Effectiveness of Low-Level Laser Therapy Associated with Strength Training in Knee Osteoarthritis: Protocol for a Randomized Placebo-Controlled Trial

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Methods and Design
2.2. Participants
3. Procedure
3.1. Randomization
3.2. Strength Training
- ST level 1: Pelvic lifts (2 × 15 RM), one-legged knee bends with maximum 60° flexion (2 × 10 RM per leg) and hip abductions with elastic band (2 × 10 RM per leg).
- ST level 2: Pelvic lifts (3 × 15 RM), one-legged knee bends with maximum 60° flexion (3 × 10 RM per leg), hip abductions with elastic band (2 × 10 RM per leg), sideways slide lunges (2 × 10 RM per leg) and backward slide lunges (2 × 10 RM per leg).
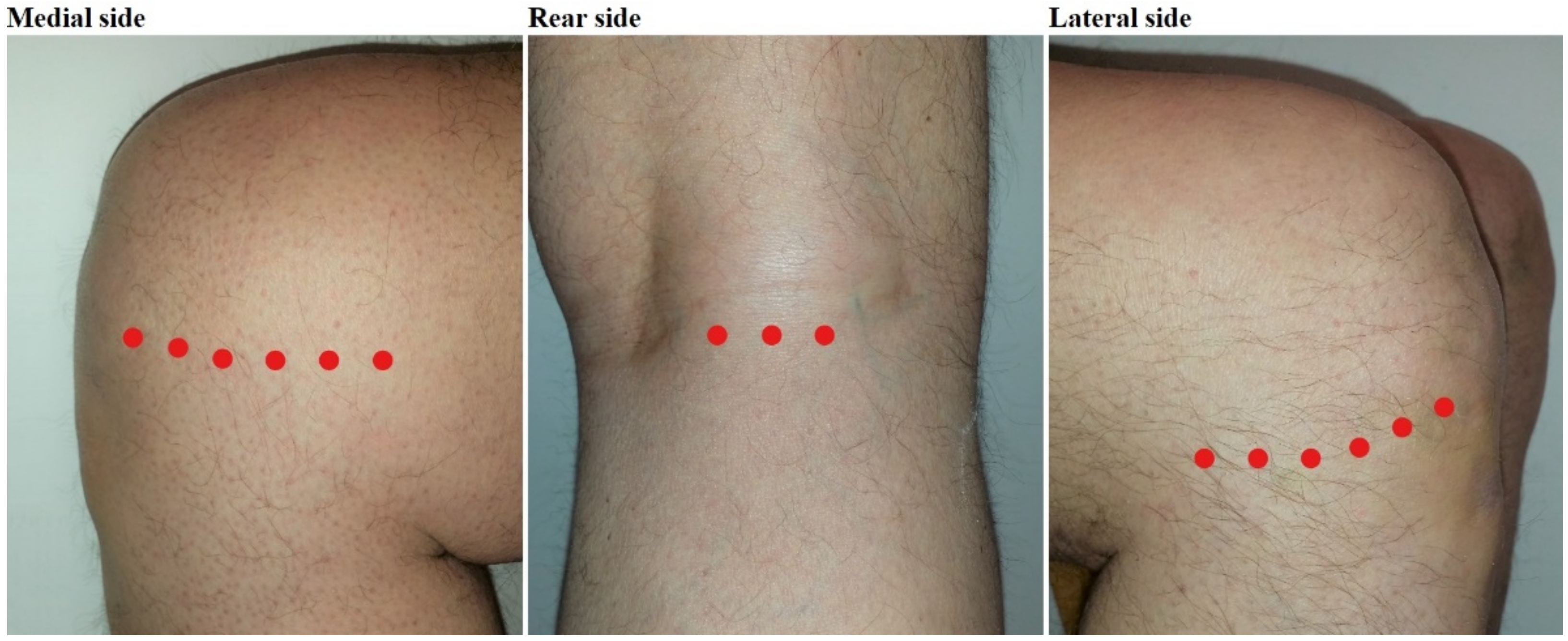
3.3. Laser Therapy and Blinding
3.4. Concomitant Interventions
3.5. Outcomes
3.5.1. VAS (Pain)
3.5.2. KOOS (Pain, Physical Function, QoL and Other Symptoms)
3.5.3. Global Health Change
3.5.4. Analgesics
3.5.5. AROM
3.5.6. 30 Second Chair Stand Test
3.5.7. Maximum Pain-Free Isometric Knee Extension Strength
3.5.8. PPT
3.5.9. RTU
3.6. Statistial Analysis
3.7. Sample Size
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heidari, B. Knee osteoarthritis prevalence, risk factors, pathogenesis and features—Part 1. Casp. J. Intern. Med. 2011, 2, 205–212. [Google Scholar]
- Berenbaum, F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthr. Cartil. 2013, 21, 16–21. [Google Scholar] [CrossRef] [Green Version]
- Tomazoni, S.S.; Leal-Junior, E.C.P.; Frigo, L.; Pallotta, R.C.; Teixeira, S.; De Almeida, P.; Bjordal, J.M.; Lopes-Martins, R.; Álvaro, B. Isolated and combined effects of photobiomodulation therapy, topical nonsteroidal anti-inflammatory drugs, and physical activity in the treatment of osteoarthritis induced by papain. J. Biomed. Opt. 2016, 21, 108001. [Google Scholar] [CrossRef] [PubMed]
