
Effect of Oral Prophylactic Measures on the Occurrence of Pre-Eclampsia (OP-PE) in High-Risk Pregnant Women: A Cluster Randomized Controlled Trial


 , and
, and
Abstract
:1. Introduction
2. Material and Methods
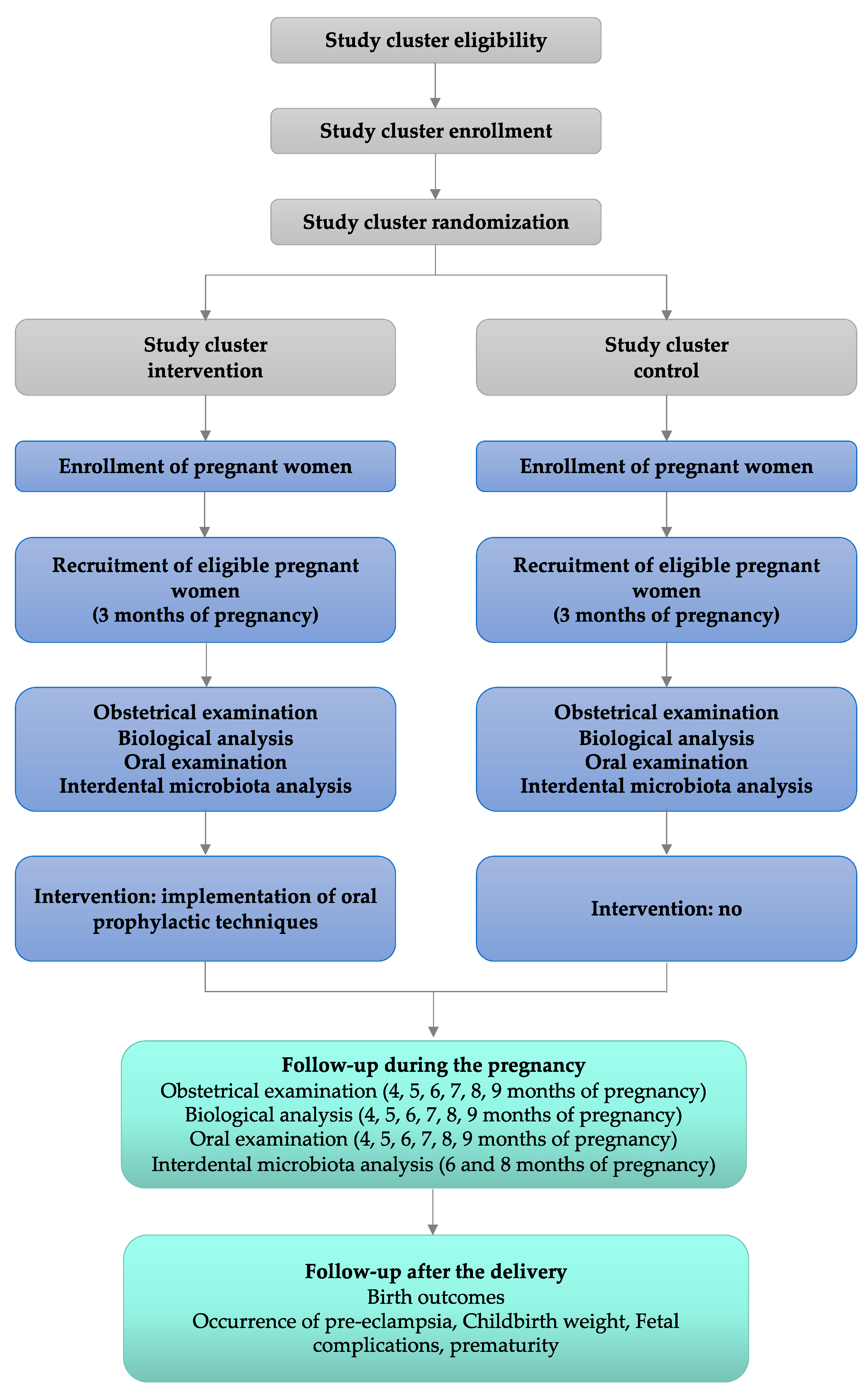
2.1. Trial Design
2.2. Study Setting
2.3. Study Population
2.3.1. Eligibility Criteria
2.3.2. Exclusion Criteria
2.4. Interventions
2.5. Outcomes
2.5.1. Primary Outcome Measures
2.5.2. Secondary Outcome Measures
- -
- Quantification of the pathogenic bacterial load of the interdental microbiota.
