Google Scholar] [CrossRef] [PubMed]
- Mazel, D.; Pochet, S.; Marliere, P. Genetic characterization of polypeptide deformylase, a distinctive enzyme of eubacterial translation. EMBO J. 1994, 13, 914–923. [Google Scholar] [CrossRef] [PubMed]
- Ben-Hamida, A.; Man, W.K.; McNeil, N.; Spencer, J. Histamine, xanthine oxidase generated oxygen-derived free radicals and Helicobacter pylori in gastroduodenal inflammation and ulceration. Inflamm. Res. 1998, 47, 193–199. [Google Scholar] [CrossRef]
- Galeotti, F.; Maccari, F.; Fachini, A.; Volpi, N. Chemical Composition and Antioxidant Activity of Propolis Prepared in Different Forms and in Different Solvents Useful for Finished Products. Foods 2018, 7, 41. [Google Scholar] [CrossRef] [Green Version]
- Radha, K.M.; Anoop, K.S.; Jaya, G.; Rikhab, C.S. Multiple biological activities of curcumin: A short review. Life Sci. 2006, 78, 2081–2087. [Google Scholar]
- Sarkar, A.; De, R.; Mukhopadhyay, A.K. Curcumin as a potential therapeutic candidate for Helicobacter pylori associated diseases. World J. Gastroenterol. 2016, 22, 2736. [Google Scholar] [CrossRef] [PubMed]
- Irving, G.R.; Karmokar, A.; Berry, D.P.; Brown, K.; Steward, W.P. Curcumin: The potential for efficacy in gastrointestinal diseases. Best Pract. Res. Clin. Gastroenterol. 2011, 25, 519–534. [Google Scholar] [CrossRef]
- Jurenka, J.S. Anti-inflammatory properties of curcumin, a major constituent of Curcuma longa: A review of preclinical and clinical research. Altern. Med. Rev. 2009, 14, 143–153. [Google Scholar]
- Kumar, D.; Kumar, M.; Saravanan, C.; Singh, S.K. Curcumin: A potential candidate for matrix metalloproteinase inhibitors. Expert Opin. Ther. Targets 2012, 16, 959–972. [Google Scholar] [CrossRef]
- Marathe, S.A.; Sen, M.; Dasgupta, I.; Chakravortty, D. Differential modulation of intracellular survival of cytosolic and vacuolar pathogens by curcumin. Antimicrob. Agents Chemother. 2012, 56, 5555–5567. [Google Scholar] [CrossRef] [Green Version]
- Vetvicka, V.; Vetvickova, J.; Fernandez-Botran, R. Effects of curcumin on Helicobacter pylori infection. Ann. Transl. Med. 2016, 4, 479, Erratum in Ann Transl. Med. 2017, 5, 153. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.R.; Yang, C.S. Protective roles of ginseng against bacterial infection. Microb. Cell 2018, 5, 472. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Yeo, M.; Jin, J.H.; Lee, K.M.; Jung, J.Y.; Choue, R.; Cho, S.W.; Hahm, K.B. Rescue of Helicobacter pylori–induced cytotoxicity by red ginseng. Dig. Dis. Sci. 2005, 50, 1218–1227. [Google Scholar] [CrossRef] [Green Version]
- Cho, W.C.; Chung, W.S.; Lee, S.K.; Leung, A.W.; Cheng, C.H.; Yue, K.K. Ginsenoside Re of Panax ginseng possesses significant antioxidant and antihyperlipidemic efficiency in streptozotocin-induced diabetic rats. Eur. J. Pharmacol. 2006, 550, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Bae, M.; Jang, S.; Lim, J.W. Protective effect of Korean Red Ginseng extract against Helicobacter pylori-induced gastric inflammation in Mongolian gerbils. J. Ginseng Res. 2014, 38, 8–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wee, J.J.; Mee, P.K.; Chung, A.S. Biological Activities of Ginseng and Its Application to Human Health. In Herbal Medicine: Biomolecular and Clinical Aspects, 2nd ed.; Benzie, I.F.F., Wachtel-Galor, S., Eds.; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2011. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK92776/ (accessed on 1 August 2021).