- Tomazoni, S.S.; Leal-Junior, E.C.P.; Pallotta, R.C.; Teixeira, S.; De Almeida, P.; Lopes-Martins, R.; Álvaro, B. Effects of photobiomodulation therapy, pharmacological therapy, and physical exercise as single and/or combined treatment on the inflammatory response induced by experimental osteoarthritis. Lasers Med. Sci. 2017, 32, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Assis, L.; Milares, L.; Almeida, T.; Tim, C.; Magri, A.; Fernandes, K.; Medalha, C.; Renno, A.M. Aerobic exercise training and low-level laser therapy modulate inflammatory response and degenerative process in an experimental model of knee osteoarthritis in rats. Osteoarthr. Cartil. 2016, 24, 169–177. [Google Scholar] [CrossRef] [Green Version]
- Pallotta, R.C.; Bjordal, J.M.; Frigo, L.; Junior, E.C.P.L.; Teixeira, S.; Marcos, R.L.; Ramos, L.; Messias, F.D.M.; Lopes-Martins, R.; Álvaro, B. Infrared (810-nm) low-level laser therapy on rat experimental knee inflammation. Lasers Med. Sci. 2012, 27, 71–78. [Google Scholar] [CrossRef] [Green Version]
- Xiang, A.; Deng, H.; Cheng, K.; Liu, H.; Lin, L.; Qu, X.; Liu, S.; Shen, X. Laser photobiomodulation for cartilage defect in animal models of knee osteoarthritis: A systematic review and meta-analysis. Lasers Med. Sci. 2020, 35, 789–796. [Google Scholar] [CrossRef]
- Geenen, R.; Overman, C.L.; Christensen, R.; Åsenlöf, P.; Capela, S.; Huisinga, K.L.; Husebø, M.E.P.; Köke, A.J.; Paskins, Z.; Pitsillidou, I.; et al. EULAR recommendations for the health professional’s approach to pain management in inflammatory arthritis and osteoarthritis. Ann. Rheum. Dis. 2018, 77, 797–807. [Google Scholar] [CrossRef] [Green Version]
- Collins, N.J.; Hart, H.F.; Mills, K.A.G. OARSI year in review 2018: Rehabilitation and outcomes. Osteoarthr. Cartil. 2019, 27, 378–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WALT. Recommended Treatment Doses for Low Level Laser Therapy 780–860 nm Wavelength. 2010. Available online: http://waltza.co.za/wp-content/uploads/2012/08/Dose_table_780–860nm_for_Low_Level_Laser_Therapy_WALT-2010.pdf (accessed on 6 May 2020).
- WALT. Recommended Treatment Doses for Low Level Laser Therapy 904 nm Wavelength. 2010. Available online: http://waltza.co.za/wp-content/uploads/2012/08/Dose_table_904nm_for_Low_Level_Laser_Therapy_WALT-2010.pdf (accessed on 6 May 2020).