- -
- Severity scores of periodontal indicators: pocket probing depth (PPD), clinical attachment level (CAL), gingival index (GI), plaque index (PI), bleeding on interdental brushing index (BOIB).
- -
- Incidence of adverse perinatal outcomes (low birth weight and preterm delivery).
2.6. Participant Timeline
2.6.1. Pre-Screening and Assessment for Eligibility
2.6.2. Inclusion, Prenatal Examination, Oral Examination, and Baseline Interdental Microbiota Sampling (T1)
- Prenatal clinical examination
- Biological analysis
- Oral clinical examination and sampling of the interdental microbiota
- Analysis of the interdental microbiota
2.6.3. Follow-Up Visits
2.6.4. Delivery Data Collection
2.7. Sample Size
2.8. Recruitment
2.9. Assignment of Interventions
2.9.1. Allocation
2.9.2. Blinding
2.10. Data Collection, Management, Analysis
2.10.1. Data Collection Methods
2.10.2. Data Management
2.10.3. Statistical Methods
2.11. Ethics Statement
3. Expected Results
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Osungbade, K.O.; Ige, O.K. Public Health Perspectives of Preeclampsia in Developing Countries: Implication for Health System Strengthening. J. Pregnancy 2011, 2011, 481095. [Google Scholar] [CrossRef] [Green Version]
- Bilano, V.L.; Ota, E.; Ganchimeg, T.; Mori, R.; Souza, J.P. Risk Factors of Pre-Eclampsia/Eclampsia and Its Adverse Outcomes in Low- and Middle-Income Countries: A WHO Secondary Analysis. PLoS ONE 2014, 9, e91198. [Google Scholar] [CrossRef] [Green Version]
- Al Khalaf, S.Y.; O’Reilly, É.J.; McCarthy, F.P.; Kublickas, M.; Kublickiene, K.; Khashan, A.S. Pregnancy Outcomes in Women with Chronic Kidney Disease and Chronic Hypertension: A National Cohort Study. Am. J. Obs. Gynecol. 2021. [Google Scholar] [CrossRef]
- Umesawa, M.; Kobashi, G. Epidemiology of Hypertensive Disorders in Pregnancy: Prevalence, Risk Factors, Predictors and Prognosis. Hypertens. Res. 2017, 40, 213–220. [Google Scholar] [CrossRef]
- Kotit, S.; Yacoub, M. Cardiovascular Adverse Events in Pregnancy: A Global Perspective. Glob. Cardiol. Sci. Pract. 2021, 2021, e202105. [Google Scholar] [CrossRef] [PubMed]
- Lisonkova, S.; Joseph, K.S. Incidence of Preeclampsia: Risk Factors and Outcomes Associated with Early- versus Late-Onset Disease. Am. J. Obstet. Gynecol. 2013, 209, 544.e1–544.e12. [Google Scholar] [CrossRef] [PubMed]
- Steegers, E.A.P.; von Dadelszen, P.; Duvekot, J.J.; Pijnenborg, R. Pre-Eclampsia. Lancet 2010, 376, 631–644. [Google Scholar] [CrossRef]
- Olaniyi, K.S.; Moodley, J.; Mahabeer, Y.; Mackraj, I. Placental Microbial Colonization and Its Association with Pre-Eclampsia. Front. Cell Infect. Microbiol. 2020, 10, 413. [Google Scholar] [CrossRef]
- Gongora, M.C.; Wenger, N.K. Cardiovascular Complications of Pregnancy. Int. J. Mol. Sci. 2015, 16, 23905–23928. [Google Scholar] [CrossRef] [PubMed]
- Melchiorre, K.; Thilaganathan, B.; Giorgione, V.; Ridder, A.; Memmo, A.; Khalil, A. Hypertensive Disorders of Pregnancy and Future Cardiovascular Health. Front. Cardiovasc. Med. 2020, 7, 59. [Google Scholar] [CrossRef] [Green Version]