- Hyunju, K.J.; Weon, L.; Hyeyoung, K. Inhibitory effect of Korean Red Ginseng extract on DNA damage response and apoptosis in Helicobacter pylori–infected gastric epithelial cells. J. Ginseng Research. 2020, 1, 79–85. [Google Scholar]
- Singh, V.K.; Singh, D.K. Pharmacological Effects of Garlic (Allium sativum L.). Annu. Rev. Biomed. Sci. 2008, 10, 6–26. [Google Scholar] [CrossRef]
- Ross, S.; Feldberg Chang, S.C.; Kotik, A.N.; Nadler, M.; Neuwirth, Z.; Sundstrom, D.C.; Thompson, N.H. In Vitro Mechanism of Inhibition of Bacterial Cell Growth by Allicin. Antimicrob. Agents Chemother. 1988, 12, 1763–1768. [Google Scholar]
- Ejaz, S.; Woong, L.C.; Ejaz, A. Extract of garlic (Allium sativum) in cancer chemoprevention. Experiment. Oncol. 2003, 25, 93–97. [Google Scholar]
- Islam, M.S.; Kusumoto, Y.; Al-Mamun, M.A. Cytotoxicity and Cancer (HeLa) Cell Killing Efficacy of Aqueous Garlic (Allium sativum) Extract. J. Sci. Res. 2011, 3, 375–382. [Google Scholar] [CrossRef] [Green Version]
- Capasso, A. Antioxidant action and therapeutic efficacy of Allium sativum L. Molecules 2013, 18, 690–700. [Google Scholar] [CrossRef]
- Zhang, Q.; Wu, W.; Zhang, J.; Xia, X. Eradication of Helicobacter pylori: The power of nanosized formulations. Nanomedicine 2020. [Google Scholar] [CrossRef]
- Fritea, L.; Banica, F.; Costea, T.O.; Moldovan, L.; Iovan, C.; Cavalu, S. A gold nanoparticles—Graphene based electrochemical sensor for sensitive determination of nitrazepam. J. Electroanalyt. Chem. 2018, 830–831, 63–71. [Google Scholar] [CrossRef]
- Vala, A.K.; Trivedi, H.; Gosai, H.; Panseriya, H.; Dave, B. Biosynthesized silver nanoparticles and their therapeutic applications. Compr. Analyt. Chem. 2021, 94, 547–584. [Google Scholar] [CrossRef]
- Roy, A. Plant Derived Silver Nanoparticles and their Therapeutic Applications. Curr. Pharm. Biotechnol. 2020. [Google Scholar] [CrossRef]
- Gurunathan, S.; Jeong, J.K.; Han, J.W.; Zhang, X.F.; Park, J.H.; Kim, J.H. Multidimensional effects of biologically synthesized silver nanoparticles in Helicobacter pylori, Helicobacter felis, and human lung (L132) and lung carcinoma A549 cells. Nanoscale Res. Lett. 2015, 10, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikhailova, E.O. Silver Nanoparticles: Mechanism of Action and Probable Bio-Application. J. Funct. Biomater. 2020, 11, 84. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.; Anwar, F.; Janjua, M.R.; Iqbal, M.A.; Rashid, U. Green synthesis of silver nanoparticles through reduction with Solanum xanthocarpum L. berry extract: Characterization, antimicrobial and urease inhibitory activities against Helicobacter pylori. Int. J. Mol. Sci. 2012, 13, 9923–9941. [Google Scholar] [CrossRef]
- Safarov, T.; Kiran, B.; Bagirova, M.; Allahverdiyev, A.M.; Abamor, E.S. An overview of nanotechnology-based treatment approaches against Helicobacter pylori. Expert Rev. Anti-Infect. Ther. 2019. [Google Scholar] [CrossRef]
- Valizadeh, H.; Mohammadi, G.; Ehyaei, R.; Milani, M.; Azhdarzadeh, M.; Zakeri-Milani, P.; Lotfipour, F. Antibacterial activity of clarithromycin loaded PLGA nanoparticles. Die Pharm. Int. J. Pharm. Sci. 2012, 67, 63–68. [Google Scholar]
- Lotfipour, F.; Valizadeh, H.; Milani, M.; Bahrami, N.; Ghotaslou, R. Study of antimicrobial effects of clarithromycin loaded PLGA nanoparticles against clinical strains of Helicobacter pylori. Drug Res. 2016, 66, 41–45. [Google Scholar] [CrossRef]
- Ramteke, S.; Jain, N.K. Clarithromycin-and omeprazole-containing gliadin nanoparticles for the treatment of Helicobacter pylori. J. Drug Target. 2008, 16, 65–72. [Google Scholar] [CrossRef]
- Pan-In, P.; Banlunara, W.; Chaichanawongsaroj, N.; Wanichwecharungruang, S. Ethyl cellulose nanoparticles: Clarithomycin encapsulation and eradication of H. pylori. Carbohydr. Polym. 2014, 109, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Cavalu, S.; Bisboaca, S.; Mates, I.M.; Pasca, P.M.; Laslo, V.; Costea, T.; Fritea, L.; Vicas, S. Novel Formulation Based on Chitosan-Arabic Gum Nanoparticles Entrapping Propolis Extract: Production, physico-chemical and structural characterization. Rev. Chim. 2018, 69, 3756–3760. [Google Scholar] [CrossRef]