- Stausholm, M.B.; Msc, I.F.N.; Joensen, J.; Lopes-Martins, R.; Álvaro, B.; Sæbø, H.; Lund, H.; Fersum, K.V.; Bjordal, J.M. Efficacy of low-level laser therapy on pain and disability in knee osteoarthritis: Systematic review and meta-analysis of randomised placebo-controlled trials. BMJ Open 2019, 9, e031142. [Google Scholar] [CrossRef]
- Alfredo, P.P.; Bjordal, J.M.; Junior, W.S.; Lopes-Martins, R.; Álvaro, B.; Stausholm, M.B.; Casarotto, R.A.; Marques, A.P.; Joensen, J. Long-term results of a randomized, controlled, double-blind study of low-level laser therapy before exercises in knee osteoarthritis: Laser and exercises in knee osteoarthritis. Clin. Rehabil. 2018, 32, 173–178. [Google Scholar] [CrossRef]
- Al Rashoud, A.S.; Abboud, R.J.; Wang, W.; Wigderowitz, C. Efficacy of low-level laser therapy applied at acupuncture points in knee osteoarthritis: A randomised double-blind comparative trial. Physiotherapy 2014, 100, 242–248. [Google Scholar] [CrossRef]
- Hinman, R.S.; McCrory, P.R.; Pirotta, M.; Relf, I.; Forbes, A.; Crossley, K.M.; Williamson, E.; Kyriakides, M.; Novy, K.; Metcalf, B.R.; et al. Acupuncture for chronic knee pain: A randomized clinical trial. JAMA 2014, 312, 1313–1322. [Google Scholar] [CrossRef] [PubMed]
- Stausholm, M.; Bjordal, J.; Lopes-Martins, R.; Joensen, J. Methodological flaws in meta-analysis of low-level laser therapy in knee osteoarthritis: A letter to the editor. Osteoarthr. Cartil. 2017, 25, e9–e10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayegani, S.M.; Raeissadat, S.A.; Heidari, S.; Moradi-Joo, M. Safety and effectiveness of low-level laser therapy in patients with knee osteoarthritis: A systematic review and meta-analysis. J. Lasers Med. Sci. 2017, 8, 12–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartholdy, C.; Juhl, C.; Christensen, R.; Lund, H.; Zhang, W.; Henriksen, M. The role of muscle strengthening in exercise therapy for knee osteoarthritis: A systematic review and meta-regression analysis of randomized trials. Semin. Arthritis Rheum. 2017, 47, 9–21. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Nambi, S.G.; Kamal, W.; George, J.; Manssor, E. Radiological and biochemical effects (CTX-II, MMP-3, 8, and 13) of low-level laser therapy (LLLT) in chronic osteoarthritis in Al-Kharj, Saudi Arabia. Lasers Med. Sci. 2017, 32, 297–303. [Google Scholar] [CrossRef]
- Kheshie, A.R.; Alayat, M.S.; Ali, M.M. High-intensity versus low-level laser therapy in the treatment of patients with knee osteoarthritis: A randomized controlled trial. Lasers Med. Sci. 2014, 29, 1371–1376. [Google Scholar] [CrossRef]
- Bellamy, N.; Kirwan, J.; Boers, M.; Brooks, P.; Strand, V.; Tugwell, P.; Altman, R.; Brandt, K.; Dougados, M.; LeQuesne, M. Recommendations for a core set of outcome measures for future phase III clinical trials in knee, hip, and hand osteoarthritis. Consensus development at OMERACT III. J. Rheumatol. 1997, 24, 799–802. [Google Scholar] [PubMed]
- Altman, R.; Asch, E.; Bloch, D.; Bole, G.; Borenstein, D.; Brandt, K.; Christy, W.; Cooke, T.D.; Greenwald, R.; Hochberg, M.; et al. Development of criteria for the classification and reporting of osteoarthritis—Classification of osteoarthritis of the knee. Arthritis Rheum. 1986, 29, 1039–1049. [Google Scholar] [CrossRef]
- Relf, I.; Chow, R.; Pirotta, M. Blinding techniques in randomized controlled trials of laser therapy: An overview and possible solution. Evid. Based Complement. Altern. Med. 2008, 5, 383–389. [Google Scholar] [CrossRef] [Green Version]
- Alghadir, A.H.; Anwer, S.; Iqbal, A.; Iqbal, Z.A. Test-retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J. Pain Res. 2018, 11, 851–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado, D.A.; Lambert, B.S.; Boutris, N.; McCulloch, P.C.; Robbins, A.B.; Moreno, M.R.; Harris, J.D. Validation of Digital Visual Analog Scale Pain Scoring with a Traditional Paper-based Visual Analog Scale in Adults. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2018, 2, e088. [Google Scholar] [CrossRef] [PubMed]
- Collins, N.J.; Prinsen, C.A.; Christensen, R.; Bartels, E.M.; Terwee, C.B.; Roos, E.M. Knee Injury and Osteoarthritis Outcome Score (KOOS): Systematic review and meta-analysis of measurement properties. Osteoarthr. Cartil. 2016, 24, 1317–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hancock, G.E.; Hepworth, T.; Wembridge, K. Accuracy and reliability of knee goniometry methods. J. Exp. Orthop. 2018, 5, 6. [Google Scholar] [CrossRef] [Green Version]