- Meqa, K.; Dragidella, F.; Disha, M.; Sllamniku-Dalipi, Z. The Association between Periodontal Disease and Preterm Low Birthweight in Kosovo. Acta Stomatol. Croat. 2017, 51, 33–40. [Google Scholar] [CrossRef]
- Ren, H.; Du, M. Role of Maternal Periodontitis in Preterm Birth. Front. Immunol. 2017, 8, 139. [Google Scholar] [CrossRef] [Green Version]
- Usin, M.M.; Menso, J.; Rodríguez, V.I.; González, A.; Tabares, S.; Parodi, R.; Sembaj, A. Association between Maternal Periodontitis and Preterm and/or Low Birth Weight Infants in Normal Pregnancies. J. Matern. Fetal Neonatal Med. 2016, 29, 115–119. [Google Scholar] [CrossRef]
- Jepsen, S.; Caton, J.G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Demirel, K.; de Sanctis, M.; Ercoli, C.; Fan, J.; et al. Periodontal Manifestations of Systemic Diseases and Developmental and Acquired Conditions: Consensus Report of Workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S219–S229. [Google Scholar] [CrossRef]
- Fischer, L.A.; Demerath, E.; Bittner-Eddy, P.; Costalonga, M. Placental Colonization with Periodontal Pathogens: The Potential Missing Link. Am. J. Obstet. Gynecol. 2019, 221, 383–392. [Google Scholar] [CrossRef]
- Terzic, M.; Aimagambetova, G.; Terzic, S.; Radunovic, M.; Bapayeva, G.; Laganà, A.S. Periodontal Pathogens and Preterm Birth: Current Knowledge and Further Interventions. Pathogens 2021, 10, 730. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Chavakis, T. Local and Systemic Mechanisms Linking Periodontal Disease and Inflammatory Comorbidities. Nat. Rev. Immunol. 2021, 1–15. [Google Scholar] [CrossRef]
- Gare, J.; Kanoute, A.; Meda, N.; Viennot, S.; Bourgeois, D.; Carrouel, F. Periodontal Conditions and Pathogens Associated with Pre-Eclampsia: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 7194. [Google Scholar] [CrossRef] [PubMed]
- Yin, C.; Chen, J.; Wu, X.; Liu, Y.; He, Q.; Cao, Y.; Huang, Y.-E.; Liu, S. Preterm Birth Is Correlated with Increased Oral Originated Microbiome in the Gut. Front. Cell Infect. Microbiol. 2021, 11, 579766. [Google Scholar] [CrossRef] [PubMed]
- Radaic, A.; Kapila, Y.L. The Oralome and Its Dysbiosis: New Insights into Oral Microbiome-Host Interactions. Comput. Struct. Biotechnol. J. 2021, 19, 1335–1360. [Google Scholar] [CrossRef] [PubMed]
- Bourgeois, D.; Bravo, M.; Llodra, J.-C.; Inquimbert, C.; Viennot, S.; Dussart, C.; Carrouel, F. Calibrated Interdental Brushing for the Prevention of Periodontal Pathogens Infection in Young Adults—A Randomized Controlled Clinical Trial. Sci. Rep. 2019, 9, 15127. [Google Scholar] [CrossRef] [Green Version]
- Bourgeois, D.; Saliasi, I.; Llodra, J.C.; Bravo, M.; Viennot, S.; Carrouel, F. Efficacy of Interdental Calibrated Brushes on Bleeding Reduction in Adults: A 3-Month Randomized Controlled Clinical Trial. Eur. J. Oral Sci. 2016, 124, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Ye, C.; Kobayashi, H.; Katagiri, S.; Miyasaka, N.; Takeuchi, Y.; Kuraji, R.; Izumi, Y. The Relationship between the Anti-Porphyromonas gingivalis Immunoglobulin G Subclass Antibody and Small for Gestational Age Delivery: A Longitudinal Study in Pregnant Japanese Women. Int. Dent. J. 2020, 70, 296–302. [Google Scholar] [CrossRef]