- Gonçalves, I.C.; Henriques, P.C.; Seabra, C.L.; Martins, M.C. The potential utility of chitosan micro/nanoparticles in the treatment of gastric infection. Expert Rev. Anti-Infect. Ther. 2014, 12, 981–992. [Google Scholar] [CrossRef]
- Lin, Y.-H.; Chang, C.-H.; Wu, Y.-S.; Hsu, Y.-M.; Chiou, S.-F.; Chen, Y.-J. Development of pH-responsive chitosan/heparin nanoparticles for stomach-specific anti-Helicobacter pylori therapy. Biomaterials 2009, 30, 3332–3342. [Google Scholar] [CrossRef]
- Hamman, J.H. Chitosan based polyelectrolyte complexes as potential carrier materials in drug delivery systems. Mar. Drugs 2010, 8, 1305–1322. [Google Scholar] [CrossRef] [Green Version]
- Bardonnet, P.-L.; Faivre, V.; Boullanger, P.; Piffaretti, J.-C.; Falson, F. Pre-formulation of liposomes against Helicobacter pylori: Characterization and interaction with the bacteria. Eur. J. Pharm. Biopharm. 2008, 69, 908–922. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.W.; Thamphiwatana, S.; Zhang, L.; Obonyo, M. Mechanism of antibacterial activity of liposomal linolenic acid against Helicobacter pylori. PLoS ONE 2015, 10, e0116519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thamphiwatana, S.; Gao, W.; Obonyo, M.; Zhang, L. In vivo treatment of Helicobacter pylori infection with liposomal linolenic acid reduces colonization and ameliorates inflammation. Proc. Natl. Acad. Sci. USA 2014, 111, 17600–17605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seabra, C.L.; Nunes, C.; Gomez-Lazaro, M.; Correia, M.; Machado, J.C.; Gonçalves, I.C.; Reis, C.A.; Reis, S.; Martins, M.C.L. Docosahexaenoic acid loaded lipid nanoparticles with bactericidal activity against Helicobacter pylori. Int. J. Pharm. 2017, 519, 128–137. [Google Scholar] [CrossRef]
- Thamphiwatana, S.; Gao, W.; Pornpattananangkul, D.; Zhang, Q.; Fu, V.; Li, J.; Obonyo, M.; Zhang, L. Phospholipase A2-responsive antibiotic delivery via nanoparticle-stabilized liposomes for the treatment of bacterial infection. J. Mater. Chem. B 2014, 2, 8201–8207. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Name/Family | Formulation | Main Outcomes In Vitro/In Vivo | Reference |
|---|---|---|---|
| Allium sativum/ Amaryllidaceae | Garlic oil and powder | In vitro (standard and clinical isolates)—significant loss of viability, inactivation irrespective of strain, depending on allicin concentration In vivo (clinical trials)-improves eradication rates, healing rates of ulcers, remission of peptic ulcers, synergism with conventional therapy | [96,97,98] |
| Bridelia micrantha/ Euphorbiaceous | Stem bark extract | In vitro (standard strains and clinical isolates)—killing rate depending on concentration and time (agar-well diffusion and MIC method) Antioxidant, anti-inflammatory properties | [99,100,101] |
| Camellia sinensis/ Theaceae | Young shoot extract | In vivo (animal model)—prevents gastritis, limits the localization of bacteria and VacA to the surface of the gastric epithelium. In vivo (clinical trial)—suppression of gastritis and prevalence of H. pylori in a dose-dependent manner. In vitro—inhibits the production and function of the urease enzyme. | [102,103,104] |
| Daucus carota/ Apiaceae | Essential oil of carrot seed | In vitro and in vivo (animal model)—co-administration with pantoprazole exhibits strong anti-H. pylori activity | [105,106] |
| Eugenia caryophillus/ Myrtaceae | Extracts of flowers | In vitro (standard strains and clinical isolates)—decrease viability of H. pylori, irrespective of the strain, at acidic pH, effective in gastritis | [107,108] |