- Dobson, F.; Hinman, R.; Roos, E.; Abbott, J.; Stratford, P.; Davis, A.; Buchbinder, R.; Snyder-Mackler, L.; Henrotin, Y.; Thumboo, J.; et al. OARSI recommended performance-based tests to assess physical function in people diagnosed with hip or knee osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1042–1052. [Google Scholar] [CrossRef] [Green Version]
- Torp-Pedersen, S.; Bartels, E.M.; Wilhjelm, J.E.; Bliddal, H. Articular cartilage thickness measured with US is not as easy as it appears: A systematic review of measurement techniques and image interpretation. Ultraschall Med. 2011, 32, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Gur, A.; Cosut, A.; Sarac, A.J.; Çevik, R.; Nas, K.; Uyar, A. Efficacy of different therapy regimes of low-power laser in painful osteoarthritis of the knee: A double-blind and randomized-controlled trial. Lasers Surg. Med. 2003, 33, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Koutenaei, F.R.; Mosallanezhad, Z.; Naghikhani, M.; Ezati, K.; Biglarian, A.; Nouroozi, M.; Ghodrati, M. The Effect of Low Level Laser Therapy on Pain and Range of Motion of Patients With Knee Osteoarthritis. Phys. Treat. Specif. Phys. Ther. J. 2017, 7, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Alghadir, A.; Omar, M.T.A.; Al-Askar, A.B.; Al-Muteri, N.K. Effect of low-level laser therapy in patients with chronic knee osteoarthritis: A single-blinded randomized clinical study. Lasers Med. Sci. 2014, 29, 749–755. [Google Scholar] [CrossRef]
- Tascioglu, F.; Armagan, O.; Tabak, Y.; Corapci, I.; Oner, C. Low power laser treatment in patients with knee osteoarthritis. Swiss. Med. Wkly. 2004, 134, 254–258. [Google Scholar] [PubMed]
- Gur, A.; Oktayoglu, P. Comparison of efficacy of 904 nm gallium arsenide low level laser and physical therapy modalities in the management of painful knee osteoarthritis. Under review.
- Delkhosh, C.T.; Fatemy, E.; Ghorbani, R.; Mohammadi, R. Comparing the immediate and long-term effects of low and high power laser on the symptoms of knee osteoarthritis. J. Maz. Univ. Med. Sci. 2018, 28, 69–77. [Google Scholar]
- Mohammed, N.; Allam, H.; ElGhoroury, E.; Zikri, E.N.; Helmy, G.A.; Elgendy, A. Evaluation of serum beta-endorphin and substance P in knee osteoarthritis patients treated by laser acupuncture. J. Complement. Integr. Med. 2018, 15. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Week 0 | Week 3 | Week 8 | Week 26 | Week 52 | |
|---|---|---|---|---|---|
| Pain during movement (VAS) | √ | √ | √ | √ | √ |
| Pain at night (VAS) | √ | √ | √ | √ | √ |
| Pain at rest (VAS) | √ | √ | √ | √ | √ |
| Global pain (KOOS) | √ | √ | √ | √ | √ |
| Disability in ADL (KOOS) | √ | √ | √ | √ | √ |
| Disability in sports/recreation (KOOS) | √ | √ | √ | √ | √ |
| Global health change | √ | ||||
| Analgesic usage | √ | √ | √ | √ | √ |
| Knee active range of motion | √ | √ | √ | √ | √ |
| 30 s chair stand | √ | √ | √ | √ | √ |
| Pain-free isometric knee extension strength | √ | √ | √ | √ | √ |
| Joint line PPT | √ | √ | √ | √ | √ |
| Tibia condyle PPT | √ | √ | √ | √ | √ |
| Suprapatellar effusion (RTU) | √ | √ | √ | √ | √ |
| Meniscal neovascularization (RTU) | √ | √ | √ | √ | √ |
| Femur cartilage thickness (RTU) | √ | √ | √ | √ | √ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stausholm, M.B.; Naterstad, I.F.; Couppé, C.; Fersum, K.V.; Leal-Junior, E.C.P.; Lopes-Martins, R.Á.B.; Bjordal, J.M.; Joensen, J. Effectiveness of Low-Level Laser Therapy Associated with Strength Training in Knee Osteoarthritis: Protocol for a Randomized Placebo-Controlled Trial. Methods Protoc. 2021, 4, 19. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4010019
Stausholm MB, Naterstad IF, Couppé C, Fersum KV, Leal-Junior ECP, Lopes-Martins RÁB, Bjordal JM, Joensen J. Effectiveness of Low-Level Laser Therapy Associated with Strength Training in Knee Osteoarthritis: Protocol for a Randomized Placebo-Controlled Trial. Methods and Protocols. 2021; 4(1):19. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4010019
Chicago/Turabian StyleStausholm, Martin Bjørn, Ingvill Fjell Naterstad, Christian Couppé, Kjartan Vibe Fersum, Ernesto Cesar Pinto Leal-Junior, Rodrigo Álvaro Brandão Lopes-Martins, Jan Magnus Bjordal, and Jon Joensen. 2021. "Effectiveness of Low-Level Laser Therapy Associated with Strength Training in Knee Osteoarthritis: Protocol for a Randomized Placebo-Controlled Trial" Methods and Protocols 4, no. 1: 19. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4010019