- Figuero, E.; Lindahl, C.; Marín, M.J.; Renvert, S.; Herrera, D.; Ohlsson, O.; Wetterling, T.; Sanz, M. Quantification of Periodontal Pathogens in Vascular, Blood, and Subgingival Samples from Patients with Peripheral Arterial Disease or Abdominal Aortic Aneurysms. J. Periodontol. 2014, 85, 1182–1193. [Google Scholar] [CrossRef] [PubMed]
- Bourgeois, D.; Inquimbert, C.; Ottolenghi, L.; Carrouel, F. Periodontal Pathogens as Risk Factors of Cardiovascular Diseases, Diabetes, Rheumatoid Arthritis, Cancer, and Chronic Obstructive Pulmonary Disease-Is There Cause for Consideration? Microorganisms 2019, 7, 424. [Google Scholar] [CrossRef] [Green Version]
- Gómez, L.A.; De Avila, J.; Castillo, D.M.; Montenegro, D.A.; Trujillo, T.G.; Suárez, L.J.; Lafaurie, G.I. Porphyromonas Gingivalis Placental Atopobiosis and Inflammatory Responses in Women with Adverse Pregnancy Outcomes. Front. Microbiol. 2020, 11, 591626. [Google Scholar] [CrossRef] [PubMed]
- Vanterpool, S.F.; Tomsin, K.; Reyes, L.; Zimmermann, L.J.; Kramer, B.W.; Been, J.V. Risk of Adverse Pregnancy Outcomes in Women with Periodontal Disease and the Effectiveness of Interventions in Decreasing This Risk: Protocol for Systematic Overview of Systematic Reviews. Syst. Rev. 2016, 5, 16. [Google Scholar] [CrossRef] [Green Version]
- Vanterpool, S.F.; Been, J.V.; Houben, M.L.; Nikkels, P.G.J.; De Krijger, R.R.; Zimmermann, L.J.I.; Kramer, B.W.; Progulske-Fox, A.; Reyes, L. Porphyromonas Gingivalis within Placental Villous Mesenchyme and Umbilical Cord Stroma Is Associated with Adverse Pregnancy Outcome. PLoS ONE 2016, 11, e0146157. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.-W.; Tetzlaff, J.M.; Gøtzsche, P.C.; Altman, D.G.; Mann, H.; Berlin, J.A.; Dickersin, K.; Hróbjartsson, A.; Schulz, K.F.; Parulekar, W.R.; et al. SPIRIT 2013 Explanation and Elaboration: Guidance for Protocols of Clinical Trials. BMJ 2013, 346, e7586. [Google Scholar] [CrossRef] [Green Version]
- Eke, P.I.; Dye, B.A.; Wei, L.; Slade, G.D.; Thornton-Evans, G.O.; Borgnakke, W.S.; Taylor, G.W.; Page, R.C.; Beck, J.D.; Genco, R.J. Update on Prevalence of Periodontitis in Adults in the United States: NHANES 2009 to 2012. J. Periodontol. 2015, 86, 611–622. [Google Scholar] [CrossRef] [Green Version]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global Burden of Severe Periodontitis in 1990-2010: A Systematic Review and Meta-Regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Bourgeois, D.; Carrouel, F.; Llodra, J.C.; Bravo, M.; Viennot, S. A Colorimetric Interdental Probe as a Standard Method to Evaluate Interdental Efficiency of Interdental Brush. Open Dent. J. 2015, 9, 431–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenauer, T.; Wagenschwanz, C.; Kuhn, M.; Kensche, A.; Stiehl, S.; Hannig, C. The Bleeding on Brushing Index: A Novel Index in Preventive Dentistry. Int. Dent. J. 2017, 67, 299–307. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus Report of Workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teerenstra, S.; Eldridge, S.; Graff, M.; de Hoop, E.; Borm, G.F. A Simple Sample Size Formula for Analysis of Covariance in Cluster Randomized Trials. Stat. Med. 2012, 31, 2169–2178. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Akhtar-Danesh, N.; Dolovich, L.; Thabane, L. The CHAT investigators Imputation Strategies for Missing Binary Outcomes in Cluster Randomized Trials. BMC Med. Res. Methodol. 2011, 11, 18. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Date of Pregnancy Procedures/Visits | Timeline | |||||||
|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T3 | T4 | T5 | T6 | T7 | |
| 3 Months * | 4 Months | 5 Months | 6 Months | 7 Months | 8 Months | 9 Months | ||
| Pre-screening | X | |||||||
| Eligibility screening | X | |||||||
| Informed consent | X | |||||||
| Obstetric examination | X | X | X | X | X | X | X | X |
| weight | X | X | X | X | X | X | X | X |
| blood pressure | X | X | X | X | X | X | X | X |
| uterine heigh | X | X | X | X | X | X | X | X |
| Biological analysis | X | X | X | X | X | X | X | X |
| red blood cells | X | X | X | X | X | X | X | X |
| white blood cells | X | X | X | X | X | X | X | X |
| neutrophils | X | X | X | X | X | X | X | X |
| C-reactive protein | X | X | X | X | X | X | X | X |
| creatinine | X | X | X | X | X | X | X | X |
| blood sugar | X | X | X | X | X | X | X | X |
| uremia | X | X | X | X | X | X | X | X |
| proteinuria | X | X | X | X | X | X | X | X |
| Oral examination | X | X | X | X | X | X | X | X |
| pocket probing depth | X | X | X | X | X | X | X | X |
| clinical attachment loss | X | X | X | X | X | X | X | X |
| plaque index | X | X | X | X | X | X | X | X |
| gingival index | X | X | X | X | X | X | X | X |
| bleeding on interdental brushing | X | X | X | X | X | X | X | X |
| Interdental microbiota analysis | X | X | X | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanoute, A.; Gare, J.; Meda, N.; Viennot, S.; Tramini, P.; Fraticelli, L.; Carrouel, F.; Bourgeois, D. Effect of Oral Prophylactic Measures on the Occurrence of Pre-Eclampsia (OP-PE) in High-Risk Pregnant Women: A Cluster Randomized Controlled Trial. Methods Protoc. 2021, 4, 61. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4030061
Kanoute A, Gare J, Meda N, Viennot S, Tramini P, Fraticelli L, Carrouel F, Bourgeois D. Effect of Oral Prophylactic Measures on the Occurrence of Pre-Eclampsia (OP-PE) in High-Risk Pregnant Women: A Cluster Randomized Controlled Trial. Methods and Protocols. 2021; 4(3):61. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4030061
Chicago/Turabian StyleKanoute, Aida, Jocelyne Gare, Nicolas Meda, Stephane Viennot, Paul Tramini, Laurie Fraticelli, Florence Carrouel, and Denis Bourgeois. 2021. "Effect of Oral Prophylactic Measures on the Occurrence of Pre-Eclampsia (OP-PE) in High-Risk Pregnant Women: A Cluster Randomized Controlled Trial" Methods and Protocols 4, no. 3: 61. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4030061