| Geum iranicum/ Rosaceae | Aqueous extract of roots | In vitro- effective against clinical isolates of H. pylori resistant to metronidazole | [109] |
| Hancornia speciosa/ Apocyanaceae | Bark’s hydroalcoholic extract | In vivo (rodent model)- anti-H. pylori effect by increasing of gastric mucus formation and antioxidant properties of polymeric pro-anthocyanidins Anti-inflammatory, antibacterial, and anticancer properties. | [110,111] |
| Myrtus communis/ Myrtaceae | Essential oil extract | In vitro—effective against clinically isolated strains resistant to nitroimidazoles and clarithromycin. Antimicrobial, antidiarrheal, anticancer, antioxidant, antiulcer, anti-inflammatory and antidiabetic activity | [112,113] |
| Malus domestica/ Rosaceae | Apple peel extract | In vitro—prevents vacuolation in HeLa cells, antiadhesive effect against H. pylori. In vivo (short-term infection model mice)—inhibitory effect on H. pylori attachment, anti-inflammatory effect on H. pylori-associated gastritis, reversible inhibitory effect | [114,115] |
| Olea europaea/ Oleaceae | Olive leaf extract | In vitro (clinically isolated meticillin resistant strains)—regulates the composition of the gastric flora, selectively reduce levels of H. pylori Antiulcer, antioxidant and antimicrobial effects | [116,117] |
| Prunus dulcis/ Rosaceae | Polyphenol extract | In vitro (standard strains and clinical isolates)—effective against H. pylori with different virulence irrespective of the cagA and vacA status. | [118,119] |
| Rumex aquaticus/ Polygonaceae | Plant extract | In vitro (human adenocarcinoma gastric cells)—cytotoxic effects against AGS cells, inhibit the production of proinflammatory cytokines, antioxidant | [120,121] |
| Stachys setifera/ Lamiaceae | Aerial part extract | In vitro (isolates)—strong inhibitory effect | [101,122] |
| Zingiber officinale/ Zingiberaceae | Rhizome extract | In vitro—potent inhibitors of proton potassium ATPase activity and H. pylori growth. In vivo (pilot study)—significant H. pylori eradication rate in dyspeptic patients, additive effect along with antibiotics | [123,124,125] |
| Propolis/ Apis melifera | Ethanolic extracts | In vitro—anti-H. pylori and anti-urease activities, 92.1% inhibition rate, synergism with clarithromycin or metronidazole | [126,127,128,129,130,131,132,133,134] |
| Curcuma longa/ Zingiberaceae | Rhizome extract, polyphenolicrich extract of the root | In vitro (clinical isolates)—stabilizes the vacuolar membrane and prevents the escape of cytosolic pathogens, suppressor of the type 1 immune response. In vivo (mouse model)—increase IL-4 serum levels and IgG, decrease IFN-γ levels | [135,136,137,138,139,140,141] |
| Ginseng/ Panax ginseng Meyer | Korean Red Ginseng extract | In vitro (infected gastric epithelial cells)—reduces reactive oxygen species and prevents cell death In vivo (animal model Mongolian gerbils)—anti-inflammatory effect on H. pylori-induced gastric inflammation | [142,143,144,145,146,147] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardos, I.A.; Zaha, D.C.; Sindhu, R.K.; Cavalu, S. Revisiting Therapeutic Strategies for H. pylori Treatment in the Context of Antibiotic Resistance: Focus on Alternative and Complementary Therapies. Molecules 2021, 26, 6078. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26196078
Cardos IA, Zaha DC, Sindhu RK, Cavalu S. Revisiting Therapeutic Strategies for H. pylori Treatment in the Context of Antibiotic Resistance: Focus on Alternative and Complementary Therapies. Molecules. 2021; 26(19):6078. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26196078
Chicago/Turabian StyleCardos, Ioana Alexandra, Dana Carmen Zaha, Rakesh K. Sindhu, and Simona Cavalu. 2021. "Revisiting Therapeutic Strategies for H. pylori Treatment in the Context of Antibiotic Resistance: Focus on Alternative and Complementary Therapies" Molecules 26, no. 19: 6078. https://0-doi-org.brum.beds.ac.uk/10.3390/molecules26196078